
Abstract
Aim
To evaluate the effect of using different short fiber-reinforced resin composites on fracture resistance and flexural strength of endodontically treated tooth and compare it with nano-filled resin composite.
Methods
Sixty human premolars were used for the fracture resistance test. Root canals were sequentially enlarged using a Pro-taper system from SX to F3 and obturated with Gutta-percha. Mesio-Occluso-Distal (MOD) cavities were prepared in all teeth. Teeth were then divided into 3 groups (n = 20 each) based on the type of resin composite. Group 1: Alert fiber-reinforced resin composite, Group 2: EverX Flow fiber-reinforced resin composite, and Group 3: Z350 nano-filled resin composite. Each group were subjected to a load till fracture using a universal testing machine to measure the fracture resistance. For the flexural strength test, 10 specimens from each material were prepared and 3- point bending tests were performed. The results of both tests were analyzed by using Weibull analysis.
Results
Teeth restored with Ever X fiber-reinforced resin composite conveyed the highest significant fracture resistance and flexural strength value when compared to the other two materials.
Conclusions
Short Fiber-reinforced resin composite can be considered a better choice for the restoration of MOD cavities in endodontically treated teeth.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Endodontically treated teeth (ETT) are more prone to fracture when compared to vital teeth, the weakened structure of endodontically treated teeth was primarily referred to the loss of anatomical structures such as marginal ridges, cusps, and pulp chamber roof due to caries, access cavity, and radicular preparation that increase tooth fragility (Kalburge et al. 2013; Hannig et al. 2005).
Cavity preparation in non-vital teeth especially the preparation of the Mesio-Occluso-Distal cavities brings a further remarkable decrease in tooth strength owing to the extensive cavity preparation and the micro-fractures that result from the applied occlusal forces. Restoration of endodontically treated teeth especially those with extensive tooth loss is a true challenge for the operators. There have been several materials developed for the restoration of endodontically treated teeth including amalgam, glass ionomer, and resin composite (Ozsevik et al.2015).
Resin-bonded composites can improve rigidity and increase the fracture resistance of non-vital teeth. Unluckily, polymerization shrinkage is still the major drawback for the use of this type of restoration, especially in large cavities, which consequently leads to tooth fracture and restoration failure (Taha et al. 2009).
To withstand this drawback in conventional resin composite, the addition of fibers of different sizes and morphology was done to modify the physical and mechanical properties of the resin composite leading to the development of a new composite under the name of Fiber-reinforced resin composites. The latter offers a reduction in polymerization shrinkage and consequantly, increases the toughness and impact strength. The fiber-reinforced resin composite was classified according to the type of fibers incorporated in the resin into a glass, carbon, or polyethylene fiber. Glass fiber-reinforced resin composite was frequently used for restoring endodontically treated teeth (Kumar et al. 2016; Goguţă et al.2012).
Recently, the short fiber-reinforced resin composite was introduced as a dentine replacement. Its structure nearly resembles the fibrous structure of natural dentine. This material is mainly used as a bulk base in large restorations, especially in stress-bearing areas. The composition of these composites was mainly E- glass short fibers and inorganic fillers embedded in an organic matrix. This structure enhances bonding properties and improves the toughness of the resin composite (Garoushi et al. 2018). Alert resin composite was the initial formulation of the short glass fiber-reinforced resin composite that was introduced into the markets in the late 1990s while a more recent formulation (Ever X Flow) was launched in the markets in 2019 (Lassila et al. 2020).
Fracture resistance is considered one of the main characteristics of dental materials as it describes the tolerance of the material to different stresses. Its values depend on the ability of the material to resist the crack propagation that originated from its internal defects which subsequently leads to microscopic fractures in the margins of the restoration or even results in bulk fractures of the filling itself (Bonilla et al. 2001). Flexural strength (transverse strength) is another test with a combination of both compressive and tensile strength, it includes elements of proportional limit and modulus of elasticity measurements. Both fracture resistance and flexural strength are part of the criteria that can estimate the clinical longevity of the restoration (Paidi et al. 2017).
