
Abstract
Background
One million individuals in the USA die from acute myocardial infarction (MI), which currently affects 3 million people globally. The available data about the early and late outcomes of both biodegradable polymer drug-eluting stents (BP-DES) and durable polymer drug-eluting stents exhibit inconsistency. We performed a meta-analysis comparing the safety and efficacy of BP-DES with DP-DES.
Methods
PubMed, Google Scholar, EMBASE, Cochrane, Ovid Medline, and Clinical Trials.gov databases were used to find out studies comparing BP-DES to DP-DES. All the analyses used the random-effects model.
Results
A total of 18 studies were incorporated in this meta-analysis that involved 28,874 patients, out of which 11,997 received the BP Stent, and the rest of 16,578 received the DP stent. Thorough analyses revealed that the risk of all-cause death was significantly higher in the BP-DES group (5.4% vs 2.7%) (RR 1.22, p 0.02) for two years or less than two-year follow-up. For studies with more than two years of follow-up, all-cause death was 9.07% (599/6603) in BP-DES and 9.47% (531/5602) in the DP-DES group but failed to achieve statistically significant levels (RR 0.97, p 0.58).
Conclusions
The study revealed no clinically significant (P value was > 0.05) differences in all-cause death, cardiac death, target lesion revascularization (TLR), late stent thrombosis, device-oriented composite endpoint/target lesion failure (DOCE/TLF), myocardial infarction (MI), target vessel MI, target vessel revascularization (TVR), target vessel infarction (TVI) between BP-DES and DP-DES for more than two years of follow-up. Additionally, all-cause death was only outcomes which found to have a statistically significant difference for less than two years of follow-up, while remaining were statistically non-significant.
Article highlights
-
1.
BP-DES results in a higher all-cause death rate over follow-up periods of < 2 years compared to DP-DES.
-
2.
There are no appreciable clinical differences between the two types of stents for follow-up periods longer than 2 years for BP-DES and DP-DES.
Similar content being viewed by others

Background
The prevalence of acute myocardial infarction has reached up to 3 million people around the world. Around 1 million patients die in the USA every year due to myocardial infarction (MI) [1]. MI causes permanent damage to the heart muscles and, ultimately, diastolic and systolic dysfunction in conjunction with many complications, including arrhythmias and heart failure [2]. Some of the identifiable risk factors include hypertension, dyslipidemia, smoking, and diabetes. Unfortunately, very little data are available on women and people from low ethnic backgrounds, which limits us from generalizing available data on the public [3]. Some recent reports from the World Health Organization have stated that in the next decade, most of the global burden of cardiovascular mortality will be from developing countries [3]. The emergency treatment of MI includes taking aspirin, nitroglycerin, oxygen, and some painkillers [4]. ST segment elevation MI requires restoration of blood flow, which is dealt with reperfusion therapy and angioplasty. Following a successful angioplasty treatment, nearly half of patients develop restenosis or re-occlusion within six months, and significant ischemia-related adverse events, such as repeat target vessel revascularization (TVR), can occur in up to 30% of instances [5]. It is critical to emphasize the benefits of stenting in this context, as it plays a pivotal role in reducing the occurrence of restenosis and re-occlusion, thereby minimizing the associated clinical events such as fatal re-infarction, nonfatal re-infarction, and repeat TVR in cases of recurrent ischemia [5].
The use of stents in percutaneous coronary intervention (PCI) has grown dramatically, leading to the evolution of several novel stent technologies for the treatment of symptomatic coronary disease [6]. When compared to bare metal stents (BMS), drug-eluting stents (DES) have considerably decreased the incidence of stent thrombosis, myocardial infarction, and death [7]. When first-generation stainless steel DES is compared to BMS, concerns regarding late complications such as in-stent restenosis and late stent thrombosis still exist [8]. Second-generation drug-eluting stents (DES) with enhanced stent platforms, biocompatible polymers, and more recent antiproliferative drugs were introduced to overcome the shortcomings of first-generation DES [9]. Nevertheless, neoatherosclerosis and late stent thrombosis have been connected to second-generation DES [10]. Due to prolonged re-endothelialization and delayed vascular healing, the polymer coating of drug-eluting stents has been linked to unfavorable outcomes, including stent thrombosis [11, 12]. In addition, stents that are bioresorbable or biodegradable were developed to lower the chance of restenosis.
BP-DES are safer and more effective than BMS and first-generation DES in lowering the incidence of very late stent thrombosis (ST) and restenosis [13]. Conflicting results exist on early and late stent thrombosis in DP-DES and BP-DES. Some research indicates that BP-DES carries a higher ST risk than DP-DES. Others argue that the BP-DES group has a lower ST rate than the DP-DES group [14, 15]. A recent meta-analysis of randomized controlled trials indicated no significant difference in very late stent thrombosis between two-year and five-year follow-ups for the two types of stents [16]. Verification of the safety and effectiveness of BP-DES is necessary due to the potential benefits it may provide individuals with acute myocardial infarction. This meta-analysis intends to assess the safety and efficacy of durable polymer drug-eluting stents (DP-DES) with biodegradable polymer drug-eluting stents (BP-DES), focusing on composite outcomes related to patients and devices. This study seeks to enhance the current literature by comparing BP-DES with DP-DES and presenting data to help formulate clinical recommendations for percutaneous coronary intervention with stenting.
