
Abstract
Objectives
Due to increased number of patients suffering from hydrocephalus (HCP) and lack of data concerning volumetric changes after shunting operations, this study aims to assess the volumetric changes in brain ventricles after successful ventriculoperitoneal (VP) shunt surgery in correlation with clinical improvement.
Patient and methods
This study included 20 patients; all of them are below the age of 2 years. All the patients had hydrocephalus, were treated surgically with VP shunts, and have clinically improved over the period of study. We measured the volumetric changes radiologically using the fronto-occipital horn ratio (FOHR) over a period of 6 months postoperatively.
Results
The frontal and occipital horn ratio was calculated in all these patients both pre and postoperatively. There was a significant radiological improvement in the majority of children after the shunt operation. One month postoperatively, the FOHR decreased to about 85% of its preoperative value in average. The FOHR was found to be significantly improving with time over a period of 6 months reaching 63% of its preoperative value.
Conclusion
Successful treatment of HCP in infants via VPS seems to be of benefit in decreasing the ventricular size gradually to a near normal FOHR with clinical improvement.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Introduction
Hydrocephalus is a common brain disorder especially in low- and middle-income countries (123 per 100,000 births) that results from discrepancy between cerebrospinal fluid (CSF) production and absorption, with subsequent accumulation of fluid in the cranial cavity and enlargement of ventricles [1, 2].
Infants and children presented with manifest radiological hydrocephalic changes would require a CSF shunting procedure which remains the treatment of choice for most children, despite the dissatisfaction with its long-term outcome [3,4,5,6].
CSF diversion in hydrocephalic children reduces the volume of the ventricles with subsequent improvement in neurological and intellectual functions. However, variation in the long-term outcome was reported, raising the need for a radiological parameter to predict the clinical outcome after surgery [6,7,8,9,10].
Measurement of ventricular size is important in pediatric patients with hydrocephalus. Especially those followed up with CSF shunts, ventricular volume measurement was reported in adults’ and infants’ hydrocephalus; magnetic resonance imaging (MRI) was frequently used in addition to computed tomography (CT) for this purpose [11,12,13,14,15]. Sequential ventricular volume assessment was beneficial to assess the outcome after shunting surgery; besides, it was used to predict impending shunt failure [16, 17]. Assessment of different CSF diversion surgeries was performed by ventricular volume change analysis; also, the pressure of shunts used were further validated by the reduction of ventricular volume measurements [16,17,18].
We aim in this study to measure the volumetric changes in ventricles which accompany clinical improvement after a successful ventriculoperitoneal shunt (VPS) surgery in infants under 2 years old.
Patient and methods
Prospective case series study was carried out in the Department of Neurosurgery at Menoufia University Hospital and Mansoura International Hospital after obtaining approval of the Ethics Committee. Patients who are under 2 years old with hydrocephalus and were managed surgically with VPS surgery and completed the follow-up for 6 months during the period from April 2016 to April 2018 were included in the study.
A written informed consent was obtained from all participants’ families after explanation of the benefits and description of the study protocol. Inclusion criteria included a working VP shunt all over the 6 months with clinical improvement. The exclusion criteria included brain tumors, subarachnoid hemorrhage or infection as a primary cause for hydrocephalic changes, history for concomitant meningeocele, and multilocular hydrocephalus.
The surgical procedure was standardized as far as possible to allow comparability. The operations were performed under general anesthesia in supine position in completely aseptic conditions.
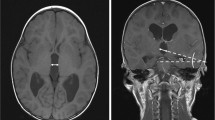
The volumetric changes in brain ventricles were assessed via the fronto-occipital horn ratio (FOHR), a ratio which averages the frontal and occipital horn width divided by twice the interparietal diameter as demonstrated in Fig. 1, measured in follow-up CT brain done at the end of the first month and the end of the sixth month comparing it to the FOHR measured preoperatively assessing the percentage of improvement with the ongoing clinical improvement.

Anatomical landmark and measurement set for the fronto-occipital horn ratio (FOHR) ratio when measured on CT brain
Data were statistically described in terms of range, mean, standard deviation (SD), median, frequencies (number of cases), and percentages when appropriate. Student t test of significance was used to determine p value of head circumference changes.
Results
Twenty children who underwent ventriculoperitoneal shunts for congenital hydrocephalus and who have clinically improved along the period of follow-up were studied. The results were analyzed. The postoperative neurological improvement was correlated with radiological findings.
