
Abstract
Background
Thoracic and lumbar fractures represent nearly 90% of traumatic spine injuries. Thoracolumbar region is susceptible to injury because of its location between the stiff kyphotic thoracic spine and the mobile lordotic lumbar region. To compare between short-segment fixation with screws into index level and long-segment fixation in maintaining angle of correction and pain.
Methods
A prospective study included 91 patients, who had single-level thoracolumbar fracture with Cobb’s angle ≤ 25° and underwent posterior fixation. Forty-four patients underwent short-segment fixation with screws into the index level, and 47 patients underwent long-segment fixation with skipped index level. The angle of correction, pain, and neurological state were regularly assessed.
Results
Forty-four patients (48.35%) had short segment and 47 (51.65%) had long-segment fixation. In the short segment group, the pre-operative mean Cobb’s angle was 19.34° ± 3.63° and the angle of correction was 8.14° ± 1.9° after 1 year, while in the long segment group, the pre-operative mean Cobb’s angle was 19.08° ± 4.0° and the angle of correction was 8.62° ± 2.59°. Regarding pain, in the short segment group, the pre-operative visual analogue scale (VAS) was 5.59 ± 2.09 that was reduced to 1.39 ± 0.58 at the 1 year follow-up, while the long segment group VAS was 5.4 ± 2.01 pre-operatively that was reduced to 1.47 ± 0.58.
Conclusions
Short-segment fixation can maintain the angle of correction as long-segment fixation for single level thoracolumbar traumatic fracture with lower complication and faster pain relief.
Trial registration
Clinicaltrials.gov/NCT03272243. Registered: 1 September 2017.
Similar content being viewed by others


Background
Thoracolumbar fractures occur when the vertebra is subjected to a significant axial and possibly flexion force vector that brings the failure of the anterior vertebral body in compression. This region (T10–L2) is uniquely susceptible to this mechanism of injury as a result of its location between the stiff kyphotic thoracic spine and the more mobile lordotic lumbar region [1].
The successful diagnosis and management of thoracolumbar fractures depend on an accurate assessment of spinal stability and the neurologic state of the patient [2].
As a simple and commonly used technique, short-segment pedicle instrumentation of thoracolumbar instability seems to have a high rate of implant failure and recurrence of instability. In the literature, there are biomechanical studies aimed to determine the effect of adding pedicle screws at the level of a burst fracture [3].
Data obtained from those studies suggested that the use of transpedicular screws at the fractured level provides the advantages of a stiffer construct, an increased biomechanical stability, and the effect of 3-point fixation of the unstable segment guard against failure of the construct [4].
Currently, short-segment pedicle instrumentation for thoracolumbar fractures is gaining popularity. Otherwise, long-segment fixation may be chosen as another treatment method [5].
The aim of this study was to compare between short-segment posterior stabilization including index level versus long-segment posterior stabilization for management of thoracolumbar spine fracture instability as regards post-operative pain and angle of correction.
Methods
This is a prospective study which was performed in the period between February 2012 and February 2016. Patients included in this study had thoracolumbar spine instability including wedge fracture or burst fracture with Thoraco-Lumbar Injury Classification and Severity (TLICS) score ≥ 4 and fulfilling the study inclusion criteria which were (1) single-level fracture, (2) less than 50% of spinal canal compromised, (3) mild kyphosis or scoliosis, Cobb’s angle ≤ 25°, and (4) with or without neurological deficit.
The exclusion criteria were patients with multiple-level fractures, patients with more than 50% spinal canal compromise, patients who needed anterior approach to decompress the canal, and those who have fracture dislocation and/or marked kyphosis and scoliosis with Cobb’s angle > 25°, who needed 360° fixation with long-segment fixation to maintain the angle of correction.
Ninety-one patients were carefully selected, randomly grouped (per surgeon preference), and operated after obtaining the ethical approval from the local ethical committee. Forty-four patients underwent short-segment posterior stabilization including index level (fractured level), and the other 47 underwent long-segment posterior stabilization skipping the index level.
Technique
Posterior approach to the spine has been used in all patients. The wound incision and exposure of lamina and facet technique was the same in both short- and long-segment approaches but they differ in the length and number of lamina exposed.
