
Abstract
Background
Multiple sclerosis (MS) is an immune-mediated, neurodegenerative disease with devastating, disabling, and negative impacts on the patients’ quality of life (QoL). Although MS was not known in Sudan, it seems to be rising in recent years. This is a cross-sectional, hospital-based study aimed at assessing the impact of MS medications on patients’ QoL in neurology clinics in Khartoum City. Sixty-four patients diagnosed with MS were recruited. SF-36 questionnaire was used to assess the patients’ QoL. Data were collected from patients’ records in addition to the hand-delivered questionnaire. Data were analyzed using ANOVA test and logistic regression; p ≤ 0.05 was considered statistically significant.
Results
The majority of patients were females from north Sudan (92.2%). The mean age was 28.2 ± 6.5. Relapsing–remitting was the most diagnosed MS type (65.6%). Fatigue and urinary incontinence were the most observed symptoms. All patients had vitamin D deficiency (5–20 ng/ml). Disease-modifying therapies (DMTs) were prescribed to 37.5% of patients.
The overall mean QoL was 53.9 ± 14.7 with fair physical and mental health (51.8 ± 19.2 and 57.0 ± 10.9, respectively). Patients on DMTs showed a significantly good QoL compared to azathioprine (p ≤ 0.01), corticosteroids (p ≤ 0.01.), and no medications (p ≤ 001). Azathioprine (OR = 0.12; p ≤ 0.05), corticosteroids (OR = 0.14; p ≤ 0.05) and no treatment (OR = 0.01; p ≤ 0.001) negatively affected MS patients’ QoL when compared to DMTs. Vitamin D supplementation was significantly (p ≤ 0.01) associated with good QoL.
Conclusions
MS was prominent in young females’ descendants of Sudanese northern tribes. DMTs improve the devastating effect of MS on patients’ QoL, and vitamin D supplementation was significantly associated with good QoL of MS patients.
Similar content being viewed by others


Background
Multiple sclerosis (MS) is an immune-mediated neurodegenerative disease which precipitates devastating, disabling, and negative impact on the patients’ overall quality of life (QoL). The disease was prevalent in the northern hemisphere of the globe which was thought to be associated with the amount of sun exposure and consequently the amount of vitamin D as the gradient moves away from the equator [1]. The sub-Sahara countries, including Sudan, have extremely low incidence of MS [2, 3]. MS was observed to be more prominent in female than males. The peak onset of the disease remains mainly between 20 and 40 years of age, but it can be detected in individuals over 60 years or younger than 20 [4, 5].
The disease was characterized by several clinical manifestations including motor impairment, autonomic dysfunction and psycho-behavioral deficits [6]. Cognitive impairment is widely recognized as a core feature of MS that negatively affects the patient’s daily activities [7]. The majority of MS patients suffer from episodic neurological symptoms with relapsing–remitting MS (RRMS). Other forms of MS include the primary progressive MS (PPMS) and secondary-progressive MS (SPMS) [8]. Multiple sclerosis may initially present as a clinically isolated syndrome (CIS) [9].
The relapsing–remitting episodes of the neurological symptoms were the characteristic signs underpinning the pathology of the condition, which can be clinically detected within the early stages of the disease course [6].
The etiology and pathogenesis of MS remain debatable; nevertheless, genetic susceptibilities, infections, nutritional and environmental factors, may play key roles in the development of MS [10,11,12]. The disease is underlined by demyelination, plaque buildup, and the recruitment of microglial cells that induces oxidative stress, inflammatory cascades and consequently disturb the redox homeostasis within the central nervous system (CNS) [13, 14]. The inflammatory state precipitates loss of the myelin-sheath surrounding the nerve axons resulting in MS relapses. Reactive radicals and degraded products of biological molecules had been detected within the CNS of MS patients. Accordingly, redox biomarkers were identified as promising tools for the diagnosis and evaluation of MS disease course [13, 14]. A link between tryptophan–kynurenine (TRP–KYN) metabolic pathway and the pathology of psychiatric and neurodegenerative disorders was reported [15, 16]. The TRP-KYN pathway synthesizes paradoxical products including oxidants, antioxidants, neurotoxins, neuroprotectants, anti-inflammatory and immunomodulators in certain pathological conditions [15, 16]. Tryptophan–kynurenine metabolites were observed to be significantly raised in the serum of MS patient [17]. Kynurenines downregulate the effector T cells and induce regulatory T cells (Tregs), which cause immune tolerance. The cytotoxic T-lymphocyte antigen 4 (CTLA-4) acts as a negative regulator of T cell-dependent immune responses and suppresses the immune system [16]; hence, low levels of CTLA-4 may be disadvantageous in MS. Cytotoxic T-lymphocyte antigen 4, kynurenines and its metabolites may be considered potential biomarkers for the diagnosis and prognosis of MS. In addition, they may serve as promising drug targets for MS treatment in the future [18].
