
Abstract
Background
Complement component 4 (C4) gene copy number (GCN) affects the susceptibility to systemic lupus erythematosus (SLE) in different populations, however the possible phenotype significance remains to be determined. This study aimed to associate C4A, C4B and total C4 GCN and SLE, focusing on the clinical phenotype and disease progression.
Methods
C4, C4A and C4B GCN were determined by real-time PCR in 427 SLE patients and 301 healthy controls, which underwent a detailed clinical evaluation according to a pre-established protocol.
Results
The risk of developing SLE was 2.62 times higher in subjects with low total C4 GCN (< 4 copies, OR = 2.62, CI = 1.77 to 3.87, p < 0.001) and 3.59 times higher in subjects with low C4A GCN (< 2 copies; OR = 3.59, CI = 2.15 to 5.99, p < 0.001) compared to those subjects with normal or high GCN of total C4 (≥4) and C4A (≥2), respectively. An increased risk was also observed regarding low C4B GCN, albeit to a lesser degree (OR = 1.46, CI = 1.03 to 2.08, p = 0.03). Furthermore, subjects with low C4A GCN had higher permanent disease damage as assessed by the Systemic Lupus International Collaborating Clinics – Damage Index (SLICC-DI; median = 1.5, 95% CI = 1.2–1.9) than patients with normal or high copy number of C4A (median = 1.0, 95% CI = 0.8–1.1; p = 0.004). There was a negative association between low C4A GCN and serositis (p = 0.02) as well as between low C4B GCN and arthritis (p = 0.02).
Conclusions
This study confirms the association between low C4 GCN and SLE susceptibility, and originally demonstrates an association between low C4A GCN and disease severity.
Similar content being viewed by others


Background
Human C4 is one of the most striking examples of genetic diversity, due to the great variation in number and size of genes between subjects, as well as some intrinsic polymorphisms. C4 is the only component of complement that displays two different isotypes encoded by two different genes: C4A and C4B. These genes differ in only five nucleotides, but the proteins encoded by them have different functions. While C4A protein is more reactive against targets containing amino groups and has greater ability to covalently bind immune complexes, C4B has greater affinity for hydroxyl groups and exhibit a hemolytic potential at least four times higher than C4A [1].
Genes encoding the C4 protein are located in the MHC class III region, in the short arm of chromosome 6, and form, together with three neighboring genes (serine-threonine kinase, steroid 21-hydroxylase and tenascin-X), a genetic unit called RCCX module [2]. Theoretically, each chromosome 6 can harbor zero to four copies of these modules, determining wide gene copy number variation of C4.
Around 80% of the Caucasians from United States and Europe have three or four C4 copies, 20% have five or six, and less than 2% have only two copies in a diploid genome [3]. Complete deficiency of components C4A and C4B is extremely rare in healthy controls [3]. C4A or C4B homozygous deficiency occurs in 0.5–1% Caucasians, while the presence of a single C4A or C4B gene occurs in approximately 20% [4, 5]. C4A deficiency has been linked to systemic autoimmune diseases, especially systemic lupus erythematosus (SLE) [6,7,8,9]; the complete absence of C4A appears in 10–15% of patients [10, 11] and the heterozygous deficiency appears in 40–60% of SLE patients in several ethnic groups [12,13,14]. The association with certain clinical manifestations, however, is still not clear as different studies show different associations [7, 15,16,17].
The significant association of C4A deficiency with SLE in different ethnic groups suggests that C4A deficiency is a risk factor for this disease. There are several potential mechanisms for this association, such as the role of C4 in humoral immune response [18] and in the clearance of immune complexes and apoptotic cells [19, 20]. Interestingly, patients with SLE in Spain have an increased frequency of C4B deficiency and not C4A, which highlights the importance of both C4A and C4B in autoimmunity control in other ethnic groups [21].
