
Abstract
Background
Modern cementless total knee arthroplasty (TKA) fixation has shown comparable long-term outcomes to cemented TKA, but the trend of using cementless TKA remains unclear. This study aimed to investigate the trend of using cementless TKA based on a national database.
Methods
The patients undergoing cementless TKA between 2015 and 2021 were retrospectively extracted from the PearlDiver (Mariner dataset) Database. The annual percentage of cementless TKA was calculated using the following formula: annual number of cementless TKA/annual number of TKA. The trend of the number of patients undergoing cementless TKA was created according to a compounded annual growth rate (CAGR) calculation of annual percentages. Patient age, comorbidity, region, insurance type, etc., were also investigated. Differences were considered statistically significant at P < 0.05.
Results
Of the 574,848 patients who received TKA, 546,731 (95%) underwent cemented fixation and 28,117 (5%) underwent cementless fixation. From 2015 to 2021, the use of cementless TKA significantly increased by 242% from 3 to 9% (compounded annual growth rate (CAGR): + 20%; P < 0.05). From 2015 to 2021, we observed a CAGR greater than 15% for all age groups (< 50, 50–59, 60–69, 70–74, 75 +), insurance types (cash, commercial, government, Medicare, Medicaid), regions (Midwest, Northeast, South, West), sex (male and female), and certain comorbidities (osteoporosis, diabetes mellitus, tobacco use, underweight (BMI < 18.5), rheumatoid arthritis) (P < 0.05 for all). Patients undergoing TKA with chronic kidney disease, prior fragility fractures, and dementia demonstrated a CAGR of + 9%–13% from 2015 to 2021 (P < 0.05).
Conclusion
From 2015 to 2021, the use of cementless TKA saw a dramatic increase in all patient populations. However, there is still no consensus on when to cement and in whom. Clinical practice guidelines are needed to ensure safe and effective use of cementless fixation.
Similar content being viewed by others


Introduction
Modern innovation in highly porous cementless implants for total knee arthroplasty has reinvigorated the decades-long debate amongst arthroplasty surgeons: to cement or not to cement [1,2,3]? Although cementless fixation is experiencing a resurgence in popularity due to its improved survivorship, the trend of the number of patients undergoing cementless TKA remains unclear.
Historically, cemented total knee arthroplasty has been the preferred fixation method in most patients, specifically those at high-risk for early implant loosening, such as those with osteoporotic peri-implant bone stock [4, 5]. In addition, the contraindications of cementless TKA included old age (≥ 65 years) and poor bone health. Thus, cemented TKA had remained the gold standard for most patients.
However, fixation failure due to inadequate durability of the bone-cement interface is a major concern, especially in younger patients [6,7,8]. The three-dimensionally-printed cancellous bone surfaces of cementless designs may provide more physiological and durable fixation [9]. The early studies suggested excellent 5-year survivorship of cementless implants comparable to cemented implants [10,11,12]. The increasing demand for TKA in younger patients prompts a renewed interest in cementless fixation [13]. With the development of new materials and technologies, the previously established contraindications may be less absolute and more flexible [14, 15]. The purpose of this retrospective study was to analyze the trend of the number of patients undergoing cementless TKA based on a national database between 2015 and 2021. We also analyzed cementless TKA regarding patient age, comorbidity, region, insurance type, etc. We hypothesized that there would be a significantly increasing use of cementless TKA.
Materials and methods
Database
We retrospectively reviewed the PearlDiver (Mariner dataset) Database (10435 Marble Creek Circle Colorado Springs, CO 80908, USA). Using the Current Procedure Terminology (CPT) and International Classification of Disease (ICD) 10 billing codes, we identified patients undergoing cementless and cemented TKA from 2015 to 2021. As PearlDiver only releases de-identified patient information to users, the study was deemed exempt from Institutional Review Board approval.
