
Abstract
Background
Knee Osteoarthritis (OA) is a highly prevalent age-related disease. The altered kinematic pattern of the knee joint as well as the adjacent joints affects to progression of knee OA. However, there is a lack of research on how asymmetry of the hip rotation angle affects the gait pattern in knee OA patients.
Research question
What are the impacts of asymmetric hip rotation range on gait biomechanical characteristics and do the gait patterns differ between patients with knee OA and healthy elderly people?
Methods
Twenty-nine female patients with knee OA and 15 healthy female elders as control group were enrolled in this study. The spatiotemporal parameters, kinematic and kinetic data during walking were measured using a three-dimensional motion capture system. The differences between knee OA and control group were analyzed using an independent t-test.
Results
The knee OA group exhibited a significant reduction in hip internal rotation range and internal/external rotation ratio on more affected side (p < 0.05). Significant differences were found in spatiotemporal parameters except to the step width. Significant reductions were also found in kinematic parameters (pelvic lateral tilt range, sagittal angle ranges in hip, knee and ankle, knee adduction mean angle). There were also significant differences in vertical ground reaction force and knee adduction moment (p < 0.05).
Conclusions
Knee OA patients have asymmetric hip rotation ranges. Especially limited hip internal rotation could lead to the reduction of pelvic lateral tilt, which may cause greater knee joint loading. Therefore, it is necessary to pay attention to recovery of hip rotation after knee surgery.
Similar content being viewed by others

Introduction
Knee osteoarthritis (OA) is the most common progressive disease among elderly people that causes difficulty in physical activities such as walking, sit to standing and descending stairs due to pain, joint stiffness and instability, and muscle weakness, all of which reduce quality of life [1]. Knee adduction moment (KAM) which provides an indication of the actual loads at the knee joint is recognized as a major clinical marker of knee OA progression [2, 3]. Many previous studies reported that poor alignments of the knee joint by tibial torsion or tibial varus deformity make people more liable to developing the knee OA and knee load increase [4, 5]. Therefore, higher dynamic knee loading is related to the progression of knee OA [6]. The movement of the human body is connected, so when a problem occurs in one joint, it can affect the other [7].
The foot posture and kinematics of the ankle joint, which is the distal joint of the knee affect the movement of the lower extremities during walking. Many studies have shown that foot progression angle is closely related to KAM [8,9,10]. The increased foot progression angle is known as the gait pattern to reduce increased KAM or to maintain mediolateral stability [11, 12]. The hip is the proximal joint of the knee. It affects the knee joint function and loading due to sharing a common segment with the knee [13, 14]. The angle of internal rotation and external rotation of the hip joint is the same at 45 degrees and is connected to each other, so if the internal rotation angle becomes small, the external rotation angle will increase [14]. Kim et al [15] reported that asymmetric hip rotation ranges increased the peak of the KAM.
Altered hip kinematics are associated with musculoskeletal problems, especially affecting adjacent joints such as knee pain and lower back pain. Until now, studies related to hip rotation asymmetry have been limited to young adults and athletes [15,16,17,18]. Although there are many patients who have difficulty walking with knee OA as well as lower back pain as they get older, studies related to hip rotation range in the elderly are insufficient. Therefore, the aim of this study is to investigate the range of hip internal rotation (IR) and external rotation (ER) and to find out the effect on gait patterns in knee OA patients. Our hypothesis was that hip internal rotation and lower limb joint angle in sagittal plane would decrease, and KAM, knee adduction angle and foot progression angle would increase in patients with knee OA.
Methods
Subjects
The power analysis was performed to determine the sample size for this study by using G-Power software (ver. 3.1.9.7; Franz Faul, University of Kiel, Germany). The effect size determined from a pilot study with 7 people in each group was 2.6. The calculated sample size was 12 (knee OA group, n = 6; control group, n = 6) with a significance level of 0.05, power of 0.95, and effect size of 2.6. This study reviewed 29 female patients with moderate to severe medial knee OA who were waiting to undergo total knee arthroplasty (TKA) surgery. We only enrolled female patients as subjects to remove the bias associated with the biomechanical gender differences. The following inclusion criteria were: (1) women aged 60 years or older; and (2) diagnosed with knee OA in the medial compartment with classified as Kellgren-Lawrence grade 3 (moderate) or 4 (severe). The exclusion criteria were: (1) concurrent back pain or any neurological disorders that could affect independent gait; (2) more osteophytes in the lateral compartment; and (3) rheumatoid arthritis. Fifteen age-matched healthy women were recruited as control group. The inclusion criteria were: (1) no clinical diagnosis of knee OA; (2) no neurological disorders or musculoskeletal disease; and (3) no history of lower limb surgery. All subjects signed the informed consent form, which was approved by the Haeundae-paik hospital Ethics Committee for Human Investigations.