Methods
To conduct this meta-analysis, we followed the principles established by Preferred Reporting Items for Systemic Review and Meta-Analysis (PRISMA) [17].
Data Source and Search Strategy
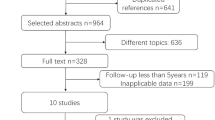
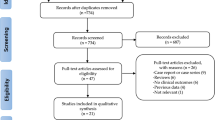
An extensive search strategy was applied on the PubMed database, Google Scholar, EMBASE, Cochrane, Ovid Medline, and Clinical Trials.gov until January 4, 2023. We applied medical subject headings (MESH terms) and specific keywords for applying the search strategy [Bio absorbable polymer OR BP STENT] AND [Durable polymer or DP STENT]. The Prisma flow chart (Fig. 1) and Supplementary Table S1 contain details regarding the search strategy.

PRISMA flow chart of the included studies
Eligibility criteria
Inclusion criteria
We included only those RCTs comparing outcomes between BP-DES and DP-DES. Patients who have undergone PCI were chosen, and the effect of the bioabsorbable and durable drug-eluting stent with its adverse outcomes was studied (all-cause death, cardiac death, target lesion revascularization, target vessel lesion, MI, stent thrombosis, DOCE, target vessel MI, target vessel infarction).
Exclusion criteria
We excluded case reports, observational studies, systematic reviews, editorials, duplicates, and those studies that have different population characteristics and different outcomes. Only studies that matched our PICO were considered for considered for this analysis.
Data extraction and quality assessment
The papers identified through the systematic search underwent exportation to the Mendeley Reference Library, where an initial screening for duplicates was conducted, and any duplicates were eliminated. Two independent reviewers, AR and SM, meticulously evaluated the remaining articles, selecting only those aligned with the pre-established criteria. The initial shortlisting of articles was based on title and abstract, followed by subsequent thorough reviews of the full papers to confirm relevance. Data extraction from the finalized reports encompassed study characteristics likes author details, publication period, study design, study participants, patients count, study rationale), clinical particulars, stent specifications, polymer type, drug details, and the drug's impact on outcomes such as all-cause death, DOCE, cardiac death, target lesion revascularization (TLR), MI, definitive, late and very late stent thrombosis, target vessel MI, target vessel revascularization (TVR), and target vessel infarction (TVI). The quality analysis of published Randomized Controlled Trials (RCTs) was conducted through the modified Cochrane’s risk of bias tool [18].
Statistical analysis
RevMan 5.4.1, a program created in 2014 by The Cochrane Center in cooperation with The Cochrane Collaboration, was used for the statistical analysis for this meta-analysis. The analysis only included comparison studies, and the findings were displayed as weighted mean differences (WMDs) for continuous outcomes and relative risks (RRs) for dichotomous results, respectively, using forest plots. The generic inverse variance with a random-effects model was utilized to ensure accurate results. P-values were subject to a significance level of less than 0.05. For every result, a funnel plot was created to evaluate the possibility of publication bias. Heterogeneity was assessed using Higgin's I2 test, and it was classified as low, moderate, or high. Our meta-analysis had very minimal heterogeneity. All outcomes with p-value < 0.05 were deemed significant, and the authors carefully examined the data to ensure accuracy and dependability. The study did not seek clearance from an ethical committee because the data came from earlier clinical studies with people who gave informed consent (Tables 1, 2).
Results
The initial product of the literature review produced a corpus of 190 articles. A subset of 18 studies [15, 19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35], all randomized controlled trials (RCTs), was found through the elimination of duplicates and rigorous evaluation of titles and abstracts. For this meta-analysis, only comparative studies were considered. A thorough search strategy was used, as shown in Fig. 1 through the PRISMA diagram. The articles in this collection span the years 2011 through 2022.
Quality assessment and publication bias
The Cochrane’s Risk of Bias tool, which consists of criteria for selection, performance, detection, attrition, and reporting bias, was used to assess the quality of eligible studies. One author (S.Q.) completed the initial data collection and quality assessment; another author (X.C.) then cross-verified the procedure. Any disparities that surfaced were resolved by consulting the initial research.
Outcomes
We evaluated a broad range of significant outcomes in our systematic review and meta-analysis comparing the long-term clinical results of BP-DES and DP-DES. These outcomes comprised of all-cause death, cardiac death, late stent thrombosis, device-oriented composite endpoint/target lesion failure (DOCE/TLF), myocardial infarction (MI), target vessel MI, TVR, and target vessel infarction (TVI). Our analysis sought a thorough understanding of the comparative performance of different stent types across these important clinical outcomes, providing valuable details about their relative efficacy and safety profiles.
All-cause death
Out of the 18 studies incorporated in our meta-analysis, data on all-cause death were provided by 17 studies. The pooled analysis showed that BP-DES is associated with an overall increased rate of all-cause death compared to DP-DES (RR: 1.05, p: 0.34). However, the findings mentioned are non-significant. Furthermore, subgroup analysis revealed that with more than two-year follow-up period, BP-DES showed a reduced risk of all-cause death in comparison with DP–DES (RR: 0.97, p: 0.58), whereas with ≤ 2-year follow-up there's a significantly higher rate of all-cause death with BP-DES (RR: 1.22, p: 0.02) (Fig. 2).