Short-segment approach
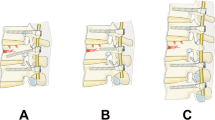
After exposure of laminae and facets of the index level with one level above and one level below, the trans-pedicular screws have been inserted under C-arm guidance in biplanar technique to all three levels. Laminectomy was done to decompress the canal if needed then postero-lateral fusion using bone graft was done Fig. 1. Cross connectors were not used in such short construct with screws in index levels.

a Pre-operative MRI sagittal view of the L1 fracture. b Pre-operative sagittal CT. c, d Post-operative CT. e Post-operative X-ray lateral view
Long-segment approach
After exposure of the laminae and facets of the index level with two levels above and two levels below, the trans-pedicular screws have been inserted under C-arm guidance to the above and below levels sparing the index level. Then, laminectomy and lateral fusion had been done like in short-segment approach Fig. 2. Cross connectors were used in only two patients over the index level in osteoporotic patients.

a Pre-operative CT of L1 fracture. b Post-operative X-ray lateral view of the long-segment fixation
Follow-up
All patients were evaluated over a period of 1 year. Clinical assessment of pain using the visual analogue scale (VAS), the Oswestry Disability Index (ODI), and Cobb’s angle was followed up by radiological assessment using plain x-ray, and CT dorsolumbar spine was done immediately post-operative then regularly in the 3rd, 6th, 9th, and 12th months post-operative at the outpatient clinic. Assessment of the neurologic state was performed through the follow-up period by using the American Spinal Injury Association Impairment (ASIA) scale. Data including follow-up were reviewed from hospital records after we had obtained the local institutional review board approval.
Statistical analysis
Statistical analysis was performed by the Statistical Program for the Social Sciences, version 19.0 (IBM SPSS Statistics for Windows, IBM Corp, Armonk, NY).
Comparative tests were performed between the first year values and baseline measurements. The paired t test used to compare changes in mean values after 1 year of the intervention within groups with regard to quantitative variables. Results of comparisons were considered not significant if P > .01 and were considered significant if P ≤ .01.
Results
Ninety-one patients were included in this study: 80 males (87.9%) and 11 females (12.1%) with a mean age 38 ± 9 years. The highest incidence of thoracolumbar vertebrae fracture was at the level of L1 (37.7%) then L2 (29.6%) followed by D12 (23%) and least incidence in D11 (6.6%) and D10 (3.3%).
The type of fractures were variable, 38 patients presented with burst fracture (41.75%), 26 patients with wedge fracture (28.57%), 15 patients had hyperextension fractures (16.48%), and 12 patients with shears fracture (13.18%). Most of burst and wedge fractures were due to falling from a height while most of hyperextension and shears fractures were due to road traffic accident.
The neurological state
Seven patients have shown alteration of their neurological state, five of them (5.4%) had some improvements and the other two patients (2.2%) were worse.
While the other 84 patients remained with the same pre-operative ASIA score, Table 1 shows the results in both groups as regard the ASIA scores. There was no statistically significant difference between both groups.
Angle of correction
There was no superiority of the long-segment over the short-segment stabilization with index level stabilization as regards the correction of kyphotic angle and maintaining the sagittal plane till fusion as shown in Table 2.
Pain
The VAS rapidly improved among short segment group than long-segment one during follow-up for 1 year. Both groups have almost similar VAS records as shown in Table 3.
The Oswestry Disability Index (ODI)
The mean pre-operative ODI in the short-segment fixation group was 34.66 ± SD 26.92, while it was 41.49 ± SD 22.09 in the long segment group. Both groups have shown a statistically significant changes in the mean ODI scores at the 1 year follow-up period with (P value = 0.000) in both groups (Table 4 and Fig. 3).

The changes in the ODI in both groups at the first year post-op evaluation
Complications
Three patients in the short-segment fixation group had complications; one patient had CSF leakage, and two patients had superficial wound infection. All of them were treated conservatively.
Five patients in the long segment group had different complications; one patient has a pullout of the upper screws, and two patients had a fractured rod. All of these three patients had a redo surgery.
The other two patients had superficial wound infection that was treated conservatively.
Discussion
Traumatic spinal fractures of the thoracolumbar area represent approximately 90% of all spinal fractures; these injuries can result in loss of neurological function, pain, disability, and deformity, and represent a great economic burden to society [6].
