
Abstract
Background
Autism spectrum disorder is a condition related to brain development that affects a person’s perception and socialization, resulting in problems in social interaction and communication. It has no single known cause, yet several different genes appear to be involved in autism. As a genetically complex disease, dysregulation of miRNA expression and miRNA–mRNA interactions might be a feature of autism spectrum disorder. The aim of the current study was to investigate the expression profile of circulating miRNA-128, miRNA-7 and SHANK gene family in ASD patients and to assess the possible influence of miRNA-128 and miRNA-7 on SHANK genes, which might provide an insight into the pathogenic mechanisms of ASD and introduce noninvasive molecular biomarkers for the disease diagnosis and prognosis. Quantitative real-time PCR technique was employed to determine expression levels of miRNA-128, miRNA-7 and SHANK gene family in blood samples of 40 autistic cases along with 30 age- and sex-matched normal volunteer subjects.
Results
Our study revealed a statistical significant upregulation of miRNA-128 expression levels in ASD cases compared to controls (p value < 0.001). A statistical significant difference in SHANK-3 expression was encountered on comparing cases to controls (p value < 0.001). However, miRNA-7 expression showed no significant difference between the studied groups.
Conclusions
MiRNA-128 and SHANK-3 gene are emerging players in the field of ASD. They are promising candidates as noninvasive biomarkers in autism. Future studies are needed to emphasize their pivotal role.
Similar content being viewed by others


Background
Autism spectrum disorder (ASD) represents a spectrum of multifaceted, pervasive and neurodevelopmental disorders that tend to manifest by 18 to 36 months of age. ASD is distinguished with social, communicative deficits and confined repetitive behavioral patterns. ASD is frequently associated with comorbidities such as epilepsy, intellectual disabilities (IDs), immune dysfunction, hyperactivity and gastrointestinal disorders [1, 2].
The prevalence of ASD is reporting an increased trend all over the world. It is estimated to be 1–2% of the population [3]. Although there are no epidemiological data for ASD in Egypt, an earlier study by Seif Eldin et al. [4] proposed a prevalence rate of 33.6% among Egyptian children with developmental disabilities. In 2017, 800,000 cases with ASD were reported in Egypt by the Social Solidarity Ministry [5]. It is worth noting that the variability in prevalence rates among different countries relies on the availability of screening tools and advanced diagnostic systems [3].
The cause of ASD remains to be elucidated; however, it is postulated that both environmental and genetic factors together play a pivotal role in risk development of ASD [6]. Currently, ASD is considered a primarily genetic disorder with 74–84% estimated heritability, the pathogenesis of which can be triggered by both pre- and postnatal environmental factors comprising maternal smoking, infections and pesticide exposure [2]. Moreover, increased risk of ASD can be attributed to prenatal drug exposure such as thalidomide, misoprostol and valproic acid [6].
SH3 and multiple ankyrin repeat domains proteins (SHANKs) are scaffolding proteins that are essential to synaptic formation, development and function. Many genetic studies proposed a strong association between the SHANK family genes (SHANK-1, SHANK-2 and SHANK-3) and ASD as well as other neurodevelopmental and neuropsychiatric disorders [7].
Deletions, duplications and coding mutations in the SHANK genes were detected in several patients with syndromic ASD and intellectual disability (ID) with higher severity in mutations in SHANK-3 and SHANK-2 genes compared to those in SHANK-1 [8].
Deletions and point mutations of SHANK-3 are correlated with Phelan-McDermid syndrome, ASD, intellectual disability, schizophrenia and bipolar disorder. Furthermore, its duplications are related to Asperger syndrome, attention deficit hyperactivity disorder, schizophrenia and bipolar disorder [9].
Point mutations of SHANK-2 and microdeletions of SHANK-1 and SHANK-2 have been implicated in patients with ASD, Alzheimer's disease, mild-to-moderate ID and non-syndromic ID [10, 11].
In view of the multifactorial nature implicated to ASD, it is possible that at least one epigenetic mechanism can be accused in ASD pathogenesis. MiRNAs can be highlighted as potential players in this field. MiRNAs are short noncoding nucleic acids that can influence the expression of entire gene networks by suppressing the transcription of messenger RNA (mRNA) into proteins [12].
MiRNAs are abundantly present in the central nervous system (CNS), producing around 70% of all miRNA species. Furthermore, changes in miRNA expression occur in the different stages of development and across various brain regions [13].
