
Abstract
Background
Thoracolumbar fractures represent a widespread injuries that can cause significant disability and strain the healthcare system. Different surgical approaches are described in the literature. This study was conducted to evaluate the fractured level inclusion in short-segment fixation of thoracolumbar junction spine fractures.
Results
Preoperative neurological deficit was reported in seven patients ranging from ASIA grade C to D. All of these patients improved to grade E by the end of the follow-up period, except for one patient who improved from grade C to D. The mean Oswestry Disability Index was 19.87%. The mean postoperative Cobb angle was 11.77° which significantly improved compared to a preoperative value of 19.37°. There was a significant improvement in the postoperative anterior and posterior vertebral body height compared to the preoperative values. The vertebral body compression ratio significantly improved during the postoperative period to a mean of 84% compared to 76% preoperative.
Conclusions
There was significant improvement of the postoperative values of the mean Cobb angle, the anterior and the posterior vertebral body height as well as the vertebral body compression ratio compared to the preoperative values.
Similar content being viewed by others

Background
Thoracolumbar spine fractures are considered as widespread injuries that can cause significant disability, deformity and neurological deficit. They constitute a broad range of injuries from simple undisplaced fractures to complex fracture dislocations [1].
More than half of these fractures are unstable and can lead to substantial disability, deformity and neurological deficit [2].
The (TLJ) thoracolumbar junction (T11–L2) is distinctively located between the rigid thoracic spine and the mobile lumbar spine. This transition exposes this region to substantial biomechanical stress. Hence, the thoracolumbar junction is the most affected area of the vertebral column [3].
In the past spine fractures were treated with external casting and immobilization but with the advances in medical technology and the increasing experience in dealing with spinal injuries, the impetus for developing an algorithm and definitive approaches in the management of patients suffering from these devastating injuries was provided. The management of spinal injuries is continuously evolving. Many different approaches exist in the treatment of these patients [4].
Pedicle screws were first introduced for the treatment of thoracolumbar fractures in 1970, by Roy-Camille et al. [5]. The traditional method of long-segment fixation was found to reduce the load on each screw. Hence, performing posterior fixation with two or more segments above and below the fractured vertebra appears to be associated with low failure rate and better stability, but significant reduction of vertebral mobility, dorsalgia and implant failure were the adverse effects of long-segment fixation [6]. On the other hand, short-segment fixation involves pedicle screw fixation at one vertebra above and one vertebra below the fracture level and it has been shown that short-segment fixation leads to inadequate stability, post-operative loss of kyphosis correction and high rate of implant failure [7], but it preserves the range of mobility of the thoracolumbar region. In 1994, Dick et al. introduced the posterior short-segment fixation with two additional screws at the fracture level (6 screw construct) [8]. Many studies have shown that inclusion of the fractured vertebra in the short-segment fixation improves stability and reduces the rate of implant failure [9,10,11].
Methods
Patients selection
Thirty patients were admitted to Neurosurgery Department, Qena University Hospital; South Valley University with thoracolumbar junction fractures between June 2019 and May 2020. All of them were operated upon in the form of short-segment fixation with inclusion of the fracture level.
Patients selected for the study were older than 18 years suffering from traumatic single level thoracolumbar junction fracture, with incomplete or no neurological deficit, where CT scans showed loss of vertebral body height less than 50% and retropulsed fragment in spinal canal less than 50% of the sagittal canal diameter with intact or unilateral fractured pedicles.
Those with multiple spine fractures, pathological fractures or fracture-dislocations who presented clinically with paraplegia or with bilateral fractured pedicles on CT scans were excluded from the study.
Preoperative clinical evaluation was done by recording the neurological status of each patient according to the American Spinal Injury Association (ASIA) classification score and the Medical Research Council (MRC) muscle strength scale as they are easy and reliable scoring systems.
Patients were evaluated radiologically with plain radiographs and computed tomography (CT) scan to determine the TLJ regional kyphosis by using Cobb angle measured from the superior endplate of the vertebra above the fracture level to the inferior endplate of the vertebra below the fracture level and the vertebral body height loss.