Multiple sclerosis association with genetics was well reported. The identification of the responsible alleles that act as a pre-disposing factor for MS, were behind the development of the successful Disease-modifying therapies (DMTs) (glatiramer acetate and interferon beta) [19]. Generally, genetic polymorphisms may influence the effectiveness of the DMTs, causing inter-individual variation in response to medications. It was observed that 30% of patients respond well to glatiramer acetate while 30–50% of patients do not respond optimally to IFN-β. Hence, extensive research focusing on the pharmacogenetic markers was ongoing to predict the individual variations in the response of DMTs in MS patients [20, 21]. Other recent advances in MS therapies include the stem cell-based therapy which is still under extensive research. On the other hand, stem cell-transplant—which is expected to reverse MS disabilities—reached clinical trials for patients with aggressive MS [22, 23]. The promotion of remyelination is a crucial therapeutic goal. Fibronectin (extracellular matrix protein) impairs remyelination via fibronectin-mediated microglia and macrophage dysfunction. Therefore, fibronectin-directed therapies, using nanocarrier systems, are promising in overcoming fibronectin-mediated remyelination failure and minimizing disease progression [24, 25].
The diagnosis of MS should be based on a combination of clinical symptoms, radiographic and laboratory findings. Magnetic resonance imaging (MRI) of the brain and spinal cord is often a confirmatory test when coupled with supportive clinical lesions. Further laboratory tests, such as spinal fluid analysis, are needed to rule out other neurodegenerative diseases [26].
In clinical practice, more than 18 DMTs options are currently approved by the US Food and Drug Administration (FDA) to reduce the MS severity, relapse and progression [8, 22, 27,28,29]. Ocrelizumab was approved by the FDA as the first-line for the treatment of RRMS and PPMS [30]. Siponimod, another FDA-approved DMT, is effective in decreasing the MRI lesions, relapse activity and disability progression in patients with relapsing forms of MS [31]. Newer oral versions of DMTs, such as fingolimod, natalizumab, alemtuzumab and ocrelizumab, showed reliable effects in improving the clinical and radiological features of the disease, as well as alleviating disability compared with the injectable forms of interferons and glatiramer acetate [32,33,34]. For newly diagnosed patients with RRMS, early treatment with high-efficacy DMTs (ofatumumab, ocrelizumab, natalizumab, alemtuzumab, and cladribine) may improve the long-term clinical outcomes by diminishing the early neurological damage [29]. In Sudan, the only available DMT is interferon beta-1a; the newer DMTs are unavailable and unaffordable for most MS patients in Sudan [35]. In practice, short courses of corticosteroids were used to alleviate the relapsing symptoms [36, 37].
Although the impact of vitamin D supplementation on the disease course was still debatable, and in need of more research, yet a line of evidence had linked MS progression with vitamin D deficiency. It was reported that vitamin D supplementation reduces clinically active MS symptoms and decreases the relapses rate [38]. Combined therapy of vitamin D3-tolerogenic dendritic cells plus IFN-β ameliorates the disease course [39].
Quality of life of MS patients has considerable importance in clinical practice as MS was frequently associated with mental and physical impairments [40]. Multidisciplinary approach was considered fundamental for better QoL; several neuropsychological screening tests facilitate better treatment interventions and more focused management decisions. In routine clinical practice, cognitive assessment helps in early detection of cognitive impairment and implementation of preventive measures and therapeutic interventions [7, 41]. Implementation of psychological support programs that address the negative impact of the COVID-19 pandemic on MS patients was considered important to strengthen the therapeutic alliance and improve the QoL [42, 43]. This study was designed to assess the impact of the available MS therapies on the QoL of Sudanese patients with MS at Khartoum City.
Methods
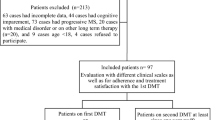
A descriptive, cross-sectional, hospital-based study was conducted in six referral neurology clinics (five private hospitals and one State Teaching Hospital). Data were collected from April 2019 to August 2019, and a total coverage sample was used. A total of 69 patients who attended these six neurology clinics in Khartoum City were registered and then sorted out into 64 patients, including men and women. Five patients were excluded because they were critically ill, unable to communicate, or unwilling to give informed consent, in addition to one child.