Patient selection
The inclusion criteria of the study included patients between 2015 and 2021 receiving (1) primary cemented TKA (unilateral and bilateral); or (2) primary cementless TKA (unilateral and bilateral); and at least a 2-year follow-up. The exclusion criteria were (1) patients with fracture indications (to only include elective TKA patients); (2) patients with malignancy indications (to only include elective TKA patients) (Fig. 1). In total, 574,848 patients were included in this study with 546,731 (95%) undergoing cemented TKA and 28,117 (5%) undergoing cementless TKA. Table 1 shows the univariate demographics and comorbidities of patients who underwent cemented and cementless TKA.

Flow diagram showing inclusion and exclusion criteria
Observation items
We observed patient age (<50, 50–59, 60–69, 70–74, and ≥75), sex (female or male), the Charlson Comorbidity Index (CCI: 0, 1, 2, 3 +), insurance type (cash, Medicare, Medicaid, commercial, Non-Medicare/Medicaid Government Insurance), region (North East, Midwest, South, West), the preoperative diagnosis of osteoporosis, a prior fragility fracture, diabetes mellitus, tobacco use, underweight (body mass index < 18.5), rheumatoid arthritis, dementia, chronic kidney disease, and prior treatment for osteoporosis.
We calculated an annual percentage of cementless TKA using the following formula: annual number of cementless TKA/annual number of TKA. The trend was created according to the annual percentages. We also observed the percentages of cementless TKA in terms of patient age and risk factors.
Statistical analysis
Compounded annual growth rate was used to determine the rate of change of cementless use from 2015 to 2021 based on the following equation: Compounded annual growth rate = (Y2 value/Y1 value)1/(Y2 – Y1) – 1, where Y1 is the first year of the analysis and Y2 is the final year. Compounded annual growth rate (CAGR) is a validated metric of annual change that is commonly used to analyze trends due to its ability to reduce the impact of short-term fluctuations on overall trends [17, 18]. Linear regression analysis was used to observe significant differences in the overall use of cementless TKA as well as the change in patient factors of patients receiving a cementless TKA. P values were recorded to show whether there was a significant difference in overall use as well as patient factors, with a P value less than 0.05 being statistically significant. With regard to patient selection analysis of those who underwent cemented and cementless TKA, a logistic regression analysis was conducted, reporting the odds ratio (OR), 95% confidence interval (95% CI), and the P-value for each variable. All statistical analyses were conducted using R Software (Vienna, Austria) provided by the PearlDiver Database.
Results
Patient demographics (univariate analysis)
In total, 574,848 patients were included in this study, with 546,731 (95%) undergoing cemented TKA and 28,117 (5%) undergoing cementless TKA. On univariate analysis, patients undergoing cementless TKA were younger (64.76 ± 9.4 versus 66.86 ± 9.4 years old; P < 0.001), more likely to be men (44% vs. 38%; P < 0.001), and less likely to have osteoporosis (5% vs. 7%; P < 0.001), dementia (3% vs. 5%; P < 0.001), and chronic kidney disease (0.8% vs. 2%; P < 0.001) when compared to cemented TKA patients (Table 1). The average CCI of cementless TKA patients was significantly lower than the average CCI of cemented TKA patients (1.97 ± 2.3 vs. 2.10 ± ; P < 0.001) (Table 1).
Factors associated with cemented vs. cementless total knee arthroplasty (multivariate analysis)
Following multivariable regression analysis, an age-dependent relationship was observed in those who underwent cementless when compared to cemented TKA. With patients younger than 55 as the reference, those aged 55 to 64 (Odds ratio: 0.90; 95% Confidence interval: 0.87–0.94), 65 to 74 (Odds ratio: 0.73; 95% Confidence interval: 0.70–0.75) and 75 + (Odds ratio [OR]: 0.57; 95% Confidence interval [CI]: 0.50–0.60) were significantly less likely to undergo cementless TKA (P < 0.001 for all; Table 2). Female patients (OR: 0.76 times; 95% CI: 0.74–0.78), those with osteoporosis (OR: 0.86; 95% CI: 0.81–0.91), those with dementia (OR: 0.84; 95% CI: 0.79–0.90), and those with chronic kidney disease (OR: 0.73; 95% CI: 0.64–0.83) were also significantly less likely to undergo cementless TKA (P < 0.001 for all; Table 2).
