
Abstract
Purpose
Proximal tibia stress fractures present a challenge when performing total knee arthroplasty (TKA) in knee arthritis (KA). The literature on treatment modalities for stress fractures with arthritis is varied and not systematically reviewed. We aimed to answer the questions: (1) Is long-stem TKA sufficient for stress fractures in arthritic knees? (2) Should stress fracture and KA be addressed simultaneously? (3) What is the role of augmentative procedures in stress fractures with knee arthritis? (4) Can a unified algorithm be established?
Methods
The PubMed and Cochrane databases were searched for keywords such as stress fracture, knee arthritis and total knee arthroplasty, published from January 1995 to 29 May 2022. A total of 472 records were screened down to 13 articles on the basis of our selection criteria. Ten data items were recorded from the included studies. The methodological index for non-randomised studies (MINORS) score for the included studies was 17 ± 3.
Results
We found long-stem TKA to be sufficient for most cases and advocated for single-stage treatment of stress fractures and arthritis. Augmentative procedures play a role in the treatment, and a unified algorithm was drafted to guide treatment.
Conclusion
Single-stage management of advanced KA with a stress fracture causes less morbidity than a staged procedure. Long-stem TKA, with or without an augmentative procedure, is an excellent option.
Similar content being viewed by others


Introduction
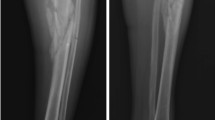
Total knee arthroplasty (TKA) is the gold standard for end-stage knee arthritis (KA) [1]. Long-standing end-stage arthritis can be complicated by a stress fracture of the proximal tibia (Figs. 1, 2). Wheeldon was the first to report stress fractures in patients with KA [2]. A stress fracture occurs due to abnormal loading of a normal bone (fatigue), normal loading of an abnormal bone (insufficiency) or a mix of both [3]. Coronal plane deformities associated with arthritis cause eccentric loading and stress concentration, leading to a stress fracture [4, 5]. Persistent malalignment predisposes to malunion, or non-union, of a stress fracture. X-ray is the imaging modality of choice for the baseline diagnosis of stress fracture. Acute stress fracture is easy to be neglected. In patients with acute-on-chronic pain, or with shin pain, in the proximal tibia, suspicion should be aroused . A magnetic resonance imaging (MRI)/computed tomography (CT)/three-phase bone scan can confirm the diagnosis [6]. While acute stress fracture may present as a single line, chronic stress fractures show subperiosteal bone formation [7].

Antero-posterior (AP) and lateral X-ray showing severe knee arthritis with proximal tibia stress fracture (extra-articular)

Antero-posterior (AP) and lateral X-ray showing severe knee arthritis with proximal tibia stress fracture (intra-articular)
Stress fractures associated with KA are more common in developing countries. Living with long-standing coronal plane deformity is commonly attributed to factors including lack of knowledge, fear of surgery, economic constraints and negligence towards KA [8, 9]. This causes a delay in surgery, which results in a progressive coronal plane deformity. Obesity, poor bone health and metabolic bone diseases are precipitating factors [3]. Proximal tibia stress fracture associated with KA usually presents with severe acute-on-chronic pain, leading to the inability to bear weight. Stress fractures cause discontinuity and deformity in the proximal tibia, making total knee arthroplasty more challenging. This presents a dilemma to surgeons whether to address them simultaneously or sequentially.
Management of proximal tibia stress fracture associated with severe KA is debatable, ranging from conservative management [10] to staged surgery involving corrective osteotomy followed by TKA [11, 12], simultaneous long-stem TKA and internal fixation of stress fracture using plating [13], the use of long stem TKA alone [14] or the use of any of the above with augmentative procedures such as proximal fibular resection (PFR) [15] and/or plating and bone grafting [9].
There has been an attempt to classify these fractures according to location (intra-articular versus extra-articular), fracture mobility, amount of deformity, and duration [9, 14], but this has added further complexity to an already rare entity. There is a paucity of literature about the management of stress fracture associated with severe KA. Very few publications state guidelines for management or have reported outcome analysis and potential complications. To the best of our knowledge, we did not find any meta-analysis or systematic review about stress fractures in severe arthritis.