A self-constructed data collection sheet was used to collect data from paper-based medical records plus a questionnaire delivered by hand to patients at the referral clinics. Informed consent was obtained from all patients prior to handing the questionnaire. The data collection sheet was composed of three major parts. Part one and two contain patients' demographic and clinical information (3 and 5 items, respectively). Clinical data included the type of disease, diagnostic test, number of attacks/years, and symptoms of the disease. Part three covered the prescribed medications for the management of the disease. Multiple sclerosis diagnosis was based on clinical, radiological, and biochemical laboratory investigations for all participants. McDonald's diagnostic criteria were applied for all patients, including patients experiencing clinically isolated syndrome (CIS) and patients with progressive disease. Magnetic resonance imaging (MRI) is the test of choice for MS diagnosis in Sudan. Laboratory tests, including cerebrospinal fluid analysis, were also performed if it is affordable to the patients [44].
The questionnaire was based on the 36-item Short-Form Health Survey (SF-36) to assess the patients’ QoL. The original questionnaire has good reliability and validity as evidenced by McHorney and colleagues [45]. The SF-36 questionnaire consists of various scales which were summarized into two: physical health composite and mental health composite. Physical health composite includes physical functioning, role limitations due to physical problems, bodily pain, fatigue/energy, and general health. Mental health composite contains emotional well-being, role limitations due to emotional problems, and social function. The scoring method is based on rating the QoL of patients from 0 (weak health) to 100 (optimal health). Quality of life was categorized into poor (mean score ≤ 33.3), intermediate (mean score 33.4–66.7) and good QoL (mean score > 66.7). To study the influence of medications on QoL of patients, the data were stratified according to the patients’ medications (patients taking DMTs, azathioprine, corticosteroids or no treatment). Quality of life was evaluated in each group for comparison analysis.
The data were coded, entered in an Excel sheet and analyzed with Statistical Package for the Social Sciences (SPSS) (version 21-2012, IBM Corporation, USA). The continuous variables (physical health domain, mental health domain and total QoL score) were summarized as mean and standard deviation. Categorical data (age, gender, tribe, attacks/year, vitamin D levels, prescribed MS medications, and categories of QoL) were calculated as frequency and percentage. The association between dependent (quality of life) and independent variables (age, numbers of attacks/year and medications) was measured with logistic regression analysis that determined the adjusted odds ratio (OR) and confidence intervals (CI). Comparatively, analysis of variance (ANOVA) test (one-way ANOVA, followed by post hoc test) was used to compare between quantitative variables (overall score of QoL, physical health and mental health states of patients taking different treatment modalities). Chi-square test was used to determine the association between categorical variables (vitamin D therapy and poor/good QoL). p-value < 0.05 was considered statistically significant.
Results
Out of 69 patients, 64 adult patients completed the questionnaire with a response rate of 92.7%. The majority of the patients were from North Sudan, and their mean age was 28.2 ± 6.5. The patients’ demographic characteristics are shown in Table 1. In addition to the medical history and neurologic examination, all patients performed brain MRI, and only 7 (10.9%) patients were diagnosed with CSF examination. Two-thirds of the patients had relapsing remitting MS, with 3–5 attacks per year. At the first presentation to the clinics, all patients were deficient in vitamin D (mean = 13.1 ± 4.6), and 6 (9.4%) patients had clinically isolated symptom (CIS) such as blurred vision (7.8%) and motor deficient (1.6%). More details about symptomatology and vitamin D status are mentioned in Table 2.
Disease-modifying therapies (DMTs) were the main line of treatment (37.5%) (Table 3). For relapse treatment, 14 (21.9%) patients received a short course of corticosteroids, either intravenous methylprednisolone (1000 mg per day for 5 days), or oral prednisolone (1 mg/kg per day, with a tapering dose, for 2 weeks). Most patients received supplementary therapy such as vitamin D (Initial dose: 1000–10000 IU per day; maintenance dose: 1000 IU/day or 50,000 IU/week), and multivitamins/omega 3. All patients received symptomatic treatments, such as analgesic, antispasmodic, or laxative drug (Table 3).
The overall score of patients' QoL was 53.9 ± 14.7, with intermediate level of physical health (51.8 ± 19.2) and mental health (57.0 ± 10.9). The overall patients’ QoL showed that 67.2% had intermediate level of QoL (Table 4).