Since the process of development of new materials was very fast, the clinicians were often confused regarding the choice of the best material that can mimic the effect of natural structure. Hence, the present study aimed to evaluate the fracture resistance and flexural strength of endodontically treated teeth restored with two short fiber-reinforced resin composite restorations compared to nano-filled resin composite restoration. The Null hypothesis test is that no difference shows in fracture resistance and flexural strength between the 2 types of short fiber-reinforced composite and nano-filled resin composite when used to restore endodontically treated teeth.
Materials and methods
Materials used, compositions, and manufacturers are illustrated in Table 1.
Methods
Sample size calculation
The power of the study was evaluated using post-hoc analysis. Sixty samples (n = 20 for each group) with a one-way ANOVA study achieves a power of 100%. The effect size f = 1.3 and the significant level was set at 0.05 (G*Power, v3.1.9.7 for windows).
Sample collection
Sixty intact single-rooted premolars that were freshly extracted for orthodontic purposes, using the luxation method, were collected from National Research Centre and used in this pre-clinical study. All teeth were examined under transillumination and magnification (2 × magnification lens) and only teeth that were free of cracks, caries, fractures, and without any previous restorations were included in the study. A hand scaler was used to remove any soft tissue and calculus deposits from the teeth, then all teeth were rinsed in distilled water and stored in a saline solution.
Sample preparation
Standardized endodontic access cavities were prepared in the teeth using 2# diamond round bur with coolant in a high-speed handpiece (Dentsply, Tulsa, USA) for penetration of the pulp chamber, and then tapering cylinder bur was used to complete the access cavity. For all specimens, MOD cavities were then prepared using cylindrical diamond burs size 2# (Diatech, Heerbrugg, Germany) by one operator with the following dimensions: The width of the occlusal isthmus was one-half of the inter-cuspal distance, the pulpal floor was 2.5 mm in depth, the axial wall depth was 1.5 mm, the width of the proximal box was half the buccolingual dimensions, the gingival floor was placed 1 mm above the cementoenamel junction. The bur was changed after each five prepared cavities.
A 10 k-file (Mani Inc, Japan) was used to establish the working lengths. The root canals were sequentially enlarged using a Pro-taper system from SX to F3 till the determined working length according to manufacturer guidelines using X Smart Endomotor (Dentsply-Maillefer, Ballaigues, Switzerland) Irrigation was performed using 3 mL of 2.5% NaOCl after every change of instrument. Following biomechanical preparation, 17% EDTA was used for 1 min, followed by distilled water for 1 min, and dried with medium paper points (Dentplus, Choonchong, Korea). After the complete preparation of the teeth, all the canals were obturated using Gutta-percha (Diadent, Group International, Korea) with the use of a cold lateral condensation technique and AD sealant (Meta Biomed, Cheongwon, Korea) (Moosavi et al. 2012). A hot instrument was used to remove excess gutta-percha from the coronal orifice of the canals, and all samples were stored for seven days in 100% humidity to allow for the setting of the sealer. After that, the pulp chamber was filled with resin-modified glass ionomer cement (GC Fuji II LC Capsule, GC Corporation) to a thickness that extended 1 mm occlusal to the cementoenamel junction (CEJ).
The Specimens were then divided randomly into three groups (n = 20 each) according to the type of resin composite used for restoration, Group 1: Alert fiber-reinforced resin composite [Alr], Group 2: Ever X flow fiber-reinforced bulk fill flowable composite [Exf], and Group 3: Filtek Z350 nano-filled resin composite [FZ3].
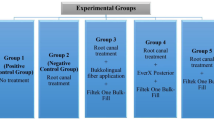
After applying auto-matrices in all spacemen, the application of 37% phosphoric acid (Ivoclar Vivadent) was done for 30 s for enamel and 15 s for dentine followed by water rinsing for 20 s then air dryness was done for 5 s. A single bond (3 M ESPE, St. Paul, MN, USA) was applied followed by light curing with Optilux 500 (Demetron-Kerr, Orange, CA, USA) with a light intensity of 1200 mW/cm2 for 10 s. In all cavities of Alert and Nano-filled composite, the first layer of resin composite (2 mm thick) was applied on the gingival seat of both proximal boxes in the MOD cavities and packed near the axial wall then light-cured for the 40 s. Subsequent layers of the same thickness were placed in a direction from the gingival floor to the occlusal surface to fill the preparation and each increment was then light-cured for the 40 s. Regarding Ever X flow resin composite application, it was applied into the cavity as one bulk layer to fill all the MOD cavities leaving only 1 mm from the occlusal surface, and then light-cured for the 40 s. A universal resin composite (GC Corporation Tokyo, Japan) was applied over the Ever X Flow for the thickness of 1 mm at the surface of the tooth and cured for 40 s. (Goda and Abogabal, 2020) (Fig. 1).