Purpose of study: our purpose was driven by the following four questions:
-
(1)
Is long-stem TKA sufficient for stress fractures in arthritic knees?
-
(2)
Should stress fracture and knee arthritis be addressed simultaneously?
-
(3)
What is the role of augmentative procedures in stress fractures with knee arthritis?
-
(4)
Can a unified algorithm be established to treat stress fractures with knee arthritis?
Materials and methods
This systematic review was conducted as per the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement (PRISMA) [16].
Data and literature sources
We performed a Boolean search on PubMed and Cochrane databases, comprising the following keywords: “stress fracture”, “Knee arthritis” and “Total knee arthroplasty”. The search was conducted for all studies indexed on the databases from January 1995 to 29 May 2022. January 1995 was selected as a start date to exclude outdated literature. A combination of Stress fracture “AND” Knee arthritis, Stress Fracture “AND” Total Knee Arthroplasty was run as the search parameters in PubMed and Cochrane.
Study selection
Eligibility criteria
Studies were included or excluded on the basis of the following criteria:
Inclusion criteria
Studies that focused on proximal tibia stress fractures in patients with knee arthritis.
Exclusion criteria
-
(1)
Studies focusing on stress fractures of sites other than the proximal tibia.
-
(2)
Studies that included pathological fractures or traumatic fractures.
-
(3)
Case reports with fewer than three patients.
-
(4)
Studies that included stress fractures occurring after arthroplasty.
-
(5)
Articles not published in English.
Data extraction
Original articles were then retrieved from our institutional repository (including institutional access to the relevant journals). The full text from each article was read, and respective data were organised and analysed independently by three reviewers, and tabled in an Excel sheet. Excel sheets from all three reviewers were then compiled into a single document.
The following data were retrieved (where possible) from the selected studies:
-
1.
The total number of patients.
-
2.
Demographic parameters.
-
3.
Aetiology of arthritis and number of patients in each study.
-
4.
Body mass index (BMI) (available in 5 studies).
-
5.
Pre-op knee deformity (available in 11 studies).
-
6.
Post-op knee score (available in 11 studies).
-
7.
Modality of treatment used (isolated TKA/long-stem TKA/corrective osteotomy + TKA/PFR + long-stem TKA/plating and bone grafting + long-stem TKA) (Figs. 3, 4).
-
8.
Time to union.
-
9.
Complications.
-
10.
Type of implant used.

A–C Scanogram, AP and lateral view of osteoarthritis (OA) B/L knee with stress fracture (extra-articular) on right side

Post-operative scanogram
We also collected data on the authors, year and source of publication.
Identification of studies
Studies were identified from the search results. A total of 472 records were identified. Ninety duplicate records and 303 studies without stress fractures were excluded from screening, and three independent authors verified the exclusion. Seventy-nine articles were then screened by the same authors, independently. Forty-one records were excluded on the basis of this study’s criteria. Out of the remaining 38 articles, 4 could not be retrieved. Six articles were found to be irrelevant to the study. Case reports (n = 14) and articles in languages other than English (n = 1) were excluded. Thirteen studies were included in the review (Fig. 5).

PRISMA flowchart showing the studies that were included in our review
Assessment of methodological quality
MINORS was used to evaluate the quality of the included studies. Each item was scored as 0 (if not reported), 1 (when reported but inadequate) and 2 (when reported and adequate) [17].
The mean MINORS score was 17 ± 3 [mean standard deviation (SD) ± 2]. Major concerns were the lack of unbiased assessment of the study endpoint (no blinding), and only one randomised control study calculated sample size before the start of the study [15].
Data synthesis and analysis
Risk assessment was done on the basis of demography. Cumulative data were analysed to determine treatment patterns and formulate a treatment algorithm. Results were reviewed independently to discuss implications. We looked for the reference range of different outcomes mentioned in the studies. Acceptable alignment post-TKA was considered according to the theory of mechanical alignment [18]. The Knee Society Score (KSS) is excellent if it lies between 80 and 100 [19, 20]. A meta-analysis was not performed because of the lack of homogeneous comparative studies. According to age groups and gender, analysis was not done because of the lack of normalised data across included studies. All data were collected, and outcomes were narrated.