The influence of medications on QoL of patients was evaluated by stratifying the QoL according to their medications (DMTs, azathioprine, corticosteroids or no treatment). The overall QoL of patients taking DMTs was observed to be better than those taking azathioprine (p ≤ 0.01), short courses of corticosteroids (p ≤ 0.01) and patients taking no medications (p ≤ 0.001). Physical health of patients taking DMTs were significantly better than those on azathioprine (p ≤ 0.01), short courses of oral or intravenous corticosteroids (p ≤ 0.01) and patients who were not under any medication (p ≤ 0.001). Mental health state of patients on DMTs was significantly higher than those taking short courses of corticosteroids (p ≤ 0.05) and patients taking no medications (p ≤ 0.001). On the other hand, patients on azathioprine had significantly high levels of overall QoL, physical activity and mental health (p ≤ 0.001, p ≤ 0.001 and p ≤ 0.05, respectively) than patients without medications (Fig. 1). A significant association had been observed between vitamin D and QoL of patients with MS (p ≤ 0.01) (Supplementary file 1).

Stratification of QOL of patients with multiple sclerosis (MS) based on their MS medications. ***p ≤ 0.001, **p ≤ 0.01and *p ≤ 0.05 (different medications compared with no treatment); †††p ≤ 0.001 and ††p ≤ 0.01 (different medications compared with corticosteroids); ‡‡p ≤ 0.01 and ‡p ≤ 0.05 (different medications compared with azathioprine), DMTs disease-modifying therapies, QoL quality of life
Predictors of good QoL among MS patients were evaluated using logistic regression analysis. Patients on azathioprine (OR = 0.12, 95% CI = 0.02–0.70, p ≤ 0.05) were less likely to have good QoL than those receiving DMTs. Moreover, there was less likelihood of having good QoL among patients receiving short courses of corticosteroids (either oral or IV) for the treatment of relapses (OR = 0.14, 95% CI = 0.02–0.86, p ≤ 0.05) or patients with no treatments (OR = 0.01, 95% CI = 0.001–0.14, p ≤ 0.001) when compared to patients taking DMTs (Table 5).
Discussion
This study was designed to evaluate the impact of MS medications on the QoL of Sudanese patients in Khartoum City. Our results showed that the majority of the assessed patients were young females from Sudanese northern tribes, with a mean age of 28.2 ± 6.5 years. This result is in line with literature that reported MS as more prevalent in women than men and usually occurs in the ages of 20–40, but it can also develop in older adults and rarely in children [46, 47]. Tribes from the northern region (a hybrid African-Arab race) were the most affected, while no incidence of the disease was observed in the south or west regions. The reason behind this ethnic variation was not known yet, but it could be due to genetic traits or environmental factors [48]. The association between MS and genetic factors was well reported [19].
Magnetic resonance imaging was adopted as the main diagnostic tool for the MS patients in Sudan. The updated McDonald diagnostic criteria have been applied for the diagnosis of clinically isolated syndrome as well as the progressive stage [44]. Cerebrospinal fluid was done for a limited number of patients as the test was quite unaffordable for most patients. Two-thirds of the patients were diagnosed with relapsing remitting MS phenotype, with 3–5 attacks per year. This result is in line with that has been reported by Idris et al.; relapsing remitting MS was the most common course affecting MS patients in Sudan [48]. Vitamin D was observed to be low (less than 15 ng/ml) in two-thirds of the assessed patients. Low levels of vitamin D were reported in MS patients especially at the northern hemisphere. In contrast, people in countries that lie around the equator, including Sudan, had been thought to have extremely low risk of MS and adequate levels of vitamin D [2].
Most patients attended the neurology clinics with multiple symptoms in the first episode, yet a limited number attended the clinics with some isolated symptoms, including blurred vision and paralysis. According to Langer-Gould and his colleagues, the CIS incidence among MS patients was rare (about 3.4 per 100,000 person/year) at the beginning of the disease course [49]. The most observed ongoing symptoms include fatigue, urinary incontinence, sensory deficit, hemifacial spasm, painful ocular motility, constipation, and trigeminal neuralgia. However, few patients experienced reversible visual loss. The clinical manifestations of the disease in this study were in line with earlier studies that reported bladder dysfunction, sensory disturbances, painful ocular motility, constipation, and walking difficulties as the most common complications of MS patients [48, 50, 51].