Illustration of different restoration groups in tooth model: pulp chamber was filled with resin-modified glass ionomer cement (RMGIC) in the 3 groups. Group 1, coronal restoration with Alert fiber-reinforced resin composite (AL); Group 2, coronal restoration with Ever X flow fiber-reinforced (Ex) followed by 1 ml of universal composite (UC); and Group 3: coronal restoration with nano-filled resin composite (NF)
In all groups after the removal of matrix bands, post-curing was done from the mesial and distal surface for the 40 s according to manufacture instructions, then restorations were finished and polished using 12# finishing bur and rubber point at a low-speed handpiece. After that, all specimens were stored in distilled water for 24 h. The self-cure acrylic resin was used to fix all the spacemen in cylindrical tubes (5 mm × 5 mm) in a direction parallel to the long axis of the tube, leaving 1 mm from the cementoenamel junction.
Fracture resistance testing
For the fracture resistance test, each group have mounted individually on a computer-controlled testing machine (Model 3345; Instron Industrial Products, Norwood, MA, USA) with a load cell of 5 k, N, then the readings were registered using computer software (Instron® Bluehill Lite Software). The spacemen were fixed by securing screws to the lower fixed chamber of the testing machine. A compressive load was applied occlusally by using a metallic cylindrical rod with a 3.8 mm round tip connected to the upper movable chamber of the testing machine traveling at a crosshead speed of 1 mm/min. The tip was parallel to the long axis of the teeth and touch 3 points on the surface of the tooth: the occlusal surface, the buccal, and the lingual walls. The failure mode was manifested by a detectable crack and was established by a recorded sharp drop in the load–deflection curve detected on the computer software (Bluehill Lite Software Instron® Instruments). Fracture load was calculated in Newton.
Flexural strength testing
For testing flexural strength 10 specimens from each tested material were prepared according to the following methodology: Stainless steel mold with a dimension of 2.5 widths × 2 length × 2 height was used to fabricate the specimen according to ISO 4049 specifications. A glass slab was placed below the mold and then the restorative material was packed into the mold-covered over the celluloid strip to obtain a finished surface then another glass slab was placed over the mold with light pressure for the removal of excess material. Polymerization of each specimen was done using a light cure machine Optilux 500 (Demetron-Kerr, Orange, CA, USA) in the 40 s each. After curing, each specimen was stored in distilled water till tested within one week.
A three-point bending flexural strength test was done using a universal mechanical testing system (Instron Corp., Canton, MA). Each specimen was placed over a 2 parallel support (2 mm in diameter each and 20 mm apart). The load with a speed of 0.75 mm\min was then applied from a 2 mm rod placed in the center between the 2 supports. The maximum force (N) exerted on the specimen before being subjected to fracture was recorded. The following equation was used for the calculation of the flexural strength (σ):
P: is the maximal force exerted on the specimens. S: is the distance between the supports (20 mm).
b and h are the widths in mm and the heights in mm of the specimen, respectively, measured immediately before testing.
Statistical analysis
Weibull analysis was used for statistically analyzing the Fracture Resistance (N) and Flexural Strength (MPa) data (R4, R Foundation for Statistical Computing, Vienna, Austria). Its parameters were calculated by Wald estimation, and pivotal confidence bounds were calculated with Monte Carlo simulation. The different groups were compared at the characteristic strength (63.2% probability of failure and 10% probability of failure) (α = 0.05).
Results
Results of fracture resistance and flexural strength are presented in Table 2 and Fig. 2. regarding fracture resistance, when using Weibull characteristic strength, no difference between all tested groups was found. However, when using P10 (estimation at 10% probability of failure) Exf showed a significantly higher fracture resistance compared to FZ3. For Flexural strength, Exf revealed a significantly higher Weibull characteristic strength compared to FZ3, while an insignificant difference between groups resulted in P10. Overall, for both fracture resistance and flexural strength, Exf showed the highest Weibull modulus which indicates reliable results for Exf.