The study included 12 males (60%) and 8 females (40%). Progressive increase in head size was the most common symptom in the examined group. Five (25%) of the children had gross delay in milestones at the time of admission. Seven patients (35%) had symptoms of increased intracranial tension and 2 (10%) had preoperative seizures (Table 1).
Head circumference was closely observed in children as a single very important predicting factor. It ranged from 37 cm to 52 cm preoperatively with mean value of 44.5 cm (Table 2), and over a period of follow-up to 6 months, the head circumference significantly improved ranging from 32cm to 42 cm with average circumference of 35.4 cm (Table 3).
The frontal and occipital horn ratio was calculated in all these patients both preoperatively and postoperatively. There was a significant improvement in almost all the children after the shunt. One month postoperatively, the FOHR decreased to about 85% of its preoperative value in average with the best improvement at 80%.
The FOHR was found to be significantly improving with time in uncomplicated patients over a period of 6 months reaching 63% of its preoperative value with the mean percentage of improvement 36% (Table 3).
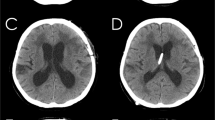
A representative case was studied of a one-year-old male infant who was delivered by cesarean section and was admitted to neonatal ICU for 7 days for respiratory distress management, then was discharged after improvement. He was presented with a large head inappropriate for age and inability to support sitting position. On physical examination, the HC was 48 cm with bulging AF. Preoperative CT brain was showing communicating HCP with FOHR = 0.758 (Fig. 2a).

A CT brain of hydrocepahic child. a Preoperative, b 1 month postoperative, and c 6 months postoperative
The patient was managed surgically with VP shunt with no postoperative complications, and the AF was flat and non-tense. The child was followed up for 6 months postoperative. One month postoperative, the FOHR decreased to be 0.615, and the HC was decreasing to reach 46 cm at the end of the first month postoperative (Fig. 2b), while 6 months postoperative, the FOHR improved to reach 0.492 and the HC was 45 cm with a well working VP shunt by examination (Fig. 2c).
Discussion
CSF diversion in hydrocephalic children reduces the ventricular dilatation. Though improvement in neurological and intellectual functioning is often seen, our 20 infants were all submitted to VP shunt surgery with the ventricular end in the lateral ventricle and the distal end intraperitoneal. Previous reports said that the standard treatment of congenital hydrocephalus is CSF diversionary device with a pressure-regulating valve, commonly known as a shunt [1, 19]. In addition, Kiesler J, Ricor R [20], said that the growth of the cranium is triggered by the pressure of the growing brain and HC is an important indicator of brain development.
In our study, HC was a main clinical issue that we gave an ultimate care to measure regularly both before and after surgery. Eighteen (90%) of the children had enlarged HC before they were submitted to shunt surgery with the least measured HC value at 37 cm and the most one at 52 cm.
In postoperative follow-up over a period of 6 months, HC evidently improved with measurements ranging from 32 cm in its lowest value up to 42 cm.
Thompson et al. [21] reported an inverse correlation of the ventricle–brain ratio (VBR) with the Bayley Mental Scale showing a correlation between brain mass and IQ in older children with uncomplicated hydrocephalus in their series. Additionally, O’Hayon B.B et al. [22] have found that the frontal and occipital horn ratio is a simple method of evaluating ventricular size in pediatric hydrocephalus patients with CSF shunts. They said that it is the best linear correlation with ventricular size (r = 0.852) and was equivalent to the ventricular–brain ratio (r = 0.891), previously shown to have the highest correlation with ventricular volume [22].
In our study, we depended on the FOHR as our reliable diagnostic tool for measuring the volumetric changes in brain ventricles. The initial measurement of the FOHR before surgery showed that it ranged from 0.536 to 0.785 with mean value of 0.67. No significant changes were observed concerning the size of the already dilated ventricles in the early postoperative period (within the first week postoperative); meanwhile, there were some signs denoting that there was a decrease in intracranial tension as white and gray matter differentiation in addition to prominent sulci and gyri. Along the course of follow-up of our patients, changes in the ventricular volume by the end of the first month postoperatively, the FOHR decreased to about 85% of its preoperative value in average with the best improvement at 80%.
Gradual changes occurred and increased with time together with the improvement in the child’s physical and mental development The FOHR was found to significantly improve with time over the 6 months with the mean value at 0.427 in comparison to a mean of 0.67 before children were submitted to shunt operation.
