
Abstract
Background
Autoimmune encephalitides with neural and glial antibodies have become an attractive field in neurology because the antibodies are syndrome-specific, explain the pathogenesis, indicate the likelihood of an underlying tumor, and often predict a good response to immunotherapy. The relevance and the management of antibody-associated encephalitides in the pediatric age group are to be discussed.
Main body
Subacutely evolving, complex neuropsychiatric conditions that are otherwise unexplained should raise the suspicion of autoimmune encephalitis. Determination of autoantibodies is the key diagnostic step. It is recommended to study cerebrospinal fluid and serum in parallel to yield highest diagnostic sensitivity and specificity. The most frequently found antibodies are those against the N-methyl-D-asparate receptor, an antigen on the neural cell surface. The second most frequent antibody is directed against glutamic acid decarboxylase 65 kDa, an intracellular protein, often found in chronic conditions with questionable inflammatory activity. Immunotherapy is the mainstay of treatment in autoimmune encephalitides. Steroids, apheresis and intravenous immunoglobulin are first-line interventions. Rituximab or cyclophosphamide are given as second-line treatments. Patients with surface antibodies usually respond well to immunotherapy whereas cases with antibodies against intracellular antigens most often do not.
Conclusion
With few exceptions, the experience in adult patients with autoimmune encephalitides can be applied to patients in the pediatric age range.
Similar content being viewed by others


Background
The discovery of immunoglobulin G (IgG) antibodies against proteins on nerve cell surfaces has been perceived as a major advance and even a breakthrough in neurology. The first specific antibodies that have relevance and validity until to date are those against the N-methyl-D-aspartate receptor (NMDAR) [1]. These were followed by those against leucine-rich glioma inactivated protein 1 (LGI1) [2, 3], contactin-associated protein-2 (CASPR2) [3, 4] and others. These new “surface antibodies” are diagnosed by incubating diluted serum or undiluted (or mildly diluted) cerebrospinal fluid (CSF) with human embryonic kidney (HEK) cells transfected with the antigens of interest [5]. The binding of antibodies is visualized by a secondary anti-human IgG antibody coupled to a dye that can be visualized under the microscope.
The combination of four properties makes these autoantibodies so valuable:
their syndrome specificity,
their pathogenetic explanatory power,
the frequently good treatability of the associated autoimmune central nervous system (CNS) syndromes
the indication of the underlying tumor probability (paraneoplastic syndromes).
Initially, these antibodies were found in adults. It quickly became clear that they also occur in childhood and are important there [6]. For all age groups, it has been shown in recent years that the antibody detection methods have a good sensitivity. Diagnostic problems are mainly related to specificity of antibody diagnostics. For example, the specificity of antibodies of immunoglobulin classes IgA and IgM for neurological syndromes is doubtful. Currently, no diagnoses should be based on the detection of IgA or IgM antibodies [7]. Another issue are minimum antibody titers for meaningful diagnoses. For CASPR2 IgG antibodies, only antibodies at a minimum serum titer level of 1:128 (or antibodies at any titer in the CSF) are specific for the diagnosis of autoimmune encephalitis [8]. The validation and interpretation of positive antibody findings based on clinical presentation is of great importance in order to avoid false-positive findings.
The list of potentially relevant antibodies that is known today may not yet be complete, as the field is still young and there are still reports of new associations from the neuropediatric age range [5]. Recently published clinical diagnostic criteria for autoimmune encephalitides [9] are of great help in identifying candidates for antibody testing and in checking the relevance of an antibody finding. The criteria should, as the authors of the Position paper say in the section “General scope and objectives” say, be used with caution in patients < 5 years of age because clinical presentation may be different in this age range [9].
In addition to autoimmune encephalitis, which primarily affects the gray matter of the CNS, demyelinating diseases can also be elucidated with the help of autoantibodies. Children and adolescents presenting with acute disseminated encephalomyelitis (ADEM), myelitis or optic neuritis often harbor antibodies to the myelin oligodendrocytic glycoprotein (MOG). The most sensitive and specific method to detect these antibodies is the use of live MOG-transfected HEK cells. Such a live cell assay is superior to a commercial fixed cell assay [10]. MOG antibodies predict a good response to immunotherapy [11].
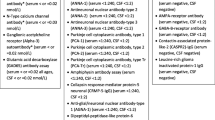
The existing case series show the correlations between syndromic presentations and antibodies given in the upper part of Table 1. For a review of autoimmune encephalitides in the pediatric age range, see [12].
In the following, present knowledge and recent challenges in the diagnostic and therapeutic management of pediatric patients with (suspected) autoimmune encephalitis are discussed:
Which patients should be evaluated regarding a potential autoimmune encephalitis?