The Weibull probability plot of the Fracture resistance (N) and flexural strength (MPa) of tested groups. The horizontal line at 63.2% probability of failure was added for comparison between the groups. Air: Alert composite, Exf: Ever X Flow-, and FZ3: Nanocomposite
Discussion
The restoration of endodontically treated teeth requires special attention to restoring their function and aesthetics (Baba et al. 2017). The most common sequelae of restoring endodontically treated teeth are fractures either vertical or cuspal fractures. The incidence of these fractures in many types of research may range from 13 to 15% (Toure et al. 2011; Mehta and Millar 2008) and in some research it reached up to 28% (Chen et al. 2008). Premolars especially with endodontic MOD cavities are more susceptible to cuspal fracture after cusp deflection during function. It was noticed that the loss of the marginal walls makes these teeth severely prone to fracture (Wu et al. 2004; Belli et al. 2006). Larson et al. reported that occlusal preparation decreases the fracture strength of the tooth by about 14–44%, while MOD preparation decreases the fracture strength by about 20–63% (Soares et al. 2008). For these reasons, premolar teeth with MOD cavities were included in the present study to represent the worst scenario as MOD cavities will decrease the fracture resistance.
Fracture resistance is the most examined for the in-vitro studies for the evaluation of the strength of different materials. Many factors can affect the result of the studies concerning fracture resistance. That includes the method of tooth mounting, type of load application device, and crosshead speed (Al-Makramani et al. 2013). Fracture resistance was tested using a universal testing machine with the help of a 6 mm stainless steel sphere by applying an axial compressive load directed toward the center of the occlusal surface. Several studies have claimed that the use of stainless steel spheres is optimum for use as it creates a uniform contact with both functional and non-functional cusps, in this study a stainless-steel bar with a 3.8 mm diameter ball end was used to contact both buccal, palatal cusp ridges, and the restoration’s center in premolar teeth with equal distance (Zarow et al. 2020). Moreover, the same idea of three-point contact was used in the current study. The load applied was in the direction of the long axis, this was by numerous studies that have used the same direction to test the fracture resistance of restorative systems (Belli et al. 2006; Nasr and Fawzy 2017).
As a result of the marked improvement in the physical and esthetic properties of advanced restorations, the resin composite becomes one of the primary choices for direct restoration. Moreover, it is not advocated for use in large restorations as its unable to reinforce the weekend tooth structure (Badakar et al. 2011). Accordingly, nano-filled composites were developed by incorporating nanometer particles into the resin matrix (Jain and Wadkar 2015). As compared to conventional composites, nanocomposites improved the abrasion resistance, they also own a greater modulus of elasticity, and higher impact, flexural, and tensile strengths (Sachdeva et al. 2015). Fiber reinforcement resin composite is a group of materials that have high strength and toughness that allow them to be used in many applications in dentistry. It was claimed that these materials can prevent crack propagation. The short fiber-reinforced resin composite was introduced to dentistry as bulk dentine replacement material. It is composed of short E-glass fiber and inorganic fillers embedded in a polymer network matrix (bis-GMA, TEGDMA, and PMMA) (Garoushi et al. 2006).
Two different commercially available short fiber reinforced composites that are especially used in stress-bearing areas were evaluated in this study regarding their fracture resistance and flexural strength when applied in MOD cavities of endodontically treated teeth. In this study, the use of conventional composite overlaying Ever X flow was recommended by many authors, especially in large cavities with high stress-bearing areas. This biomimetic technique allows for more stress distribution and decreasing in polymerization shrinkage (Goda and Abogabal 2020; Tsujimoto et al. 2016).
Although, ANOVA tests are the most popular, however, reporting the results using Weibull analysis was recommended by many authors (Armstrong et al. 2017; Abdou et al. 2021). Weibull analysis can help determine the reliability of the tested parameter. For comparison between tested groups, some authors report the comparison at “α” (Abdou et al. 2021) and others report at P10. Both are common methods of reporting and recommended to report the comparison of both parameters based on ISO standards (Tichy et al. 2020).