Forest plot showing all-cause death
Cardiac death
Data on cardiac death were provided by all the included studies. The analysis revealed that compared to DP-DES, BP-DES is associated with an overall increased rate of cardiac death (RR: 1.06, p 0.44). Additionally, the subgroup analysis for different follow-up periods showed that with ≤ 2 years of follow-up, BP-DES is associated with an increased cardiac death rate as compared to DP-DES (RR: 1.11, p: 0.38); similarly with more than 2 year follow-up BP-DES shows the same association (RR: 1.03, p: 0.75). However, the findings mentioned above are statistically non-significant (Fig. 3).

Forest plot showing cardiac death
Target lesion revascularization (TLR)
Information on TLR was acquired from all 18 studies our study. The pooled analysis generated that BP-DES has a lower overall need for TLR than DP-DES (RR: 0.95, p 0.45). Upon conducting subgroup analysis, with more than a 2 year follow-up period, BP-DES is associated with decreased necessity for revascularization as compared to DP-DES (RR:0.88, p: 0.22); moreover with two or more than two-year follow-up period, revascularization need is less necessary with DP-DES (RR: 1.02, p 0.78). However, the aforementioned findings are not statistically significant (Fig. 4).

Forest plot showing target lesion revascularization
Late stent thrombosis
16 out of the 18 studies involved in our study provided details on late stent thrombosis. The combined analysis revealed that late stent thrombosis is significantly lowered in patients treated with BP-DES compared to DP-DES (RR: 0.79, p 0.04). Furthermore, it was discovered after performing a subgroup analysis that patients who receive BP-DES appear to experience late stent thrombosis less frequently than those who receive DP-DES with both two-year or less than two-year follow-up (RR:0.84, p:0.33) as well as with more than two-year follow-up (RR: 0.75, p 0.06) (Fig. 5).

Forest plot showing late stent thrombosis
Device-oriented composite endpoint/target lesion failure (DOCE/TLF)
The rate of DOCE/TLF was reported in 11 out of 18 studies included in our study. The thorough analysis indicated a greater risk of DOCE/TLF associated with BP-DES than DP-DES (RR: 1.07, p 0.14). Likewise, subgroup analysis showed that with BP-DES the chances of DOCE/TLF are higher as compared to DP-DES with two years or less than two-year follow-up (RR: 1.08, p: 0.20) and with more than two-year follow-up (RR: 1.06, p 0.43). It is important to acknowledge that the findings presented above are insignificant (Fig. 6).

Forest plot showing device-oriented composite endpoint/target lesion failure
Myocardial infarction (MI)
In five of the 18 studies, data regarding myocardial infarction are provided. The combined analysis revealed a greater incidence of MI in patients receiving BP-DES compared to DP-DES (RR: 1.08, p 0.54). Moreover, subgroup analysis supported the same findings of higher MI occurrence with BP-DES in two years or less than two-year follow-up (RR: 1.07, p 0.60) and with more than two-year follow-up (RR: 1.12, p 0.75); however, these findings were not statistically significant (Fig. 7).

Forest plot showing Myocardial Infarction
Target vessel MI
In this meta-analysis, data on target vessel myocardial infarction were provided by four out of the 18 studies. Interestingly, our analysis did not reveal a significant difference in the risk of target vessel MI between BP-DES and DP-DES (RR: 1.00, p 0.99). After conducting subgroup analysis, BP-DES was correlated with a low risk of target vessel MI with two-year or less than two-year follow-up in comparison with DP-DES (RR: 0.98, p 0.90), but with more than two-year follow-up risk of target vessel MI is higher with BP-DES (RR: 1.14, p 0.73). Nevertheless, it is essential to note that the above-mentioned findings are not statistically significant (Fig. 8).

Forest plot showing target vessel MI
Target vessel revascularization (TVR)
Among the 18 studies, data on TVR were available from four studies. The pooled results demonstrated that patients studied with BP-DES had slightly higher rates of target vessel revascularization than DP-DES (RR: 1.01, p 0.95). On top of that, subgroup analysis revealed that with more than 2-year follow-up, there is a decreased rate of TVR with BP-DES as compared to DP-DES (RR: 0.79, p 0.31), and with two-year or less than two-year follow-up TVR risk is higher with BP-DES (RR: 1.09, p 0.63). The results described above are non-significant (Fig. 9).

Forest plot showing target vessel revascularization
Target vessel infarction (TVI)
Totally, 3 of the 18 studies involved our meta-analysis contributed data on target vessel infection. The combined analysis suggests a slightly greater incidence of TVI associated with BP-DES compared to DP-DES (RR: 1.03, p 0.73). Furthermore, sub-group analysis revealed that with two years or less than two years of follow-up, TVI incidence is higher with BP-DES (RR:1. 03, p 0.81); patients with follow-up exceeding two years displayed a lower risk of TVI with BP-DES (RR: 0.99, p 0.98) (Fig. 10).