How to do an appropriate work-up of such patients? How frequent are which antibodies in the pediatric population?
How to treat patients with the diagnosis of autoimmune encephalitis?
Patients suspicious for autoimmune encephalitis
A key feature of autoimmune encephalitides are the subacute evolution of otherwise uncommon combinations of neurological, cognitive and psychiatric symptoms. The most important paraclinical features are encephalitic magnetic resonance imaging (MRI) lesions or an inflammatory CSF. The “Graus criteria” [9] make use of these features in their introductory category of “possible autoimmune encephalitis” (Table 2). This useful definition developed within adult neurology can usually be applicated to adolescents but is not always fully adequate in children < 5 years of age, because their presentation may differ: Some young cases present without the full spectrum of symptoms (so that the aspect of the above-mentioned “uncommon symptom combination” is not evident); in other instances, the dominant features are not observed to adults (e.g. the massive arterial hypertension in young children with Morvan syndrome and CASPR2 antibodies [13]). It therefore remains a challenge to clinical experience whom to further evaluate for suspected autoimmune encephalitis.
Work-up of children and adolescents with suspected autoimmune encephalitis
MRI and CSF diagnostics are indispensable in children and adolescents with suspected autoimmune encephalitis. On the one side, they help identifying differential diagnoses (e.g., infectious encephalitides), on the other hand, they may strengthen the suspicion (e.g., by demonstrating the typical bilateral mediotemporal T2/FLAIR signal increase of limbic encephalitis or identifying autoantibodies in CSF, which is crucial for NMDAR antibodies). The central diagnostic step is the test for neural antibodies. In most labs, this is today done by means of a panel diagnostic. “Biochips” containing several fields with differently transfected HEK cells permit testing for a broad range of surface antibody reactivities in one run [14]. In addition, immunoblots containing onconeural antigens are applied. The reason is that pediatric patients may occasionally harbor onconeural antibodies, e.g. Hu antibodies in the presence of a neuroblastoma [15]. Ideally, a tissue-based assay (usually, a section of rodent brain) is applied in parallel to identify less common or potentially novel antibodies against surface antigens by a neuropil staining [5].
A frequent question is if a serum, a CSF or a serum-CSF-pair investigation is recommended. Reasons for potentially restricting the test materials are the distress for the patients by a lumbar puncture and the lower costs if only one instead of two materials is studied. In recent years, international authorities from different institutions have uniformly recommended the simultaneous testing of CSF and serum in cases of suspected autoimmune encephalitis, see e.g. [16]. The key reason is that in some cases, the antibodies are detectable only in one of the two materials. For example, NMDAR antibodies are not always found in serum [17]; in contrast, LGI1 or MOG antibodies are not always found in the CSF [16, 18]. Exceptions to the general recmmendation to test CSF-serum pairs may be girls with encephalopathy suggesting anti-NMDAR encephalitis or post-herpes autoimmune encephalitis. Both can often be finally diagnosed by testing for NMDAR antibodies in CSF only [19] so that CSF may be sufficient. However, the clinical presentation is often ambiguous, or a patient may have other antibodies in addition to NMDAR antibodies. An example are antibodies against MOG in the case of overlaps of anti-NMDAR encephalitis with demyelinating disorders [20]. Some patients with an encephalitis defined by antibodies against the γ-aminobutyric acid-A receptor (GABAAR) may look like patients with anti-NMDAR encephalitis. They would be detected at best with a delay if initially only an NMDAR antibody test was done. In this situation, the correct antibody would be only identified by using a biochip together with a tissue-based assay. The reason is that GABAAR transfected HEK cells are not yet regularly available as part of the biochips but can be readily suspected on the tissue-based assay and confirmed in a research laboratory.
The frequency of positive results during routine diagnostics in the antibody laboratory in the Epilepsy Center Bethel using a broad panel for neural antibodies from 2011 to 2015 is shown in Fig. 1. Figure 2 depicts the age distribution of the four most common antibodies. An overview (against the NMDAR, LGI1, CASPR2, the AMPAR1/2, the GABABR, the GlyR, GAD65, Hu, Yo, Ri, CV2, amphiphysin, Ma2, and Sox1) over antibodies, and associated syndromes can be found in Table 3.