Trends in use of cementless TKA
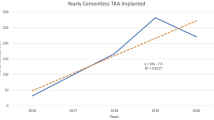
From 2015 to 2021, the use of cementless TKA significantly increased by 242% from 3 to 9% (compounded annual growth rate [CAGR]: +20%; P < 0.001; Fig. 2; Table 3). Regarding age, the use of cementless TKA significantly increased for those aged less than 50 (CAGR: +22%, P = 0.004), 50–59 (CAGR: +22%, P = 0.004), 60–69 (CAGR: +25%, P = 0.006), 70–74 (CAGR: +24%, P = 0.005), and 75 + (CAGR: +16%; P = 0.006; Table 3). The use of cementless fixation significantly increased in men (CAGR: +23%; P = 0.005) and women (CAGR: +20%; P = 0.005; Table 3).

The Trend of the number of patients undergoing cementless total knee arthroplasty between 2015 and 2021
Regarding comorbidities, the use of cementless fixation significantly increased in those with a CCI of 0 (CAGR: +19%; P = 0.004), 1 (CAGR: +22%; P = 0.005), 2 (CAGR: +25%; P = 0.007), and 3 + (CAGR: +19%; P = 0.004; Table 3). The use also increased in those with prior treatment for osteoporosis (CAGR: +13%; P = 0.002), those with a prior fragility fracture (CAGR: +13%; P = 0.003), those with tobacco use (CAGR: +26%; P = 0.009), those who are underweight (CAGR: +27%; P = 0.004), and those with a diagnosis of osteoporosis (CAGR: +17%; P = 0.004), diabetes mellitus (CAGR: +19%; P = 0.004), rheumatoid arthritis (CAGR: +19%; P = 0.004), dementia (CAGR: +11%; P = 0.001), and chronic kidney disease (CAGR: +9%; P = 0.001; Table 3).
Regarding insurance type, the use of cementless fixation increased in those who paid without insurance (CAGR: +27%; P = 0.004), those with commercial insurance (CAGR: +21%; P = 0.004), those with Medicaid insurance (CAGR: +19%; P = 0.008), those with Medicare insurance (CAGR: +23%; P = 0.007), and those with non-Medicaid/Medicare insurance (CAGR: +22%; P = 0.008; Table 3).
Discussion
Our study showed an increase in the use of cementless TKA from 3% in 2015 to 9% in 2021. The increased use of cementless TKA persisted in all age ranges (<50, 50–59, 60–69, 70–74, and ≥75), sexes (female and male), CCI (0, 1, 2, and 3 +), insurance types (cash, Medicare, Medicaid, commercial, Non-Medicare/Medicaid Government Insurance), regions (North East, Midwest, South, West), and comorbidities (preoperative diagnosis of osteoporosis, prior fragility fractures, diabetes mellitus, tobacco use, underweight (BMI < 18.5), rheumatoid arthritis, dementia, chronic kidney disease, and prior treatment for osteoporosis).
This increased use is congruent with those reported in national registries. Within this same period, the American Joint Replacement Registry (AJRR) noted an increased use of cementless TKA from 4% in 2015 to 15% in 2021 [16]. Internationally, both the Swedish Knee Arthroplasty Registry and National Joint Registry (covering England, Wales, Northern Ireland, and the Isle of Man and Guernsey) also reported a significantly increased use of cementless fixation, with 8% and 5% of TKA using cementless fixation in 2021, respectively [19, 20]. The higher 2021 reported cementless use in AJRR of 15% when compared to our 9% is most likely due to surgeon-specific factors. Although AJRR is the largest registry of hip and knee replacements in the United States, a higher proportion of contributing surgeons are Hip and Knee Reconstruction fellowship trained orthopaedic surgeons from academic centers when compared to the general population of orthopaedic surgeons [21]. As the PearlDiver database is not a registry where physicians contribute their data but rather a national insurance claims database, it is likely to capture a more generalizable utilization rate of cementless fixation among TKAs performed in the United States.