Forest plot showing target vessel infarction
Discussion
Despite tremendous progress in the medical sciences, cardiovascular diseases (CVDs), such as acute myocardial infarction (AMI) and coronary artery disease (CAD), remain a major cause of mortality [1]. The advancement of drug-eluting stents (DES) in the early 2000s demonstrated a major breakthrough in the management of acute coronary syndrome (ACS). The BP-DES and the DP-DES are the two main types of these stents being compared in this topic. The platform, antiproliferative agent, and polymer coating are essential parts of DES. Lesion preparation with a balloon angioplasty catheter, guiding catheter, and coronary wire is used for stent implantation, followed by stent deployment [36]. Stent thrombosis, myocardial infarction, re-infarction, and cardiac death are among the consequences and outcomes linked to this surgery. TVI and TVR are two important concurrent outcomes. We integrated the results of five more RCTs into this evaluation. We assessed if they differed in any way from the earlier meta-analysis [16]. Based on the length of follow-up, the 18 included RCTs were divided into two sub-groups: those with follow-ups lasting two years or less and those with follow-ups lasting longer than two years.
BP-DES, which leave behind bare metal after polymer resorption, reduce complications like very late stent thrombosis and myocardial infarction [38] in contrast with DP-DES, which carry a risk of vascular inflammation [37]. Studies, however, show that compared to particular polymer durable stents, biodegradable polymer stents have a greater risk of stent thrombosis [39]. As a result, research on the relative safety and effectiveness of BP-DES and DP-DES is ongoing, requiring strong clinical backing. This meta-analysis aims to advance the clinical evidence comparing durable versus bioabsorbable DES. We have included 18 RCTs in our systematic review and meta-analysis, whose follow-up periods ranged from 12 to 60 months (5 years). Between bioabsorbable and durable DES, we could not find any significant differences in terms of device-oriented composite outcomes, such as cardiac death, target vessel MI, TVR, and target vessel infarction. Moreover, these groups had no appreciable variations in the rates of patient-oriented outcomes (revascularization, MI, and all-cause death).
During a three-year follow-up period, a recent meta-analysis found no statistically significant difference in mortality between BP-DES and DP-DES. There was no evidence of bioabsorbable DES outperforming durable DES in terms of mortality, even after a five-year follow-up [40]. Except for all-cause death, Mridha et al.'s meta-analysis revealed no differences in the clinical outcomes between BP-DESs and DP-DESs over mid- and long-term follow-ups [16]. One noteworthy finding from our meta-analysis is that it validates the superiority of DP-DES over BP-DES for all-cause death within a two-year follow-up period or less. But this dominance fades away after a follow-up period of > 2 years.
Compared to durable polymer DES, a protracted stent thrombosis—defined by the Academic Research Consortium as lasting more than a year or twelve months—has been linked to a noticeably decreased risk [41, 42]. There is conflicting information regarding extremely late ST because both types of stents showed similarities in-stent thrombosis at the two-year and five-year follow-ups, according to the most recent meta-analysis by Mridha et al. We evaluated stent thrombosis across follow-up periods of two years or longer. However, we found no statistically significant advantage of BP-DES over DP-DES. The lack of significance is probably due to variations in follow-up durations among the included RCTs. It is believed that the potential benefit of bioabsorbable polymer will become apparent following reabsorption, which might happen nine months following implantation [43]. There is no discernible difference in stent thrombosis between BP-DES and DP-DES, even with the long follow-up period of the trials in our meta-analysis.
Our meta-analysis has numerous strengths, which include all the latest RCTs up to 2022, which make the analysis more significant and up to date. This meta-analysis has a combination of all the results so that it could be easy to look for the outcomes and study them in one place. We have used diverse plots and tests, including the funnel plot, forest plot, etc. Furthermore, the result of our meta-analysis aligns with the recent meta-analysis done by Mridha et al. but contains all recently available literature. This meta-analysis supports the data that suggest the superiority of DP-DES over BP-DES in terms of all causes of death. Also, this meta-analysis shows no difference in stent thrombosis between BP-DES and DP-DES at follow-up periods of two or less than two years and even at a follow-up period of more than two years, which is consistent with the most recent meta-analysis by Mridha et al.
This analysis produced satisfactory statistical evidence, as shown in the results and figures; it is important to list some limitations. Every RCT has a different set of patient characteristics and settings. Variations in research design, intervention strategies, and baseline features of the patients, such as BMI, age, sample size, past medical history, and different struts of the stents used, may have produced some heterogeneity. Although we tried to divide the studies based on the follow-up period, still every RCT had a different follow-up time. Those with longer follow-ups can be considered more valuable. Similarly, number of participants and the ethnic group are some of the other differences among all the studies.
Conclusions
Based on the results of this systematic review and meta-analysis, we conclude that there were no clinically significant (P value was > 0.05) differences between BP-DES and DP-DES for more than two years of follow-up. The only significant difference for less than two years of follow-up was all-cause death. BP-DES stent and DP-DES stent are equal in terms of long-term clinical outcomes.
Availability of data and materials
Yes.