Results
Our research questions and the attempts to answer them are as follows:
-
(1)
Is long-stem TKA sufficient for stress fractures in arthritic knees?
Yes, in most cases, long-stem TKA is sufficient. Treatment is also dependent on the type of stress fracture, the degree of deformity and the tools available to a surgeon.
-
(2)
Should both stress fracture and knee arthritis be addressed simultaneously?
Yes, as the treatment of both is interlinked, quite like their pathologies. Thus, a stress fracture and KA should be managed in a single-staged procedure.
-
(3)
What is the role of augmentative procedures in stress fractures with knee arthritis?
Augmentative procedures such as PFR, osteotomy at the centre of rotation and angulation (CORA) of deformity, and plating and bone grafting play a role in malunion and severe deformity to (a) correct deformity and (b) maintain alignment.
-
(4)
Can a unified algorithm be established to treat stress fractures with knee arthritis?
Yes, after going through available literature, we have drafted a unified treatment algorithm (Fig. 6). Though this may serve as a guiding light, the treatment decision should depend on the treating surgeon’s experience and expertise, and be patient specific.

Showing unified treatment algorithm for management of stress fracture in proximal tibia after severe osteoarthritis
Data on deformity correction, knee scores, implant used, procedures performed and complications have been summarised in Tables 1 and 2.
Study characteristics
Most of the articles confirmed long-stem TKA as an adequate treatment. Two articles classified stress fractures and graded the need for proximal fibular resection with long-stem TKA [14, 21]. The authors advocated for osteotomy at the malunion site in case of extra-articular deformity > 30°, as it could not be addressed only with intra-articular resection [14, 21, 22]. Gill et al. classified patients similarly to Mullaji et al., but used plating and bone grafting in conjunction with TKA (with more reported complications in contrast to the other) [9, 14].Shah et al. conducted a prospective randomised controlled trial with a sample size of 62 [15]. In the control group (n = 31) (conventional treatment without fibular resection), the authors found delayed union and non-union in five patients and advocated for PFR for an early union. Pre-operative knee deformity was mentioned in 11 studies, but only 6 discussed post-operative deformity. In their article, Shah et al. mentioned post-operative deformity and reported 1.7° valgus in the study group (long-stem TKA with PFR), whereas the controls had 1.8 + 3.1° varus. Post-operative knee scores were available in 11 studies, all of which achieved excellent results (Table 1). BMI was taken into account in five studies, out of which it was > 30 kg/m2 in three studies.
KSS [23] (n = 10) and Western Ontario and McMaster Universities Arthritis index (WOMAC) [24] score (n = 1) were calculated in 11 studies. All of them reported good results with or without augmentative procedures.
Aetiology
The included studies examined 250 patients and 260 knees with a mean age of 67.0 years. Eighty per cent of the patients (200 out of 250) were women (Table 1). Except for Mittal et al. [21], the articles mentioned aetiology, with OA being 92.5% (n = 212) and the rest rheumatoid arthritis (RA) (n = 17).
Implant design: all studies used a posterior stabilised (PS) implant design, except Pai et al. [25], who used a cruciate-retaining (CR) implant. Gill et al. (n = 5 minor) and Jabalameli et al. (n = 5) reported that the use of constrained implants was required [9, 20].
Stem length
Every author has described that the stem should cross the fracture site, but no specific length description has been given. Pai et al. stated that the stem length should exceed the fracture site by a distance of at least two cortical diameters [25]. However, it is understandable that stem length can be more due to design differences among different manufacturers. Soundarrajan et al. stated that stem length should be planned preoperatively to cross the fracture site (due to said variations provided by different implant designs) [26].
Cemented/uncemented stem
All studies used uncemented stems but cemented the tibial base plates. Cementing of the proximal part of the stem is debatable. Some advocate cementing it [14, 20, 21], while others cemented only the tibial base plate [25,26,27]. More importantly, the consensus was that care must be taken to prevent cement from entering the fracture site.