Limitations
In the follow-up of children treated surgically with VP shunt for hydrocephalus, different scales as Bayley Scales of infant development and Gesell Developmental Schedules are considered. The schedules cover major areas of behavioral development, namely, motor, adaptive, language, personal, and social development. It involves a standardized procedure of observing and evaluating the various elements of behavior in the child. It includes tests, as well as observations of the child. These schedules are applicable for children from the age of 4 months to 6 years.
In our study, we could not apply all the aspects of these scales as it needed expert pediatricians and pediatric psychiatrists, so we depended in follow-up and in choosing our clinically improved children on more applicable parameters for us as signs of increased ICT in the early postoperative stage, the motor activity, which measures the motor abilities, such as sitting, standing, walking, and so on in addition to repeated measurements of HC correlating it to its chronological age. The mental development of children was assessed roughly by noticing their attention to the surrounding effects as verbal, sound, and light stimulants beside their reactivity to the surrounding persons.
Conclusion
Hydrocephalus remains one of the most challenging and the most common neurosurgical condition in children. Surgical management of HCP with VPS is the most beneficial way in treatment. The aim of management of hydrocephalus is to achieve total clinical recovery and to obtain normal to near-normal intellectual development. Successful treatment of HCP in infants via VPS seems to be of benefit in decreasing the ventricular size to a near-normal FOHR with clinical improvement.
Recommendations
We recommend further multi-centric studies using larger number of patients and for a longer period of follow-up as we were limited by the number of patients due to lack of culture of follow-up of our patients and the limitation of follow-up duration that was 6 months.
Availability of data and materials
Data are available upon request.
Abbreviations
- AF:
-
Anterior fontanelle
- CSF:
-
Cerebrospinal fluid
- CT:
-
Computed tomography
- FOHR:
-
Fronto-occipital horn ratio
- HC:
-
Head circumference
- HCP:
-
Hydrocephalus
- ICT:
-
Intracranial tension
- ICU:
-
Intensive Care Unit
- IQ:
-
Intelligence quotient
- MRI:
-
Magnetic resonance imaging
- VBR:
-
Ventricle–brain ratio
- VP:
-
Ventriculoperitoneal
References
Dewan MC, Rattani A, Mekary R, Glancz LJ, Yunusa I, Baticulon RE, Fieggen G, Wellons JC, Park KB, Warf BC. Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. J Neurosurg. 2018:1–15. https://doi.org/10.3171/2017.10.JNS17439.
Enchev Y, Oi S. Historical trends of neuroendoscopic surgical techniques in the treatment of hydrocephalus. Neurosurg Rev. 2008;31:249–62. https://doi.org/10.1007/s10143-008-0131-y.
Auer LM, Holzer P, Ascher PW, Heppner F. Endoscopic neurosurgery. Acta Neurochir (Wien). 1988;90:1–14.
Farin A, Aryan HE, Ozgur BM, Parsa AT, Levy ML. Endoscopic third ventriculostomy. J Clin Neurosci. 2006;13:763–70. https://doi.org/10.1016/j.jocn.2005.11.029.
Fritsch MJ, Kienke S, Manwaring KH, Mehdorn HM. Endoscopic aqueductoplasty and interventriculostomy for the treatment of isolated fourth ventricle in children. Neurosurgery. 2004;55:372–7; discussion 7-9.
Albright AL, Pollack IF, Adelson PD, Solot JJ. Outcome data and analysis in pediatric neurosurgery. Neurosurgery. 1999;45:101–6.
Virhammar J, Warntjes M, Laurell K, Larsson EM. Quantitative MRI for rapid and user-independent monitoring of intracranial CSF volume in hydrocephalus. AJNR Am J Neuroradiol. 2016;37:797–801. https://doi.org/10.3174/ajnr.A4627.
Vivas-Buitrago T, Pinilla-Monsalve G, Jusue-Torres I, Oishi K, Robison J, Crawford JA, Pletnikov M, Xu J, Baledent O, Lokossou A, Hung AL, Blitz AM, Lu J, et al. Ventricular volume dynamics during the development of adult chronic communicating hydrocephalus in a rodent model. World Neurosurg. 2018;120:e1120–e7. https://doi.org/10.1016/j.wneu.2018.08.241.
Rubin RC, Hochwald G, Tiell M, Liwnicz B, Epstein F. Reconstitution of the cerebral cortical mantle in shunt-corrected hydrocephalus. Dev Med Child Neurol Suppl. 1975:151–6.