Disease-modifying therapies were observed to be the most prescribed drugs in combination with vitamin D and multivitamins. About one-third of patients received injectable interferon beta1a, and a limited number of patients were on oral DMTs (fingolimod or dimethyl fumarate). Generally, the unavailability of MS medications (especially DMTs) in Sudan was an ongoing difficulty for MS patients. To the best of our knowledge, patients on MS medications hardly try to attain their medications, in particular oral DMTs, from outside Sudan on private bases. About one-third of patients were treated with azathioprine. Acute relapses were managed with a 5-day course of intravenous methylprednisolone followed by oral prednisolone that was tapered off over 2 weeks. Steroids are the cornerstone therapies for treating acute MS relapses by reducing MS-related morbidity [37]. Vitamin D deficiency was observed in all patients in this study; a significant positive association had been observed between patients taking vitamin D supplementation and good QoL of patients. This finding concurs well with a previous survey. Vitamin D deficiency may play a key role in the pathogenesis of MS, and hypovitaminosis in MS patients is commonly associated with fatigue and seizure that negatively affect the QoL. On the other hand, the use of vitamin D supplements for MS patients remains debatable [38, 52, 53].
The QoL assessment showed that more than two-thirds of the recruited MS patients have fair levels of physical activity (51.8 ± 19.2) and mental health (57.0 ± 10.9). This result is consistent with a previous study in MS patients showing a mental health score of 53.1 ± 22.5 [54]. In contrast, earlier studies in Sudan and Mexico had shown higher scores of QoL in MS patients (66.4 ± 21.9 and 64.6 ± 17.5, respectively) [46, 55]. Such discrepancies could be attributed to differences in the QoL assessment tool or symptoms, signs, duration, severity of the disease or individual variations between MS patients [54]. Moreover, the study results showed that DMTs significantly improved QoL of the MS patients when compared to azathioprine, short courses of corticosteroids or no medication. This finding is in accordance with the reported data [56]. Disease-modifying therapies positively impact the MS patients' QoL, as shown in patients treated with glatiramer acetate [56]. Through the aggressive treatment approach with high-efficacy disease-modifying therapies, a positive long-term impact on MS patients' well-being could be achieved [57]. However, Simone et al., had shown IFN-β may induce a negative impact on MS patients QoL over time [58]. On the other hand, patients on azathioprine had significantly high levels of physical activity and mental health compared to those on no medications which was reflected on the overall good QoL. Patients on steroids or no treatment showed poor QoL. High-dose steroids are reserved for severe flare ups or periodic episodes of disease activity. Corticosteroids' side effects, such as depression, psychosis, cognitive impairment, hyperglycemia, and stomach irritation, reduce the patients' QoL with disease progression over time [59].
In clinical practice, physical and mental health of MS patients are emerging as important parameters to assess the effects of medications on QoL. Evaluation of the QoL may be beneficial in guiding the physicians to develop stratified interventions and specific plans for effective treatments tailored according to each patient's needs [56].
Conclusions
This study showed that the incidence of MS among Sudanese patients was high in young females from Sudanese northern tribes. Within the assessed patients, the relapsing remitting MS was the most observed type. The majority of patients had fair QoL, yet a limited number showed poor levels of physical and mental functioning.
The most frequently prescribed medications were DMTs which significantly improve QoL of MS patients when compared to other therapies. One-third of the patients were using injectable IFN-β. Unfortunately, oral DMTs have not yet been available or affordable for MS patients in Sudan.
Azathioprine showed significant improvement on physical activity and mental health compared to those on no medications. Although azathioprine was not approved by the FDA for MS treatment, yet, it has been used as an alternative for patients who could not tolerate DMTs or afford the high cost of DMTs [60]. On the other hand, it has been reported by Luca et al., that azathioprine efficacy was comparable to β interferons in patients with relapsing–remitting MS [61].
Limitations
The main limitations of this study include difficulty to achieve a large sample size of MS patients as the study was conducted at specific neurology referral clinics in Khartoum City. The study was bounded by a specific time window. The patients' responses to the questionnaire may be susceptible to recall bias and/or social stigmas.
Recommendations
Educational programs about adherence to medications and medical care follow-up may improve the QoL of MS patients. Integration of palliative and supportive care, such as psychological, social, spiritual support and physiotherapy, into the patient treatment plan are recommended to reduce the devastating impact of the disease on the patient’s general health and QoL. Individual evaluation of the patient's needs in clinical practice may help in establishing better management strategies, and tailored stratified interventions to implement personalized treatment plans according to the patient's needs. The study has shed light on the high incidence of MS in the northern region of Sudan, with almost 97% of cases, compared to no cases in the South and East regions; more studies focusing on genetic and environmental factors that could be behind such high incidence are recommended. A tailored study to investigate MS among children in Sudan is recommended. The availability of medical care for this category of patients was available only in Khartoum State, which enforced these patients to endure long hours of travel to receive medical care. Establishing specialized clinics in areas of high incidence is urgently needed. Potentially this study would encourage the authorities to prioritize the MS health services and medications availability for this important category of patients at areas of high incidence.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request. Email: imanabdoon@yahoo.com.