Frequency of positive results from the testing of 1426 patients < 18 years in the years 2011–2015 in the antibody laboratory of the Epilepsy Center Bethel. For each patient, only the earliest sample(s) were included. Absolute numbers and percentages are indicated in the labels

Age and sex distribution of antibody-positive patients. Males: blue; females: red. The patients with GAD65 antibodies are predominantly female, whereas in the other groups, the relationship is equal, even with NMDAR antibodies (56% female). Only one girl (4% of all patients with NMDAR antibodies) had paraneoplastic disease with an ovarian teratoma. The figures in a recent Chinese pediatric study were: 61% females (N = 54), one case with ovarian teratoma (1.1%) [28]. One pediatric series from the US (N = 32) had different results: The authors found 81% female patients and 25% paraneoplastic cases [25]. One reason seems to be that African-American patients particularly frequently have paraneoplastic anti-NMDAR encephalitis [26]
An additional note is required for MOG antibodies. Two aspects need to be considered here: These antibodies are not reliably detected by fixed cells and require live cell assays for optimal results [10]; therefore, any biochip technique comprising MOG cells would be suboptimal for their detection. Second, MOG antibodies have been traditionally linked with demyelinating disease; there are, however, encephalitic presentations with seizures and neocortical or basal ganglia lesions but no white matter demyelination with high-titer MOG antibodies in adults [21, 22]. It is conceivable that such cases have been underrecognized in the pediatric population so far. One may tentatively suggest MOG antibody serum testing through a live cell assay in cases with one or more seizures plus neocortical or basal ganglia lesions and negative results with neural autoantibodies on the usual biochip panel.
Treatment of children and adolescents with autoimmune encephalitis
Most data exist on the treatment of patients with NMDAR encephalitis. Internationally, there is no difference in the therapeutic approach to children/adolescents and adults [23]. The usual scheme is that of a first-line and a second-line immunotherapy approach as detailed in Table 4. This concept was derived from the retrospective analysis of 105 patients with that disease [24]. In addition to immunotherapy, symptomatic treatments against seizures, agitation, autonomic problems and so on are regularly given; > 40% of patients require intensive care [25,26,27]. Underlying tumors (mostly ovarian teratomata) need to be removed in addition to immunotherapy. The outcome of anti-NMDAR encephalitis is impressively good: 81% live independently 2 years after diagnosis [26]. Very similar results emerged from a pediatric cohort: 84% of patients were said to have had “complete recovery” in a Chinese series [28]. An important observation is that earlier treatment and earlier escalation to second-line treatments are associated with better outcome in children [29]. Authorities recommend escalation to second-line therapy after 10–14 days without significant improvement upon first-line therapy, especially, if the patients are on the intensive care unit [24]. Relapses are not uncommon. The relapse rate in children followed up for 1–5 years was 13.5% [28]. Relapses are usually milder than the initial disease episode and respond even faster to immunological treatment [30].
Recent animal data suggest that NMDAR antibodies in pregnant mothers may cross the placenta and may cause neuropsychiatric disorders in their offspring [31].
From anti-NMDAR encephalitis, the first-line/second-line approach has been extended to the encephalitides with other antibodies [32]. Escalation usually does not need to be done as rapidly as with NMDAR antibodies. It has been recommended to observe the effect for 1 to 2 months before moving on to a second-line intervention [33]. Patients with LGI1 or CASPR2 antibodies usually respond well to immunotherapy [28, 34, 35].
In contrast, antibodies against intracellular antigens – most frequently against glutamic acid decarboxylase 65 kDa (GAD65), rarely against an onconeural antigen -, portend a less favorable outcome. Usually, these patients take a chronic course. The most common scenario is the development of pharmacoresistant focal epilepsy. Fortunately, in many cases, the patients do not chronically deteriorate [36]. There are almost no reports on successful immunological therapies in patients with GAD65 antibodies [37].
An open question is how long one should wait for the effect of full first-line and second-line therapy. A large retrospective series showed an increasing number of improving patients over 2 years. This was the end of the observational period [26]. Later improvements are therefore possible. Recently, agents like tocilizumab or bortezomib have been advocated as third-line therapies, especially for severe anti-NMDAR encephalitis. Support for this comes from case studies [38, 39]. It remains open to discussion how big the influence of those novel agents in the immunological polypharmacy was.
For Bickerstaff encephalitis, a recent review found in the published data a good response to the predominant application of intravenous immunoglobulins (IVIG) followed by steroids and plasma exchange if needed [40]. With MOG-antibodies, therapy is based on better studied conditions like neuromyelitis optica spectrum disease with aquaporin-4 antibodies. One uses corticosteroids, IVIG, immunosuppressants (like mycophenolate mofetil, azathioprine or methotrexate) and rituximab. All these interventions seem associated with a reduction in relapse rate [16].