Time to union of stress fracture
The radiological union was considered when bony continuity in three out of four cortices re-established. We did not find any reference range for the time to union of stress fractures of the proximal tibia. Therefore, we looked at the time to union in our included studies, which ranges between 7.2 and 26.1 weeks.
Rehabilitation protocol
Patients were allowed full weight-bearing from post-operative day zero by Reddy et al. [27], Rashid et al. [28], Jablameli et al. [20] and Mittal et al. [21]. Partial weight-bearing was allowed by Pai et al. [25], Dhillon et al. [8], Mullaji et al. [14] and Soundarrajan et al. [26] for 4–6 weeks. Mobile stress fractures (with only long-stem TKA as treatment) in the study by Gill et al. [9] were made to walk full weight-bearing with a knee immobiliser, while the patients in the other group (requiring long-stem TKA with plating) were made to walk non-weight-bearing for 4 weeks. Similarly, Soundarrajan et al. [26] kept patients who underwent plating non-weight-bearing for 4–6 weeks. All studies started knee range of motion and quadriceps strengthening exercises immediately following surgery.
Discussion
Severe knee arthritis with obesity and concomitant osteoporosis are risk factors for stress fractures. Single-stage management of advanced KA with a stress fracture causes less morbidity than a staged procedure. Long-stem TKA, with or without an augmentative procedure, is an excellent option and is associated with good outcomes (early fracture union, stable correction of severe deformity, and early patient ambulation). The posterior cruciate ligament may be sacrificed to correct severe deformity; thus, a PS implant should be kept as a backup. Efforts should be made to treat cases as early as possible, as early detection and intervention are the keys to prevent disease progression and deformity. Care must be taken to ensure no distraction at the fracture site in order to prevent the occurrence of non-union. Thorough clinical evaluation, laboratory evaluation and careful preoperative planning are essential in managing this complex conundrum. A wholesome and inclusive approach should be used to address the interlinked pathologies, thus breaking a vicious cycle.
Stress fractures are reported in 1.3% of patients with KA and are more frequently seen in the South-East Asian subcontinent [8]. These stress fractures are usually the result of altered weight-bearing, coupled with poor bone quality [3]. Most patients do not seek treatment for disabilities owing to these fractures. While the pain caused may be attributed to a variety of non-scientific reasons, the fact remains that a lack of knowledge about the complications of the deformity caused by the fractures makes timely treatment improbable. Bone mineral density was measured only by Gill et al. [9], who found osteoporosis in 9 and osteopenia in 10 out of the 24 patients. Osteoporosis carries with it a significant economic burden [29]. Since a stress fracture can occur due to fatigue (insufficiency) of the proximal tibia, patients should be worked up for altered bone metabolism, and the treatment offered should be wholesome and inclusive .
Mullaji et al. classified stress fractures into intra-articular and extra-articular fractures [14]. The authors further subclassified intra-articular into malunited and united, and extra-articular into impending, acute, uniting, malunited and united. A closed-wedge osteotomy and TKA with tibial stem extender in malunited extra-articular deformity, and debridement in conjunction with TKA with tibial stem extender and segmental fibulectomy, were performed in cases with non-union [14]. The opinions of authors included in the study were used to tackle the lack of consensus on treatment of stress fractures with KA. Fracture stability is an important concern and has been tackled in multiple ways. Fluoroscopy was used intraoperatively to check alignment, guide and check reaming in severe deformity and ascertain stem length [8, 14, 25, 26].
Shah et al. noted delayed union and non-union in five patients in the control group and advocated for PFR for early union [15]. However, in contrast, three studies have reported an earlier union without PFR [20, 25, 27]. Though the role of PFR remains inconclusive for early union, it may be helpful in stiff non-unions for the correction of the deformity.
A wholesome approach to treating stress fractures in arthritic knees in a single sitting has been advocated by all modern studies. TKA in conjunction with modular stems, with or without augmentative procedures, shows a good outcome. Early mobilisation, coupled with excellent KSS, makes outcomes of TKA in patients with stress fractures comparable to those of TKA performed in patients without stress fractures [32].
