
Abstract
Background
Injection for vaccinations is the most prevalent source of iatrogenic pain in infants. The facilitated rocking movement is a new technique which is to be evaluated to reduce vaccination-induced pain in newborns and young infants. Hence, the present study was designed to study the effect of facilitated rocking movement in reducing vaccination-induced pain in young infants.
Method
A total of 70 infants < 6 months attending vaccination clinic, full-term born babies with weight > 2.5 kg and clinically well infants were enrolled and randomized in two equal groups, i.e., facilitated rocking movement (treatment/group 1) and classical holding group (control/group 2).
Results
Both the groups were comparable and found no significant (p > 0.05) difference as regards education, occupation, socioeconomic status, type and number of deliveries, gestational age of mother as well as birth weight, gender and hemodynamic parameters of infants. The crying time was significantly (p = 0.0001) lower among children of group 1 (35.79 ± 5.12 s) than group 2 (59.71 ± 7.93 s). There was a significant difference (p = 0.0001) in NIPS score among the groups after baseline. At baseline, mild severity of pain was observed in the majority of children in both groups (92.9% in each), while at 1 min after prick mild severity of pain was more in group 1 (92.9%) than in group 2 (28.6%), (p = 0.0001).
Conclusion
The assisted rocking movement proved more helpful than the traditional holding position in alleviating pain caused by vaccinations in infants aged less than 6 months. As a result of its easy, cheap and noninvasive application, this position can be utilized in combination with pharmacological techniques during painful procedures. Further ascertainment by comparing other techniques such as the analgesic effects of sucrose, expressed breast milk and breast-feeding should be carried out.
Similar content being viewed by others


Background
Pain is a complex, unique, subjective and universal finding in infants. Routine injections without pain control are the most common painful treatments performed throughout infancy. Vaccinations are initially given to infants when they are very young (Kucukoglu et al. 2015). Although sweet solutions and breast-feeding are widely suggested for decreasing acute immunization discomfort, their usage in clinical practice has limits. When compared to psychological or pharmacological therapies for pain alleviation, physical interventions are the least expensive and easiest to be implemented (Reis et al. 1998). Swaddling, shushing, swinging, sucking and posture are typical ways for reducing acute vaccination pain. However, few studies have been conducted on the different physical treatments for reducing acute vaccination discomfort in young babies. So far, the effects of physical interventions on vaccine responses have been disputed (Harrington et al. 2012; MacLaren and Cohen 2007).
Rocking, a physical intervention method, has been used for centuries to relax babies and toddlers or to promote their sleep. The facilitated rocking movement is a new technique which is to be evaluated to reduce vaccination-induced pain in newborns and young infants. In this technique, the newborn after vaccination is given side-to-side rocking movement to reduce the level of pain arousal in newborn. It has been stated that it stimulates the child's natural regulatory mechanisms, prevents unpleasant impulses from the outside environment and reduces discomfort felt by the infant by allowing heat and tactile sensations (Omlin et al. 2018).
Furthermore, this method stabilizes infant’s physiological parameters and thus aids them in gaining a feeling of safety based on the position, supports their motor development and preserves their energy. Hence, the current study was undertaken to compare the effect of facilitated rocking movement vis-a-vis classical holding position as a pain-relieving strategy after vaccination in young infants (< 6 months) and also to compare the severity of pain during and after vaccination in young infants < 6 months.
Methods
This randomized controlled trial adheres to CONSORT guidelines and was carried out in the Department of Pediatrics, Santosh Medical College and Hospital, Ghaziabad, UP, during a period of 1 year from May 2019 to May 2020. The study was submitted and approved by the institutional ethics committee of Santosh Medical College & Hospital. Informed written consent was taken from the parents. Totally, 70 infants < 6 months of either sex attending vaccination clinic, full-term born babies with weight > 2.5 kg and clinically well infants were enrolled in the study. Child with any history of trauma, neurological disease, any sick babies and newborns who had congenital malformations, requiring positive pressure ventilation support, and received pain-relieving and sedative treatment were excluded from the study. A detailed antenatal/postnatal history was elicited from the parents, and full general examination and anthropometry of the enrolled babies were done. Intramuscular injection of the due vaccine was given via 2-ml syringe. Anterolateral aspect of mid-thigh was cleaned with 70% alcohol for vaccination. Deep intramuscular injection was given perpendicular to the surface of skin as quickly as possible.
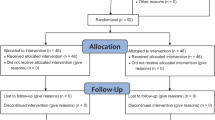
All the selected children were randomized in two different groups by random numbers, into treatment and control group, to receive either facilitated rocking movements after receiving vaccination or classical holding position. Comparison was restricted to the first vaccination visit only. Blinding was not possible in this study since the observer had to observe immediate response soon after the intervention.
Group 1—Facilitated rocking movement (treatment group): Immediately after the vaccine was injected, the vaccinator holds the baby’s head and shoulder 45 degree from the table with his left hand without lifting the hip from the table; the vaccinator then rocked the baby sideways (horizontal direction) in the maximum permissible range for 1 min. While the rocking movement was being done, the vaccinator would assess cry, behavior, facial expression and score as per NIPS score.
Group 2—Classical holding position (control group): Immediately after the vaccine was injected to babies falling in this group, the vaccinators lifted the baby in his arms and assess the cry, behavior, facial expression as per the Neonatal Infant Pain Scale (NIPS) score noted by observer. The NIPS was used to evaluate pain at the baseline state, at the impact of needle, and 30 s and 1 min after the prick.
The NIPS is divided into one physiological part and five behavioral sections, which include face expression, cry, breathing pattern, arms and legs, and level of arousal. The cry portion is for 0 to 2 points, while the other sections are worth 0 to 1 point. The total score ranges from 0 to 7, with a higher score indicating more discomfort. Using this approach, a statistical examination was performed, and a p value was obtained.
Statistical analysis
The data were expressed in the form of frequencies, percentages and mean standard deviation. To compare categorical variables between groups, the chi-square test was utilized. To compare continuous variables between groups, the unpaired t test was employed. The p value of 0.05 was deemed significant. SPSS 16.0 was used for all of the analysis (Chicago, Inc., USA).
Results
A total of 70 children were enrolled in the study and randomly divided into two groups of 35 infants in each group. Both the groups were comparable and found no significant (p > 0.05) difference as regards education, occupation and socioeconomic status (SES) of mother as well as type and number of deliveries as shown in Table 1. The mean gestational age of mother of group 1 and group 2 was 36.06 ± 2.85 weeks and 35.97 ± 2.89 weeks, respectively (p > 0.05).
There was no significant (p > 0.05) difference in birth weight and sex distribution of infants between two groups as shown in Table 2.
Both the groups were comparable and found no significant (p > 0.05) difference in hemodynamic parameters of infants before, during and after the procedure as depicted in Fig. 1.

Comparison of hemodynamic parameters before, during and after the procedure between two groups
The crying time was significantly (p = 0.0001) lower among children of facilitated rocking movement (35.79 ± 5.12 s) than classical holding position (59.71 ± 7.93 s). Figure 2 shows the comparison of NIPS score between the groups at various time periods, and we found significant (p = 0.0001) difference in NIPS score between the groups after baseline (Fig. 2).

Comparison of NIPS score between the groups at baseline to subsequent time periods
Mild severity of pain was in the majority of children in both facilitated rocking movement (92.9%) and classical holding position (92.9%) at baseline. Mild severity of pain was 92.9% in children of facilitated rocking movement and in 28.6% of classical holding position at 1 min after prick. There was a significant (p = 0.0001) difference in severity of pain between the groups after baseline as shown in Table 3.
Discussion
The measurement of newborn pain remains a difficulty for healthcare workers. There is a greater emphasis on newborn pain, its evaluation and therapy of acute pain caused by unpleasant procedures in clinical settings. To properly measure neonates' pain perception, a range of pain assessment methodologies, including behavior observation and physiological techniques, have been utilized (Johnston and Strada 1986). The present study was carried out to compare the effect of facilitated rocking movement vis-a-vis classical holding position as a pain-relieving strategy after vaccination in young infants (< 6 months). In this study, both the groups were comparable and found no significant (p > 0.05) difference in regards to socio-demographic (education, occupation and SES) and obstetric characteristics (type of delivery, parity, gestational age) of mothers. More than half of the deliveries in both group 1 (61.4%) and group 2 (58.6%) were vaginal (p > 0.05) which is similar to Sujatha et al.’s study (2017).
Also, both the groups were comparable and found no significant (p > 0.05) difference in birth weight and sex distribution of infants. Half of infants in control group (56; 52.8%) and (62; 56.3%) in experimental group were in 6–12 weeks of age-group. More than half of children in both group 1 (60%) and group 2 (58.6%) were males (p > 0.05). A newborn's response to discomfort may include physiological alterations; these changes should be observed until the parameters return to normal during the process (Lago et al. 2009). Physiological symptoms induced by painful stimuli reveal the body's overall stress level. Although the most common physiological indicators, such as heart rate, blood pressure, respiration and oxygen saturation, are utilized to measure pain caused by acute operations, hormonal and metabolic variables are also employed. In terms of fever, pulse, respiration and oxygen saturation before and after the surgery, there was no significant difference between the groups (p > 0.05). During the operation, the respiration rate of infants in the control group was considerably greater than that of neonates in the treatment group (p < 0.05). As a result, in the current investigation, all of the factors that may cause external bias were matched.
Crying was employed as an indication of pain in the current investigation. Cry time was significantly reduced in the assisted rocking movement group compared to the conventional holding posture. The research intervention was related to total cry time, and there was a substantially lower total mean cry time in newborns getting assisted rocking movement than in neonates receiving traditional holding posture. The analgesic effects of sucrose, expressed breast milk and breast-feeding during heel pricks were compared in a research by Bilgen et al. (2001). Breast-feeding before, during and after heel pricking decreased screaming and grimacing and avoided a rise in heart rate in term newborns when compared to swaddled babies in their cribs, according to Gray et al. (2002). Henderson (2015) discovered that giving infants a few drops of 24 percent sucrose solution and briefly exposing them to radiant warmth, which mimics some aspects of breast-feeding, before vaccination resulted in a 50% reduction in the amount of time the newborns cried and grimaced after the vaccination. However, in a study of vaccine administration conducted by Kaur et al. (2009), it was discovered that infants in the experimental group (infant placed on breast while injecting vaccine) had a mean duration of cry of 49.3 s, whereas infants in the control group (infant not placed on breast while injecting vaccine) had a mean duration of cry of 87.4 s. The t test findings indicated that infants in the experimental group cried for substantially less time than infants in the control group (p < 0.01).
The Neonatal Infant Pain Scale (NIPS) was employed in the current investigation to objectively assess the pain reported by the neonates while taking behavioral responses into consideration. At baseline, we observed that the majority of children in both groups had mild pain, with children in group 1 having more mild pain than children in group 2. As a result, there was a significant (p = 0.0001) difference in pain severity across the groups after baseline. These findings are consistent with the findings of Sujatha et al. (2017). Pain severity should be assessed using multidimensional pain measures appropriate for baby circumstances, on which validity and reliability studies have been done to assess pain experienced by neonates (Akyürek and Conk 2006). Individualized developmental care approaches and an environment that promotes the infant's developing skills while also allowing the newborn to deal with stress and discomfort should be established (Dağoğlu 2008). When the literature was studied, it was discovered that the facilitated tucking posture was a successful approach for reducing various procedural pains (such as heel stick, suctioning and venipuncture) in babies (Ward-Larson et al. 2004; Axelin et al. 2006).
One of the research's weaknesses was the limited sample size and short study time. Studies with a bigger sample size and a longer research time are necessary to get more robust results.
Conclusions
The assisted rocking movement proved more helpful than the traditional holding position in alleviating pain caused by vaccinations in infants aged less than 6 months. As a result of its easy, cheap and noninvasive application, this position can be utilized in combination with pharmacological methods during painful procedures. Further ascertainment by comparing other techniques such as the analgesic effects of sucrose, expressed breast milk and breast-feeding should be carried out.
Availability of data and materials
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- NIPS:
-
Neonatal Infant Pain Scale
- UP:
-
Uttar Pradesh
References
Akyürek B, Conk Z (2006) The efficacy of non-pharmacological pain relief methods in injection: application to newborns. Ege Üniversitesi Hemşirelik Yüksek Okulu Dergisi 22:1–17
Axelin A, Salanterä S, Lehtonen L (2006) Facilitated tucking by parents in pain management of preterm infants: a randomized crossover trial. Early Hum Dev 82:241–247
Bilgen H, Ozek E, Cebeci D, Ors R (2001) Comparison of sucrose, expressed breast milk, and breast feeding on neonatal responses to heel prick. J Pain 2(5):301–305
Dağoğlu T (2008) Newborn development and enviromental factors. In: Dağoğlu T, Görak G (eds) Basic neonatology and nursing principles. Nobel Medical Publications, Istanbul, pp 759–67
Gray L et al (2002) Breast feeding is analgesic in healthy newborns. Pediatrics 109(4):590–593
Harrington JW, Logan S, Harwell C et al (2012) Effective analgesia using physical interventions for infant immunizations. Pediatrics 129(5):815–822
Henderson D (2015) Sucrose plus radiant warmth relieves newborns' pain. Pediatrics
Johnston CC, Strada ME (1986) Acute pain response in infants: a multidimensional description. Pain 24:373–382
Kaur L, Kaur S, Kalia R, Bharti B (2009) Analgesic effect of breast feeding in infants during immunization injections: randomized control trial. https://nrfninechd.com/analgesic-effect-of-breast-feeding-in-infants-during-immunization-injections-randomized-control-trial/
Kucukoglu S, Kurt S, Aytekin A (2015) The effect of the facilitated tucking position in reducing vaccination-induced pain in newborns. Ital J Pediatr 41:61
Lago P, Garetti E, Merazzi D, Pieragostini L, Ancora G, Pirella A et al (2009) Guidelines for procedural pain in the newborn. Acta Paediatr 98:932–939
MacLaren JE, Cohen LL (2007) Interventions for paediatric procedure-related pain in primary care. Paediatr Child Health 12(2):111–116
Omlin X, Crivelli F, Näf M et al (2018) The effect of a slowly rocking bed on sleep. Sci Rep 8(1):2156
Reis EC, Jacobson RM, Tarbell S, Weniger BG (1998) Taking the sting out of shots: control of vaccination-associated pain and adverse reactions. Pediatr Ann 27(6):375–386
Sujatha S, Rebecca S, Christopher A (2017) Sucrose and facilitated tucking for pain among neonates receiving vaccination, Puducherry. Int J Pharm Clin Res 9(3):260–263
Ward-Larson C, Horn RA, Gosnell F (2004) The efficacy of facilitated tucking forrelieving procedural pain of endotracheal suctioning in very lowbirthweight infants. MCN Am J Matern Child Nurs 29:151–156
Acknowledgements
Not applicable.
Funding
Nil.
Author information
Authors and Affiliations
Contributions
JY collected the data; AA contributed to idea of research, writing and proofreading; VDS analyzed and interpreted the data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was submitted and approved by the institutional ethics committee of Santosh Medical College & Hospital, Ghaziabad, Uttar Pradesh, and written informed consent from parents to participate in study was taken.
Consent for publication
Consent for publication from parent was taken.
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yadav, J.P., Agrawal, A. & Sawant, V.D. Effect of facilitated rocking movement in reducing vaccination-induced pain in young infants: a randomized control trial. Bull Natl Res Cent 46, 117 (2022). https://doi.org/10.1186/s42269-022-00807-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42269-022-00807-y