Most epidemiologic studies of C4 in SLE, however, do not consider Copy Number Variation (CNV) of both C4A and C4B. In fact, there are few studies demonstrating that a low copy number of C4A and C4B increases the susceptibility to SLE [7,8,9, 17]. In the present study, we originally investigated the association of C4, C4A and C4B GCN variation with SLE in a large cohort of Brazilian adult patients and healthy controls, as well as a possible association with the disease phenotype and severity.
Methods
Study subjects
This observational cross-sectional study included 427 patients with SLE and 301 healthy controls. SLE patients were recruited consecutively from the Autoimmune Rheumatic Diseases Out-patient Clinic of the University Hospital, and fulfilled four or more classification criteria for SLE from the American College of Rheumatology [22]. Patients underwent a detailed clinical evaluation, with emphasis on SLE clinical manifestations, recurrent infections, current and previous medications, age at SLE onset, presence of other autoimmune diseases, and determination of Systemic Lupus International Collaborating Clinics – Damage Index (SLICC-DI) [23]. All subjects were at least 18 years old and signed the informed consent. This study was approved by the hospital ethics committee (protocol CEP#0330/09). The healthy volunteers answered a questionnaire, emphasizing signs and symptoms of autoimmune diseases and recurrent infections, which could be related to deficiency of some component of Complement. In this study, recurrent infections was defined according to the criteria suggested by Modell et al. [24], i.e., two or more upper respiratory infections (otitis or sinusitis, in the absence of the allergy) or pneumonias in one year (for more than one year), recurrent viral infections (herpes, warts), persistent fungal infections or tuberculosis. All data collected were used to analyze possible associations with the configuration of the complex gene C4A/C4B. Subjects with changes detected in any of the items in the questionnaire or a family history of SLE or other autoimmune rheumatic disease were excluded from the control group.
Determination of GCN of C4A, C4B and total C4
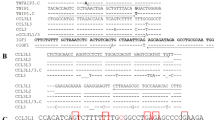
Genomic DNA was extracted from peripheral blood using the FlexiGene DNA purification kit (Qiagen). GCN was determined by real time PCR (qPCR) using TaqMan probes conjugated with a minor groove binder (MGB), as described in the study of Szilagyi et al. [5]. In both reactions to determine C4A and C4B GCN, we used 250 nM of forward C4 primer (5′-GCAGGAGACATCTAACTGGCTTCT-3′) and 500 nM of reverse (5′-CCGCACCTGCATGCTCCT-3′), 250 nM of the TaqMan probe specific for C4A (5′-FAM-ACCCCTGTCCAGTGTTAG-MGB-3′) or C4B (5’FAM-ACCTCTCTCCAGTGATAC-MGB-3′), 1x TaqMan Universal Master Mix with UNG (Applied Biosystems, Foster City, CA) and 30 ng of genomic DNA in a total volume of 25 μL. Reactions targeting RNase P, which was our single-copy reference gene, contained the mix of primers and TaqMan probe labeled with VIC for this gene (Applied Biosystems Foster City, CA), 30 ng of genomic DNA and 1x TaqMan Universal Master Mix with UNG (Applied Biosystems),
Triplicates of each reaction were amplified and read on the Rotor Gene 3000 (Corbett, Sidney) using the following conditions (50 °C for 2 min, 95 °C for 10 min, 45 cycles of 95 °C for 15 s and 60 °C for 1 min). The results were analyzed by Rotor Gene 3000 software. For the relative quantification of the number of alleles C4A and C4B, we used control DNA samples with previously defined C4A and C4B GCN, kindly provided by Szilagyi et al. [5]. The RNase P constitutive gene was used as a control for the amplification reaction. The calculation of GCN was made using the ΔΔCT method [25].
Statistical analysis
Continuous variables with normal distribution were analyzed with the Student’s t test and those with non-parametric distribution were analyzed with the Mann-Whitney test. Qualitative parameters were analyzed by the Chi-square test and the Fisher’s exact test when appropriate. Multiparametric analyses were performed with the one-way ANOVA test with Bonferroni’s test as a post-hoc test when appropriate. Correlation analysis was performed by the Spearman’s correlation method. To calculate the risk of developing disease (OR + 95% CI), we performed a binary logistic regression analysis. Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS) version 17.0 (SPSS Inc., 2008). Statistical inference level was set at 0.05.