Limitations
The quality of this systematic review is inherently related to the quality of the included studies. While there was only one level I comparative clinical trial, the rest were level II, III and IV studies. This heterogeneity and lack of level I studies were significant shortcomings of our systematic review. Patient selection bias/uncontrolled confounding factors are more common in level III and IV studies. There were not enough homogeneous comparative studies available, which precluded us from analysing the results with a meta-analysis. Our analysis also could not control several factors that might have influenced the outcomes, such as various patient characteristics and implant designs used for treatment. To avoid the influence of this heterogeneity on our results, we decided not to pool the results and only report the values as a range. Limited studies have stated the treatment concerning the severity of the deformity. In the spirit of evidence-based medicine, these drawbacks should be analysed and reported in future studies to help guide an orthopaedic surgeon and better address patients’ expectations.
Conclusion
Single-stage management of advanced KA with stress fracture causes less morbidity than a staged procedure. Long-stem TKA, with or without an augmentative procedure, is an excellent option.
Data availability
All data generated or analysed during this study are included in this published article.
References
Zeni JA, Axe MJ, Snyder-Mackler L (2010) Clinical predictors of elective total joint replacement in persons with end-stage knee osteoarthritis. BMC Musculoskelet Disord. 11:86
Wheeldon FT (1961) Spontaneous fractures of the shin in the presence of knee deformities. Proc R Soc Med. 54:1108
Oh Y, Yamamoto K, Yoshii T, Kitagawa M, Okawa A (2021) Current concept of stress fractures with an additional category of atypical fractures: a perspective review with representative images. Ther Adv Endocrinol Metab. 12:204201882110496
Reynolds MT (1972) Stress fractures of the tibia in the elderly associated with knee deformity. Proc R Soc Med. 65:377–380
Sourlas I, Papachristou G, Pilichou A, Giannoudis PV, Efstathopoulos N, Nikolaou VS (2009) Proximal tibial stress fractures associated with primary degenerative knee osteoarthritis. Am J Orthop (Belle Mead NJ). 38:120–124
Expert Panel on Musculoskeletal Imaging: Bencardino JT, Stone TJ, Roberts CC, Appel M, Baccei SJ, Cassidy RC, Chang EY, Fox MG, Greenspan BS, Gyftopoulos S, Hochman MG, Jacobson JA, Mintz DN, Mlady GW, Newman JS, Rosenberg ZS, Shah NA, Small KM, Weissman BN (2017) ACR appropriateness criteria® stress (fatigue/insufficiency) fracture, including sacrum, excluding other vertebrae. J Am Coll Radiol. 14:S293–S306
Moran DS, Evans RK, Hadad E (2008) Imaging of lower extremity stress fracture injuries. Sports Med. 38:345–356
Dhillon MS, Prabhakar S, Bali K (2011) Management options for total knee arthroplasty in osteoarthritic knees with extra-articular tibial stress fractures: a 5-year experience. J Arthroplasty. 26:1020–1024
Gill UN, Noor SS, Haneef M, Ahmed N, Iqbal F, Najjad MKR (2021) Management of early and late presenting tibial stress fracture with advanced osteoarthritis of the knee: a dilemma among arthroplasty surgeons in developing countries. Knee. 29:95–100
Satku K, Kumar V, Pho R (1987) Stress fractures of the tibia in osteoarthritis of the knee. J Bone Joint Surg Br. 69-B:309–311
Cameron HU (1993) Double stress fracture of the tibia in the presence of arthritis of the knee. Can J Surg. 36:307–310
Wolff AM, Hungerford DS, Pepe CL (1991) The effect of extraarticular varus and valgus deformity on total knee arthroplasty. Clin Orthop Relat Res. 271:35–51
Moskal JT, Mann JW (2001) Simultaneous management of ipsilateral gonarthritis and ununited tibial stress fracture: combined total knee arthroplasty and internal fixation. J Arthroplasty. 16:506–511
Mullaji A, Shetty G (2010) Total knee arthroplasty for arthritic knees with tibiofibular stress fractures: classification and treatment guidelines. J Arthroplasty. 25:295–301