Accumulating evidence reveals that miRNAs are implicated in many biological and physiological processes including neurogenesis, neuroproliferation and synaptic plasticity in the CNS; thus, dysregulation of miRNAs is linked to behavioral and cognitional changes figured out in many neuropsychiatric disorders [6]. Altered peripheral miRNA expressions have been reported in a number of psychiatric disorders. Correlations between changes in neuroendocrine/ neuroimmune responses and different peripheral miRNAs patterns have been documented. Since brain tissue is not easily accessible, blood-based miRNAs, that are inexpensively, noninvasively and easily obtained, have been presented as clinically applicable biomarkers of psychiatric disorders [14].
In the case of ASD, it has been postulated that differentially upregulated miRNAs with high expression levels mostly suppress genes related to neuronal and synaptic dysfunction, whereas differentially downregulated miRNAs cause abnormal activation of genes involved in inflammatory and compensatory processes [13].
MicroRNA-128 is a brain-enriched miRNA highly expressed in the cortex, cerebellum and maturing cortical neurons. It functions in the context of regulating neurogenesis in the embryonic cortex, as well as proliferation and differentiation of neural progenitor cells (NPCs) by suppressing pericentriolar material 1 (PCM1). Thus, abnormal cortical development that underlies the pathophysiology of ASD can be attributed to aberrant expression of miR-128 [15]. Furthermore, dysregulated miR-128 potentially targets genes which are known genetic causes of ASD including neurexin 1, SHANK-3 and reelin genes [16, 17].
Recently, Aamodt identified miR-128 as a potential therapeutic target for ASD. His study postulated that inhibiting miR-128 could normalize microglia reactivity in autistic patients and thus improve clinical symptom severity. As miR-128 is a negative regulator of vocal learning, then reducing its levels in ASD patients could restore plasticity, or their capacity to learn to speak [18].
Another ASD-related miRNA, miR-7, which regulates the expression of the ASD risk gene SHANK-3, has a crucial role in proper development of cortical neural progenitors and cortical growth through its interactions with genes in P53 pathway. Thus, its dysregulation can result in abnormal development of hippocampal neurons [9, 19, 20].
In this study, we aimed to investigate the expression profile of circulating miRNA-128, miRNA-7 and SHANK gene family in ASD patients in comparison with typically developing children and to explore the posttranscriptional regulation of SHANK genes by miRNA-128 and miRNA-7, which might provide an insight into the pathogenic mechanisms of ASD and the possibility of employing the expression profiles of SHANK genes and the studied miRNAs as potential diagnostic biomarkers for ASD. A better understanding of ASD pathogenesis will pave the way for the introduction of new therapeutic approaches to improve the clinical symptoms in autistic patients.
Methods
Study design and sample collection
The present case–control study recruited 40 autistic participants; their ages ranged between 2 and 10 years, and 30 age- and sex-matched control subjects. Diagnosis of autistic disorder was assigned according to routine clinical interview and psychiatric examination using the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria [21] and Autism Diagnostic Interview-Revised (ADI-R) [22]. The Childhood Autism Rating Scale (CARS) was used for the assessment of autism severity [23].
Participants with congenital syndromes, neurological, metabolic disorders or malignancy were excluded from the present study as miRNA dysregulations have been demonstrated in these conditions [24,25,26]. Furthermore, Kichukova et al. [13], Vaccro et al. [28] and Vasu et al. [29] excluded such cases while studying miRNAs expression in ASD [13, 27, 28].
Full history taking with general emphasis on family history constructing a pedigree, consanguinity status, family history of similar conditions was carried out for all participants.
Five milliliters of peripheral venous blood were withdrawn from each participant under complete aseptic conditions; 3 milliliters was anticoagulated with ethylenediaminetetraacetic acid (EDTA) for immediate processing. Rest of blood was left to clot at room temperature (25 °C) and then centrifuged, and sera were separated and added to QIAZol in uniquely and properly identified sterile tubes for each individual subject and stored at − 80 °C.
