
Abstract
Purpose
The purpose of this study was to demonstrate closer-to-normal knee kinematics following primary total knee arthroplasty (TKA) performed establishing asymmetric gap balancing intraoperatively.
Material and method
Two age-, sex-, BMI-matched groups of patients underwent medially stabilized TKA because of isolated knee disease. Group A (12 patients) underwent “unrestricted” kinematic alignment (uKA) according to Howell while group B (15 patients) received robot-assisted “simplified” KA (sKA) with an alignment goal (Hip-Knee-Ankle axis-HKA) ± 5° respect to the mechanical axis. Intraoperatively, in group B, the flexion gap at 90° was first set at an average of 1.5 mm (0–5 mm; SD 4.4 mm) tighter in the medial compartment with respect to the lateral; in the same way, the extension gap was then set at an average of 2.0 mm (0–4.5 mm; SD 3.1 mm) tighter in the medial compartment with respect to the lateral. All patients, including a non-arthritic cohort (group C: 5 controls) underwent gait analysis using an instrumented treadmill (WalkerView–WV) equipped with an instrumented belt armed with a 3D video camera. The WV software evaluated multiple spatiotemporal and kinematic parameters, including: (1) contact time (s); (2) knee ROM during gait cycle; (3) step length percentage with respect to total gait (%) and pure step length (cm). Statistical analyses included t-Test and ANOVA and were conducted by using SPSS.
Results
At the final FU, significant differences were noted during gait between the two TKA groups (uKA-sKA) and the controls. Both TKA groups showed superior mean contact time on the surgical knee (uKA 1 s; sKA 0.97 s) as compared to the controls (0.72 s) (P = 0.002) while no differences were found between them (P = 0.11). TKA groups showed a lower, maximum ROM in the surgical knee (mean uKA 36º; mean sKA 49º) relative to the controls (mean 57º) (P < 0.05) but a statistical difference was found between them (P = 0.003). Both TKA groups showed a higher step length percentage with respect to the total gait and a shorter step length on the surgical side (uKA: mean 8.28% and mean step length 35.5 cm; sKA: mean 8.38% and mean step length 34.6 cm) in comparison to the controls (mean 3.38%; mean step length 71.4 cm) (P < 0.05) while no statistical differences were found between them.
Conclusion
To our knowledge, this was the first study to exhibit the kinematic advantages of a slightly asymmetric gap balancing during KA TKA. Combining a medially-stabilized implant design and a surgical technique aiming to obtain a tighter medial compartment represents a promising approach to improve outcomes after TKA.
Graphical Abstract

Similar content being viewed by others

Introduction
Historically, normal knee kinematics has not been reproduced following total knee arthroplasty (TKA) even when cruciate sparing designs and a mechanical alignment (MA) surgical technique were intraoperatively selected [1].
Both surgical techniques historically used to balance a TKA (“measured resection” and “gap balancing”) aimed for a perfect, symmetric balancing between the lateral and medial knee compartments [2]. Unfortunately, it has been shown that the recreation of symmetric and rectangular spaces in flexion and extension [3] does not match the kinematic profile of the native knee [4].
We and some other authors challenged the dogma that achieving symmetric gaps during the balancing phase of the TKA procedure should still represent the “gold standard” [5, 6]. Thanks to the introduction of enhanced digital technologies, such as robotics, smart sensors, and augmented reality tools, the empirical and surgeon-dependent definition of a well-balanced knee can be finally replaced by the accuracy in gap measurements yielded by computer-assisted technologies. However, an exact quantification of the desirable amount of inter-compartmental asymmetry during the TKA procedure is still lacking. This is also because gait analysis studies comparing symmetrically-balanced and asymmetrically-balanced knees are lacking. The fear of mid-flexion instability also pushed surgeons to stay in the “safe zone” of symmetric gap balancing since surgical technique-related risk factors have been believed to be responsible for this complication [7].
We recently published a robot-assisted, simplified surgical technique [8], which was based on the recreation of clearly defined, slightly asymmetric flexion and extension gaps. This surgical technique was combined with the use of a medially-stabilized TKA design. This gait analysis study hypothesized that the robotic-guided, intraoperative reproduction of a slight mediolateral gap asymmetry during TKA improved the postoperative knee kinematics compared to the traditional inter-compartmental gap symmetry.
