
Abstract
Background
Epididymitis has several etiologies that can be related to infectious and non-infectious causes, autoimmune conditions, aseptic causes, and even certain pharmaceutical medications (amiodarone and chemotherapeutic agents). Some cases of epididymitis are complicated with pyocele formation that requires emergent surgical intervention to prevent testicular gangrene. This report describes the case of a 66-year-old male who developed severe bilateral epididymitis complicated by bilateral pyocele and ensuing sepsis. Astonishingly, the condition resolved completely without surgical intervention.
Case presentation
We are presenting a case of a non-sexually active male who developed bilateral severe epididymitis complicated by pyocele that led to the development of septic shock. Further history revealed that the patient was not sexually active with male or female partners and denied any form of trauma. Physical examination demonstrated scrotal swelling and erythema on inspection and severe tenderness on palpation. Digital rectal examination as well as abdominal examinations was unremarkable. Laboratory investigations disclosed severe leukocytosis with a neutrophil predominance (39,000 K/UL, normal range 4500–11,000 K/UL), as well as an elevation of systemic inflammatory markers such as erythrocyte sedimentation rate and C-reactive protein. Urine culture was positive for Escherichia coli. Ultrasound revealed bilateral epididymitis and pyocele. This patient was managed with a course of meropenem, resolving the epididymitis and pyocele without the need of surgical intervention.
Conclusions
Surgical intervention is considered the standard of care and the approved management for pyocele to avoid further complications such as Fournier’s gangrene. However, this patient was treated solely with antibiotics, and his condition was stabilized without the need of surgical intervention that would result in additional cost and length of stay for the patient. This case raises further questions regarding the potentially better bioavailability of this antibiotic in the scrotum compared to elsewhere in the body and the potential for a non-surgical alternative approach in the management of patients with pyocele and requires further research.
Similar content being viewed by others


Background
The epididymis is a tubular structure that is located on the posterior, upper, portion of the testes; both organs are enclosed within the tunica vaginalis (Luzzi and O'Brien 2001; Bedford 1994; Banyra and Shulyak 2012). Epididymitis occurs because of infectious and non-infectious causes, autoimmune diseases, aseptic causes, and even certain pharmaceutical medications (amiodarone and chemotherapeutic agents) (Zhao et al. 2020; Tracy et al. 2008). The incidence is about 2.5–6.5 per 100,000 individuals annually (Ludwig 2008). Potential long-term complications of epididymitis include, but are not limited to, sub-fertility due to oligospermia or even infertility due to azoospermia (Ludwig 2008; Sivaraj et al. 2021). Furthermore, some patients can develop orchitis due to its anatomical proximity to the epididymis (Bedford 1994; Sivaraj et al. 2021). Rarely, epididymitis can lead to the development of pyocele, which is considered one of the most serious urological emergencies that requires prompt surgical intervention to prevent serious complications such as Fournier’s gangrene, permanent infertility, sepsis, or even in some cases death (Banyra and Shulyak 2012; Ludwig 2008).
Case presentation
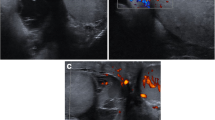
A 66-year-old male with a past medical history significant for hypertension, Parkinson’s disease, and benign prostatic hyperplasia (BPH) treated with transurethral resection of the prostate (TURP) in 2019 presented to the emergency department with severe scrotal pain, fatigue, and diaphoresis on admission. Vital signs revealed that the patient was febrile and quickly indicated presumed septic shock and sepsis protocol was initiated. Further history from the patient revealed no sexual activity in the past eight months with either male or female partners and was negative for any trauma. Further inquiry into the patient’s additional medical, familial, social, or surgical history was unremarkable. Physical examination demonstrated scrotal swelling and erythema on inspection and severe tenderness on palpation. Digital rectal examination and abdominal examinations were both unremarkable. Laboratory investigation disclosed severe leukocytosis with a neutrophil predominance (39,000 K/UL, normal range of 4500–11,000 K/UL), as well as an elevation of systemic inflammatory markers such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). The patient’s comprehensive metabolic panel (CMP) was found to be within normal limits. The scrotal ultrasound shown below (Fig. 1) demonstrated severe bilateral epididymitis/orchitis complicated by pyocele. In addition to normal saline fluid resuscitation and analgesia control, the patient was initiated on an antibiotic regimen consisting of vancomycin (1.25 g Q12H IV) and meropenem (1 g Q8H IV).