Procedure
MiRNAs expression assay
Total RNA was isolated using QIAgen miRNeasy Mini isolation kit according to manufacturer’s protocol. MiR-128 and miR-7 were reversely transcribed using the TaqMan MicroRNA Reverse Transcription Kit (Applied Biosystems) and specific miRNA reverse transcription (RT) primers according to the manufacturer’s instructions in a final volume of 15 μL (incubated for 30 min at 16 °C, 30 min at 42 °C, 5 min at 85 °C and then maintained at 4 °C) and then stored at − 80 °C until analysis.
mRNAs expression assay
Extraction was done from whole blood using QIAamp RNA blood kit (QIAgen, Germany) according to manufacturer's instructions followed by immediate conversion to cDNA using High capacity cDNA Archive kit (Applied Biosystems) in a final volume of 20 μL (incubated for 10 min. at 25 °C, 120 min. at 37 °C, 5 min. at 85 °C and then maintained at 4 °C) and then stored at − 80 °C until analysis.
RNA concentration and quality were determined using NanoDrop 2000c spectrophotometer® (Thermo Fisher Scientific Inc. USA). Assessment of A260/A280 ratios revealed that all RNA samples are with sufficient quality for qPCR analysis (1.93–2.10).
For real-time PCR
Two microliters of RT products were mixed with 10 μL of Taqman PCR master mixture (No UNG), 1 μL TaqMan miRNA or mRNA assays and 7 μL nuclease-free water in a final volume of 20 μL.
All reactions were performed on QuantStudio 12 k flex Real-time system (Applied Biosystems) with the following conditions: 95 °C for 10 min, followed by 40 cycles at 95 °C for 15 s, and 60 °C for 1 min. Relative expression of target miRNAs was normalized to miRNA-16, and target mRNAs was normalized to B-actin. The fold changes of candidate miRNAs and mRNA expression were calculated by the equation 2−ΔΔCt (Fig. 1).

Flowchart illustrating the study methodology
Statistical analysis
All data were converted and manipulated by using SPSS software program version 18.0. Data were analyzed; mean and standard deviation were calculated for quantitative data. The quantitative variables were compared, and t-test was applied for parametric data. Mann–Whitney was applied for nonparametric data. The difference between groups was considered statistically significant when p < 0.05 and considered highly statistically significant when p < 0.01.
Results
A total of 70 participants aged between 2 and 10 years participated in the current research, comprising 40 autistic patients and 30 age- and sex-matched healthy individuals. The median age of autistic participants was 4 years, while that of controls was 3.6 years, with a statistically insignificant difference between patients and controls (p = 0.94, t = 0.2). The patient group included 29 (72.5%) males and 11 (27.5%) females, while the control group showed 22 (73.3%) males and 8 (26.7%) females, and the difference was statistically insignificant (p = 0.93).
The history and clinical data of the autistic cases are shown in Table 1.
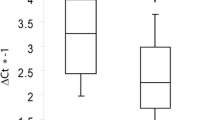
The upregulation of miRNA-128 expression level was statistically highly significant in cases than controls (p < 0.001). However, miRNA-7 showed no significant difference between the studied groups (p > 0.05) (Table 2; Figs. 2 and 3).

MiRNA-128 expression among the studied groups

MiRNA-7 expression among the studied groups
The expression of Shank-3 was upregulated in cases compared to controls with a statistical significant difference p < 0.001. However, both Shank-1 and Shank-2 expressions showed no significant difference in cases compared to that of controls (p = 0.8, p = 0.2, respectively) (Table 3; Figs. 4, 5, 6).

Shank-1 expression among the studied groups

Shank-2 expression among the studied groups

Shank-3 expression among the studied groups
The difference was insignificant in miR-7, miR-128 and Shank genes family expression levels considering gender and consanguinity among the patients group (Tables 4, 5).
Considering the family history of neuropsychiatric disorders, a statistically significant difference was detected between it and the expression of both miR-7 and Shank-2 gene among the patients group (p = 0.03) (Table 6).
Table 7 reveals a weak positive correlation between miR-7 and miR-128 (p = 0.001).
Discussion
ASD is highly heritable, with genetic contributions representing about 80% of ASD risk, and a higher risk observed autistic children’s siblings. Although epidemiological studies link the genetic contribution to autism, less is known about the putative genes involved [29, 30].
The developing brain encompasses many posttranscriptional mechanisms like microRNAs that adjust gene expression with the preservation of the genetic code. Such mechanisms are dysregulated in autistic cases. Altered miRNA expressions are detected in the brain, blood, saliva and olfactory precursor cells of ASD patients [31].