Consistent with prior findings, this study found younger patients and men were more likely to undergo cementless TKA [10, 22,23,24,25]; whereas patients with osteoporosis, chronic kidney disease, and dementia were more likely to undergo cemented TKA [26, 27]. Surgeons’ decision-making regarding fixation modality is highly correlated with bone health. Osteoporosis continues to be a major risk factor for cementless TKA implant failure due to the inherent compromised bone stock and poor potential for bone ingrowth [28, 29]. Therefore, cementation is preferred in this patient population to minimize the risk of periprosthetic fracture [30]. As bone quality is negatively correlated with age, surgeons are more likely to perform cemented TKAs in elderly patients. In addition to osteoporosis, chronic kidney disease (CKD) is highly correlated with postoperative fracture and osteoporosis, prompting surgeons to use cemented fixation [31].
Although younger male patients, without a history of osteoporosis, chronic kidney disease, and dementia are more likely to undergo cementless fixation, our study showed that the increased use of this fixation type still significantly increased in all patient populations assessed from 2015 to 2021. We speculate that the increased use of cementless TKA could be attributed to its cost-effectiveness and lower postoperative complications while maintaining comparable implant survivorship when compared to cemented TKA. In a recent randomized control trial by Tanariyakul et al., cementless TKA was found to have similar functional outcomes and recovery patterns to cemented TKA at a 2-year follow-up [32]. Other randomized control trials have found little to no difference in implant migration or survivorship and clinical, radiographic, or patient-reported outcomes between cementless and cemented TKA components at a 5-, 6-, and 10-year follow-up [1, 3, 33,34,35,36,37]. In a database study by Stavrakis et al. done in 2022, a large cohort of 6,415 cementless TKA patients from 2015 to 2019 was found to have no difference in aseptic loosening when compared with a matched cemented TKA cohort at 90-day, 1-, and 2-year follow-up [27]. However, the authors did find a greater rate of periprosthetic joint infections and fractures in the cementless TKA cohort. From mid- to long-term follow-up, implant survivorship for cementless TKA ranged from 100% at 6-years to 96–99.6% at 10-years, indicating an excellent prognosis that is similar to cemented TKA [34,35,36]. A meta-analysis by Zhou et al. found no significant differences in implant survivorship and clinical outcomes between both fixation modalities [38]. Prasad et al.’s more recent meta-analysis in 2020 confirmed these findings, showing cementless fixation to be as efficacious as cemented one with an average of 8-year follow-up [39]. Although similarly efficacious, modern cementless fixation may be more cost-effective than cemented ones [40, 41]. While the cost of cementless implants is generally higher than cemented ones, the cost of implanting, considering the cost of cement and operative time, was found to be lower with cementless fixation [40].
As cementless fixation historically has been indicated in younger patients, it is unsurprising that the increased use of cementless fixation is congruent in the younger population. However, our analysis also observed a significantly increased use in the elderly. The emergence of newer bone-preserving implant designs and highly porous metals has permitted the expansion of cementless fixation to older patients [10, 22, 24]. With an average of 4-year follow-up, Goh et al. were among the first to recognize that elderly patients with cementless implants achieve similar patient-reported outcomes and survivorship to those with cemented implants in TKA, explaining the increased use in this patient population [14]. As these implants have been shown to be safe in older patients with most likely lower-quality bone, it stands to reason that this safety profile is congruent in patients with osteoporosis and those at high-risk, as shown by our study’s increased use in these patients. However, long-term implant survivability in these sub-populations has yet to be observed, warranting future works. Additionally, our study found an increased use of cementless fixation regardless of CCI score. CCI is mostly based on medical comorbidities, such as coronary artery diseases, with many not related to bone health. The expansion to “sicker” patients suggests that surgeons may be more comfortable performing this fixation, sticking to bone health factors as their main determinant of fixation type. Lastly, as there are no strict utilization guidelines, there is always the potential for disparities in access. Reassuringly, our results showed increased use of cementless fixation in all insurance types, a known surrogate for social deprivation [42].