Fractures were classified according to their load-sharing score calculated using the scoring system of McCormack et al. [12].
Surgical method
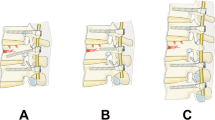
Standard posterior spinal approach was performed in all cases. Trans-pedicular screws were inserted in the adjacent vertebrae above and below the fractured vertebra under image guidance then a trans-pedicular screw/s were inserted in the fractured vertebra according to integrity of the pedicles. Spinal canal decompression was done at the fracture level in cases with compromised canal or neural structure compression. Connecting rods were placed on either side after precontouring them according to the sagittal profile of the thoracic kyphosis and the lumbar lordosis and the bone graft collected from decompression process was stuffed laterally to enhance lateral intertransverse spinal fusion (Figs. 1, 2).

a Pre-operative CT, sagittal view, showing unstable L1 fracture. b Pre-operative CT, axial view showing retropulsed fragment. c Pre-operative CT, 3D reconstruction, sagittal view showing L1 fracture. d Post-operative CT, sagittal view, showing screws in place with adequate reduction of retropulsed fragment. e Post-operative CT, 3D reconstruction, posterior view, showing 2 screws in D12, 2 screws in L2 and 1 screw in L1

a Pre-operative CT, sagittal view, showing unstable L2 fracture and Cobb angle measurement. b Pre-operative CT, sagittal view showing the measurement of AVBH and PVBH. c Pre-operative CT, 3D reconstruction, sagittal view showing L2 fracture. d Post-operative CT, sagittal view, showing screws in place and Cobb angle measurement. e Post-operative CT, sagittal view, showing screws in place with AVBH and PVBH measurement
Outcome evaluation
Primary outcome included the following:
Clinical evaluation was done by determining the ASIA grade and the MRC scale at the immediate postoperative period (2nd day), 1, 3 and 6 months following surgery while the Oswestry disability score was recorded 6 month after surgery. Radiological evaluation in the form of Cobb angle measurement and vertebral body height at the immediate postoperative period (2nd day), 1, 3 and 6 months following surgery (Fig. 3).

a Pre-operative CT, sagittal view showing unstable L1 #. b Pre-operative MRI, T2WI, sagittal view showing L1 #. c Post-operative CT, sagittal view showing screws in place with adequate reduction of retropulsed fragment. d Post-operative CT, 3D reconstruction, posterior view showing 2 screws in D12, 2 screws in L2, and 1 screw in L1
Secondary outcome including the operative time, the amount of intraoperative blood loss and the postoperative hospital stay were recorded.
Results
The study included thirty patients with thoracolumbar junction fractures (T11–L2), twenty one males and nine females. The mean age was 32.47 years (range: 18–63 years).
According to the mode of trauma, we found that the majority of cases (nineteen) were caused by fall from height while eight patients had road traffic accidents. According to level of fracture, twelve patients had L1#, while L2 and D12 fractures occurred in nine cases each.
According to McCormack scoring system, 76.7% of the fractures included in our study had a load-sharing score ≤ 6. The remaining fractures scored > 7.
Preoperative evaluation revealed that twenty three patients were neurologically intact (ASIA grade E), while seven patients had incomplete neurological deficit (six ASIA grade D and one ASIA grade C). According to MRC scale, twenty three patients were grade 5, four patients were grade 4, two patients were grade 3, one patient was grade 1 and.
Postoperative clinical evaluation showed that the patients who had neurological deficits reported to the outpatient clinic with improved neurologic status compared to the pre-operative deficits as shown in Table 1. According to the ASIA scale, one patient with pre-operative ASIA C grade improved to grade D, while six patients with ASIA grade D improved to ASIA grade E at the end of the follow-up period.
Oswestry disability index was estimated at the end of the follow-up period and it was found that the patients had minimal to moderate disability with Oswestry disability index score ranging from 6.0 to 48.0% and a mean score of 19.87%.