Several studies evaluated the effect of fiber-reinforced resin composite on the teeth strength, their results varied according to the type of fiber used, the technique of fiber insertion, and the test method applied (Fennis et al. 2005; Garoushi et al. 2013; Shafiei et al. 2014; Abouelleil et al. 2015; Garoushi et al. 2015). According to the results obtained from this current study, EverX flow had statistically the highest fracture resistance and flexural strength when compared to the other types of resin composite. On the other hand, Alert has more fracture resistance and flexural strength when compared to nano-filled resin composite even though the difference between them was statistically insignificant. These findings were following that of previous studies which show superior fracture resistance and flexural strength owing to short fiber-reinforced resin composite when compared to bulk fill resin composites or conventional composites (Garoushi et al. 2013; Abouelleil et al. 2015). The superior effect of EverX flow may be explained by its unique structure which contains E-glass fiber fillers that approximately equal to or slightly exceed the critical fiber length, this results in random orientation of these shot fibers inside the restorations. This randomly oriented short fiber in addition to the low density of the polymer matrix increases the ability of the restoration to resist fracture and also improves the transformation of stresses from the matrix to the fibers (Moosavi et al. 2012; Garoushi et al. 2015). On the other hand, adequate fiber length enhances proper adhesion between the fiber and the polymer matrix, this good adhesion with minimal voids improves the strength of the composite (Lassila et al. 2020). In addition, several authors claimed that short fiber-reinforced composite can react more naturally as it had more dentine-like fracture resistance which is the case in EverX flow (Garoushi et al. 2015; Fennis et al. 2005).
Other possible explanations could be the chemical bond between the resin and the fiber and also the properties of the fiber itself. The presence of leno weave in the fiber of the EverX flow acts as a barrier to crack propagation and thus increases the crack resistance and decreases the shrinkage stress (Mohan et al. 2019). Each fiber act separately as a crack stopper by absorbing the stress forces applied to the matrix and thus preserving the structural integrity of the tooth and decreasing the failure mode. On the other hand, part of the composite was replaced by the fiber which result in a diminishing of the volumetric contraction of the resin (Ayad et al. 2010).
On contrary, Fráter et al. (2014) demonstrated that there was no statistical difference in fracture toughness between short fiber-reinforced resin composite and conventional composite material. Moreover, Atalay et al. (2016) stated that EverX was not significantly different from other tested restorative materials in fracture resistance. This contradiction may be accredited to the difference in material application, the difference in sample preparation, or may be related to the variance in the type of adhesive used.
According to the result of this study, the EverX flow resin composite shows higher fracture resistance in contrast to the Alert. The fiber length and diameter have a great effect on the distribution of forces among the polymer matrix, EverX flow has a fiber length of 200–300 µm and a diameter of 6 µm while Alert has a fiber length of 20–60 µm and diameter of 7 µm. Thus, EverX flow has a longer fiber length with a shorter diameter that approximates the range of the recorded critical fiber length. This allows the EverX flow to act as a biomimetic restoration that reproduces a similar layer as in the natural teeth (Lassila et al. 2020).
Flexural strength resembles the flexibility of the materials, which means that the high flexural strength of the material indicates brittle properties and high hardness (El-Shekeil et al. 2012). According to the result of this study nanocomposites show the lowest flexural strength. On the other hand, EverX flow was statistically higher in flexural strength than Nanocomposite. Benkhelladi et al. 2020 stated that the addition of fibers increased the flexural properties of the composites, they also noticed that the incorporation of more than 40 wt% fiber in the composite improves its mechanical properties. All the 3 tested composite types have fiber content that exceeds the recommended fiber percentage. However, the low flexural strength of nanocomposite may be attributed to the size of the fiber incorporated in its matrix, claiming to its nano size, these nanofibers started to form bundles or clusters that create mechanical weak points in the composite and led to a decrease in conversion rate and thus lower the mechanical properties of the material (Badakar et al. 2011; Vidotti et al. 2015).
The superior strength outcome of the EverX flow in comparison to Alert and nanocomposite may be appertaining to the size and weight of short fibers incorporated in the matrix that impair the bonding resistance. Accordingly, the null hypothesis was rejected as EverX flow short-fiber-reinforced resin composite resulted in improved fracture resistance of MOD restored cavities.