Materials and methods
Two retrospectively matched (age, sex, BMI) groups of patients underwent medially-stabilized TKA because of isolated knee disease. Patient demographics are shown in Table 1. Inclusion criteria in both TKA groups were: (1) age > 18 years, (2) successful TKA with Knee Society Clinical Score > 80, and (3) preoperative, unilateral bicompartmental knee OA. Exclusion criteria included the presence of chronic inflammatory diseases or other disorders affecting the execution of the gait analysis. Group A (12 patients) underwent “unrestricted” kinematic alignment (uKA) with symmetric gap balancing according to Howell et al. [9]; the same medial pivot implant (GMK Sphere, Medacta, Castel San Pietro, Switzerland) was used in all cases. Group B (15 patients) underwent robot-assisted “simplified” kinematic alignment (sKA) with an alignment goal (Hip-Knee-Ankle axis-HKA) ± 5° with respect to mechanical axis and a slight mediolateral asymmetry of the flexion and extension gaps [8]. The same medially-congruent implant (Persona MC, Zimmer Biomet, Warsaw, IN, USA) was employed in all cases. In group B, the flexion gap at 90° was set first at an average of 1.5 mm (0–4.5 mm; SD 3.1 mm) tighter in the medial compartment with respect to the lateral. In the same way, the extension gap was then set at an average of 2 mm (0–5 mm; SD 4.4 mm) tighter in the medial compartment with respect to the lateral. All surgeries were performed under spinal anesthesia with the use of a tourniquet.
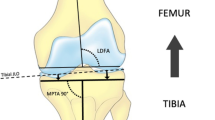
All TKA patients were radiologically evaluated before gait analysis. The final LDFA, MPTA, and final HKA were measured on weight-bearing, full-leg films to correlate the final HKA axis to the gait analysis data.
All patients, including a non-arthritic cohort (Group C: 5 healthy controls) underwent gait analysis evaluation. The gait analysis was carried out utilizing a modern instrumented treadmill (WalkerView™-WV-by TecnoBody, Dalmine, Italy) equipped with an instrumented belt enriched with 8 load cells, a 48"-wide LCD screen providing continuous virtual reality/biofeedback, a 3D video camera (Kinect v2, Microsoft, USA) and a control, 15" touchscreen interfaced to PC. The WV-integrated software utilized for the gait analysis (TecnoBody MS, Dalmine, Italy) evaluated, in real-time fashion, multiple spatiotemporal parameters (cadence, stance/swing times, step time, and step length) and kinematic variables (spine, hips and knees ROM).
Gait analysis setup and data processing
All TKA patients underwent gait analysis at a minimum follow-up (FU) of 9 months (270 days) from the surgical procedure. On average, the gait analysis was performed 289 days after the index procedure (range, 274–302 days). No patients underwent preoperative gait analysis. Before gait trials, healthy controls and patients were asked to familiarize themselves with the WV treadmill platform by undertaking a 20-min walk at their comfortable speed (maximum 20 km/h).
After a 15-min trial, all participants underwent a 3-min gait test at their comfortable speed (Fig. 1). In particular, the belt speed was increased to the comfortable one gradually (about 30 s), then data of 2 min were captured, and lastly, the belt speed was gradually reduced to a stop (about 30 s). The recorded gait spatiotemporal and kinematic parameters were as follows: spine/hips/knees ROM; left/right load symmetry/asymmetry; cadence (cycle/s); left and right step length; time of ground contact; center of gravity variation during gait (cm and %).

A 69-year-old patient undergoing gait analysis using an instrumented treadmill (WalkerView, TecnoBody MS, Dalmine, Italy)
Particular attention was paid to the following spatiotemporal and kinematic parameters: (1) Contact time (s); (2) Knee peak ROM during gait cycle; (3) Step length percentage with respect to total gait (%) and pure step length (cm). The same physical therapist (MB), with experience in gait analysis, oversaw the correct execution of the test and acquired all data.
Statistical analysis
Spatiotemporal and kinematic parameters outcomes were compared using SPSS statistical package, version 25 (SPSS Inc, Chicago, IL, USA). Data from the three groups (control group, uKA group and simplified-KA group) were statistically compared for each variable of interest using student t-Test and one-way analysis of variance (ANOVA). The level of significance was set at P < 0.05. The study was approved by the internal review board (IRB: SABES 71/2023) and was performed according to Helsinki’s declaration.
Results
A total of 32 gait trials were acquired: 5 in the control group, 12 in the uKA group, and 15 in the simplified KA group. In the control group, spatiotemporal and kinematic parameters were reported as an average between the left and right lower extremities, while, in the two TKA groups, data were reported and compared between the contralateral, healthy side, and surgical side.