Measurement protocol
We used a standard 12-inch plastic round universal goniometer to measure passive hip rotation range of motion. When measuring hip rotation, subjects were placed in the supine position on an examining table and they wore short pants. Leg alignment was visualized with two reference points (on the anterior tibial tuberosity and at the intersection of the bimalleolar line and the anterior crest of the tibia). The hip being measured was flexed to 90° and the contralateral hip was placed in neutral. The knee was flexed to 90° and the examiner moved ankle to produce hip rotation. The pelvic was stabilized with a strap firmly tightened over the sacrum to prevent the pelvic movement [17]. Through the above process, we acquired the hip IR and ER range and calculated additionally IR/ER ratio for easy comparison of the changed angles between IR and ER.
A VICON motion capture system (VICON Motion Systems Ltd, Oxford, UK) was used to collect the gait parameters including kinetic and kinematic data. Prior to the gait test, 16 retro-reflective markers (diameter of 14 mm) were placed on the patient. The locations of markers were based on the Plug-in-Gait model marker set for lower limb biomechanics (bilateral anterior and posterior superior iliac spines, lateral thigh, femoral epicondyle, tibia malleolus, second metatarsal head, and posterior calcaneus). All markers were fixed by the same examiner. After a static standing posture was captured, the patient was asked to walk along an 8-m walkway with two ground-embedded force plates (AMTI, Advanced Mechanical Technology Inc., Watertown, MA, USA) in the middle.
The marker data were synchronized with the kinematic data via Nexus software (VICON, version 1.7) and filtered at 6 Hz using a zero-lag, bidirectional second-order Butterworth filter. The kinetic data including knee adduction moment (KAM) and ground reaction force (GRF) were recorded using two force plates with a sampling rate of 1,000 Hz and processed using a low-pass filter with a cut-off frequency of 50 Hz. Spatiotemporal parameters, kinematic and kinetic data were calculated for each patient according to her anthropometric characteristic. Each subject walked at preferred speed until at least four gait cycles had been completed and were repeated more than three trials separately. Analyses were performed only for the leg scheduled for TKA surgery and if both legs were planned for surgery, more affected leg was selected for analysis. Only data on which each foot was precisely stepped on the force plate were selected, and two gait trials were averaged and analyzed. The pelvic lateral tilt and rotation, sagittal plane hip and knee range was calculated as maximum minus minimum value throughout gait cycle. Sagittal plane ankle range was calculated as maximum minus minimum value during mid- to terminal stance phase. Knee adduction and foot progression angle was calculated as mean value during stance phase. Peak external KAM and ground reaction force (GRF) was identified during stance phase. Acquired gait data were analyzed by using Polygon software (VICON, version 3.1) and the gait data were time normalized to the gait cycle. The KAM was normalized for body weight and height (%BW·Ht), and GRF was normalized to the body weight (%BW).
Statistical analysis
SPSS software (version 22.0, Chicago, IL, USA) was used for statistical analyses. Data were normally distributed, thus the general participant characteristics and gait parameters from the two groups were compared using independent t-tests. The level of statistical significance was considered value of p less than 0.05.
Results
There were significant differences in the mechanical axis and body mass index of demographic characteristics (Table 1). Significant reductions were in hip internal rotation range (p = 0.001) and IR/ER ratio (p = 0.003) between more affected side in knee OA group and right side in control group (Table 2).
In spatiotemporal parameters, we found that the walking speed, cadence and step length were decreased in knee OA group than in control group (p<0.05). There was no significant difference in step width between two groups (Table 3).
In kinematic and kinetic data, we found that pelvic lateral tilting range throughout gait cycle was significantly smaller in knee OA group than in control group (p = 0.022). Mean value of knee adduction angle during stance phase was significantly greater in knee OA group than in control group (p = 0.000). There were no significant differences in pelvic rotation range and foot progression angle between two groups. Peak vertical ground reaction force was significantly lower (p = 0.000) and KAM was significantly higher (p = 0.037) in knee OA group than in control group (Table 3).