Summary
Most neuropediatric cases of autoimmune encephalitis harbor NMDAR antibodies in CSF. Cases with other antibodies occur. The frequency of MOG antibodies in pediatric encephalitides remains to be determined; it might be higher than known today. The existing data justify the use of multiparametric testing for neural antibodies at disease onset in serum and CSF with panel diagnostic through biochips. There are no fundamental differences between autoimmune encephalitides in pediatric and adult cases and their management. Neuropediatricians can therefore rely on insights from adult neurology. Therapy follows a first-line (steroids, IVIG, apheresis) and second-line (rituximab, less frequently cyclophosphamide) concept.
Availability of data and materials
Not applicable.
Abbreviations
- ADEM:
-
Acute disseminated encephalomyelitis myelitis
- CASPR2:
-
Contactin-associated protein-2
- CNS:
-
Central nervous system
- CSF:
-
Cerebrospinal fluid
- DNER:
-
Delta/Notch-like EGF-related receptor
- DR2:
-
Dopamine receptor 2
- GABAAR:
-
γ-aminobutyric acid-A receptor
- GABABR:
-
γ-aminobutyric acid-B receptor
- GAD65:
-
Glutamic acid decarboxylase 65 kDa
- GlyR:
-
Glycine receptor
- HEK cells:
-
Human embryonic kidney cells
- IgA, IgG, IgM:
-
Immunoglobulin A, G, M
- IVIG:
-
Intravenous immunoglobulins
- LGI1:
-
Leucine-rich glioma inactivated protein 1
- mGluR:
-
metabotropic glutamate receptor 1
- mGluR5:
-
metabotropic glutamate receptor 5
- MOG:
-
Myelin oligodendrocytic glycoprotein
- MRI:
-
Magnetic resonance imaging
- NMDAR:
-
N-methyl-D-aspartate receptor
References
Dalmau, J., Tüzün, E., Wu, H. Y., Masjuan, J., Rossi, J. E., Voloschin, A., Baehring, J. M., Shimazaki, H., Koide, R., King, D., et al. (2007). Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Annals of Neurology, 61, 25–36.
Lai, M., Huijbers, M. G., Lancaster, E., Graus, F., Bataller, L., Balice-Gordon, R., Cowell, J. K., & Dalmau, J. (2010). Investigation of LGI1 as the antigen in limbic encephalitis previously attributed to potassium channels: a case series. Lancet Neurology, 9, 776–785. https://doi.org/10.1016/S1474-4422(10)70137-X.
Irani, S. R., Alexander, S., Waters, P., Kleopa, K. A., Pettingill, P., Zuliani, L., Peles, E., Buckley, C., Lang, B., & Vincent, A. (2010). Antibodies to Kv1 potassium channel-complex proteins leucine-rich, glioma inactivated 1 protein and contactin-associated protein-2 in limbic encephalitis, Morvan's syndrome and acquired neuromyotonia. Brain, 133, 2734–2748. https://doi.org/10.1093/brain/awq213.
Lancaster, E., Huijbers, M. G., Bar, V., Boronat, A., Wong, A., Martinez-Hernandez, E., Wilson, C., Jacobs, D., Lai, M., Walker, R. W., et al. (2011). Investigations of Caspr2, an autoantigen of encephalitis and neuromyotonia. Annals of Neurology, 69, 303–311. https://doi.org/10.1002/ana.22297.
Bien, C. G. (2019). Diagnosing autoimmune encephalitis based on clinical features and autoantibody findings. Expert Review of Clinical Immunology, 15, 511–527. https://doi.org/10.1080/1744666X.2019.1573676.
Wright, S., Hacohen, Y., Jacobson, L., Agrawal, S., Gupta, R., Philip, S., Smith, M., Lim, M., Wassmer, E., & Vincent, A. (2015). N-methyl-D-aspartate receptor antibody-mediated neurological disease: results of a UK-based surveillance study in children. Archives of Disease in Childhood, 100, 521–526. https://doi.org/10.1136/archdischild-2014-306795.
Hara, M., Martinez-Hernandez, E., Arino, H., Armangue, T., Spatola, M., Petit-Pedrol, M., Saiz, A., Rosenfeld, M. R., Graus, F., & Dalmau, J. (2018). Clinical and pathogenic significance of IgG, IgA, and IgM antibodies against the NMDA receptor. Neurology, 90, e1386–e1394. https://doi.org/10.1212/WNL.0000000000005329.
Bien, C. G., Mirzadjanova, Z., Baumgartner, C., Onugoren, M. D., Grunwald, T., Holtkamp, M., Isenmann, S., Kermer, P., Melzer, N., Naumann, M., et al. (2017). Anti-contactin-associated protein-2 encephalitis: relevance of antibody titres, presentation and outcome. European Journal of Neurology, 24, 175–186. https://doi.org/10.1111/ene.13180.