Abbreviations
- BP-DES:
-
Biodegradable polymer drug-eluting stents
- DP-DES:
-
Durable polymer drug-eluting stents
- MI:
-
Myocardial infarction
- TVR:
-
Target vessel revascularization
- BMS:
-
Bare metal stent
- PCI:
-
Percutaneous coronary intervention
- TLR:
-
Target lesion revascularization
- TVI:
-
Target vessel infarction
- DOCE/TLF:
-
Device-oriented composite endpoint/target lesion failure
- ACS:
-
Acute coronary syndrome
References
Kim SJ (2021) Global awareness of myocardial infarction symptoms in general population. Korean Circ J 51(12):997–1000. https://doi.org/10.4070/kcj.2021.0320
Mechanic OJ, Gavin M, Grossman SA (2023) Acute myocardial infarction. 2022 Aug 8. In: StatPearls. Treasure Island (FL): StatPearls Publishing
Oliveira GB, Avezum A, Roever L (2015) Cardiovascular disease burden: evolving knowledge of risk factors in myocardial infarction and stroke through population-based research and perspectives in global prevention. Front Cardiovasc Med 2:32. https://doi.org/10.3389/fcvm.2015.00032
Erhardt L, Herlitz J, Bossaert L, Halinen M, Keltai M, Koster R, Marcassa C, Quinn T, van Weert H, Task Force on the management of chest pain (2002) Task force on the management of chest pain. Eur Heart J 23(15):1153–76. https://doi.org/10.1053/euhj.2002.3194.
Antoniucci D, Valenti R, Trapani M, Moschi G (1999) Current role of stenting in acute myocardial infarction. Am Heart J 138(2 Pt 2):S147–S152. https://doi.org/10.1016/s0002-8703(99)70335-2
Hoole SP, Bambrough P (2020) Recent advances in percutaneous coronary intervention. Heart 106(18):1380–1386. https://doi.org/10.1136/heartjnl-2019-315707. (Epub 2020 Jun 10)
Jensen LO, Maeng M, Kaltoft A, Thayssen P, Hansen HH, Bottcher M, Lassen JF, Krussel LR, Rasmussen K, Hansen KN, Pedersen L, Johnsen SP, Soerensen HT, Thuesen L (2007) Stent thrombosis, myocardial infarction, and death after drug-eluting and bare-metal stent coronary interventions. J Am Coll Cardiol 50(5):463–470. https://doi.org/10.1016/j.jacc.2007.06.002. (Epub 2007 Jun 29)
De Luca G, Dirksen MT, Spaulding C, Kelbaek H, Schalij M, Thuesen L, van der Hoeven B, Vink MA, Kaiser C, Musto C, Chechi T, Spaziani G, Díaz de la Llera LS, Pasceri V, Di Lorenzo E, Violini R, Cortese G, Suryapranata H, Stone GW, Drug-Eluting Stent in Primary Angioplasty (DESERT) Cooperation. Drugeluting vs bare-metal stents in primary angioplasty: a pooled patient-level meta-analysis of randomized trials. Arch Intern Med. 2012;172(8):611–21; discussion 621–2. https://doi.org/10.1001/archinternmed.2012.758.
Dehghani P (2017) Bioresorbable polymers and stent devices. Curr Treat Options Cardiovasc Med 19(2):12. https://doi.org/10.1007/s11936-017-0510-1
Park SJ, Kang SJ, Virmani R, Nakano M, Ueda Y (2012) In-stent neoatherosclerosis: a final common pathway of late stent failure. J Am Coll Cardiol 59(23):2051–2057. https://doi.org/10.1016/j.jacc.2011.10.909
Nebeker JR, Virmani R, Bennett CL, Hoffman JM, Samore MH, Alvarez J, Davidson CJ, McKoy JM, Raisch DW, Whisenant BK, Yarnold PR, Belknap SM, West DP, Gage JE, Morse RE, Gligoric G, Davidson L, Feldman MD (2006) Hypersensitivity cases associated with drug-eluting coronary stents: a review of available cases from the Research on Adverse Drug Events and Reports (RADAR) project. J Am Coll Cardiol 47(1):175–181. https://doi.org/10.1016/j.jacc.2005.07.071. (Epub 2005 Dec 1)
Serruys PW, Daemen J (2007) Are drug-eluting stents associated with a higher rate of late thrombosis than bare metal stents? Late stent thrombosis: a nuisance in both bare metal and drug-eluting stents. Circulation 115(11):1433–9; discussion 1439. https://doi.org/10.1161/CIRCULATIONAHA.106.666826. Epub 2007 Mar 7.