Discussion
The most important finding of this study is that knee OA patients have asymmetric hip rotation range and IR/ER ratio. This was mostly consistent with our hypothesis, but the foot progression angle was not.
The hip internal rotation angle and IR/ER ratio on more affected side of knee OA group was significantly smaller than it on the right side of control group. This is similar to the previous results. Kim et al [15] showed that people who responded to the specialized mobility footwear had properties more related to the knee OA progression. The responders showed lower hip IR range and IR/ER muscle strength ratio. Cibulka et al [17] reported that the less hip IR range compared to ER often show the weakness of the hip internal rotator muscles. The larger difference between hip IR and ER range is associated with a more mal-alignment of the lower limb such as genu varum and valgus, pes planus [16, 19].
One of interesting findings of this study was that patients with knee OA with reduced hip IR showed significantly decreased pelvic lateral tilting range compared to control group. The hip internal rotation and pelvic 4° lateral tilting during loading response phase plays roles as absorbing the impact of the joint and helps the contralateral pelvic advancing. Hayot et al [20] emphasized that the pelvic lateral tilting has an important influence as strategies to minimize energy consumption during walking. Therefore, limiting the internal rotation of the hip joint leads to the limitation of the pelvic drop, which increases knee joint loading and prevents contralateral leg advancing [21]. In addition, if the external rotation movement is repeated due to the limitation of internal rotation of the hip joint, the stress on the ligaments around the hip and knee may increase. This repeated hip external rotation seems to have contributed to increasing pelvic backward rotation. The hip extensors and abductors play a primary action to make step length through late terminal swing to midstance phase [21]. In our study, there was no significant difference in pelvic rotation between groups. We consider that patients with knee OA may increase the pelvic rotation during gait to compensate the reduced sagittal hip and knee joint angles [22].
As the previous studies on gait analysis in patients with knee OA [23,24,25], walking speed, step length and cadence decreased and kinematic ranges of lower limb joints decreased, and KAM and knee adduction angle increased compared to the controls. Abnormal gait patterns are related to the knee pain and muscle weakness, and greater knee varus alignment led to the less knee flexion and greater KAM [12, 26, 27]. Since GRFs shows a strong correlation with faster walking speed [28], it could be expected that vertical GRF in knee OA patients would show a significant decrease. The KAM is calculated by GRF and its lever arm which the perpendicular distance between the vector line and the knee joint center [29]. Therefore, a significant increase in moment arm due to knee varus alignment would have contributed to knee OA progression, which showed greater KAM despite a significantly decreased GRF. In this study, only step width was no significant difference among spatiotemporal parameters. Elderly adults usually walk with wider step width compared to the youngers to ensure the dynamic stability [30]. According to a recent study [31], step width among people with knee OA affects trunk and gait patterns, and in this study, all patients with wide or narrow step width were included, so it seems that there is no difference from the control group.
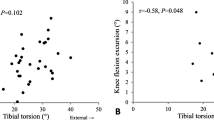
Contrary to the hypothesis that foot progression angle would increase in knee OA, we found that there was no significant difference between the two groups. Many previous studies have reported that out toeing gait compensate to reducing KAM [12, 32, 33], but a study has reported that KAM decreases during in-toeing gait [34]. Previous studies have shown that FPA in knee OA patients is still controversial. In our study, there was wide distribution in FPA including 4 patients with toe-in angle. Also, the external foot rotation appears as one of the compensation strategies for front plane stability walking. In this study, there was no significant difference in step width, so it is thought that it did not affect FPA. Yoon & Shin [31] reported that among female OA patients, those with wider step width showed greater foot progression angles. In addition, a recent study reported that external tibial torsion was related to external foot progression [35], but it is difficult to compare because external tibial torsion as one of our study limitations is not measured in this study.
There were several limitations in this study. First, there was a difference in BMI between the two groups. BMI is one of the important risk factors for knee OA. Therefore, it may affect the results of this study. Second, we did not include patients with mild knee OA because our subjects were composed of female patients with knee OA requiring TKA surgery. Therefore, there is a limit to the application to all patients with knee OA. Third, only the affected legs were compared, and the compensatory movement of contralateral side was not included in this study. Forth, we did not consider the patients’ hip anteversion that could affect hip rotation angle. Last, only the angles of hip IR and ER were compared without measuring the internal and external rotation muscle strength of the hip joint. Hip rotation cannot be separated from the role of the muscles involved. Therefore, additional study is needed to interpret hip rotation in patients with knee OA based on the dynamic role of muscles.