Graus, F., Titulaer, M. J., Balu, R., Benseler, S., Bien, C. G., Cellucci, T., Cortese, I., Dale, R. C., Gelfand, J. M., Geschwind, M., et al. (2016). A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurology, 15, 391–404. https://doi.org/10.1016/S1474-4422(15)00401-9.
Waters, P. J., Komorowski, L., Woodhall, M., Lederer, S., Majed, M., Fryer, J., Mills, J., Flanagan, E. P., Irani, S. R., Kunchok, A. C., et al. (2019). A multicenter comparison of MOG-IgG cell-based assays. Neurology, 92, e1250–e1255. https://doi.org/10.1212/WNL.0000000000007096.
Hacohen, Y., Wong, Y. Y., Lechner, C., Jurynczyk, M., Wright, S., Konuskan, B., Kalser, J., Poulat, A. L., Maurey, H., Ganelin-Cohen, E., et al. (2018). Disease Course and Treatment Responses in Children With Relapsing Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease. JAMA Neurology. https://doi.org/10.1001/jamaneurol.2017.4601.
Dale, R. C., Gorman, M. P., & Lim, M. (2017). Autoimmune encephalitis in children: clinical phenomenology, therapeutics, and emerging challenges. Current Opinion in Neurology, 30, 334–344. https://doi.org/10.1097/WCO.0000000000000443.
Syrbe, S., Stettner, G. M., Bally, J., Borggraefe, I., Bien, C. I., Ferfoglia, R. I., Huppke, P., Kern, J., Polster, T., Probst-Müller, E., et al. (2019). CASPR2-autoimmunity in children, expanding to mild encephalopathy with hypertension. Neurology in press.
Stöcker, W., Saschenbrecker, S., Rentzsch, K., Komorowski, L., & Probst, C. (2013). Autoantikörperdiagnostik in der Neurologie mittels nativer und rekombinanter Antigensubstrate. Nervenarzt, 84, 471–476. https://doi.org/10.1007/s00115-012-3607-5.
Morales La Madrid, A., Rubin, C. M., Kohrman, M., Pytel, P., & Cohn, S. L. (2012). Opsoclonus-myoclonus and anti-Hu positive limbic encephalitis in a patient with neuroblastoma. Pediatric Blood & Cancer, 58, 472–474. https://doi.org/10.1002/pbc.23131.
Reindl, M., & Waters, P. (2019). Myelin oligodendrocyte glycoprotein antibodies in neurological disease. Nature Reviews. Neurology, 15, 89–102. https://doi.org/10.1038/s41582-018-0112-x.
Gresa-Arribas, N., Titulaer, M. J., Torrents, A., Aguilar, E., McCracken, L., Leypoldt, F., Gleichman, A. J., Balice-Gordon, R., Rosenfeld, M. R., Lynch, D., et al. (2014). Antibody titres at diagnosis and during follow-up of anti-NMDA receptor encephalitis: a retrospective study. Lancet Neurology, 13, 167–177. https://doi.org/10.1016/S1474-4422(13)70282-5.
van Sonderen, A., Roelen, D. L., Stoop, J. A., Verdijk, R. M., Haasnoot, G. W., Thijs, R. D., Wirtz, P. W., Schreurs, M. W., Claas, F. H., Sillevis Smitt, P. A., et al. (2017). Anti-LGI1 encephalitis is strongly associated with HLA-DR7 and HLA-DRB4. Annals of Neurology, 81, 193–198. https://doi.org/10.1002/ana.24858.
Alexopoulos, H., Akrivou, S., Mastroyanni, S., Antonopoulou, M., Dinopoulos, A., Giorgi, M., Konstantinou, K., Kouremenos, E., Lariou, M., Naoumis, D., et al. (2018). Postherpes simplex encephalitis: a case series of viral-triggered autoimmunity, synaptic autoantibodies and response to therapy. Therapeutic Advances in Neurological Disorders, 11, 1756286418768778. https://doi.org/10.1177/1756286418768778.
Titulaer, M. J., Höftberger, R., Iizuka, T., Leypoldt, F., McCracken, L., Cellucci, T., Benson, L. A., Shu, H., Irioka, T., Hirano, M., et al. (2014). Overlapping demyelinating syndromes and anti-N-methyl-D-aspartate receptor encephalitis. Annals of Neurology, 75, 411–428. https://doi.org/10.1002/ana.24117.