The mean preoperative Cobb angle was 19.37° which improved significantly to 11.77° at the end of the follow-up period (P < 0.001).
The mean preoperative anterior vertebral body height of the fractured vertebra was 15.18 mm, this improved in the immediate postoperative period to 17.10 mm with 13.94% improvement. At the end of the follow-up period, the mean anterior vertebral body height was 18.04 mm with 19.64% improvement compared to the preoperative values. The mean posterior vertebral body height of the fractured vertebra was 19.41 mm. In the immediate postoperative period, this value improved to be 20.79 mm with 7.33% improvement and at the final follow-up evaluation it was 21.31 mm with 10.12% improvement. This shows significant restoration of the vertebral body height after fixation and that this restoration was maintained until the end of the follow-up period (Table 2).
Discussion
Many studies showed that the most common causes for spinal fractures are fall from height and road traffic accidents respectively [13, 14].
Although the thoracolumbar junction fractures constitute a major portion of spine fractures as it represents more than 54% of all spine fractures, the instrumentation of this region remains a matter of great controversy, however nowadays posterior short-segment trans-pedicular screw fixation is preferred for fixation of these fractures than long-segment fixation since it offers less operative time, less intraoperative blood loss and better preservation of motion. However, this method was associated with higher rates of implant failure and recurrence of kyphosis and pain [15]. Inclusion of the fractured level in the short-segment construct was first described by Dick et al. [8] in 1994 and this method since then has advanced to overcome these drawbacks, he concluded that adding screws at the fracture level enhanced spinal stability, provided stronger fixation and diminished stress on the remaining pedicle screws in the short-segment construct [16].
Of the thirty cases included in the study, seven patients were presented with incomplete neurological deficits (ASIA grade D & C). These patients reported improvement of the neurological state in the follow-up period as six patients improved to ASIA grade E and one patient to ASIA grade D.
Patients reported minimal to moderate disability on the Oswestry disability index after surgery. The mean ODI was 19.87%. The study of Sun et al. [17], reported similar results with mean ODI of 16.7% in the group treated with short segment-fixation including the fracture level.
Our study showed that the mean operative time was 102.17 min, while in the study done by Dobran et al. [13], the mean operative time in the long-segment fixation group was 172 min that was longer than our used method by about 70 min indicating that short segment fixation provides a time saving method better than the long-segment one. These results were in concordance with the results of Adawi et al. [18], where the mean operative time was 129.7 min.
As regarding the kyphotic angle, the current study showed a significant improvement in postoperative Cobb angle when compared to preoperative values (P ≤ 0.001) as the mean preoperative Cobb angle was 19.37° while the mean postoperative Cobb angle was 11.77°. Our results agreed with a study conducted by El Behairy et al. [19], concluded that short segment pedicle screw fixation including the fractured vertebra accomplished good correction of segmental kyphosis and maintained at the end of a 2-year study. Dobran et al. [13] showed no significant difference between short-segment fixation including fractured level and long-segment fixation in kyphosis correction and maintenance. While, Farrokhi et al. [20] showed that correction of kyphosis was better achieved with short-segment fixation including the fractured level than short-segment fixation excluding the fractured level.
In our study, measurement of the vertebral body height showed that there was significant restoration of vertebral body height after fixation. The mean preoperative anterior and posterior vertebral body height were 15.18 mm and 19.41 mm respectively. These values improved to be 18.04 mm and 21.31 mm respectively at the end of the follow-up period. This was supported by the study of Kanna et al. [21] that showed significant restoration of vertebral body height which was maintained till the end of the follow-up period as they found that the mean preoperative anterior vertebral body height was 13.86 mm that improved to 21.6 mm in the immediate postoperative and to 21.1 mm at the end of the follow-up period. The study also found that the mean preoperative posterior vertebral body height was 25.7 mm that improved to 28.1 mm after surgery and to 28.1 mm at the end of the follow-up period. The study done by El Behairy et al. [19], also confirmed that with inclusion of the fractured level in the short-segment construct provided better restoration and maintenance of vertebral body height for up to 2 years after surgery.