Abbreviations
- MS:
-
Multiple sclerosis
- QoL:
-
Quality of life
- DMTs:
-
Disease-modifying therapies
- CIS:
-
Clinically isolated syndrome
- MRI:
-
Magnetic resonance imaging
- CSF:
-
Cerebrospinal fluid
- CNS:
-
Central nervous system
- 36-SF:
-
36-Short Form Survey
- FDA:
-
Food and Drug Administration
- SPSS:
-
Statistical Package for the Social Sciences
- ANOVA:
-
Analysis of variance
- OR:
-
Odds ratio
References
Pierrot-Deseilligny C, Souberbielle JC. Vitamin D and multiple sclerosis: an update. Mult Scler Relat Disord. 2017;14:35–45.
Simpson S Jr, Blizzard L, Otahal P, Van der Mei I, Taylor B. Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. J Neurol Neurosurg Psychiatry. 2011;82:1132–41.
Ostkamp P, Salmen A, Pignolet B, Görlich D, Andlauer TFM, Schulte-Mecklenbeck A, et al. Sunlight exposure exerts immunomodulatory effects to reduce multiple sclerosis severity. Proc Natl Acad Sci. 2021;118: e2018457118.
Waldman A, Ghezzi A, Bar-Or A, Mikaeloff Y, Tardieu M, Banwell B. Multiple sclerosis in children: an update on clinical diagnosis, therapeutic strategies, and research. Lancet Neurol. 2014;13:936–48.
Naseri A, Nasiri E, Sahraian MA, Daneshvar S, Talebi M. Clinical features of late-onset multiple sclerosis: a systematic review and meta-analysis. Mult Scler Relat Disord. 2021;50: 102816.
Javalkar V, McGee J, Minagar A. clinical manifestations of multiple sclerosis: an overview. In: Minagar A, editor. Multiple sclerosis. San Diego: Academic Press; 2016. p. 1–12.
Portaccio E, Amato MP. Cognitive impairment in multiple sclerosis: an update on assessment and management. NeuroSci. 2022;3:667–76.
Goldschmidt C, McGinley MP. Advances in the treatment of multiple sclerosis. Neurol Clin. 2021;39:21–33.
López-Gómez J, Sacristán-Enciso B, Caro-Miró MA, Querol Pascual MR. Clinically isolated syndrome: diagnosis and risk of developing clinically definite multiple sclerosis. Neurologia (Engl Ed). 2021;S0213-4853(21)(00028-1).
Michel L. Environmental factors in the development of multiple sclerosis. Rev Neurol. 2018;174:372–7.
Sini P, Dang TBC, Fais M, Galioto M, Padedda BM, Lugliè A, et al. Cyanobacteria, cyanotoxins, and neurodegenerative diseases: dangerous liaisons. Int J Mol Sci. 2021;22:8726.
Ciccarelli O, Barkhof F, Bodini B, Stefano ND, Golay X, Nicolay K, et al. Pathogenesis of multiple sclerosis: insights from molecular and metabolic imaging. Lancet Neurol. 2014;13:807–22.
Tanaka M, Vécsei L. Monitoring the redox status in multiple sclerosis. Biomedicines. 2020;8:406.
Arslan B, Arslan GA, Tuncer A, Karabudak R, Dinçel AS. Evaluation of thiol homeostasis in multiple sclerosis and neuromyelitis optica spectrum disorders. Front Neurol. 2021;12:1348.
Tanaka M, Tóth F, Polyák H, Szabó Á, Mándi Y, Vécsei L. Immune influencers in action: metabolites and enzymes of the tryptophan-kynurenine metabolic pathway. Biomedicines. 2021;9:734.
Tanaka M, Toldi J, Vécsei L. Exploring the etiological links behind neurodegenerative diseases: inflammatory cytokines and bioactive kynurenines. Int J Mol Sci. 2020;21:2431.
Tanaka M, Szabó Á, Spekker E, Polyák H, Tóth F, Vécsei L. Mitochondrial impairment: a common motif in neuropsychiatric presentation? The link to the tryptophan-kynurenine metabolic system. Cells. 2022;11:2607.