Neural progenitor cells can either divide or become specific types of neurons. If this proper scenario did not take place—for instance, if progenitors did not stop dividing in order to mature—various neurodevelopmental disorders may arise, comprising autism spectrum disorder [15].
MicroRNAs control gene activity and protein expression such as miR-128 that aids the newly formed neurons to travel to the correct region of the cortex, which is crucial for several cognitive processes including thought and language [15].
Our study demonstrated a significantly higher expression of serum miR-128 in autistic patients compared to age- and sex-matched healthy controls (p < 0.001), consistent with a study conducted by Zhang et al. [15], who investigated the role of miR-128 in the developing cortex of mice. Their results postulated that miR-128 prohibits cortical NPCs from dividing or development into more specialized cells. Overproduction of miR-128 in the progenitor cells caused the cells to divide less often and promoted their maturation into neurons. Contrarily, removing miR-128 from the progenitor cells enhanced their division and reduced neurons’ formation. Further investigation showed that miR-128 represses the production PCM1 protein that controls the proper division of the cells.
The observed actions of miR-128 are concordant with a Ge et al.’s study [32], who elucidated that PCM1 loss evoked the early exit of NPCs from the cell cycle and encouraged their premature differentiation to neurons. In their study, knockdown of PCM1 lead to the impairment of interkinetic nuclear migration of NPCs that causes the overproduction of neurons and premature exhaustion of the NPC pool in the developing neocortex.
In our study, miR-7 levels showed no significant difference among the studied patients and controls, which was concordant with a study conveyed by Mundalil Vasu et al. [28], in which miR-7 levels were not differentially expressed in ASD individuals and neither in controls. Contrasting studies were published by Hicks et al. [33] and Sehovic et al. [34], who presented a significant upregulation of miR-7 in saliva of autistic children.
Our study reported a significant association between both miR-7 and SHANK-2 gene with a family history of neuropsychiatric disorder. This result was revealed also by a study done by Zhang et al. [35] who detected that the circulating level of miR-7 was significantly increased in schizophrenia patients. They reported that overexpression of miR-7 suppressed the expression of SHANK-3 causing a significantly decline in the levels of SHANK-3 mRNA and protein. They concluded that miR-7 potentially plays a pivotal role in the pathophysiology of schizophrenia by binding to 3-prime untranslated regions of the mRNA and altering the morphology and function of neurons. Moreover, a study done by Viorel et al. [36] reported the frequent dysregulation of miR-7 in the brains of patients with neurocognitive disorders and in animal models of Alzheimer, Huntington’s and Parkinson’s diseases, implying that using agonist or antagonist miRNA oligonucleotides in the correction of miRNA expression might be a promising approach to ameliorate or even to cure such diseases.
Regarding SHANK-2, our results were consistent with that offered by Homann et al. [37], who sequenced the genomes of 90 individuals across nine families. Each family comprised at least three available relatives suffering from a psychotic illness and three available unaffected relatives. In one family, seven siblings with schizophrenia spectrum disorders each carried a new private missense variant within the SHANK-2 gene. This variant lied within the consensus SH3 protein-binding motif by which SHANK-2 can interact with postsynaptic glutamate receptors. Moreover, previous publications reported the alterations in the SHANK-2 gene locus in neuropsychiatric patients; they recognized SHANK-2 variations comprising truncations, missense mutations, deletions and SHANK-2 promoter regions mutations; all of these findings emphasized the causative link of SHANK-2 variants to ASD, IDs and schizophrenia [38, 39].
Mutations of genes that code synaptic cell adhesion molecules and scaffolding proteins which are important for the formation, stabilization and homeostasis of synapses, like neuroligins, neurexins and SHANK genes have been reported in patients with ASD. SHANK family genes code for scaffolding proteins lying in the postsynaptic density of glutamatergic synapses. Deletions and mutations of SHANK-3 are among the major genetic abnormalities in neurodevelopmental disorders, ASD, IDs and schizophrenia [40].
In our study, the SHANK-3 gene was significantly overexpressed in the patients’ group compared to the controls (p < 0.001). Our result was consistent with a study conveyed by Moessner et al. [41], who found that over-expression of SHANK-3 may result in ASD, as proved by a report of Asperger syndrome in an individual with three copies of SHANK-3 locus, supporting the hypothesis that autism is caused by improper excitatory/inhibitory neuronal ratios in the brain [42].