The results of this study should be interpreted with respect to its limitations. First, the study was limited to the use of retrospective patient information. We could only report on trends observed and must practice caution in overinterpreting significant results as causation. Second, our analysis was limited to variables provided by the database and was unable to look at surgeon-, hospital-, or implant-specific factors. Third, participating institutions in this nationwide database may have different methods or practices in reporting variables and thus there was the risk of selection biases. Lastly, although we were able to observe that certain patient populations were more or less likely to undergo cementless fixation, we are unable to extrapolate in which patient population cementless fixation should be performed. We observed a universally increased use of cementless TKA across many patient demographics, but surgeons should be aware of some recently reported failures of common cementless implants and avoid their use in high-risk patients [43, 44]. As modern day cementless implants and coatings continue to revolutionize total knee arthroplasty, future studies and clinical practice guidelines should be updated to ensure safe and effective use of cementless fixation.
Conclusion
From 2015 to 2021, the usage of cementless TKA witnessed a dramatic increase in all patient populations, underscoring an almost universal increase in popularity with limited clarity on when to cement and in whom. Future prospective studies as well as clinical practice guidelines should explore various patient populations to uncover who should undergo cementless fixation based on long-term implant survivorship and incidence of postoperative complications.
Availability of data and materials
The data that support the findings of this study are available from the PearlDiver database, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the PearlDiver database.
Abbreviations
- TKA:
-
Total Knee Arthroplasty
- CCI:
-
Charlson Comorbidity Index
- AJRR:
-
American Joint Replacement Registry
- CKD:
-
Chronic Kidney Disease
- CAGR:
-
Compounded Annual Growth Rate
- OR:
-
Odds Ratio
- CI:
-
Confidence Interval
References
Nam D, Lawrie CM, Salih R, Nahhas CR, Barrack RL, Nunley RM. Cemented versus cementless total knee arthroplasty of the same modern design: a prospective, randomized trial. J Bone Joint Surg Am. 2019;101(13):1185–92. https://doi.org/10.2106/JBJS.18.01162.
Miller AJ, Stimac JD, Smith LS, Feher AW, Yakkanti MR, Malkani AL. Results of cemented vs cementless primary total knee arthroplasty using the same implant design. J Arthroplasty. 2018;33(4):1089–93. https://doi.org/10.1016/j.arth.2017.11.048.
Fricka KB, McAsey CJ, Sritulanondha S. To cement or not? Five-year results of a prospective, randomized study comparing cemented vs cementless total knee arthroplasty. J Arthroplasty. 2019;34(7S):S183–7. https://doi.org/10.1016/j.arth.2019.02.024.
Wilson DA, Richardson G, Hennigar AW, Dunbar MJ. Continued stabilization of trabecular metal tibial monoblock total knee arthroplasty components at 5 years-measured with radiostereometric analysis. Acta Orthop. 2012;83(1):36–40. https://doi.org/10.3109/17453674.2011.645196.
Li MG, Nilsson KG. The effect of the preoperative bone quality on the fixation of the tibial component in total knee arthroplasty. J Arthroplasty. 2000;15(6):744–53. https://doi.org/10.1054/arth.2000.6617.
Kandahari AM, Yang X, Laroche KA, Dighe AS, Pan D, Cui Q. A review of UHMWPE wear-induced osteolysis: the role for early detection of the immune response. Bone Res. 2016;4:16014.
Wang ML, Sharkey PF, Tuan RS. Particle bioreactivity and wear- mediated osteolysis. J Arthroplasty. 2004;19(08):1028–38.