Spatiotemporal parameters
The main spatiotemporal findings are presented in Table 2. No statistical differences were found between the healthy controls and the two TKA groups other than in cadence and healthy knee step length (%). No statistical differences were found between the two TKA groups.
Kinematic parameters
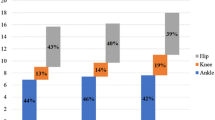
The main kinematic findings are given in Table 3. Statistical differences were found between the healthy controls and the two TKA groups in several kinematic parameters, including anteroposterior (AP) spine flexion, and knee ROM (surgery side and healthy side). Statistical differences were found between the two TKA groups in AP spine flexion and knee peak ROM (surgery side and healthy side) (Fig. 2). A not statistically significant trend was also demonstrated between the two TKA groups in the peak hip ROM.

Knee range of motion (ROM) during the gait cycle: comparison between controls, uKA and simplified KA (sKA). sKA: simplified kinematic alignment [8]; uKA: unrestricted kinematic alignment. ROM was expressed as average values, and the gait curves have been extracted utilizing the software PlotDigitizer (Porbital, USA). SS: statistically significant differences were calculated using one-way analysis of variance (ANOVA)
Radiological evaluation
No statistical differences were found between the uKA and simplified KA groups in the final alignment (Table 4).
Discussion
To the authors’ knowledge, this was the first study to show the “in vivo” kinematic advantages of a slightly asymmetric intercompartmental gap balancing during primary TKA. When compared with simplified KA with slightly asymmetric gaps, patients following uKA with traditional symmetric gap balancing showed reduced knee flexion during the early stance and initial knee extension (i.e., midstance) phases of gait, reduced knee flexion during mid-swing and also higher hip extensor contribution to the total support moment during the early stance phase of gait. These findings confirmed previous reports [10], showing that individuals with less natural knee kinematics and joint instability demonstrated significantly reduced flexion and axial rotation knee motion excursions during the loading response phase of gait. Recently, Meneghini et al. [6] reported superior PROMs for patients with more lateral laxity, manually evaluated using a calibrated tensor device, at 90° of flexion compared with patients with more medial laxity. The authors [6] used a lateral conforming or a posterior-stabilized (PS) inserts, different from the current study where only medially-stabilized inserts were used. In the current study, the authors used the imageless robotic system in a navigation mode to accurately define the mediolateral asymmetry in the flexion and extension gaps [8]. It has been recently shown that enabling technologies allow for micrometric precision in intraoperative gap balancing [11]. Most commercially available robotic systems provide a touchscreen with integrated software, controlled directly by the surgeon, capable of extreme accuracy (μm) during intraoperative gap determination.
The current results also challenged the recent concept that the reproduction of the constitutional knee alignment in its extreme variants represents the main driver to a close-to-normal knee kinematics and joint proprioception: if the reproduction of the joint obliquity through pre-planned bone cuts has a major role on the coronal and transverse plane alignment of the knee joint at initial contact [12], the restoration of pre-arthritic, “static joint” line is not sufficient to recover the real, pre-arthritic kinematics of knee joint, which is “dynamic” by definition. Multiple studies [13,14,15,16] confirmed that the static measures in frontal radiographs are not necessarily a casual predictor of the dynamic contact loads in vivo. The uKA with its “pure resurfacing” principles has multiple fascinating features: it is applicable using standard instrumentation upgraded with 2-mm shims to compensate for the predicted cartilage wear, does not require advanced forms of radiologic evaluation (i.e., CT scans) and it is independent from the use of enabling technologies. This “one size fits all”, pure measured resection surgical technique, anyway, is based on the reproduction of a rigorously symmetric extension gap, to a point that the original authors recommend a 2-mm bone recut (especially in originally varus knees) to ensure the symmetry of the gap itself [9] if a slight asymmetry is intraoperatively noted. Edelstein et al. [17] recently published a worrisome report on the relationship between laxity, balance, and alignment following uKA TKA: in 382 simulated TKAs, only less than 30% had a mediolateral extension ligament balance within ± 1 mm and up to 56% had a medial flexion gap looser than the lateral one.