Radiological signs of spinal fusion were assessed in the follow-up radiographs, there was no lucency around the screws in 96.7% of cases, bridging bone formation was present in 93.3% of cases and there was no displacement or breakage of screws. Despite being popular, posterior short-segment fixation has its drawbacks including higher rates of implant failure than long-segment fixation and loss of kyphosis correction over time. An alternative method is including the fracture level in the short-segment construct. This method provides fewer rates of implant failure and recurrence of kyphosis. This was supported by a study conducted by Mahar et al. [9] reported increased biomechanical stability using this technique. Also the studies of Guven et al. [10] and Bolesta et al. [16] showed increased stability and maintained kyphosis correction when inclusion of fracture level was used.
Conclusions
Inclusion of the fracture level in the short-segment construct has offered a safe effective method in kyphosis correction, in addition to lower implant failure rates, without additional complications and with a comparable clinical and functional outcome. We recommend insertion of screws into the pedicles of the fractured vertebra when considering a short-segment posterior fixation for thoracolumbar spine fractures.
Availability of data and materials
The data and materials of this manuscript are available for sharing.
Abbreviations
- #:
-
Fracture
- ASIA:
-
American Spinal Injury Association
- CT:
-
Computed tomography
- MRC:
-
Medical Research Council
- MRI:
-
Magnetic Resonance Imaging
- Min:
-
Minutes
- Ml:
-
Milliliter
- Mm:
-
Millimeter
- ODI:
-
Oswestry disability index
- VBCR:
-
Vertebral body compression ratio
- AVBH:
-
Anterior vertebral body height
- PVBH:
-
Posterior vertebral body height
References
Wood KB, Li W, Lebl DR, Ploumis A. Management of thoracolumbar spine fractures. Spine J Off J N Am Spine Soc. 2014;14(1):145–64.
Misra S, Sen S, Das S, Chatterjee A, Sengupta A, Saha S. Evaluation the results of surgical management of traumatic paraplegia in traumatic thoracolumbar fractures. Int J Res Med Sci. 2016;4:2262–70.
Gertzbein SD. Scoliosis research society. Multicenter spine fracture study. Spine. 1992;17(5):528–40.
Scheer JK, Bakhsheshian J, Fakurnejad S, Oh T, Dahdaleh NS, Smith ZA. Evidence-based medicine of traumatic thoracolumbar burst fractures: a systematic review of operative management across 20 years. Glob Spine J. 2015;5(1):73–82.
Yu SW, Fang KF, Tseng IC, Chiu YL, Chen YJ, Chen WJ. Surgical outcomes of short-segment fixation for thoracolumbar fracture dislocation. Chang Gung Med J. 2002;25:253–9.
Koller H, Acosta F, Hempfing A, Rohrmuller D, Tauber M, Lederer S, Resch H, Zenner J, Klampfer H, Schwaiger R, Bogner R, Hitzl W. Long-term investigation of nonsurgical treatment for thoracolumbar and lumbar burst fractures: an outcome analysis in sight of spinopelvic balance. Eur Spine J. 2008;17:1073–95.
Tezeren G, Kuru I. Posterior fixation of thoracolumbar burst fracture: short-segment pedicle fixation versus long-segment instrumentation. J Spinal Disord Tech. 2005;18:485–8.
Dick JC, Jones MP, Zdeblick TA, Kunz DN, Horton WC. A biomechanical comparison evaluating the use of intermediate screws and cross-linkage in lumbar pedicle fixation. Clin Spine Surg. 1994;7(5):402–7.
Mahar A, Kim C, Wedemeyer M, Mitsunaga L, Odell T, Johnson B, Garfin S. Short-segment fixation of lumbar burst fractures using pedicle fixation at the level of the fracture. Spine. 2007;32(14):1503–7.
Guven O, Kocaoglu B, Bezer M, Aydin N, Nalbantoglu U. The use of screw at the fracture level in the treatment of thoracolumbar burst fractures. J Spinal Disord Tech. 2009;22:417–21.