Moreover, SHANK-3 overexpression was also observed by Jin et al. [43], who detected an unanticipated increase in SHANK-3 transcripts in the brain regions that occurred in SHANK-3 heterozygous knockout mice with partial deletions of specific exons. This increase in SHANK-3 mRNA was not likely a nonspecific consequence of chromosomal alterations in the SHANK-3 that mostly occurred in the N-terminal exons in SHANK-3 mutant mice, which proposes selective compensatory activation of upstream SHANK-3 promoters in the process. One candidate player for this feedback mechanism is β-catenin, which, upon loss of synaptic SHANK-3, moves from the synapse to the nucleus to elicit histone deacetylase-2 dependent transcriptional modifications. Whether β-catenin directly binds to the upstream SHANK-3 promoters to stimulate their transcription needs to be confirmed [44].
Conclusions
In conclusion, our results demonstrate that the levels of miRNA-128 and SHANK-3 mRNA showed a statistical significant upregulation in Autistic patients. We suggest that this may reflect their metabolic imbalance in vivo; hence, this may provide a new insight regarding their molecular clues for recognizing autism disease.
A greater sample size of autistic patients is still needed in order to support these conclusions.
MiRNA-128 and SHANK-3 are emerging players in the field of ASD; future studies are needed to assess their implementation as diagnostic biomarkers and therapeutic targets in autism.
Availability of data and material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ASDs:
-
Autism spectrum disorders
- ADI-R:
-
Autism Diagnostic Interview-Revised
- CARS:
-
Childhood Autism Rating Scale
- ID:
-
Intellectual disabilities
- IQR:
-
Interquartile range
- MiRNA:
-
MicroRNA
- mRNA:
-
Messenger RNA
- NRCs:
-
Neural progenitor cells
- PCM1:
-
Repressing pericentriolar material 1
- SHANK:
-
SH3 and multiple ankyrin repeat domains protein
References
Salloum-Asfar S, Satheesh NJ, Abdulla SA (2019) Circulating miRNAs, small but promising biomarkers for autism spectrum disorder. Front Mol Neurosci 12:253
Yang G, Shcheglovitov A (2020) Probing disrupted neurodevelopment in autism using human stem cell-derived neurons and organoids: an outlook into future diagnostics and drug development. Dev Dyn 249:6
Baio J, Wiggins L, Christensen DL, Maenner MJ, Daniels J, Warren Z et al (2018) Prevalence of autism spectrum disorder among children aged 8 years-autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveill Summ 67:1
Seif Eldin A, Habib D, Noufal A, Farrag S, Bazaid K, Al-Sharbati M, Badr H et al (2008) Use of M-CHAT for a multinational screening of young children with autism in the Arab countries. Int Rev Psychiatry 20:281
Ereny G, Su M, Patrick S (2019) Education of children and young people with autistic spectrum disorders in Egypt. Br J Learn Disabil 47:29
Sehovic E, Spahic L, Smajlovic-Skenderagic L, Pistoljevic N, Dzanko E, Hajdarpasi A (2020) Identification of developmental disorders including autism spectrum disorder using salivary miRNAs in children from Bosnia and Herzegovina. PLoS ONE 15:e0232351
Sala C, Vicidomini C, Bigi I, Mossa A, Verpelli C (2020) Shank synaptic scaffold proteins: keys to understanding the pathogenesis of autism and other synaptic disorders. J Neurochem 135:849
Mossa A, Pagano J, Ponzoni L, Tozzi A, Vezzoli E, Sciaccaluga M, Costa C, Beretta S, Francolini M, Sala M, Calabresi P, Boeckers TM (2021) Sala1 C and Verpelli C: developmental impaired Akt signaling in the Shank1 and Shank3 double knockout mice. Mol Psychiatry. https://doi.org/10.1038/s41380-020-00979-x
Choi S, Pang K, Kim JY, Ryu RJ, Kang H, Liu Z et al (2015) Post-transcriptional regulation of SHANK3 expression by microRNAs related to multiple neuropsychiatric disorders. Mol Brain 8:74
Jiang Yh, Ehlers MD (2013) Modeling autism by SHANK gene mutations in mice. Neuron 78:8–27