The current study also showed that major differences still exist between the normal knee (as shown in the control group) and both TKA groups. Previous studies, including those from the senior author’s institution [18, 19], showed strong kinematic differences when knees were evaluated during the stance phase of gait (center of rotation being on the lateral knee compartment) or during the swing phase of gait, like stairs ascending activities and squatting, having the center of rotation on the medial compartment. This normal kinematics was guided by the anterior cruciate ligament (ACL), which is routinely removed during TKA. Interestingly, what has been proposed as the gold standard for many years, a cruciate sparing TKA design combined with an MA surgical technique, showed inferior kinematics when compared with the same design in combination with a KA surgical technique [1], highlighting the role of the alignment in TKA kinematics.
The current study also showed that a final HKA alignment ± 3° might play a minor role in postoperative knee kinematics. In fact, no statistically significant differences in final HKA alignment were found between uKA and simplified KA cohorts, suggesting that the statistical differences between patients in those cohorts were mainly due to the different balancing techniques. On this topic, Vendittoli et al. [20] showed that 51% of knees could be treated indiscriminately with a uKA [9] or restricted-KA surgical technique and had a final HKA ± 5°.
Another interesting finding of the current study was the ROM determined in the contro-lateral, healthy knee. In both cohorts (uKA and simplified KA), the healthy knee ROM during the stance and swing phases of gait was similar to the surgical knee. This finding confirmed previous reports [21] showing a “symmetrical gait” between the surgical and non-surgical knee in patients who underwent TKA. The implementation of these compensatory strategies in the non-operated side may subsequently result in altered joint loading and progression of OA in the non-operated knee.
The current study has several limitations. First, this is a single institution study analyzing three small cohorts of patients and the conclusions of this study may not apply to larger cohorts. Second, two different medially-stabilized designs were used in this study. This was done because of the lack of availability of a robotic system for the uKA knee system used in the study (GMK Sphere, Medacta, Castel San Pietro, Switzerland). Different designs with different geometries may result in different findings. Third, a clear definition of an optimal intercompartmental gap difference in flexion as well as in extension has not been established yet and the authors proposed their own. Fourth, the surgery was performed under regional anesthesia using a tourniquet, and the resulting kinematics could be altered. However, it has been reported that this measurement system had satisfactory reproducibility [22]. Finally, detailed clinical outcomes have not been reported but all TKA patients had a score > 80 on the Knee Society Clinical Score scale.
Conclusion
In summary, patients with a slight increase in the lateral laxity, in extension as well as in flexion, showed closer to normal knee kinematics. This study, one more time, showed that modern surgical techniques, improved enabling technologies, and new-generation implant designs cannot inherently reproduce normal knee kinematics following TKA. However, the current study was the first to define slightly asymmetric targets during intraoperative knee balancing with the help of advanced technologies: the clinical benefit of this robotic-assisted, surgical approach needs to be proved by further studies.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Watanabe M, Kuriyama S, Nakamura S, Nishitani K, Tanaka Y, Sekiguchi K, Ito H, Matsuda S. Abnormal knee kinematics caused by mechanical alignment in symmetric bicruciate-retaining total knee arthroplasty are alleviated by kinematic alignment. Knee. 2020;27(5):1385–95. (Epub 2020 Aug 15).
Dennis DA. Measured resection: an outdated technique in total knee arthroplasty. Orthopedics. 2008;31(9):940, 943–4.
Daines BK, Dennis DA. Gap balancing vs. measured resection technique in total knee arthroplasty. Clin Orthop Surg. 2014;6(1):1–8. (Epub 2014 Feb 14).
Freeman MA, Pinskerova V. The movement of the normal tibio-femoral joint. J Biomech. 2005;38(2):197–208.
Risitano S, Indelli PF. Is “symmetric” gap balancing still the gold standard in primary total knee arthroplasty? Ann Transl Med. 2017;5(16):325.
Meneghini RM, Deckard ER, Warth LC. Optimizing asymmetric native knee flexion gap balance promotes superior outcomes in primary total knee arthroplasty. J Am Acad Orthop Surg. 2023;31(19):e834–44. (Epub 2023 Jun 30).
Vajapey SP, Pettit RJ, Li M, Chen AF, Spitzer AI, Glassman AH. Risk factors for mid-flexion instability after total knee arthroplasty: a systematic review. J Arthroplasty. 2020;35(10):3046–54. (Epub 2020 May 21).
Valpiana P, Ghirardelli S, Valtanen RS, Risitano S, Iannotti F, Schaller C, Zepeda K, Engl M, Indelli PF. Biomechanical considerations for an easily-restricted robot-assisted kinematic alignment: a surgical technique note. Arthroplasty. 2023;5(1):29.