Conclusion
This study compared the hip rotation angles between patients with knee OA and controls, and investigated how asymmetric hip rotation angle affects the gait pattern in patients with knee OA. The patients with knee OA had asymmetric hip rotation ranges. Especially limited hip internal rotation could lead to the reduction of pelvic lateral tilt, which may cause greater knee joint loading during walking. Therefore, it is necessary to pay attention to recovery of hip rotation after knee surgery.
Availability of data and materials
Not applicable.
References
Sharma L, Dunlop DD, Cahue S, Song J, Hayes KW (2003) Quadriceps strength and osteoarthritis progression in malaligned and lax knees. Ann Intern Med 138:613–619
Kutzner I, Trepczynski A, Heller MO, Bergmann G (2013) Knee adduction moment and medial contact force–facts about their correlation during gait. PLoS ONE 8:e81036
Chang A, Hayes K, Dunlop D, Song J, Hurwitz D, Cahue S, Sharma L (2005) Hip abduction moment and protection against medial tibiofemoral osteoarthritis progression. Arthritis Rheum 52:3515–3519
Yang NH, Nayeb-Hashemi H, Canavan PK, Vaziri A (2010) Effect of frontal plane tibiofemoral angle on the stress and strain at the knee cartilage during the stance phase of gait. J Orthop Res 28:1539–1547
Iorio R, Healy WL (2003) Unicompartmental arthritis of the knee. JBJS 85:1351–1364
Miyazaki T, Wada M, Kawahara H, Sato M, Baba H, Shimada S (2002) Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann Rheum dis 61:617–622
Bennell KL, Hunt MA, Wrigley TV, Hunter DJ, Hinman RS (2007) The effects of hip muscle strengthening on knee load, pain, and function in people with knee osteoarthritis: a protocol for a randomised, single-blind controlled trial. BMC Musculoskelet Disord 8:1–9
McPoil TG, Warren M, Vicenzino B, Cornwall MW (2011) Variations in foot posture and mobility between individuals with patellofemoral pain and those in a control group. J Am Podiatr Med Assoc 101:289–296
Lynn SK, Kajaks T, Costigan PA (2008) The effect of internal and external foot rotation on the adduction moment and lateral–medial shear force at the knee during gait. J Sci Med Sport 11:444–451
Cho Y, Ko Y, Lee W (2015) Relationships among foot position, lower limb alignment, and knee adduction moment in patients with degenerative knee osteoarthritis. J Phys Ther Sci 27:265–268
Rebula JR, Ojeda LV, Adamczyk PG, Kuo AD (2017) The stabilizing properties of foot yaw in human walking. J Biomech 53:1–8
Hurwitz DE, Ryals AB, Case JP, Block JA, Andriacchi TP (2002) The knee adduction moment during gait in subjects with knee osteoarthritis is more closely correlated with static alignment than radiographic disease severity, toe out angle and pain. J Orthop Res 20:101–107
Powers CM (2010) The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther 40:42–51
Neumann DA (2010) Kinesiology of the musculoskeletal system. Foundations for Physical Rehabilitation, St. Louis
Kim Y, Richards J, Lidtke RH, Trede R (2018) Characteristics of clinical measurements between biomechanical responders and non-responders to a shoe designed for knee osteoarthritis. Gait Posture 59:23–27
Mirzaie G, Kajbafvala M, Rahimi A, Manshadi FD, Kalantari KK (2016) Altered hip mechanics and patellofemoral pain. A review of literature. Ortop Traumatol Rehabil 18:215–221
Cibulka MT, Strube MJ, Meier D, Selsor M, Wheatley C, Wilson NG, Irrgang JJ (2010) Symmetrical and asymmetrical hip rotation and its relationship to hip rotator muscle strength. Clin Biomech 25:56–62
Almeida GPL, de Souza VL, Sano SS, Saccol MF, Cohen M (2012) Comparison of hip rotation range of motion in judo athletes with and without history of low back pain. Man ther 17:231–235
Stief F, Böhm H, Schwirtz A, Dussa CU, Döderlein L (2011) Dynamic loading of the knee and hip joint and compensatory strategies in children and adolescents with varus malalignment. Gait Posture 33:490–495