Results
Study subjects
The female to male ratio was 286:15 in the healthy control group and 406 to 21 in the SLE group, with ages varying from 18 to 61 years old (35.1 ± 11.1) and 17 to 77 years old (39.9 ± 12.2), respectively. Patients and controls did not differ regarding gender distribution, although patients were significantly older (p < 0.001). Patients presented more recurrent infections (n = 60; 14.05%) compared to healthy controls (n = 10; 3.33%; p < 0.001). The clinical characteristics of SLE patients are depicted in Table 1.
Gene copy number of total C4, C 4A and C 4B in SLE patients and healthy controls
Total C4 GCN ranged from two to eight in controls and from one to eight in SLE patients. C4A GCN varied from zero to six in patients and in controls, while C4B GCN varied from zero to five in both groups. SLE patients presented lower mean GCN for total C4 and C4A compared to healthy controls (Table 2).
Accordingly, patients had a higher frequency of low GCN for total C4 and C4A compared to healthy controls (Fig. 1a-b). Comparing to healthy controls, the SLE group showed higher frequency of subjects with two (SLE = 7% vs controls = 1%, p < 0.001) and three copies of total C4 (SLE = 22% vs controls = 12.6%, p = 0.001). On the other hand, a higher number of controls with four copies of total C4 was observed compared to patients (SLE = 52.5% vs controls = 63.1%, p < 0.01) (Fig. 1a; Table 3).

Distributions of gene copy number (GCN) for total C4, C4A and C4B in healthy controls and systemic lupus erythematosus patients. GCN for total C4 (a), C4A (b) and C4B (c) was determined in 427 patients with systemic lupus erythematosus (SLE) and 301 healthy controls by quantitative real time PCR
Regarding C4A GCN, there was a higher frequency of SLE patients with only one copy (SLE = 18.3% vs controls = 6.3%, p < 0.001), while there was a greater proportion of controls with two copies of C4A (SLE = 58.3% vs controls = 69.4%, p < 0.01) (Table 3). There was a trend toward higher frequency of total absence of C4A genes (C4A = 0) in SLE patients (2.1%) compared to controls (0.3%; p = 0.053) (Fig. 1b). Although there was no significant difference of the C4B GCN between the two studied groups (p = 0.192), the distribution of subjects according to the GCN resembled the distribution curve for total C4 and C4A (Fig. 1c). Interestingly, a lower percentage of patients with two copies of C4B compared to controls was observed (SLE = 57.4% vs controls = 65.8%; p = 0.025) (Table 3).
There was a higher frequency of SLE patients in the group of subjects with low GCN (total C4 < 4, C4A or C4B < 2) than in the group of subjects with normal or high GCN (total C4 ≥ 4, C4A or C4B ≥ 2) (Table 4). The risk of developing SLE was 2.62 times higher in subjects with low total C4 GCN and 3.59 times higher in subjects with low C4A GCN compared to those with normal or high C4 and C4A GCN. The same was observed regarding C4B, albeit to a lesser degree (OR = 1.46).
Total C4, C 4A and C 4B GCN impacts in SLE progression and clinical phenotype
The clinical phenotype analysis showed no association between low GCN for C4, C4A or C4B and a specific clinical manifestation. On the contrary, a higher frequency of articular involvement was seen in SLE patients with high C4B GCN compared to those with low GCN (p = 0.022; Table 5). Furthermore, there was higher frequency of serositis in patients with high C4A copy number compared to those with low copy number (p = 0.019).