Although short-segment stabilization approach, one level above and one level below, has high failure rate, it become preferred approach after renovation by addition of screws into the fractured level (index level). Several studies were done to ensure biomechanical stability of this short construct, and most of studies revealed its low failure rate and high pull out resistance [7].
In a prospective, randomized study of 80 patients, Farrokhi et al. in 2010 found that placement of pedicle screws into the pedicles of the fractured level during short-segmental fixation for thoracolumbar fractures led to better kyphosis correction, fewer instrument failures, and comparable or better clinical outcomes [8].
Eno et al. in 2012 found that pedicle screw fixation at the fractured level did not achieve greater correction of the segmental kyphotic angle compared to conventional intersegmental fixation; however, pedicle screw fixation more effectively restored the height of the fractured vertebra. Recovery of height is as important as the recovery of the angle, and it is helpful for the recovery of the integrity in the adjacent segments and the whole spine [9].
Interestingly, the additional pedicle screw fixation (six-screw fixation) at the fractured vertebra allowed patients to ambulate approximately 10 days earlier than patients who underwent conventional four-screw intersegmental fixation [10]. On the other hand, our study results revealed that pedicular screws into the fracture level in short-segment fixation can correct the kyphotic angle provided that kyphotic angle range from 10° to 25° with minimum correction angle 4° and maximum correction angle 14°.
Adding bilateral index level screws to short-segment fixation increased the stability of the construct by 25%. The increase in stability was significant during flexion and lateral bending [11].
In vitro burst fracture model with pig spines was done to compare short fixation (so-called one above–one below) with short fixation plus intermediate screws. They found that intermediate screws significantly decreased segmental flexibility in all axes of motion by an average of 26%. The reduction in flexibility was least prominent during axial rotation [12].
Pain
The short segment group has less pain in immediate post-operative evaluation than long segment group in whom more analgesia (opioid analgesia) was needed. Pain follow-up of all cases every 3 months over 1 year by VAS (visual analogue scale) revealed rapid pain relief among short segment group than long segment group, and the pain became minimal after fusion had occurred. Both groups had shown reduction of the ODI score with significant changes at the 1-year follow-up. Kim et al. had addressed outcomes including pain in different three groups underwent short-segment stabilization with screws in index vertebra; the first group (n = 26) was similar to our short segment group. The mean VAS scores were 7.6 before surgery and 3.0 at the last follow-up, while in our group, VAS scores were 5.59 and 1.39 respectively [11].
Angle of correction
We notice that there is initial less correction of kyphotic angle then the correction became more corrected in both groups till fusion occurs after about 6 months to 1 year.
Mahar et al. in 2007 concluded that an average of 15° of kyphosis correction could be obtained using limited posterior segmental fixation. This is likely better than traditional, non-segmental pedicle screw fixation. This compared to our study in which the average amount of correction for short-segment fixation was 14.2°. However, the amount of correction was slightly higher with long-segment fixation (16.9°) but no significant statistical difference was found, which is similar to the findings of Guven et al. in 2007 who found no statistically significant difference regarding the correction between long-segment fixation and short-segment fixation with pedicle screw at the fractured level. But still more than 70% of cases of long-segment fixation had more than 70% kyphosis correction. On the other hand, short-segment fixation and poor initial post-operative kyphosis correction were both significantly associated with correction loss [13].
In a systematic review by Verlaan et al. in 2005 where different modalities for the treatment of traumatic thoracic and lumbar spine fractures were analyzed. Their review included posterior long and short constructs, anterior-only fixation, and circumferential fixation. They concluded that regardless of the severity of injury, no technique was able to correct and maintain the fracture segment to the physiological level and kyphotic angle. This statement was reaffirmed by Wang et al., who also found no correlation between the degree of kyphosis and residual back pain [14].
More studies are needed to understand the effect of short fixation on adjacent levels and on the maintenance of deformity correction in the thoracolumbar spine, either as a stand-alone procedure or as an adjunct to anterior fixation.
Study limitations
-
1.
The follow-up evaluation was limited to a 1-year period which is considered to be a short term.
-
2.
Many patients with multilevel fractures have been excluded from the study. The need for assessment of multiple adjacent index levels fusion should be taken in consideration in the upcoming research.
Conclusions
There is no superiority of long-segment over short-segment stabilization with index level screws in the correction of kyphotic angle and maintaining sagittal plane. Moreover, short-segment stabilization has faster relief of pain, lesser tissue destruction than long segment with the same biomechanical stability.