Huang W, Luo T. Efficacy analysis of pedicle screw internal fixation of fractured vertebrae in the treatment of thoracolumbar fractures. Exp Ther Med. 2013;5:678–82.
McCormack T, Karaikovic E, Gaines RW. The load sharing classification of spine fractures. Spine. 1994;19(15):1741–4.
Dobran M, Nasi D, Brunozzi D, Di Somma L, Gladi M, Iacoangeli M, Scerrati M. Treatment of unstable thoracolumbar junction fractures: short-segment pedicle fixation with inclusion of the fracture level versus long-segment instrumentation. Actaneurochirurgica. 2016;158(10):1883–9.
Elshoura SA, Elsamea MA. Inclusion of the fracture level in short-segment fixation of unstable traumatic thoracolumbar spine fractures. Al-Azhar Assiut Med J. 2016;14(4):153.
Muratore M, Allasia S, Viglierchio P, Abbate M, Aleotti S, Masse A, Bistolfi A. Surgical treatment of traumatic thoracolumbar fractures: a retrospective review of 101 cases. Musculoskelet Surg. 2020;5:1–1.
Bolesta MJ, Caron T, Chinthakunta SR, Vazifeh PN, Khalil S. Pedicle screw instrumentation of thoracolumbar burst fractures: biomechanical evaluation of screw configuration with pedicle screws at the level of the fracture. Int J Spine Surg. 2012;6:200–5.
Sun C, Guan G, Liu X, Zhang H, Wang B. Comparison of short-segment pedicle fixation with versus without inclusion of the fracture level in the treatment of mild thoracolumbar burst fractures. Int J Surg. 2016;1(36):352–7.
Adawi MM, Aboulfetouh I, Saleh A, Younis W. Posterior short-segment fixation with implanting pedicle screw in the fractured level as a feasible method for treatment of thoracolumbar fracture. Egypt J Neurosurg. 2019;34(1):6.
El Behairy HF, Abdelaziz AM, Saleh AK, Elsherief FAH, Abuomira IEA, Elkawary AI, Aldahshan W, Mahmoud WS. Short-segment fixation of thoracolumbar fractures with incorporated screws at the level of fracture. Orthop Surg. 2020;12(1):170–6.
Farrokhi MR, Razmkon A, Maghami Z, Nikoo Z. Inclusion of the fracture level in short segment fixation of thoracolumbar fractures. Eur Spine J. 2010;19(10):1651–6.
Kanna RM, Shetty AP, Rajasekaran S. Posterior fixation including the fractured vertebra for severe unstable thoracolumbar fractures. Spine J. 2015;15(2):256–64.
Acknowledgements
Not applicable.
Funding
No available fund (This research was funded by the authors).
Author information
Authors and Affiliations
Contributions
All authors have contributed to the content of this paper. ‘EE’: Shared in putting study design, collection of data, analysis and interpretation of data, writing the manuscript, and final approval of the version to be published. ‘AH’: Shared in putting study design, collection of data, analysis and interpretation of data, writing the manuscript, and final approval of the version to be published. ‘AT’: Collection of data, analysis and interpretation of data, and final approval of the version to be published. ‘RN’: Conception and design of study, drafting of article, analysis and interpretation of data, and final approval of the version to be published. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study has been performed in accordance with the Declaration of Helsinki, and an informed signed consent was taken from all the patients before enrolling them into the study after approval of Ethical Committee (Number: 06/19), Qena Faculty of Medicine, South Valley University.
Consent for publication
A written consent has been obtained from every included patients regarding publishing theirs details and images.
Competing interests
There is no conflict of interest on this manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hamdan, A.R., Mahmoud, R.N., Tammam, A.G. et al. Inclusion of the fractured level into the construct of short segment fixation in patients with thoracolumbar fractures: clinical and radiological outcome. Egypt J Neurosurg 36, 41 (2021). https://doi.org/10.1186/s41984-021-00137-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41984-021-00137-7