In addition, we investigated if the GCN for C4, C4A and C4B correlates with the progression of the disease in 335 SLE patients, using for that, the permanent damage index (DI) of the disease as measured by SLICC [23]. The Spearman correlation coefficient showed a mild but significant negative correlation between SLICC-DI and the GCN for total C4 (rho = − 0.133, p = 0.015) and C4A (rho = − 0.136, p = 0.012), but not C4B (rho = 0.223, p = 0.675). Moreover, patients with low C4A GCN had higher permanent damage index (median = 1.5; 95% CI: 1.2–1.9) than patients with normal or high C4A GCN (median = 1.0; 95% CI: 0.8–1.1; p = 0.004), regardless of age of onset and number of years of disease. This association was not observed for low total C4 [1.3 (1.0–1.6) vs 1.0 (0.8–1.2); p = 0.087] or low C4B [1.0 (0.8–1.3) vs 1.0 (0.9–1.2); p = 0.916]. There was no correlation between the GCN for C4, C4A or C4B and age onset of SLE.
Discussion
The present study confirmed, also in the peculiar blended Brazilian ethnicity, the association between low total C4 and C4A GCN and adult SLE previously reported in other ethnicities [7,8,9], and expanded this concept to low C4B GCN. This result corroborates a previous study with 90 patients with juvenile SLE and 170 patients with adult-onset SLE in Brazilian population, which showed a strong association with low number of copies of C4, C4A and C4B with SLE, remarkably in juvenile-onset lupus [26]. In addition, the present study originally demonstrated the impact of a lower C4A GCN on the progression of the disease. The distribution of total C4, C4A and C4B GCN in healthy controls was similar to that observed in other studies, with the majority of subjects presenting four copies of total C4 (63.1%), two copies of C4A (69.4%) and two copies of C4B (65.8%). Interestingly, 20% of healthy subjects had less than two copies of C4B, whereas only 6% had less than two copies of C4A.
Although most SLE patients presented four copies of total C4, there was a higher percentage of subjects with less than four copies compared to controls, as well as less than two copies of C4A. Moreover, the risk of developing SLE was 2.6 and 3.6 times higher in subjects with lower total C4 GCN and lower C4A GCN, respectively. These data are consistent with those previously observed in European, American and Asian samples, albeit with minor differences [7, 9, 27]. Only one study in the literature, performed with Japanese subjects, failed to demonstrate this association [28]. These genetic background differences had already been demonstrated, since C4A gene deletion has been more frequently reported in SLE patients in African American and Caucasian [11, 29, 30] than in Asian patients [12, 31, 32]. Moreover, the 2 bp insertion in exon 29, which leads to a C4A-null allele, was reported in Caucasian and African American SLE patients, but not in Asians [7, 28].
Although with a lower level of statistical significance, there was an association between low C4B GCN and SLE in our cohort. Previous studies have shown correlation between C4B deficiency and SLE in Spanish population [21, 27], in contrast to the UK cohort that revealed an association between high C4B GCN and SLE. Other studies failed to find association between C4B GCN and SLE [7, 9, 17]. Thus, the association between C4B GCN and SLE seems to be strongly influenced by ethnicity and further studies are needed to pinpoint the underlying genomic basis.
Despite the association of SLE with low GCN for C4, C4A and C4B, there were some SLE patients with normal or even high GCN for these genes. Conversely, some normal individuals had low GCN for these genes. This indicates that the SLE phenotype may be favored by low GCN of the C4 gene system, but this is a relative factor that is integrated with a host of modulating genetic and environmental factors that ultimately define the fate of the phenotype.
While the association between low C4 GCN and SLE has been consistently demonstrated, the impact of C4 CNV on the disease phenotypes remains controversial. In our previous study in juvenile-onset SLE, the low GCN for total C4 and C4A was associated with pericarditis [26]. A study in Chinese Han patients reported an association between low C4A deficiency and arthritis [7], while a more recent study reported serositis as the only clinical manifestation associated with low C4A GCN [17]. The current study adds some degree of complexity to this issue by showing a “protective” effect of low C4B GCN regarding the occurrence of arthritis, as well as between high C4A GCN and serositis. This apparent paradox of the “protective” effect of low C4 GCN in the development of some SLE manifestations may reflect the dual role of the Complement system in autoimmune diseases. If C4 deficiency may favor autoimmune diseases onset, due to the impairment in the clearance of autoantigens and negative selection of auto-reactive B cells, on the other hand it may reduce inflammation, because the classical cascade of the Complement system will be also partially hampered in the context of low C4A GCN [33].