Extensive complex fluid collection and septation and heterogeneous with increase blood flow seen in A and B, this indicated large size pyocele (white arrows). Severe inflammation of epididymis (left epididymis is enlarged to 4.9 × 2.9 cm, and right epididymis is enlarged to 4.1 × 1.7 cm) and orchitis are observed in C and D (white arrows)
The patient was counseled on the need for surgical intervention, but formally declined all surgical treatments. At this point, the patient remained on the course of antibiotics and was scheduled to complete the regimen. Further investigation revealed abnormal urinalysis parameters, indicating the presence of a urinary tract infection. The patient’s urine and blood cultures were reported as positive for Escherichia coli (E. coli) with sensitivity to meropenem. At this stage, vancomycin was discontinued. Moreover, the urine nucleic acid amplification test (NAAT) test was negative for Chlamydia trachomatis and Neisseria gonorrhea. The patient was monitored under strict clinical, serological, and radiographical observation. Within a few days of initiating the antibiotic regimen, the patient’s clinical and hemodynamic status indicated signs of improvement. Of note, upon completion of fourteen days of meropenem, the patient’s condition resolved. This was confirmed by the clinical picture as well as testicular ultrasonographic findings revealing the resolution of the patient’s pyocele with no complicating factors or side effects (Fig. 2).

Significant improvement of epididymitis in A, B, and C (arrows), only mild epididymitis seen in C (arrow). No pyocele or septations are observed. The organs are normal in echogenicity and homogeneous in echotexture
Discussion
Pyocele is one of the most serious urological emergencies that requires prompt surgical intervention, particularly in adults. However, in the pediatric patient population there are several cases where different management approaches were performed successfully: treatment with antibiotics in addition to surgery or with antibiotics alone. Victoria T. et al. diagnosed an infant with pyocele and sepsis (Terentiev et al. 2015). Tian-Qu H. et al. performed a statistical analysis on 56 newborns with pyocele to determine the prognosis and recovery times among a conservatively managed (antibiotics alone) group (42 patients) versus a non-conservatively (surgical) managed group (14 patients). As a result of the analysis, the recovery times among the group treated with antibiotics compared with the surgical group were statistically different (8–17 days and 6–16 days, respectively). However, only one case from the conservative group developed testicular retardation, while in the surgical group two patients had testicular retardation. The authors concluded that conservative management was superior to that of surgical intervention with respect to the management of pyocele in the pediatric patient population (He et al. 2022). Kate H. et al. reported four cases of pyocele that were treated with non-surgical intervention in children with no complications (Kraft et al. 2012). Kutin ND. et al. reported three idiopathic cases of pyocele that were treated with surgery alone (Kutin et al. 1986). There are various other cases of pyocele in children that were treated with non-surgical intervention successfully (Oberlin and Cheng 2015; Mondal et al. 2016; Aguilera-Alonso et al. 2018). Nonetheless, most cases reported in adults were managed with surgery alone (Slavis et al. 1989; Butler and Chambers 2008; Patil et al. 2014).
In this case, an elderly male developed a severe case of bilateral epididymitis complicated by sepsis and pyocele formation because of gram-negative bacteria (E. coli). This patient was treated with meropenem alone, although surgical intervention is considered the standard of care in pyocele (Slavis et al. 1989; Butler and Chambers 2008; Patil et al. 2014).
There are various causes of epididymitis; foremost of the potential etiologies, we have infectious causes such as sexually transmitted bacteria such as Neisseria gonorrhea (NG) and Chlamydia trachomatis (CT), and non-sexually transmitted bacteria such as E. coli, klebsiella sp., and Proteus sp., etc. Viral causes such as Mumps have also been documented (Luzzi and O'Brien 2001; Bedford 1994; Banyra and Shulyak 2012). Non-infectious causes include chemical exposure, trauma, and medications (amiodarone, chemotherapeutic agents), as well as autoimmune disorders (Luzzi and O'Brien 2001; Tracy et al. 2008; Sivaraj et al. 2021). In most cases, epididymitis concomitantly develops with orchitis due to the anatomical proximity of both organs (Terentiev et al. 2015; Bruner et al. 2012). In young sexually active male adults (< 39 years old), both conditions can develop secondarily to sexually transmitted and related bacteria, particularly GN and CT. Patients typically present indolently with severe scrotal manifestations (tenderness, swelling, erythema) (Sivaraj et al. 2021; Terentiev et al. 2015; He et al. 2022; Bruner et al. 2012; Oberlin and Earl 2015). Furthermore, systemic and constitutional signs and symptoms may also be observed. These include, but are not limited to fever, chills, diaphoresis, fatigue, respiratory distress, abdominal pain, dysuria, urinary urgency, rash, and arthralgia (Bruner et al. 2012; Oberlin and Earl 2015). Additionally, adults 40 years of age and older may develop the above-described ailments secondary to non-sexually transmitted microorganisms following instances of trauma, surgery, and urological procedures (Luzzi and O'Brien 2001; Kraft et al. 2012; Ramjit et al. 2020). In these cases, gram-negative bacteria (E. coli, Klebsiella sp., Proteus sp., and Pseudomonas sp., etc.) are potential causative agents for prostatitis, cystitis, and pyelonephritis, in addition to epididymitis and orchitis (Bruner et al. 2012). The concomitant presentation may be seen in patients with pre-existing prostatitis or cystitis. In rare cases, these conditions may be further complicated by pyocele formation, which validates additional investigation for the potential need of emergent surgical intervention and exploration (Ludwig 2008; Slavis et al. 1989; Butler and Chambers 2008; Patil et al. 2014).