Howell SM, Hull ML, Nedopil AJ, Rivière C. Caliper-verified kinematically aligned total knee arthroplasty: rationale, targets, accuracy, balancing, implant survival, and outcomes. Instr Course Lect. 2023;72:241–59.
Farrokhi S, Tashman S, Gil AB, Klatt BA, Fitzgerald GK. Are the kinematics of the knee joint altered during the loading response phase of gait in individuals with concurrent knee osteoarthritis and complaints of joint instability? A dynamic stereo X-ray study. Clin Biomech (Bristol, Avon). 2012;27(4):384–9. (Epub 2011 Nov 8).
Rossi SMP, Sangaletti R, Perticarini L, et al. High accuracy of a new robotically assisted technique for total knee arthroplasty: an in vivo study. Knee Surg Sports Traumatol Arthrosc. 2023;31:1153–61.
Winnock de Grave P, Van Criekinge T, Luyckx T, Moreels R, Gunst P, Claeys K. Restoration of the native tibial joint line obliquity in total knee arthroplasty with inverse kinematic alignment does not increase knee adduction moments. Knee Surg Sports Traumatol Arthrosc. 2023;31(11):4692–704. (Epub 2023 Jun 14).
Miller EJ, Pagnano MW, Kaufman KR. Tibiofemoral alignment in posterior stabilized total knee arthroplasty: static alignment does not predict dynamic tibial plateau loading. J Orthop Res. 2014;32:1068–74.
Rivière C, Ollivier M, Girerd D, Argenson JN, Parratte S. Does standing limb alignment after total knee arthroplasty predict dynamic alignment and knee loading during gait? Knee. 2017;24:627–33.
Trepczynski A, Kutzner I, Schütz P, Dymke J, List R, Von Roth P, et al. Tibio-femoral contact force distribution is not the only factor governing pivot location after total knee arthroplasty. Sci Rep. 2019;9:182.
Trepczynski A, Moewis P, Damm P, Schütz P, Dymke J, Hommel H, Taylor WR, Duda GN. Dynamic knee joint line orientation is not predictive of tibio-femoral load distribution during walking. Front Bioeng Biotechnol. 2021;2(9):754715.
Edelstein AI, Wakelin EA, Plaskos C, Suleiman LI. Laxity, balance, and alignment of a simulated kinematic alignment total knee arthroplasty. Arthroplast Today. 2023;18(23):101204.
Koo S, Andriacchi TP. The knee joint center of rotation is predominantly on the lateral side during normal walking. J Biomech. 2008;41(6):1269–73.
Mikashima Y, Harman MK, Coburn J, Hodge WA, Banks SA. In vivo kinematics of an Acl-substituting knee arthroplasty during gait and stair activities. Orthop Proc. 2010;92-B(SUPP_I):120–1.
Vendittoli PA, Martinov S, Blakeney WG. Restricted kinematic alignment, the fundamentals, and clinical applications. Front Surg. 2021;20(8):697020.
Aljehani M, Madara K, Snyder-Mackler L, Christiansen C, Zeni JA Jr. The contralateral knee may not be a valid control for biomechanical outcomes after unilateral total knee arthroplasty. Gait Posture. 2019;70:179–84. (Epub 2019 Mar 8).
Majima T, Sawaguchi N, Kasahara Y, Tomita T, Sugamoto K. Measurements of knee kinematics during TKA surgery using navigation system correlate with postoperative kinematics. Orthopaedic Proc. 2012;94(SUPP_XXV):135–135.
Acknowledgements
The authors thank Karlos Zepeda for the copy editing of the manuscript.
Funding
None.
Author information
Authors and Affiliations
Contributions
P.F.I.: data collection, analysis, manuscript preparation; P.V.: data collection, analysis, manuscript preparation; S.G.: data analysis, manuscript preparation; A.G.S.: manuscript preparation and copy editing in English; G.P.: manuscript preparation; G.A.: manuscript preparation; M.B.: gait analysis execution and data gathering; C.S.: data analysis. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study has been reviewed by the institutional research governance board and deemed not to require approval from a research ethics committee.
Consent for publication
The authors read and approved the final manuscript, giving consent for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Valpiana, P., Salvi, A.G., Ghirardelli, S. et al. Asymmetric gap balancing improves knee kinematic following primary total knee arthroplasty. Arthroplasty 6, 29 (2024). https://doi.org/10.1186/s42836-024-00243-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42836-024-00243-5