Recent studies have suggested that low C4A GCN may also be linked to increased susceptibility to infections [34]. However, this is also far from unanimous, since other authors found no association between low levels of C4A and C4B proteins or different haplotypes of C4 with recurrent infections [35, 36]. In our series, there was no association between C4 CNV and infectious diseases, and only 14% of SLE patients had recurrent infections. The differences in the results of the several studies may be secondary to the criteria used to define recurrent infections. In our study, we used the criteria suggested by Modell et al. for the definition of recurrent infections [24]. It is important to consider, however, that such information was collected by questionnaire or during the retrospective analysis of medical records. Although this bias could have affected equally the groups of lupus patients and healthy controls, it is reasonable to hypothesize that this could underestimate the prevalence of infections in the present study.
An interesting and original finding of the present study was the association between low C4A GCN and permanent damage measured by SLICC-DI, suggesting that patients with low C4A GCN may have worse prognosis than those with normal or high GCN. The SLICC-DI measures permanent damage caused by SLE, by therapeutics and comorbidities. Actually, there are several studies associating C4 CNV and obesity [4] diabetes mellitus [35] and cardiovascular disease [37]. It is, therefore, possible that non-SLE conditions related to low C4 GCN may contribute to the observed increase in permanent damage in the present cohort.
Since C4 deficiency increases the activation of auto-reactive B cells and autoantibody production in animal models [38], we might expect an association between low GCN, especially of C4A, and the presence of events related to immune complex deposition, such as glomerulonephritis. However, such association was not observed either in the present study or in the one reported by Lv et al. [7], analyzing 924 Chinese SLE patients. It is possible that several genetic and adaptive factors interact, promoting or protecting against the disease and certain manifestations, what result in a wide and heterogeneous clinical spectrum.
Recently, several studies showed the association between lupus susceptibility or phenotypic features and polymorphism of different genes, such as PDCD1, BLK, TNIP1, TNFAIP3, SLC15A4, ETS1, and RasGRP3 IKZF1 [39,40,41]. The knowledge of the interplay between susceptibility genes and disease phenotypes can help us understand the clinical heterogeneity of this disease and its pathophysiology. Ultimately, this knowledge may contribute to the development of individualized approach for each patient.
In summary, the present study determined the distribution of C4 GCN in a sample of the Brazilian SLE patients and healthy controls. We confirmed the association between low C4A and low total C4 GCN and SLE, as previously described, and additionally showed similar findings for low C4B GCN. Furthermore, we originally documented a higher cumulative damage in patients with low C4A GCN as well as lower frequency of serositis in low C4A GCN patients. Finally, we observed an increased frequency of arthritis in patients with normal or high C4B GCN. Therefore, as demonstrated in this and in previous studies, low C4 GCN may be a genetic risk factor for the development of SLE and may be related to other factors, culminating in a worse disease outcome.
Conclusions
Low gene copy number for C4 genes, especially the C4A isoform, is a risk factor for development of systemic lupus erythematosus in the Brazilian population. In addition, low C4A gene copy number favors the occurrence of serositis and a more severe disease, while normal to high number of C4B genes favors the occurrence of arthritis in lupus patients. Therefore, the determination of C4 gene copy number may be useful in sub-phenotyping and managing SLE patients.
Availability of data and materials
The primary data referent to the present study is available upon request to the corresponding author.
Abbreviations
- C4 :
-
Complement C4 gene
- C4A :
-
Complement C4A gene
- C4B :
-
Complement C4B gene
- CNV:
-
Copy number variation
- GCN:
-
Gene copy number
- SLE:
-
Systemic lupus erythematosus
- SLICC-DI:
-
Systemic Lupus International Collaborating Clinics – Damage Index
References
Law SK, Dodds AW, Porter RR. A comparison of the properties of two classes, C4A and C4B, of the human complement component C4. EMBO J. 1984;3:1819–23.