Epididymitis and orchitis can be diagnosed via urinalysis, NAAT, seminal fluid analysis, blood culture, or with the aid of imaging modalities such as ultrasound (Luzzi and O'Brien 2001; Tracy et al. 2008; Oberlin and Earl 2015). The blood culture ensures that the patient is placed on the appropriate antibiotic regimen. The development of complications associated with epididymitis and orchitis, such as pyocele, sepsis, and necrotizing fasciitis, and Fournier’s gangrene may also warrant the necessity for further management. Once more, documented pyocele formation is an emergency and necessitates prompt surgical intervention that can elude life-altering consequences such as Fournier’s gangrene and permanent testicular damage (Zhao et al. 2020; Silva et al. 2018). In addition, bilateral epididymitis and orchitis can increase the incidence of infertility, which can be of grave consequences especially in young adult males due to ductular damage and fibrosis (Bedford 1994; Oberlin and Earl 2015; Ramjit et al. 2020; Silva et al. 2018). Those patients should be further investigated for sexually transmitted diseases, including human immunodeficiency virus (HIV), syphilis, and human papillomavirus (Ramjit et al. 2020; Silva et al. 2018).
This patient was treated with meropenem with no side effects reported and avoided surgical intervention with the complete resolution of the condition. This can be elucidated by the excellent bioavailability of meropenem within the scrotum which aided in the resolution of the disease. The patient was satisfied with the outcome and the cost-effective nature of the care provided.
Conclusions
This case report highlights the serious consequences of complicated epididymitis with pyocele, which may lead to permanent testicular damage, Fournier’s gangrene, or even, in some cases, death. The gold standard of management is surgery; however, an antibiotic approach to the management of pyocele may serve as a viable alternative cure of the disease if a high enough bioavailability in the scrotum can be achieved. Further research is warranted to determine the best treatment options for the management of pyocele.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BPH:
-
Benign prostatic hyperplasia
- TURP:
-
Transurethral resection of the prostate
- ESR:
-
Erythrocyte sedimentation rate
- CRP:
-
C-reactive protein
- NAAT:
-
Nucleic acid amplification test
- E. coli :
-
Escherichia coli
- NG:
-
Neisseria gonorrhea
- CT:
-
Chlamydia trachomatis
- HIV:
-
Human immunodeficiency virus
References
Aguilera-Alonso D, Del Rosal T, Pérez Muñoz S, Baquero-Artigao F (2018) Neonatal epididymo-orchitis with pyocele caused by Escherichia coli: successful treatment with antimicrobial therapy alone. Enferm Infecc Microbiol Clin (engl Ed) 36(8):530–531. https://doi.org/10.1016/j.eimc.2017.10.027
Banyra O, Shulyak A (2012) Acute epididymo-orchitis: staging and treatment. Cent Eur J Urol 65(3):139–143. https://doi.org/10.5173/ceju.2012.03.art8
Bedford JM (1994) The status and the state of the human epididymis. Hum Reprod. https://doi.org/10.1093/oxfordjournals.humrep.a138416
Bruner DI, Ventura EL, Devlin JJ (2012) Scrotal pyocele, Uncommon urologic emergency. J Emerg Trauma Shock 5(2):206. https://doi.org/10.4103/0974-2700.96504
Butler JM, Chambers J (2008) An unusual complication of epididymo-orchitis: scrotal pyocele extending into the inguinal canal mimicking a strangulated inguinal hernia. J Emerg Med 35(4):379–384. https://doi.org/10.1016/j.jemermed.2007.02.029
He TQ, Zhu LH, Li CY, Peng QL, Zu JC, Liu Y, Zhao YW (2022) Clinical analysis of pyocele of tunica vaginalis in 56 newborns. Urol Int 106(7):700–705. https://doi.org/10.1159/000519096