Gallo J, Goodman SB, Konttinen YT, Wimmer MA, Holinka M. Osteolysis around total knee arthroplasty: a review of pathogenetic mechanisms. Acta Biomater. 2013;9(09):8046–58.
Kamath AF, Siddiqi A, Malkani AL, Krebs VE. Cementless fixation in primary total knee arthroplasty: historical perspective to contemporary application. J Am Acad Orthop Surg. 2021;29(8):e363–79. https://doi.org/10.5435/JAAOS-D-20-00569.
Mont MA, Gwam C, Newman JM, et al. Outcomes of a newer-generation cementless total knee arthroplasty design in patients less than 50 years of age. Ann Transl Med. 2017;5(Suppl 3):S24. https://doi.org/10.21037/atm.2017.08.20.
Kamath AF, Lee GC, Sheth NP, Nelson CL, Garino JP, Israelite CL. Prospective results of uncemented tantalum monoblock tibia in total knee arthroplasty: minimum 5-year follow-up in patients younger than 55 years. J Arthroplasty. 2011;26(8):1390–5. https://doi.org/10.1016/j.arth.2011.06.030.
DeFrancesco CJ, Canseco JA, Nelson CL, Israelite CL, Kamath AF. Uncemented tantalum monoblock tibial fixation for total knee arthroplasty in patients less than 60 years of age: mean 10-year follow-up. J Bone Joint Surg Am. 2018;100(10):865–70. https://doi.org/10.2106/JBJS.17.00724.
Gwam CU, George NE, Etcheson JI, Rosas S, Plate JF, Delanois RE. Cementless versus cemented fixation in total knee arthroplasty: usage, costs, and complications during the inpatient period. J Knee Surg. 2019;32(11):1081–7. https://doi.org/10.1055/s-0038-1675413.
Goh GS, Fillingham YA, Ong CB, Krueger CA, Courtney PM, Hozack WJ. Redefining indications for modern cementless total knee arthroplasty: clinical outcomes and survivorship in patients >75 years old. J Arthroplasty. 2022;37(3):476-481.e1. https://doi.org/10.1016/j.arth.2021.11.031.
Newman JM, Khlopas A, Chughtai M, et al. Cementless total knee arthroplasty in patients older than 75 years. J Knee Surg. 2017;30(9):930–5. https://doi.org/10.1055/s-0037-1599253.
American Joint Replacement Registry (AJRR): 2021 Annual Report. Rosemont, IL: American Academy of Orthopaedic Surgeons (AAOS), 2021.
Lopez CD, et al. Recent trends in medicare utilization and reimbursement for lumbar spine fusion and discectomy procedures. Spine J Off J North Am Spine Soc. 2020;20:1586–94.
Eltorai AEM, et al. Trends in medicare reimbursement for orthopedic procedures: 2000 to 2016. Orthopedics. 2018;41:95–102.
National Joint Registry. National Joint Registry 18th Annual Report. https://www.njrcentre.org.uk/njrcentre/Reports-Publications-and Minutes/Annual-reports. Accessed Oct 5, 2021.
Update to Swedish Knee Arthroplasty Register. Swedish Knee Arthroplasty Register 2020 Annual Report. https://www.myknee.se/pdf/SVK_2020_Eng_1.0.pdf. Accessed Oct 5, 2021.
Hallstrom BR, Hughes RE, Huddleston JI 3rd. State-Based and National U.S. Registries: The Michigan Arthroplasty Registry Collaborative Quality Initiative (MARCQI), California Joint Replacement Registry (CJRR), and American Joint Replacement Registry (AJRR). J Bone Joint Surg Am. 2022;104(Suppl 3):18–22. https://doi.org/10.2106/JBJS.22.00564
Chen C, Li R. Cementless versus cemented total knee arthroplasty in young patients: a meta-analysis of randomized controlled trials. J Orthop Surg Res. 2019;14(1):262. https://doi.org/10.1186/s13018-019-1293-8. Published 2019 Aug 19.