Palmerini T, Biondi-Zoccai G, Della Riva D, Mariani A, Sabaté M, Smits PC, Kaiser C, D’Ascenzo F, Frati G, Mancone M, Genereux P, Stone GW (2014) Clinical outcomes with bioabsorbable polymer- versus durable polymer-based drug-eluting and bare-metal stents: evidence from a comprehensive network metaanalysis. J Am Coll Cardiol 63(4):299–307. https://doi.org/10.1016/j.jacc.2013.09.061. (Epub 2013 Nov 6)
Kang SH, Park KW, Kang DY, Lim WH, Park KT, Han JK, Kang HJ, Koo BK, Oh BH, Park YB, Kandzari DE, Cohen DJ, Hwang SS, Kim HS (2014) Biodegradable-polymer drug-eluting stents vs. bare metal stents vs. durable-polymer drug-eluting stents: a systematic review and Bayesian approach network meta-analysis. Eur Heart J 35(17):1147–58. https://doi.org/10.1093/eurheartj/eht570. Epub 2014 Jan 23
Serruys PW, Farooq V, Kalesan B, de Vries T, Buszman P, Linke A, Ischinger T, Klauss V, Eberli F, Wijns W, Morice MC, Di Mario C, Corti R, Antoni D, Sohn HY, Eerdmans P, Rademaker-Havinga T, van Es GA, Meier B, Jüni P, Windecker S (2013) Improved safety and reduction in stent thrombosis associated with biodegradable polymer-based biolimus-eluting stents versus durable polymer-based sirolimus-eluting stents in patients with coronary artery disease: final 5-year report of the LEADERS (Limus Eluted From A Durable Versus ERodable Stent Coating) randomized, noninferiority trial. JACC Cardiovasc Interv 6(8):777–789. https://doi.org/10.1016/j.jcin.2013.04.011
Mridha N, Subhaharan D, Niranjan S, Rashid MK, Psaltis P, Singh K (2019) A meta-analysis of randomized controlled trials to compare long-term clinical outcomes of bioabsorbable polymer and durable polymer drug-eluting stents. Eur Heart J Qual Care Clin Outcomes 5(2):105–113. https://doi.org/10.1093/ehjqcco/qcy036.Erratum.In:EurHeartJQualCareClinOutcomes.2019;5(1):82
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 29(372):n71. https://doi.org/10.1136/bmj.n71
Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, Thomas J. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10(10):ED000142. https://doi.org/10.1002/14651858.ED000142
Baber U, Chandiramani R, Mehta SR, Sartori S, Zhang Z, Claessen BE, Briguori C, Sharma S, Dangas G, Mehran R (2021) Safety and efficacy of the bioabsorbable polymer everolimus-eluting stent versus durable polymer drug-eluting stents in high-risk patients undergoing PCI: TWILIGHT-SYNERGY. Catheter Cardiovasc Interv 97(1):63–71. https://doi.org/10.1002/ccd.28995. (Epub 2020 Jun 10)
van Geuns RJ, Chun-Chin C, McEntegart MB, Merkulov E, Kretov E, Lesiak M, O’Kane P, Hanratty CG, Bressollette E, Silvestri M, Wlodarczak A, Barragan P, Anderson R, Protopopov A, Peace A, Menown I, Rocchiccioli P, Onuma Y, Oldroyd KG (2022) Bioabsorbable polymer drug-eluting stents with 4-month dual antiplatelet therapy versus durable polymer drug-eluting stents with 12-month dual antiplatelet therapy in patients with left main coronary artery disease: the IDEAL-LM randomised trial. EuroIntervention 17(18):1467–1476. https://doi.org/10.4244/EIJ-D-21-00514
Katagiri Y, Onuma Y, Lurz P, Buszman P, Piek JJ, Wykrzykowska JJ, Asano T, Kogame N, Takahashi K, Chang CC, de Winter RJ, Serruys PW, Wijns W; Collaborators (2020) Clinical outcomes of bioabsorbable polymer sirolimus-eluting stents versus durable polymer everolimus-eluting stents: two-year follow-up of the DESSOLVE III trial. EuroIntervention 15(15):e1366–e1374. https://doi.org/10.4244/EIJ-D-18-00944
de Winter RJ, Katagiri Y, Asano T, Milewski KP, Lurz P, Buszman P, Jessurun GAJ, Koch KT, Troquay RPT, Hamer BJB, Ophuis TO, Wöhrle J, Wyderka R, Cayla G, Hofma SH, Levesque S, Żurakowski A, Fischer D, Kośmider M, Goube P, Arkenbout EK, Noutsias M, Ferrari MW, Onuma Y, Wijns W, Serruys PW (2018) A sirolimus-eluting bioabsorbable polymer-coated stent (MiStent) versus an everolimus-eluting durable polymer stent (Xience) after percutaneous coronary intervention (DESSOLVE III): a randomised, single-blind, multicentre, non-inferiority, phase 3 trial. Lancet 391(10119):431–440. https://doi.org/10.1016/S0140-6736(17)33103-3. (Epub 2017 Dec 5)
van der Heijden LC, Kok MM, Zocca P, Jessurun GAJ, Schotborgh CE, Roguin A, Benit E, Aminian A, Danse PW, Löwik MM, Linssen GCM, van der Palen J, Doggen CJM, von Birgelen C (2018) Bioresorbable polymer-coated orsiro versus durable polymer-coated resolute Onyx Stents (BIONYX): rationale and design of the randomized TWENTE IV multicenter trial. Am Heart J 198:25–32. https://doi.org/10.1016/j.ahj.2017.12.011. (Epub 2017 Dec 21)