Kraft KH, Lambert SM, Snyder HM 3rd, Canning DA (2012) Pyocele of the scrotum in the pediatric patient. J Pediatr Urol 8(5):504–508. https://doi.org/10.1016/j.jpurol.2011.10.005
Kutin ND, Schwartz DL, So HB, Becker JM (1986) Idiopathic infant pyoceles. J Pediatr Surg 21(5):441–442. https://doi.org/10.1016/s0022-3468(86)80516-4
Ludwig M (2008) Diagnosis and therapy of acute prostatitis, epididymitis and orchitis. Andrologia 40(2):76–80. https://doi.org/10.1111/j.1439-0272.2007.00823.x
Luzzi GA, O’Brien TS (2001) Acute epididymitis. BJU Int 87(8):747–755. https://doi.org/10.1046/j.1464-410x.2001.02216.x
Mondal N, Sharma S, Balachander B, Vaishnav D, Plakkal N, Vishnu Bhat B (2016) Neonatal sepsis presenting as pyocele. Indian J Pediatr 83(8):862–863. https://doi.org/10.1007/s12098-015-2023-9
Oberlin DT, Cheng EY (2015) Management of pediatric pyocele using percutaneous imaging-guided aspiration. Int J Surg Case Rep 16(2):119–121. https://doi.org/10.1016/j.ijscr.2015.09.003
Patil S, Goel A, Singh V, Sankhwar SN (2014) A rare case of stricture urethra presenting as pyocele and urethrotunica vaginalis fistula. BMJ Case Rep. https://doi.org/10.1136/bcr-2013-202180
Ramjit A, Shin C, Hayim M (2020) Complete testicular infarction secondary to epididymoorchitis and pyocele. Radiol Case Rep 15(4):420–423. https://doi.org/10.1016/j.radcr.2020.01.001
Silva EJR, Ribeiro CM, Mirim AFM, Silva AAS, Romano RM, Hallak J, Avellar MCW (2018) Lipopolysaccharide and lipotheicoic acid differentially modulate epididymal cytokine and chemokine profiles and sperm parameters in experimental acute epididymitis. Sci Rep 8(1):103. https://doi.org/10.1038/s41598-017-17944-4
Sivaraj V, Ahamed A, Artykov R, Menon-Johansson A (2021) Epididymitis and its aetiologies in a central London sexual health clinic. Int J STD AIDS 32(1):96–99. https://doi.org/10.1177/0956462420963879
Slavis SA, Kollin J, Miller JB (1989) Pyocele of scrotum: consequence of spontaneous rupture of testicular abscess. Urology 33(4):313–316. https://doi.org/10.1016/0090-4295(89)90274-4
Terentiev V, Dickman E, Zerzan J, Arroyo A (2015) Idiopathic infant pyocele: a case report and review of the literature. J Emerg Med 48(4):e93–e96. https://doi.org/10.1016/j.jemermed.2014.07.038
Tracy CR, Steers WD, Costabile R (2008) Diagnosis and management of epididymitis. Urol Clin North Am 35(1):101–108. https://doi.org/10.1016/j.ucl.2007.09.013
Zhao H, Yu C, He C, Mei C, Liao A, Huang D (2020) The immune characteristics of the epididymis and the immune pathway of the epididymitis caused by different pathogens. Front Immunol 11:2115. https://doi.org/10.3389/fimmu.2020.02115
Acknowledgements
We thank Dr. Lamia Naseer for her assistance and organization of the images.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
HH, EG, AF, ARJ, and ZFS conceived the study and wrote the paper. AB, SA, LM, and MAS wrote the paper. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This research has received all the required approvals. The patient has provided written informed consent and had no objections or comments regarding the publication of this case report and its content.
Consent for publication
A written informed consent to publish this information was obtained from the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hussain, H., Fadel, A., Garcia, E. et al. Surgery versus antibiotics in pyocele: a case report. Bull Natl Res Cent 47, 50 (2023). https://doi.org/10.1186/s42269-023-01025-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42269-023-01025-w