Franceschetti E, Torre G, Palumbo A, et al. No difference between cemented and cementless total knee arthroplasty in young patients: a review of the evidence. Knee Surg Sports Traumatol Arthrosc. 2017;25(6):1749–56. https://doi.org/10.1007/s00167-017-4519-5.
Kim YH, Park JW, Jang YS. The 22 to 25-year survival of cemented and cementless total knee arthroplasty in young patients. J Arthroplasty. 2021;36(2):566–72. https://doi.org/10.1016/j.arth.2020.08.001.
Sheridan GA, Cassidy RS, McKee C, Hughes I, Hill JC, Beverland DE. Survivorship of 500 Cementless Total Knee Arthroplasties in Patients under 55 Years of Age [published online ahead of print, 2022 Oct 26]. J Arthroplasty. 2022;S0883–5403(22)00972-X. doi:https://doi.org/10.1016/j.arth.2022.10.035
Walsh CP, Han S, Canham CD, Gonzalez JL, Noble P, Incavo SJ. Total knee arthroplasty in the osteoporotic tibia: a biomechanical evaluation of the role of stem extensions and cementing techniques. J Am Acad Orthop Surg. 2019;27(10):370–4. https://doi.org/10.5435/JAAOS-D-17-00736.
Stavrakis A, Arshi A, Chiou D, Hsiue P, Horneff JG 3rd, Photopoulos C. Cemented versus noncemented total knee arthroplasty outcomes. J Am Acad Orthop Surg. 2022;30(6):273–80. https://doi.org/10.5435/JAAOS-D-21-00353.
Bernatz JT, Krueger DC, Squire MW, Illgen RL 2nd, Binkley NC, Anderson PA. Unrecognized osteoporosis is common in patients with a well-functioning total knee arthroplasty. J Arthroplasty. 2019;34(10):2347–50. https://doi.org/10.1016/j.arth.2019.05.041.
Bernatz JT, Brooks AE, Squire MW, Illgen RI 2nd, Binkley NC, Anderson PA. Osteoporosis is common and undertreated prior to total joint arthroplasty. J Arthroplasty. 2019;34(7):1347–53. https://doi.org/10.1016/j.arth.2019.03.044.
Gandhi R, Tsvetkov D, Davey JR, Mahomed NN. Survival and clinical function of cemented and uncemented prostheses in total knee replacement: a meta-analysis. J Bone Joint Surg Br. 2009;91(7):889–95. https://doi.org/10.1302/0301-620X.91B7.21702.
Lips P, Goldsmith D, de Jongh R. Vitamin D and osteoporosis in chronic kidney disease. J Nephrol. 2017;30(5):671–5. https://doi.org/10.1007/s40620-017-0430-x.
Tanariyakul Y, Kanitnate S, Tammachote N. Cementless and cemented total knee arthroplasties have similar outcomes but cementless patellar component migration was observed in a paired randomized control trial. J Arthroplasty. 2023;S0883–5403(23):01100–2. https://doi.org/10.1016/j.arth.2023.10.055.
van der Lelij TJN, Marang-van de Mheen PJ, Kaptein BL, Toksvig-Larsen S, Nelissen RGHH. Continued Stabilization of a Cementless 3D-Printed Total Knee Arthroplasty: Five-Year Results of a Randomized Controlled Trial Using Radiostereometric Analysis. J Bone Joint Surg Am. 2023;105(21):1686–1694. doi:https://doi.org/10.2106/JBJS.23.00221
Hannon CP, Salih R, Barrack RL, Nunley RM. Cementless versus cemented total knee arthroplasty: concise midterm results of a prospective randomized controlled trial. J Bone Joint Surg Am. 2023;105(18):1430–4. https://doi.org/10.2106/JBJS.23.00161.