Conclusions
Based on the finding of the present study, it can be concluded that the commercially available short-fiber reinforcement composite has adequate fracture resistance and flexural strength which promote it to be a suitable material for the restoration of endodontically treated teeth with a large cavities.
Recommendations
Further studies must be done with the inclusion of thermocycling and water storage tests to further mimic the in vivo conditions in order to evaluate the plasticizing effect of these tests on different types of fiber-reinforced composite.
Availability of data and materials
The raw data required to reproduce these findings are available upon reasonable request from the corresponding author. The processed data required to reproduce these findings are available upon reasonable request from the corresponding author.
Abbreviations
- MOD:
-
Mesio-Occluso-Distal cavities
- ETT:
-
Endodontically treated teeth
- CEJ:
-
Cementoenamel junction
- Alr:
-
Alert fiber-reinforced resin composite
- Exf:
-
Ever X Fiber-reinforced composite
- FZ3:
-
Filtek Z350 nano-filled resin composite
References
Abdou A, Takagaki T, Alghamdi A, Tichy A, Nikaido T, Tagami J (2021) Bonding performance of dispersed filler resin composite cad/cam blocks with different surface treatment protocols. Dent Mater J 40:209–219. https://doi.org/10.4012/dmj.2020-049
Abouelleil H, Pradelle N, Villat C, Attik N, Colon P, Grosgogeat B (2015) Comparison of mechanical properties of a new fiber-reinforced composite and bulk filling composite. Restore Dent Endod 40(4):262–270. https://doi.org/10.5395/rde.2015.40.4.262
Al-Makramani BM, Razak AA, Ng MY, Ying SY, Al-Sanabani FA (2013) Effect of restorative techniques on fracture resistance of endodontically treated premolars. Open J Stomatol 3(07):379. https://doi.org/10.4236/ojst.2013.37064
Armstrong S, Breschi L, Özcan M, Pfefferkorn F, Ferrari M, Van Meerbeek B (2017) Academy of dental materials guidance on in vitro testing of dental composite bonding effectiveness to dentin/enamel using micro-tensile bond strength (μTBS) approach. Dent. Mater. 33:133–143. https://doi.org/10.1016/j.dental.2016.11.015
Atalay C, Yazici AR, Horuztepe A, Nagas E, Ertan A, Ozgunaltay G (2016) Fracture resistance of endodontically treated teeth restored with bulk fill, bulk fill flowable, fiber-reinforced, and conventional resin composite. Oper Dent 41(5):E131–E140. https://doi.org/10.2341/15-320-L
Ayad MF, Maghrabi AA, Garcia-Godoy F (2010) Resin composite polyethylene fiber reinforcement: effect on fracture resistance of weakened marginal ridges. Am J Dent 23(3):133
Baba NZ, White SN, Bogen G (2017) Restoration of endodontically treated teeth. In: Endodontic prognosis. Springer, Cham, pp 161–192. https://doi.org/10.1007/978-3-319-42412-5_10
Badakar CM, Shashibhushan KK, Naik NS, Reddy VV (2011) Fracture resistance of microhybrid composite, nanocomposite and fiber-reinforced composite used for incisal edge restoration. Dent Traumatol 27(3):225–229. https://doi.org/10.1111/j.1600-9657.2011.00990.x
Belli S, Cobankara FK, Eraslan O, Eskitascioglu G, Kabhari V (2006) The effect of fiber insertion on fracture resistance of endodontically-treated molars with MOD cavity and reattached fracture lingual cusps. J Biomed Mater Res Part B Biomater 79:35–41. https://doi.org/10.1002/jbm.b.30508
Benkhelladi A, Laouici H, Bouchoucha A (2020) Tensile and flexural properties of polymer composites reinforced by flax, jute, and sisal fibres. J Adv Manuf Technol 108(3):895–916. https://doi.org/10.1007/s00170-020-05427-2
Bonilla ED, Mardirossian G, Caputo AA (2001) Ftoughness of posterior resin composites. Quintessence Int 32(3):206–210
Chen SC, Chueh LH, Hsiao CK et al (2008) First untoward events and reasons for tooth extraction after nonsurgical endodontic treatment in Taiwan. J Endod 34:671–674. https://doi.org/10.1016/j.joen.2008.03.016