Arroyo D, Gendre G, Schukraft S, Kallinikou Z, Müller O, Baeriswyl G, Stauffer JC, Goy JJ, Togni M, Cook S, Puricel S (2017) Comparison of everolimus- and biolimus-eluting coronary stents with everolimus-eluting bioresorbable vascular scaffolds: two-year clinical outcomes of the EVERBIO II trial. Int J Cardiol 243:121–125. https://doi.org/10.1016/j.ijcard.2017.05.053. (Epub 2017 May 12)
Jiménez VA, Iñiguez A, Baz JA, Valdés M, Ortiz A, Vuilliomenet A, Mainar V, Dudek D, Banai S, Tüller D, Bonnet JL, De Miguel A, Bastos G, Wijns W, Saito S (2016) A randomized comparison of novel bioresorbable polymer sirolimus-eluting stent and durable polymer everolimus-eluting stent in patients with acute coronary syndromes: the CENTURY II high risk ACS substudy. Cardiovasc Revasc Med 17(6):355–361. https://doi.org/10.1016/j.carrev.2016.04.001. (Epub 2016 Apr 19)
Jinnouchi H, Kuramitsu S, Shinozaki T, Hiromasa T, Kobayashi Y, Morinaga T, Yamaji K, Soga Y, Shirai S, Ando K (2016) Two-year clinical outcomes of the NOBORI biolimus-eluting stents versus XIENCE/PROMUS everolimus-eluting stents in small vessel disease. Catheter Cardiovasc Interv 88(5):E132–E138. https://doi.org/10.1002/ccd.26360. (Epub 2015 Dec 28)
Wijns W, Suttorp MJ, Zagozdzon L, Morice MC, McClean D, Stella P, Donohoe D, Knape C, Ormiston J (2016) Evaluation of a crystalline sirolimus-eluting coronary stent with a bioabsorbable polymer designed for rapid dissolution: two-year outcomes from the DESSOLVE I and II trials. EuroIntervention 12(3):352–355. https://doi.org/10.4244/EIJY15M09_14
Zbinden R, Piccolo R, Heg D, Roffi M, Kurz DJ, Muller O, Vuilliomenet A, Cook S, Weilenmann D, Kaiser C, Jamshidi P, Franzone A, Eberli F, Jüni P, Windecker S, Pilgrim T (2016) Ultrathin strut biodegradable polymer sirolimus-eluting stent versus durable-polymer everolimus-eluting stent for percutaneous coronary revascularization: 2-year results of the BIOSCIENCE trial. J Am Heart Assoc 5(3):e003255. https://doi.org/10.1161/JAHA.116.003255
Kaiser C, Galatius S, Jeger R, Gilgen N, Skov Jensen J, Naber C, Alber H, Wanitschek M, Eberli F, Kurz DJ, Pedrazzini G, Moccetti T, Rickli H, Weilenmann D, Vuillomenet A, Steiner M, Von Felten S, Vogt DR, Wadt Hansen K, Rickenbacher P, Conen D, Müller C, Buser P, Hoffmann A, Pfisterer M, BASKET-PROVE II study group (2015) Long-term efficacy and safety of biodegradable-polymer biolimus-eluting stents: main results of the Basel Stent Kosten-Effektivitäts Trial-PROspective Validation Examination II (BASKET-PROVE II), a randomized, controlled noninferiority 2-year outcome trial. Circulation 131(1):74–81. https://doi.org/10.1161/CIRCULATIONAHA.114.013520. Epub 2014 Nov 19.
Xu B, Dou KF, Han YL, Lü SZ, Yang YJ, Huo Y, Wang LF, Chen YD, Wang HC, Li WM, Chen JY, Wang L, Wang Y, Ge JB, Li W, Gao RL (2011) A prospective multicenter parallel-controlled trial of TIVOLI biodegradable-polymer-based sirolimus-eluting stent compared to ENDEAVOR zotarolimus-eluting stent for the treatment of coronary artery disease: 8-month angiographic and 2-year clinical follow-up results. Chin Med J (Engl) 124(6):811–816
Meredith IT, Verheye S, Dubois C, Dens J, Farah B, Carrié D, Walsh S, Oldroyd K, Varenne O, El-Jack S, Moreno R, Christen T, Allocco DJ (2018) Final five-year clinical outcomes in the EVOLVE trial: a randomised evaluation of a novel bioabsorbable polymer-coated, everolimus-eluting stent. EuroIntervention 13(17):2047–2050. https://doi.org/10.4244/EIJ-D-17-00529
Natsuaki M, Kozuma K, Morimoto T, Kadota K, Muramatsu T, Nakagawa Y, Akasaka T, Igarashi K, Tanabe K, Morino Y, Ishikawa T, Nishikawa H, Awata M, Abe M, Okada H, Takatsu Y, Ogata N, Kimura K, Urasawa K, Tarutani Y, Shiode N, Kimura T (2015) Final 3-year outcome of a randomized trial comparing second-generation drug-eluting stents using either biodegradable polymer or durable polymer: NOBORI biolimus-eluting versus xience/promus everolimus-eluting stent trial. Circ Cardiovasc Interv 8(10):e002817. https://doi.org/10.1161/CIRCINTERVENTIONS.115.002817
Vlachojannis GJ, Smits PC, Hofma SH, Togni M, Vázquez N, Valdés M, Voudris V, Slagboom T, Goy JJ, den Heijer P, van der Ent M (2017) Biodegradable polymer biolimus-eluting stents versus durable polymer everolimus-eluting stents in patients with coronary artery disease: final 5-year report from the COMPARE II trial (abluminal biodegradable polymer biolimus-eluting stent versus durable polymer everolimus-eluting stent). JACC Cardiovasc Interv 10(12):1215–1221. https://doi.org/10.1016/j.jcin.2017.02.029. (Epub 2017 May 31)
Chevalier B, Wijns W, Silber S, Garcia E, Serra A, Paunovic D, Serruys P; NOBORI 1 investigators (2015) Five-year clinical outcome of the Nobori drug-eluting coronary stent system in the treatment of patients with coronary artery disease: final results of the NOBORI 1 trial. EuroIntervention 11(5):549–54. https://doi.org/10.4244/EIJY14M12_13.