Guilmatre A, Huguet G, Delorme R, Bourgeron T (2014) The emerging role of SHANK genes in neuropsychiatric disorders. Dev Neurobiol 74:113
Hicks SD, Carpenter RL, Wagner KE, Pauley R, Barros M, Tierney-Aves C et al (2020) Saliva microRNA differentiates children with autism from peers with typical and atypical development. J Am Acad Child Adolesc Psychiatry 59:296
Kichukova T, Petrov V, Popov N, Minchev D, Naimov S, Minkov I, Vachev T (2021) Identification of serum microRNA signatures associated with autism spectrum disorder as promising candidate biomarkers. Heliyon 7:e07462
Lee SY, Lu RB, Wang LJ, Chang CH, Lu T, Wang TY, Tsai KW (2020) Serum miRNA as a possible biomarker in the diagnosis of bipolar II disorder. Sci Rep 10:1131
Zhang W, Kim PJ, Chen Z, Lokman H, Qiu L, Zhang K, Rozen SG, Tan EK, Je HS, Zeng L (2016) MiRNA-128 regulates the proliferation and neurogenesis of neural precursors by targeting PCM1 in the developing cortex. Elife 5:e11324
Abu-Elneel K, Liu T, Gazzaniga FS, Nishimura Y, Wall DP, Geschwind DH, Lao K, Kosik KS (2008) Heterogeneous dysregulation of microRNAs across the autism spectrum. Neurogenetics 9:153
Ching A-S, Ahmad-Annuar A (2015) A perspective on the role of microRNA-128 regulation in mental and behavioral disorders. Front Cell Neurosci 9:465
- Aamodt CM (2021) Characterizing microRNA-128 as a therapeutic target for vocal communication deficits. UCLA. ProQuest ID: Aamodt_ucla_0031D_19561. Merritt ID: ark:/13030/m5g50fnb. Retrieved from, https://escholarship.org/uc/item/6sx3t1qn
Gao H, Zhong J, Huang Q, Wu X, Mo X, Lu L, Liang H (2021) Integrated systems analysis explores dysfunctional molecular modules and regulatory factors in children with autism spectrum disorder. J Mol Neurosci 71:358–368
Pollock A, Bian S, Zhang C, Chen Z, Sun T (2014) Growth of the developing cerebral cortex is controlled by miRNA-7 through the p53 pathway. Cell Rep 7:1184
American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edn. American Psychiatric Publishing, Arlington, p 50
Rutter M, Le Couteur A, Lord C (2003) ADI-R. Autism diagnostic interview revised. Manual. Western Psychological Services, Los Angeles
Schopler E, Reichler R, Rochen RB (1988) The childhood autism rating scale. Western Psychological Services, Vancouver
Paola ED, Verdile V, Paronetto MP (2019) Dysregulation of microRNA metabolism in motor neuron diseases: novel biomarkers and potential therapeutics. Non-Coding RNA Res 4(1):15–22
Sliwinska A, Kasinska MA, Drzewoski J (2017) MicroRNAs and metabolic disorders—where are we heading? Arch Med Sci 13(4):885–896
Syeda ZA, Langden SSS, Munkhzul C, Lee M, Song SJ (2020) Regulatory mechanism of MicroRNA expression in cancer. Int J Mol Sci 21:1723
Vaccro TS, Sorrentino JM, Salvador S, Veit T, Souza DO, Almeida RF (2018) Alterations in the MicroRNA of the blood of autism spectrum disorder patients: effects on epigenetic regulation and potential biomarkers. Behav Sci 8:75
Vasu MM, Anitha A, Thanseem I, Suzuki K, Yamada K, Takahashi T, Wakuda T, Iwata K, Tsujii M, Sugiyama T, Mori N (2014) Serum microRNA profiles in children with autism. Molecular Autism 5:40
Xie S, Karlsson H, Dalman C, Widman L, Rai D, Gardner RM, Magnusson C, Sandin S, Tabb LP, Newschaffer CJ, Lee BK (2020) The familial risk of autism spectrum disorder with and without intellectual disability. Autism Res 13:2242–2250
Tonacci A, Bagnato G, Pandolfo G, Billeci L, Sansone F, Conte R et al (2019) MicroRNA cross-involvement in autism spectrum disorders and atopic dermatitis: a literature review. J Clin Med 8:88
Hicks SD, Middleton FA (2016) A comparative review of microRNA expression patterns in autism spectrum disorder. Front Psychiatry 7:167
Ge X, Frank CL, de Anda FC, Tsai L-H (2010) Hook3 interacts with PCM1 to regulate pericentriolar material assembly and the timing of neurogenesis. Neuron 65:191