Hayot C, Sakka S, Lacouture P (2013) Contribution of the six major gait determinants on the vertical center of mass trajectory and the vertical ground reaction force. Hum Mov Sci 32:279–289
Perry J, Burnfield JM (2010) Gait analysis. Normal and pathological function, 2nd edn. Slack, California
Bejek Z, Paróczai R, Illyés Á, Kiss RM (2006) The influence of walking speed on gait parameters in healthy people and in patients with osteoarthritis. Knee Surg Sports Traumatol Arthrosc 14:612–622
Dai J, Jin X, Ma JX, Wu YF, Lu B, Bai HH, Xl Ma (2023) Spatiotemporal and kinematic gait analysis in patients with knee osteoarthritis and femoral varus deformity. Gait Posture 105:158–162
Zeni JA Jr, Higginson JS (2009) Differences in gait parameters between healthy subjects and persons with moderate and severe knee osteoarthritis: a result of altered walking speed? Clin Biomech 24:372–378
Ismailidis P, Hegglin L, Egloff C, Pagenstert G, Kernen R, Eckardt A, Ilchmann T, Nüesch C, Mündermann A (2021) Side to side kinematic gait differences within patients and spatiotemporal and kinematic gait differences between patients with severe knee osteoarthritis and controls measured with inertial sensors. Gait Posture 84:24–30
Farrokhi S, O’Connell M, Gil AB, Sparto PJ, Fitzgerald GK (2015) Altered gait characteristics in individuals with knee osteoarthritis and self-reported knee instability. J Orthop Sports Phys Ther 45:351–359
Slemenda C, Heilman DK, Brandt KD, Katz BP, Mazzuca SA, Braunstein EM, Byrd D (1998) Reduced quadriceps strength relative to body weight: a risk factor for knee osteoarthritis in women? Arthritis Rheum 41:1951–1959
White S, Tucker C, Brangaccio J, Lin H (1996) Relation of vertical ground reaction forces to walking speed. Gait Posture 2:206
Sharma L, Hurwitz DE, Thonar EJM, Sum JA, Lenz ME, Dunlop DD, Schnitzer TJ, Kirwan-Mellis G, Andriacchi TP (1998) Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum 41:1233–1240
Dean JC, Alexander NB, Kuo AD (2007) The effect of lateral stabilization on walking in young and old adults. IEEE Trans Biomed Eng 54:1919–1926
Yoon JY, Shin SS (2024) Impact of step width on trunk motion and gait adaptation in elderly women with knee osteoarthritis. J Back Musculoskelet Rehabil
Guo M, Axe MJ, Manal K (2007) The influence of foot progression angle on the knee adduction moment during walking and stair climbing in pain free individuals with knee osteoarthritis. Gait Posture 26:436–441
Lynn SK, Costigan PA (2008) Effect of foot rotation on knee kinetics and hamstring activation in older adults with and without signs of knee osteoarthritis. Clin Biomech 23:779–786
Richards RE, Andersen MS, Harlaar J, van den Noort JC (2018) Relationship between knee joint contact forces and external knee joint moments in patients with medial knee osteoarthritis: effects of gait modifications. Osteoarthritis Cartilage 26:1203–1214
Huang C, Chan PK, Chiu KY, Yan CH, Yeung SS, Lai CW, Leung AK, Fu SN (2023) The association between tibial torsion, knee flexion excursion and foot progression during gait in people with knee osteoarthritis: a cross-sectional study. BMC Sports Sci Med Rehabil 15:110
Acknowledgements
This work was supported by a grant from Research year of Inje University in 2019(20190017).
Funding
None.
Author information
Authors and Affiliations
Contributions
JYY analyzed the data and wrote the manuscript. SWM designed the study, interpreted the data and wrote the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved Haeundae-Paik Hospital Ethics Committee for Human Investigation (#2021–10-032).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Yoon, Jy., Moon, S.W. Impacts of asymmetric hip rotation angle on gait biomechanics in patients with knee osteoarthritis. Knee Surg & Relat Res 36, 23 (2024). https://doi.org/10.1186/s43019-024-00226-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43019-024-00226-5