Awwad GEH, Ahedi H, Angadi D, Kandhari V, Coolican MRJ. A prospective randomised controlled trial of cemented and uncemented tibial baseplates: functional and radiological outcomes. Arch Orthop Trauma Surg. 2023;143(9):5891–9. https://doi.org/10.1007/s00402-023-04831-z.
Gibon E, Lewallen DG, Larson DR, Stuart MJ, Pagnano MW, Abdel MP, John N. Insall award: randomized clinical trial of cementless versus cemented tibial components: durable and reliable at a mean 10-years follow-up. J Arthroplasty. 2023;38(6S):S14–20. https://doi.org/10.1016/j.arth.2023.03.015.
Peddada KV, Delman CM, Holland CT, Meehan JP, Lum ZC. Tantalum Cementless Versus Cemented Total Knee Arthroplasty: A Meta-analysis of Level 1 Studies. J Am Acad Orthop Surg Glob Res Rev. 2023;7(4):e22.00219. https://doi.org/10.5435/JAAOSGlobal-D-22-00219
Zhou K, Yu H, Li J, Wang H, Zhou Z, Pei F. No difference in implant survivorship and clinical outcomes between full-cementless and full-cemented fixation in primary total knee arthroplasty: a systematic review and meta-analysis. Int J Surg. 2018;53:312–9. https://doi.org/10.1016/j.ijsu.2018.04.015.
Prasad AK, Tan JHS, Bedair HS, Dawson-Bowling S, Hanna SA. Cemented vs. cementless fixation in primary total knee arthroplasty: a systematic review and meta-analysis. EFORT Open Rev. 2020;5(11):793–798. doi:https://doi.org/10.1302/2058-5241.5.200030. Published 2020 Nov 13.
Lawrie CM, Schwabe M, Pierce A, Nunley RM, Barrack RL. The cost of implanting a cemented versus cementless total knee arthroplasty. Bone Joint J. 2019;101-B(7_Supple_C):61–63. https://doi.org/10.1302/0301-620X.101B7.BJJ-2018-1470.R1
Yayac M, Harrer S, Hozack WJ, Parvizi J, Courtney PM. The use of cementless components does not significantly increase procedural costs in total knee arthroplasty. J Arthroplasty. 2020;35(2):407–12. https://doi.org/10.1016/j.arth.2019.08.063.
Cheng AL, McDuffie JV, Schuelke MJ, Calfee RP, Prather H, Colditz GA. How should we measure social deprivation in orthopaedic patients? Clin Orthop Relat Res. 2022;480(2):325–39. https://doi.org/10.1097/CORR.0000000000002044.
Fokter SK, Gubeljak N, Punzón-Quijorna E, et al. Total knee replacement with an uncemented porous tantalum tibia component: a failure analysis. Materials (Basel). 2022;15(7):2575. https://doi.org/10.3390/ma15072575.Published2022Mar31.
Scully WF, Deren ME, Bloomfield MR. Catastrophic tibial baseplate failure of a modern cementless total knee arthroplasty implant. Arthroplast Today. 2019;5(4):446–52. https://doi.org/10.1016/j.artd.2019.09.002.Published2019Oct16.
Acknowledgements
Not applicable.
Funding
This study was funded by the Gildenhorn Institute for Bone and Joint Health at Sibley Memorial Hospital and Johns Hopkins Medicine, USA.
Author information
Authors and Affiliations
Contributions
A.R.A., S.R., and A.U. created the research question. A.R.A. conducted the data analysis. E.V.K. and A.G. wrote the manuscript. G.J.G., S.C.T., G.S., A.U., S.R. edited the manuscript. A.U. and S.R. provided supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study received institutional review board approval. Consent was waived due to the retrospective nature of this study.
Consent for publication
No individual patient data were obtained and thus no consent was needed for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Agarwal, A.R., Kuyl, EV., Gu, A. et al. Trend of using cementless total knee arthroplasty: a nationwide analysis from 2015 to 2021. Arthroplasty 6, 24 (2024). https://doi.org/10.1186/s42836-024-00241-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42836-024-00241-7