Basile MS, Bramanti P, Mazzon E. The role of cytotoxic T-lymphocyte antigen 4 in the pathogenesis of multiple sclerosis. Genes (Basel). 2022;13:1319.
Parnell GP, Booth DR. The multiple sclerosis (MS) genetic risk factors indicate both acquired and innate immune cell subsets contribute to MS pathogenesis and identify novel therapeutic opportunities. Front Immunol. 2017;8:425.
Carrasco-Campos MI, Pérez-Ramírez C, Macías-Cortés E, Puerta-García E, Sánchez-Pozo A, Arnal-García C, et al. Pharmacogenetic predictors of response to interferon beta therapy in multiple sclerosis. Mol Neurobiol. 2021;58:4716–26.
Zarzuelo-Romero MJ, Pérez-Ramírez C, Cura Y, Carrasco-Campos MI, Marangoni-Iglecias LM, Ramírez-Tortosa MC, et al. Influence of genetic polymorphisms on clinical outcomes of glatiramer acetate in multiple sclerosis patients. J Pers Med. 2021;11:1032.
Bross M, Hackett M, Bernitsas E. Approved and emerging disease modifying therapies on neurodegeneration in multiple sclerosis. Int J Mol Sci. 2020;21:4312.
Smith JA, Nicaise AM, Ionescu RB, Hamel R, Peruzzotti-Jametti L, Pluchino S. Stem cell therapies for progressive multiple sclerosis. Front Cell Dev Biol. 2021;9: 696434.
van Schaik PEM, Zuhorn IS, Baron W. Targeting fibronectin to overcome remyelination failure in multiple sclerosis: the need for brain- and lesion-targeted drug delivery. Int J Mol Sci. 2022;23:8418.
Wei SS, Chen L, Yang FY, Wang SQ, Wang P. The role of fibronectin in multiple sclerosis and the effect of drug delivery across the blood-brain barrier. Neural Regen Res. 2023;18:2147–55.
Travers BS, Tsang BK, Barton JL. Multiple sclerosis: diagnosis, disease-modifying therapy and prognosis. Aust J Gen Pract. 2022;51:199–206.
Abdel-mannan OA, Manchoon C, Rossor T, Southin JC, Tur C, Brownlee W, et al. Use of disease-modifying therapies in pediatric relapsing-remitting multiple sclerosis in the United Kingdom. Neurol Neuroimmunol Neuroinflamm. 2021;8: e1008.
Bourque J, Hawiger D. Current and future immunotherapies for multiple sclerosis. Mo Med. 2021;118:334–9.
Freeman L, Longbrake EE, Coyle PK, Hendin B, Vollmer T. High-efficacy therapies for treatment-naïve individuals with relapsing-remitting multiple sclerosis. CNS Drugs. 2022;36:1285–99.
Lin M, Zhang J, Zhang Y, Luo J, Shi S. Ocrelizumab for multiple sclerosis. Cochrane Database Syst Rev. 2022;5: CD013247.
Cohan SL, Benedict RHB, Cree BAC, DeLuca J, Hua LH, Chun J. The two sides of siponimod: evidence for brain and immune mechanisms in multiple sclerosis. CNS Drugs. 2022;36:703–19.
Jalkh G, Abi Nahed R, Macaron G, Rensel M. Safety of newer disease modifying therapies in multiple sclerosis. Vaccines (Basel). 2020;9:12.
Boziki M, Bakirtzis C, Sintila SA, Kesidou E, Gounari E, Ioakimidou A, et al. Ocrelizumab in patients with active primary progressive multiple sclerosis: clinical outcomes and immune markers of treatment response. Cells. 2022;11:1959.
Hauser SL, Bar-Or A, Comi G, Giovannoni G, Hartung HP, Hemmer B, et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. 2017;376:221–34.
Ibrahim EAA, Gassoum A. The patterns of clinical presentation of multiple sclerosis in patients admitted to the national center of neurological sciences, Khartoum, Sudan 2018. Mult Scler Relat Disord. 2018;26:238.
Berkovich R. Treatment of acute relapses in multiple sclerosis. Neurotherapeutics. 2013;10:97–105.
Smets I, Van Deun L, Bohyn C, van Pesch V, Vanopdenbosch L, Dive D, et al. Corticosteroids in the management of acute multiple sclerosis exacerbations. Acta Neurol Belg. 2017;117:623–33.
Boltjes R, Knippenberg S, Gerlach O, Hupperts R, Damoiseaux J. Vitamin D supplementation in multiple sclerosis: an expert opinion based on the review of current evidence. Expert Rev Neurother. 2021;21:715–25.