Kufner S, Byrne RA, Valeskini M, Schulz S, Ibrahim T, Hoppmann P, Schneider S, Laugwitz KL, Schunkert H, Kastrati A (2016) Intracoronary stenting and angiographic results: test efficacy of 3 Limus-Eluting Stents (ISAR-TEST4) investigators. five-year outcomes from a trial of three limus-eluting stents with different polymer coatings in patients with coronary artery disease: final results from the ISAR-TEST 4 randomised trial. EuroIntervention 11(12):1372–9. https://doi.org/10.4244/EIJY14M11_02
Yelamanchili VS, Hajouli S. Coronary Artery Stents (2022) In: StatPearls. Treasure Island (FL): StatPearls Publishing
Byrne RA, Kastrati A, Massberg S, Wieczorek A, Laugwitz KL, Hadamitzky M, Schulz S, Pache J, Fusaro M, Hausleiter J, Schömig A, Mehilli J, ISAR-TEST 4 Investigators (2011) Biodegradable polymer versus permanent polymer drug-eluting stents and everolimus- versus sirolimus-eluting stents in patients with coronary artery disease: 3-year outcomes from a randomized clinical trial. J Am Coll Cardiol 58(13):1325–1331
Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, Kutys R, Skorija K, Gold HK, Virmani R (2006) Pathology of drug-eluting stents in humans: delayed healing and late thrombotic risk. J Am Coll Cardiol 48(1):193–202
Palmerini T, Biondi-Zoccai G, Della Riva D, Mariani A, Sabaté M, Smits PC, Kaiser C, D’Ascenzo F, Frati G, Mancone M, Genereux P, Stone GW (2014) Clinical outcomes with bioabsorbable polymer- versus durable polymer-based drug-eluting and bare-metal stents: evidence from a comprehensive network meta-analysis. J Am Coll Cardiol 63(4):299–307
Lu P, Lu S, Li Y, Deng M, Wang Z, Mao X (2017) A comparison of the main outcomes from BP-BES and DP-DES at five years of follow-up: a systematic review and meta-analysis. Sci Rep 7(1):14997
Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, Steg PG, Morel MA, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M, Krucoff MW, Serruys PW, Academic Research Consortium (2007) Clinical end points in coronary stent trials: a case for standardized definitions. Circulation 115(17):2344–2351
Ye Y, Xie H, Zeng Y, Zhao X, Tian Z, Zhang S (2013) Efficacy and safety of biodegradable polymer biolimus-eluting stents versus durable polymer drug-eluting stents: a meta-analysis. PLoS ONE 8(11):e78667
Ostojic M, Sagic D, Beleslin B, Jung R, Perisic Z, Jagic N, Nedeljkovic M, Mangovski L, Milosavljevic B, Stojkovic S, Orlic D, Antonic Z, Miloradovic V, Topic D, Paunovic D (2008) First clinical comparison of Nobori -Biolimus A9 eluting stents with Cypher- Sirolimus eluting stents: Nobori Core nine months angiographic and one year clinical outcomes. EuroIntervention: J EuroPCR Collab Work Group Intervent Cardiol Eur Soc Cardiol 3(5):574–579
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
The collaborative efforts of these authors collectively adhere to the rigorous authorship criteria set forth by the International Committee of Medical Journal Editors (ICMJE). AR, IEA, AN, RI, QR, ARSS, SJZ, SM, MMK, SK, MK, FS, and TM have demonstrated their commitment to ethical authorship practices. Each author has made substantial contributions to their respective research endeavors, encompassing tasks such as study conception, data analysis, manuscript drafting, critical revisions, and final approval for publication. Regardless of their diverse affiliations spanning institutions such as Shaikh Zayed Hospital, Federal Medical and Dental College, Dow University of Health Sciences, Quetta Institute of Medical Sciences, and Wayne State University, the uniformity in their dedication to fulfilling ICMJE guidelines reflects the collective integrity and excellence in the field of medical research.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Yes.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rehman, A., Ahmed, I.E., Nouman, A. et al. Comparison of long-term clinical outcomes of bioabsorbable polymer versus durable polymer drug-eluting stents: a systematic review and meta-analysis. Egypt Heart J 76, 91 (2024). https://doi.org/10.1186/s43044-024-00522-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43044-024-00522-1