Shah VI, Upadhyay S, Shah K, Sheth A, Kshatriya A, Patil J (2020) Proximal fibular resection improves knee biomechanics and enhances tibial stress fracture healing in patients with osteoarthritis with varus deformity: a prospective, randomized control analysis. Arthroplast (London, England). 2:11
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 372:n71
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J (2003) Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 73:712–716
Lording T, Lustig S, Neyret P (2016) Coronal alignment after total knee arthroplasty. EFORT open Rev. 1:12–17
Asif S, Choon DSK (2005) Midterm results of cemented Press Fit Condylar Sigma total knee arthroplasty system. J Orthop Surg (Hong Kong). 13:280–284
Jabalameli M, Hadi HA, Bagherifard A, Rahbar M, Sajjadi MM (2018) Long-stem total knee arthroplasty for proximal tibial stress fractures in the elderly patients. Arch Bone Jt Surg. 6:376–380
Mittal A, Bhosale PB, Suryawanshi AV, Purohit S (2013) One-stage long-stem total knee arthroplasty for arthritic knees with stress fractures. J Orthop Surg (Hong Kong). 21:199–203
Sculco PK, Kahlenberg CA, Fragomen AT, Rozbruch SR (2019) Management of extra-articular deformity in the setting of total knee arthroplasty. J Am Acad Orthop Surg. 27:e819–e830
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the knee society clinical rating system. Clin Orthop Relat Res. 248:13–14
McConnell S, Kolopack P, Davis AM (2001) The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): a review of its utility and measurement properties. Arthritis Rheum. 45:453–461
Pai SN, Kumar MM, Vanchi PK, Ravi R, Kiswanth P (2022) Total knee arthroplasty with long tibial stem for tibial stress fractures with knee osteoarthritis: two birds with one stone. Chinese J Traumatol (English Ed) Chinese Medical Association.
Soundarrajan D, Rajkumar N, Dhanasekararaja P, Rajasekaran S (2018) Proximal tibia stress fracture with osteoarthritis of knee—radiological and functional analysis of one stage TKA with long stem. SICOT-J. 4:13
Reddy NVR, Saini MK, Reddy PJ, Thakur AS, Reddy CD (2022) Analysis of clinical and radiological outcomes of long tibial stemmed total knee arthroplasty in knee osteoarthritis complicated by tibial stress fracture. Knee Surg Relat Res BioMed Central. 34:1–8
Rashid RH, Zubairi AJ, Umer M, Hashmi PM, Lakdawala RH (2018) Management of stress fractures of the proximal tibia in patients with advance knee osteoarthritis. A case series. Acta Orthop Belg. 84:436–442
Fogel HA, Jenis LG (2020) The economic burden of osteoporosis. Vertebral compression fractures in osteoporotic and pathologic bone. Springer International Publishing, Cham, pp 21–29
Tomlinson MPW, Dingwall IM, Phillips H (1995) Total knee arthroplasty in the management proximal tibial stress fractures. J Arthroplasty. 10:707–713
Sawant MR, Bendall SP, Kavanagh TG, Citron ND (1999) Nonunion of tibial stress fractures in patients with deformed arthritic knees. Treatment using modular total knee arthroplasty. J Bone Joint Surg Br. 81:663–666
Barlow BT, Oi KK, Lee YY, Joseph AD, Alexiades MM (2017) Incidence, indications, outcomes, and survivorship of stems in primary total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 25(11):3611–3619
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
SP, SS and AR are involved in conception and design, acquisition of data, interpretation of data, and drafting the manuscript. RM helped in drafting and revising it critically for important intellectual content. TK is involved in the acquisition of data and interpretation of data. All the authors have given final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Not required.
Consent for publication
Not required.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shekhar, S., Rai, A., Prakash, S. et al. Single-stage long-stem total knee arthroplasty in severe arthritis with stress fracture: a systematic review. Knee Surg & Relat Res 35, 4 (2023). https://doi.org/10.1186/s43019-023-00178-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43019-023-00178-2