Ogawa, R., Nakashima, I., Takahashi, T., Kaneko, K., Akaishi, T., Takai, Y., Sato, D. K., Nishiyama, S., Misu, T., Kuroda, H., et al. (2017). MOG antibody-positive, benign, unilateral, cerebral cortical encephalitis with epilepsy. Neurology-Neuroimmunology Neuroinflammation, 4, e322. https://doi.org/10.1212/NXI.0000000000000322.
Cobo-Calvo, A., Ruiz, A., Maillart, E., Audoin, B., Zephir, H., Bourre, B., Ciron, J., Collongues, N., Brassat, D., Cotton, F., et al. (2018). Clinical spectrum and prognostic value of CNS MOG autoimmunity in adults: The MOGADOR study. Neurology, 90, e1858–e1869. https://doi.org/10.1212/WNL.0000000000005560.
Kong, S. S., Chen, Y. J., Su, I. C., Lin, J. J., Chou, I. J., Chou, M. L., Hung, P. C., Hsieh, M. Y., Wang, Y. S., Chou, C. C., et al. (2019). Immunotherapy for anti-NMDA receptor encephalitis: Experience from a single center in Taiwan. Pediatrics and Neonatology, 60, 417–422 S1875-9572(18)30354-1.
Dalmau, J., Lancaster, E., Martinez-Hernandez, E., Rosenfeld, M. R., & Balice-Gordon, R. (2011). Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurology, 10, 63–74. https://doi.org/10.1016/S1474-4422(10)70253-2.
Florance, N. R., Davis, R. L., Lam, C., Szperka, C., Zhou, L., Ahmad, S., Campen, C. J., Moss, H., Peter, N., Gleichman, A. J., et al. (2009). Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis in children and adolescents. Annals of Neurology, 66, 11–18.
Titulaer, M. J., McCracken, L., Gabilondo, I., Armangue, T., Glaser, C., Iizuka, T., Honig, L. S., Benseler, S. M., Kawachi, I., Martinez-Hernandez, E., et al. (2013). Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurology, 12, 157–165. https://doi.org/10.1016/S1474-4422(12)70310-1.
de Montmollin, E., Demeret, S., Brule, N., Conrad, M., Dailler, F., Lerolle, N., Navellou, J. C., Schwebel, C., Alves, M., Cour, M., et al. (2016). Anti-N-methyl-D-aspartate Receptor Encephalitis in Adult Patients Requiring Intensive Care. American Journal of Respiratory and Critical Care Medicine. https://doi.org/10.1164/rccm.201603-0507OC.
Zhang, J., Ji, T., Chen, Q., Jiang, Y., Cheng, H., Zheng, P., Ma, W., Lei, T., Zhang, Y., Jin, Y., et al. (2019). Pediatric Autoimmune Encephalitis: Case Series From Two Chinese Tertiary Pediatric Neurology Centers. Frontiers in Neurology, 10, 906. https://doi.org/10.3389/fneur.2019.00906.
Byrne, S., Walsh, C., Hacohen, Y., Muscal, E., Jankovic, J., Stocco, A., Dale, R. C., Vincent, A., Lim, M., & King, M. (2015). Earlier treatment of NMDAR antibody encephalitis in children results in a better outcome. Neurology-Neuroimmunology Neuroinflammation, 2, e130. https://doi.org/10.1212/NXI.0000000000000130.
Gabilondo, I., Saiz, A., Galan, L., Gonzalez, V., Jadraque, R., Sabater, L., Sans, A., Sempere, A., Vela, A., Villalobos, F., et al. (2011). Analysis of relapses in anti-NMDAR encephalitis. Neurology, 77, 996–999. https://doi.org/10.1212/WNL.0b013e31822cfc6b.
Jurek, B., Chayka, M., Kreye, J., Lang, K., Kraus, L., Fidzinski, P., Kornau, H. C., Dao, L. M., Wenke, N. K., & Long, M. (2019). Human gestational N-methyl-d-aspartate receptor autoantibodies impair neonatal murine brain function. Annals of Neurology, 86, 656–670.
Lee, W. J., Lee, S. T., Byun, J. I., Sunwoo, J. S., Kim, T. J., Lim, J. A., Moon, J., Lee, H. S., Shin, Y. W., Lee, K. J., et al. (2016). Rituximab treatment for autoimmune limbic encephalitis in an institutional cohort. Neurology, 86, 1683–1691. https://doi.org/10.1212/WNL.0000000000002635.
Stingl, C., Cardinale, K., & Van Mater, H. (2018). An Update on the Treatment of Pediatric Autoimmune Encephalitis. Current Treatment Options in Rheumatology, 4, 14–28. https://doi.org/10.1007/s40674-018-0089-z.