El-Shekeil YA, Sapuan SM, Abdan K, Zainudin ES (2012) Influence of fiber content on the mechanical and thermal properties of Kenaf fiber reinforced thermoplastic polyurethane composites. Mater Des 40:299–303. https://doi.org/10.1016/J.MATDES.2014.01.047
Fennis WM, Tezvergil A, Kuijs RH, Lassila LV, Kreulen CM, Creugers NH et al (2005) In vitro fracture resistance of fiber-reinforced cusp-replacing composite restorations. Dent Mater 21:565–572. https://doi.org/10.1016/j.dental.2004.07.019
Fráter M, Forster A, Keresztúri M, Braunitzer G, Nagy K (2014) In vitro fracture resistance of molar teeth restored with a short fiber-reinforced composite material. J Dent 42(9):1143–1150. https://doi.org/10.1016/j.jdent.2014.05.004
Garoushi S, Lassila LV, Tezvergil A, Vallittu PK (2006) The load-bearing capacity of fiber-reinforced and particulate filler composite resin combination. J Dent 34:179–184. https://doi.org/10.1016/j.jdent.2005.05.010
Garoushi S, Sailynoja E, Vallittu PK, Lassila L (2013) Physical properties and depth of cure of a new short fiber-reinforced composite. Dent Mat 29(8):835–841. https://doi.org/10.1016/j.dental.2013.04.016
Garoushi SK, Hatem M, Lassila LVJ, Vallittu PK (2015) The effect of short fiber composite base on microleakage and load-bearing capacity of posterior restorations. Acta Biomater Odonto Scand 1(1):6–12. https://doi.org/10.3109/23337931.2015.1017576
Garoushi S, Gargoum A, Vallittu PK, Lassila L (2018) Short fiber-reinforced composite restorations: A review of the current literature. J Invest Clin Dent 9:e12330. https://doi.org/10.1111/jicd.12330
Goda A, Abogabal A (2020) Efficacy of bulk fill flowable composite reinforced with short fibers in fracture resistance of restored extensive premolars cavities. Al-Azhar Assiut Dent J 3:153–172. https://doi.org/10.21608/aadj.2020.118235
Goguţă LM, Bratu D, Jivănescu A, Erimescu R, Mărcăuţeanu C (2012) Glass fibre reinforced acrylic resin complete dentures: a 5-year clinical study. Gerodontology 29(1):64–69. https://doi.org/10.1111/j.1741-2358.2010.00385.x
Hannig C, Westphal C, Becker K, Attin T (2005) Fracture resistance of endodontically treated maxillary premolars restored with CAD/CAM ceramic inlays. J Prosthet Dent 94(4):342–349. https://doi.org/10.1016/j.prosdent.2005.08.004
Jain N, Wadkar A (2015) Effect of nanofiller technology on surface properties of nano filled and nanohybrid composites. Int J Dent Oral Health. https://doi.org/10.16966/2378-7090.103
Kalburge V, Yakub SS, Kalburge J, Hiremath H, Chandurkar A (2013) A comparative evaluation of fracture resistance of endodontically treated teeth, with variable marginal ridge thicknesses, restored with composite resin and composite resin reinforced with Ribbond: an in vitro study. Indian J Dent Res 24(2):193–198. https://doi.org/10.4103/0970-9290.116676
Kumar A, Tekriwal S, Rajkumar B, Gupta V, Rastogi R (2016) A review on fibre reinforced composite resins. Ann Prosthodont Restor Dent 2(1):11–16
Lassila L, Keulemans F, Vallittu PK, Garoushi S (2020) Characterization of restorative short-fiber reinforced dental composites. Dent Mat J 39(6):992. https://doi.org/10.4012/dmj.2019-088
Mehta SB, Millar BJ (2008) A comparison of the survival of fibre posts cemented with two different composite resin systems. Br Dent J 205(11):E23. https://doi.org/10.1038/sj.bdj.2008.1023
Mohan M, Ramciya KV, Baby J (2019) Comparison of fracture resistance of teeth restored with micro-hybrid, fiber-reinforced and nanohybrid composite resins an in-vitro study. Int J Recent Sci Res 10:34460–34465
Moosavi H, Zeynali M, Pour ZH (2012) Fracture resistance of premolars is restored by various types and placement techniques of resin composites. Int J Dent 201(3):973641. https://doi.org/10.1155/2012/973641