Yang Z, Mendoza AR, Welch TR, Zipf WB, Yu CY. Modular variations of the human major histocompatibility complex class III genes for serine/threonine kinase RP, complement component C4, steroid 21-hydroxylase CYP21, and tenascin TNX (the RCCX module). A mechanism for gene deletions and disease associations. J Biol Chem. 1999;274:12147–56.
Blanchong CA, Zhou B, Rupert KL, Chung EK, Jones KN, Sotos JF, et al. Deficiencies of human complement component C4A and C4B and heterozygosity in length variants of RP-C4-CYP21-TNX (RCCX) modules in caucasians. The load of RCCX genetic diversity on major histocompatibility complex-associated disease. J Exp Med. 2000;191:2183–96.
Yang Y, Chung EK, Zhou B, Blanchong CA, Yu CY, Füst G, et al. Diversity in intrinsic strengths of the human complement system: serum C4 protein concentrations correlate with C4 gene size and polygenic variations, hemolytic activities, and body mass index. J Immunol. 2003;171:2734–45.
Szilagyi A, Blasko B, Szilassy D, Fust G, Sasvari-Szekely M, Ronai Z. Real-time PCR quantification of human complement C4A and C4B genes. BMC Genet. 2006;7:1.
Fan Q, Uring-Lambert B, Weill B, Gautreau C, Menkes CJ, Delpech M. Complement component C4 deficiencies and gene alterations in patients with systemic lupus erythematosus. Eur J Immunogenet. 1993;20:11–21.
Lv Y, He S, Zhang Z, Li Y, Hu D, Zhu K, et al. Confirmation of C4 gene copy number variation and the association with systemic lupus erythematosus in Chinese Han population. Rheumatol Int. 2012;32:3047–53.
Wu YL, Yang Y, Chung EK, Zhou B, Kitzmiller KJ, Savelli SL, et al. Phenotypes, genotypes and disease susceptibility associated with gene copy number variations: complement C4 CNVs in European American healthy subjects and those with systemic lupus erythematosus. Cytogenet Genome Res. 2008;123:131–41.
Yang Y, Chung EK, Wu YL, Savelli SL, Nagaraja HN, Zhou B, et al. Gene copy-number variation and associated polymorphisms of complement component C4 in human systemic lupus erythematosus (SLE): low copy number is a risk factor for and high copy number is a protective factor against SLE susceptibility in European Americans. Am J Hum Genet. 2007;80:1037–54.
Man XY, Luo HR, Li XP, Yao YG, Mao CZ, Zhang YP. Polymerase chain reaction based C4AQ0 and C4BQ0 genotyping: association with systemic lupus erythematosus in Southwest Han Chinese. Ann Rheum Dis. 2003;62:71–3.
Olsen ML, Goldstein R, Arnett FC, Duvic M, Pollack M, Reveille JD. C4A gene deletion and HLA associations in black Americans with systemic lupus erythematosus. Immunogenetics. 1989;30:27–33.
Yamada H, Watanabe A, Mimori A, Nakano K, Takeuchi F, Matsuta K, et al. Lack of gene deletion for complement C4A deficiency in Japanese patients with systemic lupus erythematosus. J Rheumatol. 1990;17:1054–7.
Steinsson K, Jónsdóttir S, Arason GJ, Kristjánsdóttir H, Fossdal R, Skaftadóttir I, et al. A study of the association of HLA DR, DQ, and complement C4 alleles with systemic lupus erythematosus in Iceland. Ann Rheum Dis. 1998;57:503–5.
Yang Y, Lhotta K, Chung EK, Eder P, Neumair F, Yu CY. Complete complement components C4A and C4B deficiencies in human kidney diseases and systemic lupus erythematosus. J Immunol. 2004;173:2803–14.
Sturfelt G, Truedsson L, Johansen P, Jonsson H, Nived O, Sjöholm AG. Homozygous C4A deficiency in systemic lupus erythematosus: analysis of patients from a defined population. Clin Genet. 1990;38:427–33.