Quirant-Sánchez B, Mansilla MJ, Navarro-Barriuso J, Presas-Rodríguez S, Teniente-Serra A, Fondelli F, et al. Combined therapy of vitamin D3-tolerogenic dendritic cells and interferon-β in a preclinical model of multiple sclerosis. Biomedicines. 2021;9:1758.
Rezapour A, Almasian Kia A, Goodarzi S, Hasoumi M, Nouraei Motlagh S, Vahedi S. The impact of disease characteristics on multiple sclerosis patients’ quality of life. Epidemiol Health. 2017;39: e2017008.
Taranu D, Tumani H, Holbrook J, Tumani V, Uttner I, Fissler P. The TRACK-MS test battery: a very brief tool to track multiple sclerosis-related cognitive impairment. Biomedicines. 2022;10:2975.
Donisi V, Gajofatto A, Mazzi MA, Gobbin F, Busch IM, Ghellere A, et al. Insights for fostering resilience in young adults with multiple sclerosis in the aftermath of the COVID-19 emergency: an Italian survey. Front Psychiatry. 2020;11: 588275.
Gil-González I, Martín-Rodríguez A, Conrad R, Pérez-San-Gregorio M. Quality of life in adults with multiple sclerosis: a systematic review. BMJ Open. 2020;10: e041249.
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17:162–73.
McHorney CA, Ware Jr JE, Lu JF, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care. 1994;32:40–66.
Ibrahim EAAE, Gassoum A, IshagAgib IEI. Quality of life among Sudanese patients with multiple sclerosis in Khartoum state using (MSQoL-54) questionnaire. BMC Res Notes. 2019;12:533.
Romero-Pinel L, Bau L, Matas E, León I, Muñoz-Vendrell A, Arroyo P, et al. The age at onset of relapsing-remitting multiple sclerosis has increased over the last five decades. Mult Scler Relat Disord. 2022;68: 104103.
Idris MN, Sokrab TE, Ibrahim EA, Ali HE, Elzibair MA, Abadalatif M, et al. Multiple sclerosis in Sudan: a prospective study of clinical presentation and outcome. Mult Scler. 2009;15:1537–8.
Langer-Gould A, Brara SM, Beaber BE, Zhang JL. The incidence of clinically isolated syndrome in a multi-ethnic cohort. J Neurol. 2014;261:1349–55.
Ghasemi N, Razavi S, Nikzad E. Multiple sclerosis: pathogenesis, symptoms, diagnoses and cell-based therapy. Cell J. 2017;19:1–10.
Ford H. Clinical presentation and diagnosis of multiple sclerosis. Clin Med (Lond). 2020;20:380–3.
Feige J, Moser T, Bieler L, Schwenker K, Hauer L, Sellner J. Vitamin D supplementation in multiple sclerosis: a critical analysis of potentials and threats. Nutrients. 2020;12:783.
Ayele BA, Wuhib MZ, Zenebe BG, Metaferia GZ. Serum vitamin D level among multiple sclerosis patients in the tropics: experience from a private clinic in Addis Ababa, Ethiopia. Ethiop J Health Sci. 2021;31:611–8.
Visser LA, Louapre C, Uyl-de Groot CA, Redekop WK. Health-related quality of life of multiple sclerosis patients: a European multi-country study. Arch Public Health. 2021;79:39.
Ochoa-Morales A, Hernández-Mojica T, Paz-Rodríguez F, Jara-Prado A, Trujillo-De Los Santos Z, Sánchez-Guzmán MA, et al. Quality of life in patients with multiple sclerosis and its association with depressive symptoms and physical disability. Mult Scler Relat Disord. 2019;36: 101386.
Jongen PJ. Health-related quality of life in patients with multiple sclerosis: impact of disease-modifying drugs. CNS Drugs. 2017;31:585–602.
Simonsen CS, Flemmen H, Broch L, Brunborg C, Berg-Hansen P, Moen SM, et al. Early high efficacy treatment in multiple sclerosis is the best predictor of future disease activity over 1 and 2 years in a Norwegian population-based registry. Front Neurol. 2021;12: 693017.
Simone IL, Ceccarelli A, Tortorella C, Bellacosa A, Pellegrini F, Plasmati I, et al. Influence of interferon beta treatment on quality of life in multiple sclerosis patients. Health Qual Life Outcomes. 2006;4:96.
Ou G, Bressler B, Galorport C, Lam E, Ko HH, Enns R, et al. