
Abstract
Background
This randomized, double-blind study was designed to compare single injection pectoral nerve block (Pecs I and Pecs II) versus local anesthetic infiltration for ambulatory breast augmentation under monitored anesthesia care (MAC).
Methods
In this randomized, double-blind, prospective study, 80 patients scheduled for breast augmentation under MAC using dexmedetomidine were divided into two groups. Pecs group: Ultrasound-guided pectoral nerve block was performed on both sides of the chest. Local anesthetic (LA) group: Local anesthetic infiltration was performed in the desired plane and skin incision site of each breast. The number of patients converted to general anesthesia was calculated. Postoperative pain intensity was measured using visual analog scale (VAS), and morphine consumption in the first 24 h and patient satisfaction were measured.
Results
The success rate of the ultrasound-guided block versus local infiltration to complete surgery without conversion to general anesthesia was statistically non-significant. VAS, time of the first analgesia, and total morphine consumption were statistically significantly different between the two studied groups with significantly higher values in the LA group than Pecs group. Patient satisfaction was significantly higher in the Pecs group than in the LA group.
Conclusion
The combination of Pecs blocks with MAC is helpful in patients undergoing breast augmentation.
Similar content being viewed by others


Background
Breast augmentation surgery is commonly performed on an ambulatory basis under general anesthesia (GA) or monitored anesthesia care (MAC) (Chung et al., 2012). MAC using a variety of local and regional techniques is advantageous over GA in reducing postoperative pain and avoiding complications related to GA (Song et al., 2000). However, the regional anesthesia (RA) techniques, such as intercostal nerve block, thoracic paravertebral block (TPVB), and thoracic epidural block, are invasive and associated with the risk of perioperative complications, and they are not appropriate for ambulatory surgery (Sidiropoulou et al., 2008a).
MAC with local anesthesia infiltration is a safe technique and has been established as a preferred method of perioperative analgesia in breast augmentation (Fayman et al., 2003). The ultrasound (US) pectoral nerves block (Pecs block) is a novel superficial nerve block and less invasive than the abovementioned RA techniques, which provides good perioperative analgesia for ambulatory breast surgery (Blanco, 2011). However, it has been used as adjuvant to GA (Bashandy & Abbas, 2015; Syal & Chandel, 2017) and no previous studies used it with MAC.
The aim of this study was to compare the effect of ultrasound-guided pectoral nerve block and local anesthetic infiltration during ambulatory breast augmentation under MAC with dexmedetomidine on postoperative morphine consumption (our primary outcome), pain scores, postoperative nausea and vomiting (PONV), and patients’ satisfaction.
Patient and methods
This prospective, double-blinded, randomized, parallel group study enrolled 80 healthy females American Society of Anesthesiologists (ASA) class I or II aged 21–50 years old who were scheduled for breast augmentation at the day surgery units of Ain Shams University Hospitals in Cairo, Egypt, from January 2015 through January 2018. The current study was approved by the local Ethics Committee. All the patients gave written consent. Exclusion criteria were ASA class ≥ III, contraindications to regional anesthesia (including coagulopathy and infection at the injection site), history of chronic use of opioids, body mass index (BMI) ≥ 35, uncooperative patients, and patients with known allergy to local anesthetics, opioids, NSAIDs, or paracetamol.
After arrival at the day surgery unit, patients were randomly assigned by a computer-generated list of random numbers using opaque, sealed envelopes to two groups, Pecs group (pectoral nerve block) and LA group (local anesthesia infiltration) of 30 patients each. Anesthesia management was done by an anesthesiologist who did not involve in outcome assessment. The patient and the investigator who collected the data were blinded to the study groups. All patients received supplemental oxygen through nasal prong, 3 L/min. Mean arterial blood pressure (MAP), heart rate (HR), respiratory rate (RR), and SpO2 were monitored during surgery.
MAC consisted of an initial infusion of dexmedetomidine loading dose of 1 μg/kg over 10 min followed by a maintenance dose of 0.2–0.7 μg/kg/h. Ultrasound-guided pectoral nerve block or local anesthetic infiltration of the surgical site was commenced when the patient was relaxed with slurred speech.
For Pecs group
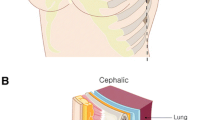
Ultrasound-guided pectoral nerve block was performed on both sides of the chest as described by Blanco (Blanco, 2011) and Blanco and colleagues (Blanco et al., 2012), using S-Nerve ultrasound apparatus (SonoSite Inc, Bothell, Washington, USA) and a 6–13-MHz linear transducer (HFL 38; SonoSite Inc). The patients were positioned supine with the ipsilateral arm abducted and externally rotated. The infraclavicular and axillary regions were cleaned with chlorhexidine; the ultrasound probe was placed infraclavicular then moved laterally to identify the pectoralis major and minor muscles just above the second rib under sterile condition. We started counting the ribs from 2nd rib under the axillary artery and maintaining the pectoralis major as a reference, and we moved distally and laterally until the lateral border of pectoralis major was reached. The needle was inserted in plane with the transducer into the fascial plane between the pectoralis muscles and 10 ml of bupivacaine 0.25% was injected. The transducer was then moved towards the axilla until the serratus anterior muscle was identified above the third and fourth ribs; the needle was then reinserted until the tip of the needle was in contact with the surface of the fourth rib. Then, 20 ml of 0.25% bupivacaine was injected beneath the serratus anterior muscle at the fourth rib in increments of 5 ml after confirming negative aspiration.
We confirmed the loss of sensation over T2–T6 of dermatomes by a pinprick test.
For LA group
Local anesthetic infiltration was performed by the surgeon using 50 ml of LA mixture in the desired plane and skin incision site of each breast. LA mixture was prepared of 15 ml of 0.5% bupivacaine, 15 ml of 2 % lidocaine, and 70 ml of normal saline with adrenaline 1:200,000.
Subsequently, the infusion dose of dexmedetomidine was increased according to the Ramsay sedation scale (Ramsay et al., 1974) (target score 3). If still insufficient analgesia, the infusion rate of the dexmedetomidine was titrated up by 25–50% of initial infusion. Insufficient analgesia was defined as expression of pain, discomfort, and/or patient movement. Heart rate (HR) and systolic blood pressure (SBP) exceeding baseline values by 20% were also considered to be signs of insufficient analgesia. Ramsay Sedation Score (sedation scale)
Clinical score | Level of sedation |
1 | Anxious, agitated, or restless |
2 | Co-operative, oriented, and tranquil |
3 | Responds to command |
4 | Asleep, but has a brisk response to light glabellar tap or loud auditory stimulus |
5 | Asleep, has a sluggish response to a light glabellar tap or loud auditory stimulus |
6 | Asleep, no response |
In both groups, conversion to general anesthesia during surgery could be performed at the patient’s request after giving rescue analgesia by fentanyl 0.5 μg/kg. The number of rescue doses was recorded.
Adverse events such as respiratory depression (respiratory rate less than 8 breaths/ min or SaO2 ≤ 95%) or significant cardiovascular depression (bradycardia, heart rate (HR) ≤ 50 bpm, hypotension, systolic blood pressure (SBP) ≤ 80 mmHg) were recorded, and the necessary interventions were performed and documented.
At the end of surgery, patients in both groups were transferred to the post-anesthesia care unit (PACU) for the first 2 h. Pain intensity was measured using VAS (1–10) at 1, 6, 12, 18, and 24 h. Postoperative pain was treated with patient-controlled intravenous morphine Pump (Accufuser). It was composed of 40 mg morphine in 100 ml saline. The PCA pumps were programmed to deliver an infusion rate of 4 ml/h and 1-ml dose as a bolus, with a lockout interval of 15 min, and total morphine consumption in the first 24 h was recorded.
Postoperative nausea, vomiting, or pruritus were recorded and treated. Patients’ satisfaction was recorded according to a satisfaction score (0 = complete dissatisfaction, 10 = most satisfaction) (Erdurmus et al., 2008).
The primary outcome variable was morphine consumption in the first 24 h. Secondary outcome measures were pain scores, intraoperative dexomedetomedine consumption, postoperative nausea and vomiting (PONV), and Patients’ satisfaction.
Statistical analysis
The primary endpoint in this study was the morphine consumption at 24 h. Based on previous studies (Sidiropoulou et al., 2008b), the average mean (+ SD) 24-h morphine consumption was 40.65 (+ 11) mg. the sample size was calculated to detect a 10-mg reduction in morphine consumption. A sample size of 21 patients per study group was calculated by a two-sided t test, with a level of significance of 0.05 and a power of 0.8. We enrolled 60 patients to allow for a 30% dropout.
The statistical analysis was performed using a standard SPSS software package version 17 (Chicago, IL). Collected data are expressed as mean (SD), number (percentage), or median and interquartile range. Chi-square test was used to compare ordinal data. The independent-sample Student’s t test was used to compare normally distributed numerical data. Mann-Whitney U test was used to compare non-normally distributed numerical data. Repeated-measures ANOVA was used to compare measurements over time (MAP, HR, RR, and Sao2). To compare the data (MAP, HR, RR, and Sao2) at each time point, t test was used. P < 0.05 is considered statistically significant.
Results
Eighty female patients undergoing breast augmentation were enrolled in this study. Twelve of them were not meeting the inclusion criteria, eight refused to participate in the study, and the remaining sixty patients were equally randomized to either the LA group (n = 30) or the Pecs group (n = 30) (Fig. 1).

Flow chart in the study
The patients’ characteristics of the two study groups are summarized in Table 1. Statistical analysis revealed non-significant differences between the two study groups as regards age, weight, ASA physical status, and the duration of surgery.
The success of the ultrasound-guided block or local anesthetic infiltration was tested by recording the number of patients who completed the surgical procedure without using general anesthesia from the start or during the procedure. It was found that only one out of thirty patients in Pecs group could not tolerate the surgery under regional block and also after giving the supplementary fentanyl doses. This patient needed to be converted to general anesthesia to complete the surgery. However, in LA group, only four out of thirty patients needed to receive general anesthesia. Comparison between the two study groups as regards the success rate of the ultrasound-guided block versus local infiltration to complete surgery without conversion to general anesthesia was statistically non-significant 3.3% in Pecs group versus 13.3 % in LA group (Table 1).
Intraoperative dexmedetomidine consumption was statistically significantly high in in the LA group (P < 0.05) (Table 1). Also, the number of intraoperative rescue doses of fentanyl between the two studied groups was significantly high LA group compared to Pecs group (Table 2).
Intraoperative heart rate, mean arterial blood pressure, and respiratory rate were lower in LA group compared to Pecs group but without significant differences (Figs. 2, 3, and 4). Complications of local anesthetic did not happen in both groups.

Intraoperative heart rate in both groups

Intraoperative mean arterial pressure in both groups

Intraoperative respiratory rate in both groups
As regards VAS, time of first analgesia, and total morphine consumption, there was statistically significantly different between the two studied groups with higher values in the LA group than in the Pecs group (Table 3).
Intraoperative patients’ vital data, postoperative complications, and patients’ satisfaction are shown in Table 4. Complications were minimal with no significant difference between the groups with respect to blood pressure, heart rate, respiratory rate, SpO2, nausea, vomiting, or pruritus. patients’ satisfaction was significantly greater in the Pecs group than in the LA group (P < 0.05) (Table 4).
Discussion
This randomized double-blind trial compared ultrasound guided pectoral nerve block and local anesthetic infiltration on perioperative analgesia during ambulatory breast augmentation and found that pectoral nerve block significantly decreased the number of patients who required intraoperative fentanyl rescue analgesia, 24-h morphine consumption with increased time of first analgesia and less postoperative pain scores. In addition, patients’ satisfaction was significantly higher in Pecs group. The incidence of adverse effects was comparable in both groups.
Pecs block is considered a safe and efficient procedure. Pecs block has no risk of sympathectomy or restrictions on the use of anticoagulants, as compared to TPVB or neuraxial blocks (Ramsay et al., 1974). Only few cases of Pecs blocks have been reported as the primary anesthesia for breast surgery and were always combined with general anesthesia. In a study, successful placement of an implantable cardiac resynchronization device was performed under Pecs I block (10 ml, 0.375% ropivacaine) combined with first and second intercostal nerve blocks (4 ml, 0.375% ropivacaine) and light intravenous sedation in a high-risk patient who was intolerable to GA and neuraxial blockade (Fujiwara et al., 2014). Also, using dexmedetomidine was beneficial to the patient due to its analgesic, sedative, anxiolytic, and sympatholyic properties. It may prolong the duration of sensory block of spinal and peripheral nerve blocks (Abdallah et al., 2016).
There were a lot of studies on the efficacy of local anesthetic infiltration as a method of intraoperative and postoperative analgesia in a variety of breast surgeries such as simple mastectomy, segmental mastectomy, breast reduction surgeries, and benign lumpectomy, and the authors noted that the reductions for both pain scores and opioid consumption were clinically insignificant and only lasted a couple of hours postoperatively (Byager et al., 2014). Similarly in our case, we also found reduction in pain scores mainly for the first 2 h post-surgery, and by the end of the 2nd hour, most of the patients demanded rescue analgesia, reflecting inadequacy of local anesthetic infiltration for post-surgical analgesia.
Both Pecs blocks and LA infiltration ensured good perioperative analgesia, but only Pecs blocks were able to provide satisfactory intraoperative and postoperative patient comfort, as indicated by less perioperative opioid consumption and superior patient satisfaction. Other advantages of Pecs block over LA infiltration is that Pecs block can be repeated if local anesthetic duration is shorter than the duration of surgery without wound’s border alteration. However, local anesthetic infiltration is contraindicated and inadequate due to presence of surgical wound with shortening the time of anesthesia due to drainage of LA solutions simultaneously with blood when bleeding is present. Therefore, increase intraoperative sedative and analgesic drug use for pain control to conclude surgery.
Conclusion
Combination of Pecs blocks with MAC is helpful in patients undergoing breast augmentation.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- LA:
-
Local anesthetic
- MAC:
-
Monitored anesthesia care
- Pecs block:
-
Pectoral nerve block
- TPVB:
-
Thoracic paravertebral block
References
Abdallah FW, Dwyer T, Chan VW, Niazi AU, Ogilvie-Harris DJ, Oldfield S, Patel R, Oh J, Brull R (2016) IV and perineural dexmedetomidine similarly prolong the duration of analgesia after interscalene brachial plexus blocka randomized, three-arm, triple-masked, placebo-controlled trial. Anesthesiology: The Journal of the American Society of Anesthesiologists. 124(3):683–695
Bashandy GM, Abbas DN (2015) Pectoral nerves I and II blocks in multimodal analgesia for breast cancer surgery: a randomized clinical trial. Regional anesthesia and pain medicine 40(1):68–74
Blanco R (2011) The ‘pecs block’: a novel technique for providing analgesia after breast surgery. Anaesthesia 66(9):847–848
Blanco R, Fajardo M, Maldonado TP (2012) Ultrasound description of Pecs II (modified Pecs I): a novel approach to breast surgery. Revista espanola de Anestesiologia y Reanimacion. 59(9):470–475
Byager N, Hansen MS, Mathiesen O, Dahl JB (2014) The analgesic effect of wound infiltration with local anaesthetics after breast surgery: a qualitative systematic review. Acta Anaesthesiologica Scandinavica 58(4):402–410
Chung K-J et al (2012) Usefulness of intravenous anesthesia using a target-controlled infusion system with local anesthesia in submuscular breast augmentation surgery. Archives of plastic surgery 39(5):540
Erdurmus M, Aydin B, Usta B, Yağcı R, Gozdemir M, Totan Y (2008) Patient comfort and surgeon satisfaction during cataract surgery using topical anesthesia with or without dexmedetomidine sedation. European journal of ophthalmology 18(3):361–367
Fayman M, Beeton A, Potgieter E, Becker PJ (2003) Comparative analysis of bupivacaine and ropivacaine for infiltration analgesia for bilateral breast surgery. Aesthetic plastic surgery 27(2):100–103
Fujiwara A, Komasawa N, Minami T (2014) Pectoral nerves (PECS) and intercostal nerve block for cardiac resynchronization therapy device implantation. Springerplus. 3(1):409
Ramsay MA, Savege TM, Simpson BR, Goodwin R (1974) Controlled sedation with alphaxalone-alphadolone. Br Med J 2:656–659
Sidiropoulou T, Buonomo O, Fabbi E, Silvi MB, Kostopanagiotou G, Sabato AF, Dauri M (2008a) A prospective comparison of continuous wound infiltration with ropivacaine versus single-injection paravertebral block after modified radical mastectomy. Anesthesia & Analgesia. 106(3):997–1001
Sidiropoulou T, Buonomo O, Fabbi E, Silvi MB, Kostopanagiotou G, Sabato AF, Dauri M (2008b) A prospective comparison of continuous wound infiltration with ropivacaine versus single-injection paravertebral block after modified radical mastectomy. Anesthesia & Analgesia. 106(3):997–1001
Song D, Greilich NB, White PF, Watcha MF, Tongier WK (2000) Recovery profiles and costs of anesthesia for outpatient unilateral inguinal herniorrhaphy. Anesthesia & Analgesia 91(4):876–881
Syal K, Chandel A (2017) Comparison of the post-operative analgesic effect of paravertebral block, pectoral nerve block and local infiltration in patients undergoing modified radical mastectomy: a randomised double-blind trial. Indian journal of anaesthesia. 61(8):643
Acknowledgements
The authors thank all their colleagues in the plastic surgery department in Ain Shams University Hospital for their help in this research.
Funding
Nil
Author information
Authors and Affiliations
Contributions
MA analyzed and interpreted the patient data. KYH was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by Ain Shams University ethics committee.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Hakim, K.Y.K., Wahba, W.Z. Single injection pectoral nerve block (Pecs I and Pecs II) versus local anesthetic infiltration for ambulatory breast augmentation combined with monitored anesthesia care. Ain-Shams J Anesthesiol 11, 18 (2019). https://doi.org/10.1186/s42077-019-0033-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42077-019-0033-y