Petri M, Watson R, Winkelstein JA, McLean RH. Clinical expression of systemic lupus erythematosus in patients with C4A deficiency. Medicine (Baltimore). 1993;72:236–44.
Tsang-A-Sjoe MWP, Bultink IEM, Korswagen LA, et al. Comprehensive approach to study complement C4 in systemic lupus erythematosus: gene polymorphisms, protein levels and functional activity. Mol Immunol. 2017;92:125–31.
Fischer MB, Ma M, Goerg S, Zhou X, Xia J, Finco O, et al. Regulation of the B cell response to T-dependent antigens by classical pathway complement. J Immunol. 1996;157:549–56.
Davies KA, Erlendsson K, Beynon HL, Peters AM, Steinsson K, Valdimarsson H, et al. Splenic uptake of immune complexes in man is complement-dependent. J Immunol. 1993;151:3866–73.
Korb LC, Ahearn JM. C1q binds directly and specifically to surface blebs of apoptotic human keratinocytes: complement deficiency and systemic lupus erythematosus revisited. J Immunol. 1997;158:4525–8.
Naves M, Hajeer AH, Teh LS, Davies EJ, Ordi-Ros J, Perez-Pemen P, et al. Complement C4B null allele status confers risk for systemic lupus erythematosus in a Spanish population. Eur J Immunogenet. 1998;25:317–20.
Hochberg MC. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40:1725.
Gladman D, Ginzler E, Goldsmith C, Fortin P, Liang M, Urowitz M, et al. The development and initial validation of the systemic lupus international collaborating clinics/American College of Rheumatology damage index for systemic lupus erythematosus. Arthritis Rheum. 1996;39:363–9.
Modell V, Gee B, Lewis DB, Orange JS, Roifman CM, Routes JM, et al. Global study of primary immunodeficiency diseases (PI)--diagnosis, treatment, and economic impact: an updated report from the Jeffrey Modell Foundation. Immunol Res. 2011;51:61–70.
Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(−Delta Delta C(T)) method. Methods. 2001;25:402–8.
Pereira KMC, Faria AGA, Liphaus BL, Jesus AA, Silva CA, Carneiro-Sampaio M, Andrade LEC. Low C4, C4A and C4B gene copy numbers are stronger risk factors for juvenile-onset than for adult-onset systemic lupus erythematosus. Rheumatology. 2016;55(5):869–73.
Boteva L, Morris DL, Cortés-Hernández J, Martin J, Vyse TJ, Fernando MM. Genetically determined partial complement C4 deficiency states are not independent risk factors for SLE in UK and Spanish populations. Am J Hum Genet. 2012;90:445–56.
Kamatani Y, Matsuda K, Ohishi T, Ohtsubo S, Yamazaki K, Iida A, et al. Identification of a significant association of a single nucleotide polymorphism in TNXB with systemic lupus erythematosus in a Japanese population. J Hum Genet. 2008;53:64–73.
Reveille JD, Anderson KL, Schrohenloher RE, Acton RT, Barger BO. Restriction fragment length polymorphism analysis of HLA-DR, DQ, DP and C4 alleles in Caucasians with systemic lupus erythematosus. J Rheumatol. 1991;18:14–8.
Hartung K, Baur MP, Coldewey R, Fricke M, Kalden JR, Lakomek HJ, et al. Major histocompatibility complex haplotypes and complement C4 alleles in systemic lupus erythematosus. Results of a multicenter study. J Clin Invest. 1992;90:1346–51.
Doherty DG, Ireland R, Demaine AG, Wang F, Veerapan K, Welsh KI, et al. Major histocompatibility complex genes and susceptibility to systemic lupus erythematosus in southern Chinese. Arthritis Rheum. 1992;35:641–6.
Hong GH, Kim HY, Takeuchi F, Nakano K, Yamada H, Matsuta K, et al. Association of complement C4 and HLA-DR alleles with systemic lupus erythematosus in Koreans. J Rheumatol. 1994;21:442–7.