Change history
31 October 2018
In the publication of this article [1], unfortunately not the latest version of the Declarations section has been published.
Abbreviations
- ASIA:
-
American Spinal Injury Association Impairment Scale
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- ODI:
-
Oswestry Disability Index
- SD:
-
Standard deviation
- TLICS:
-
Thoraco-Lumbar Injury Classification and Severity
- VAS:
-
Visual analogue scale
References
Patel AA, Vaccaro AR. Thoracolumbar spine trauma classification. J Am Acad Orthop Surg. 2010;18(2):63–71.
Vaccaro AR, et al. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005;18(3):209–15.
Toyone T, Tanaka T, Kato D. The treatment of acute thoracolumbar burst fractures with transpedicular intracorporeal hydroxyapatite grafting following indirect reduction and pedicle screw fixation: a prospective study. Spine (Phila Pa 1976). 2006;31(7):E208–14.
Anekstein Y, Brosh T, Mirovsky Y. Intermediate screws in short segment pedicular fixation for thoracic and lumbar fractures: a biomechanical study. J Spinal Disord Tech. 2007;20(1):72–7.
Yu SW, Fang KF, Tseng IC. Surgical outcomes of short-segment fixation for thoracolumbar fracture dislocation. Neurosurg Focus. 2010;25(4):253–9.
Lewkonia P, Paolucci EO, Thomas K. Reliability of the thoracolumbar injury classification and severity score and comparison with the denis classification for injury to the thoracic and lumbar spine. Spine (Phila Pa 1976). 2012;37(26):2161–7.
Yang M, Ding GZ, Xu ZJ. Surgical outcome in thoracolumbar fractures managed by short-segment pedicle instrumentation. Ann Acad Med Singap. 2014;43(1):24–32.
Farrokhi MR, Razmkon A, Maghami Z, Nikoo Z. Inclusion of the fracture level in short segment fixation of thoracolumbar fractures. Eur Spine J. 2010;19(10):1651–6.
Fradet L, et al. Biomechanics of thoracolumbar junction vertebral fractures from various kinematic conditions. Med Biol Eng Comput. 2014;52(1):87–94.
Eno JJ, Chen JL, Mitsunaga MM. Short same-segment fixation of thoracolumbar burst fractures. Hawaii J Med Public Health. 2012;71(1):19–22.
Kim HS, et al. Short segment fixation for thoracolumbar burst fracture accompanying osteopenia: a comparative study. J Korean Neurosurg Soc. 2013;53(1):26–30.
Watts A, et al. A biomechanical comparison of short segment long bone fracture fixation techniques: single large fragment plate versus 2 small fragment plates. J Orthop Trauma. 2012;26(9):528–32.
Mahar A, et al. Short-segment fixation of lumbar burst fractures using pedicle fixation at the level of the fracture. Spine (Phila Pa 1976). 2007;32(14):1503–7.
Ilharreborde B, et al. Circumferential fusion with anterior strut grafting and short-segment multipoint posterior fixation for burst fractures in skeletally immature patients: a preliminary report. J Pediatr Orthop. 2012;32(5):440–4.
Funding
All patients included in this study were operated under the cover of the Egyptian Health Insurance System. The procedures were done in the Ain Shams University Hospitals and the Arab Contractors Medical Center. The study design and statistical methodology was approved by the Ain Shams University Ethical Committee Review.
Availability of data and materials
Readers can find the supporting data of this study in the following link: https://doi.org/10.5281/zenodo.1210185.
Author information
Authors and Affiliations
Contributions
AMS, AKA, and MAH contributed to the study conception and design. AMS, WAAG, AFT, SHAM, AABS, and MSK contributed to the acquisition of data. AMS and MAN contributed to the analysis and interpretation of data. WAAG and MAN contributed to the drafting of the manuscript. WAAG contributed to the revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Consent for publication
This study reported no personal data for any patients; informed consents were obtained for all patients included in this study for participation and publish of results.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sallam, A.M., Abdel Ghany, W.A., Ali, A.K. et al. Short-segment posterior fixation with index level screws versus long-segment posterior fixation for thoracolumbar spine fracture: angle of correction and pain. Egypt J Neurosurg 33, 11 (2018). https://doi.org/10.1186/s41984-018-0012-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41984-018-0012-9