Nosadini, M., Toldo, I., Tascini, B., Bien, C. G., Parmeggiani, L., De Gaspari, P., Zuliani, L., & Sartori, S. (2019). LGI1 and CASPR2 autoimmunity in children: Systematic literature review and report of a young girl with Morvan syndrome. Journal of Neuroimmunology, 335, 577008 S0165-5728(19)30293-0.
Schimmel, M., Frühwald, M. C., & Bien, C. G. (2018). Limbic encephalitis with LGI1 antibodies in a 14-year-old boy. European Journal of Paediatric Neurology, 22, 190–193 S1090-3798(17)30893-0.
Vinke, A. M., Schaper, F. L. W. V. J., Vlooswijk, M. C. G., Nicolai, J., Majoie, M. H. J. M., Martinez Martinez, P., Hoffmann, C., Damoiseaux, J. G. M. C., & Rouhl, R. P. W. (2018). Anti-GAD antibodies in a cohort of neuropsychiatric patients. Epilepsy & Behavior, 82, 25–28 https://doi.org/10.1016/j.yebeh.2018.03.004.
Malter, M. P., Frisch, C., Zeitler, H., Surges, R., Urbach, H., Helmstaedter, C., Elger, C. E., & Bien, C. G. (2015). Treatment of immune-mediated temporal lobe epilepsy with GAD antibodies. Seizure, 30, 57–63. https://doi.org/10.1016/j.seizure.2015.05.017.
Scheibe, F., Pruss, H., Mengel, A. M., Kohler, S., Numann, A., Kohnlein, M., Ruprecht, K., Alexander, T., Hiepe, F., & Meisel, A. (2017). Bortezomib for treatment of therapy-refractory anti-NMDA receptor encephalitis. Neurology, 88, 366–370. https://doi.org/10.1212/WNL.0000000000003536.
Randell, R. L., Adams, A. V., & Van Mater, H. (2018). Tocilizumab in refractory autoimmune encephalitis: a series of pediatric cases. Pediatric Neurology, 86, 66–68.
Michev, A., Musso, P., Foiadelli, T., Trabatti, C., Lozza, A., Franciotta, D., Simoncelli, A. M., & Savasta, S. (2019). Bickerstaff Brainstem Encephalitis and overlapping Guillain-Barre syndrome in children: Report of two cases and review of the literature. European Journal of Paediatric Neurology, 23, 43–52 S1090-3798(18)30395-7.
Haberlandt, E., Bast, T., Ebner, A., Holthausen, H., Kluger, G., Kravljanac, R., Kroll-Seger, J., Kurlemann, G., Makowski, C., Rostasy, K., et al. (2011). Limbic encephalitis in children and adolescents. Archives of Disease in Childhood, 96, 186–191 adc.2010.183897.
Clardy, S. L., Lennon, V. A., Dalmau, J., Pittock, S. J., Jones Jr., H. R., Renaud, D. L., Harper Jr., C. M., Matsumoto, J. Y., & McKeon, A. (2013). Childhood onset of stiff-man syndrome. JAMA Neurology, 70, 1531–1536. https://doi.org/10.1001/jamaneurol.2013.4442.
Chou, I. J., Wang, H. S., Lin, J. J., Kuo, C. F., Lin, K. L., Chou, M. L., Hung, P. C., Hsieh, M. Y., & Lin, Y. T. (2013). Limbic encephalitis in Taiwanese children and adolescence: a single center study. Pediatrics and Neonatology, 54, 246–253. https://doi.org/10.1016/j.pedneo.2013.01.016.
Korff, C., Parvex, P., Cimasoni, L., Wilhelm-Bals, A., Hampe, C.S.; Schwitzgebel, V.M., Michel, M., Siegrist, C.-A., Lalive, P.H., Seeck, M. (2011). Encephalitis Associated With Glutamic Acid Decarboxylase Autoantibodies in a Child: A Treatable Condition? Arch Neurol., 68, 1065–1068. https://doi.org/10.1001/archneurol.2011.177.
Carvajal-Gonzalez, A., Leite, M. I., Waters, P., Woodhall, M., Coutinho, E., Balint, B., Lang, B., Pettingill, P., Carr, A., Sheerin, U. M., et al. (2014). Glycine receptor antibodies in PERM and related syndromes: characteristics, clinical features and outcomes. Brain, 137, 2178–2192. https://doi.org/10.1093/brain/awu142.