Gilliam BE, Reed MR, Chauhan AK, Dehlendorf AB, Moore TL. Significance of complement components C1q and C4 bound to circulating immune complexes in juvenile idiopathic arthritis: support for classical complement pathway activation. Clin Exp Rheumatol. 2011;29:1049–56.
Kainulainen L, Peltola V, Seppänen M, Viander M, He Q, Lokki ML, et al. C4A deficiency in children and adolescents with recurrent respiratory infections. Hum Immunol. 2012;73:498–501.
Liberatore RR, Barbosa SF, Alkimin M, Bellinati-Pires R, Florido MP, Isaac L, et al. Is immunity in diabetic patients influencing the susceptibility to infections? Immunoglobulins, complement and phagocytic function in children and adolescents with type 1 diabetes mellitus. Pediatr Diabetes. 2005;6:206–12.
Guerra-Junior G, Grumach AS, de Lemos-Marini SH, Kirschfink M, Condino Neto A, de Araujo M, et al. Complement 4 phenotypes and genotypes in Brazilian patients with classical 21-hydroxylase deficiency. Clin Exp Immunol. 2009;155:182–8.
Arason GJ, Bödvarsson S, Sigurdarson ST, Sigurdsson G, Thorgeirsson G, Gudmundsson S, et al. An age-associated decrease in the frequency of C4B*Q0 indicates that null alleles of complement may affect health or survival. Ann N Y Acad Sci. 2003;1010:496–9.
Einav S, Pozdnyakova OO, Ma M, Carroll MC. Complement C4 is protective for lupus disease independent of C3. J Immunol. 2002;168:1036–41.
Thorburn CM, Prokunina-Olsson L, Sterba KA, Lum RF, Seldin MF, Alarcon-Riquelme ME, et al. Association of PDCD1 genetic variation with risk and clinical manifestations of systemic lupus erythematosus in a multiethnic cohort. Genes Immun. 2007;8:279–87.
Zhang Z, Zhu KJ, Xu Q, Zhang XJ, Sun LD, Zheng HF, et al. The association of the BLK gene with SLE was replicated in Chinese Han. Arch Dermatol Res. 2010;302:619–24.
He CF, Liu YS, Cheng YL, Gao JP, Pan TM, Han JW, et al. TNIP1, SLC15A4, ETS1, RasGRP3 and IKZF1 are associated with clinical features of systemic lupus erythematosus in a Chinese Han population. Lupus. 2010 Sep;19(10):1181–6.
Acknowledgements
We gratefully acknowledge Dr. Agnes Szilagyi, for all the support to develop the method for C4 quantification and for kindly providing the DNA samples with previously determined number of C4A and C4B genes.
Funding
This study was supported by grants from public agencies for research funding, which poses no conflict of interests for the authors.
This study was supported by grants #2008/57316–1 and #2009/53449–0 from Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP).
Author information
Authors and Affiliations
Contributions
KMCP contributed with the conception, design of the work, collection of subject samples, acquisition, analysis and interpretation of data and have drafted the manuscript; SP contributed with the collection of subject samples and had a major contribution in writing the manuscript; AGAF contributed with the collection of subject samples and acquisition of the data; ESM contributed with the analysis and interpretation of data and revised the manuscript; VCS and MG contributed with the collection of subject samples; NPS contributed with the design of the work, analysis and interpretation of data; LECA contributed with the conception, design of the work, analysis and interpretation of data and substantively revised the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the hospital ethics committee (protocol CEP#0330/09). All participating subjects signed the informed consent form.
Consent for publication
All authors are aware of the full content of the manuscript and provided consent for the submission to Advances in Rheumatology.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Pereira, K.M.C., Perazzio, S., Faria, A.G.A. et al. Impact of C4, C4A and C4B gene copy number variation in the susceptibility, phenotype and progression of systemic lupus erythematosus. Adv Rheumatol 59, 36 (2019). https://doi.org/10.1186/s42358-019-0076-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42358-019-0076-6