Nasr AE, Fawzy A (2017) Fracture resistance of endodontically treated teeth restored with four different restorative technologies. Egypt Dent J 63:1659–1668. https://doi.org/10.21608/edj.2017.74562
Ozsevik AS, Yildirim C, Aydin U, Culha E, Surmelioglu D (2015) Effect of fiber-reinforced composite on the fracture resistance of endodontically treated teeth. Aust Endod J. 42:82–87. https://doi.org/10.1111/aej.12136
Paidi SK, Yalavarthi RS, Kalluri S, Sharma S, Modalavalasa H, Tedlapu SK (2017) Comparative study of flexural strength and fracture resistance of two different types of provisional restorative materials reinforced with two different fibers—an in vitro study. Int J Curr Res 9(6):52688–52694
Sachdeva S, Kapoor P, Tamrakar AK, Noor R (2015) Nanocomposite dental resins: an overview. Ann Dent Spec 3(2):52–55
Shafiei F, Tavangar MS, Ghahramani Y, Fattah Z (2014) Fracture resistance of endodontically treated maxillary premolars restored by silorane-based composite with or without fiber or nano ionomer. J Adv Prosthodont 6:200–206. https://doi.org/10.4047/jap.2014.6.3.200
Soares PV, Santos-Filho PC, Martins LR, Soares CJ (2008) Influence of restorative technique on the biomechanical behavior of endodontically treated maxillary premolars. Part I: fracture resistance and fracture mode. J Prosthet Dent 99(1):30–7. https://doi.org/10.1016/S0022-3913(08)60006-2
Taha NA, Palamara JE, Messer HH (2009) Cuspal deflection, strain, and microleakage of endodontically treated premolar teeth restored with direct resin composites. J Dent 37(9):724–730. https://doi.org/10.1016/j.jdent.2009.05.027
Tichy A, Hosaka K, Abdou A, Nakajima M, Tagami J (2020) Degree of conversion contributes to dentin bonding durability of contemporary universal adhesives. Oper Dent 40:556–566. https://doi.org/10.2341/19-165-L
Toure B, Faye B, Kane AW et al (2011) Analysis of reasons for extraction of endodontically treated teeth: a prospective study. J Endod 37:1512–1515. https://doi.org/10.1016/j.joen.2011.07.002
Tsujimoto A, Barkmeier WW, Takamizawa T (2016) Relationship between mechanical properties and bond durability of short fiber- reinforced resin composite with universal adhesive. Eur J Oral Sci 124:480–489
Vidotti HA, Manso AP, Leung V, do Valle AL, Ko F, Carvalho RM (2015) Flexural properties of experimental nanofiber-reinforced composite are affected by resin composition and nanofiber/resin ratio. Dent Mater 31:1132–114. https://doi.org/10.1016/j.dental.2015.06.018
Wu MK, van der Sluis LW, Wesselink PR (2004) Comparison of mandibular premolars and canine with respect to their resistance to vertical root fracture. J Dent 32:265–268. https://doi.org/10.1016/j.jdent.2003.12.002
Zarow M, Vadini M, Chojnacka-Brozek A, Szczeklik K, Milewski G, Biferi V, Darcangelo C, De Angelis F (2020) Effect of fiber posts on stress distribution of endodontically treated upper premolars. Nanomaterials 10:1708. https://doi.org/10.3390/nano10091708
Acknowledgements
Not applicable.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
WG: Conceptualization, Methodology, Investigation, Writing-original draft. AA: Formal analysis, Visualization. GS: Conceptualization, Investigation, Writing-original draft. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The current research was organized by the Ethics of the World Medical Association, following the assumption conveyed in the Declaration of Helsinki. The approval of this research was earned from the local Ethical Committee of the National Research Centre, Cairo, Egypt with approval number (3435062021).
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gamal, W., Abdou, A. & Salem, G.A. Fracture resistance and flexural strength of endodontically treated teeth restored by different short fiber resin composites: a preclinical study. Bull Natl Res Cent 46, 276 (2022). https://doi.org/10.1186/s42269-022-00964-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42269-022-00964-0