Figlerowicz, M., Kemnitz, P., Mania, A., Mazur-Melewska, K., Tomczak, E., Kuls, K., Jonczyk-Potoczna, K., Graus, F., & Sluzewski, W. (2018). Autoimmune encephalitis with GABAA receptor antibodies in a 10-year-old girl. Clinical Neurology and Neurosurgery, 164, 160–163 S0303-8467(17)30348-7.
Caputo, D., Iorio, R., Vigevano, F., & Fusco, L. (2018). Febrile infection-related epilepsy syndrome (FIRES) with super-refractory status epilepticus revealing autoimmune encephalitis due to GABAAR antibodies. European Journal of Paediatric Neurology, 22, 182–185 S1090-3798(17)31815-9.
Nikolaus, M., Knierim, E., Meisel, C., Kreye, J., Prüss, H., Schnabel, D., & Kallinich, T. (2018). Severe GABAA receptor encephalitis without seizures: A paediatric case successfully treated with early immunomodulation. European Journal of Paediatric Neurology, 22, 558–562.
Kruer, M. C., Hoeftberger, R., Lim, K. Y., Coryell, J. C., Svoboda, M. D., Woltjer, R. L., & Dalmau, J. (2014). Aggressive course in encephalitis with opsoclonus, ataxia, chorea, and seizures: the first pediatric case of gamma-aminobutyric acid type B receptor autoimmunity. JAMA Neurology, 71, 620–623 1834619.
Rosenbaum, T., Gartner, J., Korholz, D., Janssen, G., Schneider, D., Engelbrecht, V., Gobel, U., & Lenard, H. G. (1998). Paraneoplastic limbic encephalitis in two teenage girls. Neuropediatrics, 29, 159–162.
Alavi, S. (2013). Paraneoplastic neurologic syndromes in children: a review article. Iranian Journal of Child Neurology, 7, 6–14.
Kunstreich, M., Kreth, J., Oommen, P., Schaper, J., Karenfort, M., Aktas, O., Tibussek, D., Distelmaier, F., Borkhardt, A., & Kuhlen, M. (2017). Paraneoplastic limbic encephalitis with SOX1 and PCA2 antibodies and relapsing neurological symptoms in an adolescent with Hodgkin lymphoma. European Journal of Paediatric Neurology, 21, 661–665.
Spatola, M., Sabater, L., Planaguma, J., Martinez-Hernandez, E., Armangue, T., Pruss, H., Iizuka, T., Caparo Oblitas, R. L., Antoine, J. C., Li, R., et al. (2018). Encephalitis with mGluR5 antibodies: Symptoms and antibody effects. Neurology, 90, e1964–e1972. https://doi.org/10.1212/WNL.0000000000005614.
Dale, R. C., Merheb, V., Pillai, S., Wang, D., Cantrill, L., Murphy, T. K., Ben-Pazi, H., Varadkar, S., Aumann, T. D., Horne, M. K., et al. (2012). Antibodies to surface dopamine-2 receptor in autoimmune movement and psychiatric disorders. Brain, 135, 3453–3468. https://doi.org/10.1093/brain/aws256.
Sinmaz, N., Tea, F., Pilli, D., Zou, A., Amatoury, M., Nguyen, T., Merheb, V., Ramanathan, S., Cooper, S. T., Dale, R. C., et al. (2016). Dopamine-2 receptor extracellular N-terminus regulates receptor surface availability and is the target of human pathogenic antibodies from children with movement and psychiatric disorders. Acta Neuropathologica Communications, 4, 126. https://doi.org/10.1186/s40478-016-0397-1.
Marques-Matos, C., Melo, C., Sampaio, M., Rodrigues, E., Sousa, R., & Alves, D. (2018). Child Neurology: Treatable bilateral striatal lesions related to anti-dopamine 2 receptor autoimmunity. Neurology, 91, 98–101. https://doi.org/10.1212/WNL.0000000000005774.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
CGB wrote the first draft of the article, and CIB revised it substantially. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The retrospective study on antibody frequency was approved by the Ethics committee of the University of Münster, Germany (2017–005-f-S).
Consent for publication
Not applicable.
Competing interests
CGB obtained honoraria for speaking engagements from UCB (Monheim, Germany), Desitin (Hamburg, Germany), and Euroimmun (Lübeck, Germany). He receives research support from Deutsche Forschungsgemeinschaft (German Research Council, Bonn, Germany) and Gerd-Altenhof-Stiftung (Deutsches Stiftungs-Zentrum, Essen, Germany).
CIB has no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Bien, C.G., Bien, C.I. Autoimmune encephalitis in children and adolescents. Neurol. Res. Pract. 2, 4 (2020). https://doi.org/10.1186/s42466-019-0047-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42466-019-0047-8