Hicks S, Ignacio C, Gentile K, Middleton F (2016) Salivary miRNA profiles identify children with autism spectrum disorder, correlate with adaptive behavior, and implicate ASD candidate genes involved in neurodevelopment. BMC Pediatr 16:52
Sehovic E, Spahic L, Smajlovic-Skenderagic L, Pistoljevic N, Dzanko E, Hajdarpasi A (2020) Identification of developmental disorders including autism spectrum disorder using salivary miRNAs in children from Bosnia and Herzegovina. PLoS ONE. https://doi.org/10.1371/journal.pone.0232351
Zhang Z, Sun X, Zhang L (2015) MicroRNA-7/Shank3 axis involved in schizophrenia pathogenesis. J Clin Neurosci 22:1254
Viorel S, Wissem DN, Helene B, Chantal P, Severine ML, Patrick B (2017) Pharmaco-modulation of microRNA expression in neurocognitive diseases: obstacles and future opportunities. Curr Neuropharmacol 15:276
Homann OR, Misura K, Lamas E, Sandrock RW, Nelson P, McDonough SI, Delsi LE (2016) Whole-genome sequencing in multiplex families with psychoses reveals mutations in the SHANK2 and SMARCA1 genes segregating with illness. Mol Psychiatry 21:1690
Peykov S, Berkel S, Schoen M, Weiss K, Degenhardt F, Weiss B et al (2015) Identification and functional characterization of rare SHANK2 variants in schizophrenia. Mol Psychiatry 20:1489
Eltokhi A, Rappold G, Sprengel R (2018) Distinct phenotypes of Shank2 mouse models reflect neuropsychiatric spectrum disorders of human patients with SHANK2 variants. Front Mol Neurosci 11:240
Leblond C, Heinrich J, Delorme R, Proepper C, Betancur C, Huguet G et al (2012) Genetic and functional analyses of SHANK2 mutations suggest a multiple hit model of autism spectrum disorders. PLOS Genet 8:e1002521
Moessner R, Marshall CR, Sutcliffe JS, Skaug J, Pinto D, Vincent J et al (2007) Contribution of SHANK3 mutations to autism spectrum disorder. Am J Hum Genet 81:1289
Bozdagi O, Sakurai T, Papapetrou D, Wang X, Dickstein DL, Takahashi N et al (2010) Haploinsufficiency of the autism-associated Shank3 gene leads to deficits in synaptic function, social interaction, and social communication. Mol Autism 17:1
Jin C, Kang HR, Kang H, Zhang Y, Lee Y, Kim Y et al (2019) Unexpected compensatory increase in Shank3 transcripts in Shank3 knock-out mice having partial deletions of exons. Front Mol Neurosci 12:1
Qin L, Ma K, Wang ZJ, Hu Z, Matas E, Wei J, Yan Z (2018) Social deficits in Shank3-deficient mouse models of autism are rescued by histone deacetylase (HDAC) inhibition. Nat Neurosci 21:564
Acknowledgements
The authors are gratefully acknowledging to the studied participants for their enrollment in the project.
Funding
National Research Centre funded this work under project (No. 11010161).
Author information
Authors and Affiliations
Contributions
AH participated in preparing the research design, conducting the laboratory work and preparing the paper for submission and final approval of the version to be published. OM participated in preparing the design of the research, data collection and statistical analysis. NA is responsible for patient’s selection and recruiting and diagnosis of the patients. MH participated in performing the laboratory work and revising the manuscript. MM participated in performing the laboratory work and data collection. SN participated in conducting the laboratory work and helped to draft the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Each participant’s guardian provided an informed written consent after full acknowledgement about the research. All procedures performed in our study involving human participants were in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the ethical committee of the National Research Centre (Registration number 16373).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abdelrahman, A.H., Eid, O.M., Ibrahim, M.H. et al. Evaluation of circulating miRNAs and mRNAs expression patterns in autism spectrum disorder. Egypt J Med Hum Genet 22, 81 (2021). https://doi.org/10.1186/s43042-021-00202-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43042-021-00202-8