Bilginer B, Oguz KK, Akalan N. Endoscopic third ventriculostomy for malfunction in previously shunted infants. Childs Nerv Syst. 2009;25:683–8. https://doi.org/10.1007/s00381-008-0779-1.
Haubrich C, Czosnyka M, Diehl R, Smielewski P, Czosnyka Z. Ventricular volume load reveals the mechanoelastic impact of communicating hydrocephalus on dynamic cerebral autoregulation. PLoS One. 2016;11:e0158506. https://doi.org/10.1371/journal.pone.0158506.
Onder H, Hanalioglu S. Does the volume of CSF removed affect the response to a tap in normal pressure hydrocephalus? AJNR Am J Neuroradiol. 2018;39:E5–6. https://doi.org/10.3174/ajnr.A5422.
Tan K, Meiri A, Mowrey WB, Abbott R, Goodrich JT, Sandler AL, Suri AK, Lipton ML, Wagshul ME. Diffusion tensor imaging and ventricle volume quantification in patients with chronic shunt-treated hydrocephalus: a matched case-control study. J Neurosurg. 2018;129:1611–22. https://doi.org/10.3171/2017.6.JNS162784.
Singer OC, Melber J, Hattingen E, Jurcoane A, Keil F, Neumann-Haefelin T, Klein JC. MR volumetric changes after diagnostic CSF removal in normal pressure hydrocephalus. J Neurol. 2012;259:2440–6. https://doi.org/10.1007/s00415-012-6525-3.
Xenos C, Sgouros S, Natarajan K. Ventricular volume change in childhood. J Neurosurg. 2002;97:584–90. https://doi.org/10.3171/jns.2002.97.3.0584.
Azab WA, Mijalcic RM, Nakhi SB, Mohammad MH. Ventricular volume and neurocognitive outcome after endoscopic third ventriculostomy: Is shunting a better option? A review. Childs Nerv Syst. 2016;32:775–80. https://doi.org/10.1007/s00381-016-3032-3.
Di Rocco F, Grevent D, Drake JM, Boddaert N, Puget S, Roujeau T, Blauwblomme T, Zerah M, Brunelle F, Sainte-Rose C. Changes in intracranial CSF distribution after ETV. Childs Nerv Syst. 2012;28:997–1002. https://doi.org/10.1007/s00381-012-1752-6.
Xenos C, Sgouros S, Natarajan K, Walsh AR, Hockley A. Influence of shunt type on ventricular volume changes in children with hydrocephalus. J Neurosurg. 2003;98:277–83. https://doi.org/10.3171/jns.2003.98.2.0277.
Basauri L, Cornejo J, Vargas F. Treatment of congenital and acquired hydrocephalus with the ventricular shunt system. Neurocirugia. 1968;26:34–41.
Kiesler J, Ricer R. The abnormal fontanel. Am Fam Physician. 2003;67:2547–52.
Thompson MG, Eisenberg HM, Levin HS. Hydrocephalic infants: developmental assessment and computed tomography. Childs Brain. 1982;9:400–10.
O'Hayon BB, Drake JM, Ossip MG, Tuli S, Clarke M. Frontal and occipital horn ratio: a linear estimate of ventricular size for multiple imaging modalities in pediatric hydrocephalus. Pediatr Neurosurg. 1998;29:245–9. https://doi.org/10.1159/000028730.
Acknowledgements
Nothing to be added
Funding
None
Author information
Authors and Affiliations
Contributions
TMH, ASM, and SEA were responsible for the conception of the study. TMH did the acquisition of data. TMH, ASM, and SEA were responsible for the analysis and interpretation of data. TMH and ASM drafted the article. ASM, SEA, HAA, and MLA critically revised the article. TMH did the statistical analysis. ASM, SEA, and HAA did administrative, technical, and material support. HAA did the study supervision. All the authors designed the study and reviewed submitted version of the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Ethics Committee Council approval was on the 26th of October 2016 by the monthly held scientific research committee meeting of Menoufia University Graduate School of Medicine. Informed written consents were obtained from parents/guardians of infants included in the study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hasanin, T.M., Mansour, A.S., Alemam, S.E. et al. Ventricular volume changes after successful shunting in hydrocephalic infants. Egypt J Neurosurg 35, 10 (2020). https://doi.org/10.1186/s41984-020-00075-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41984-020-00075-w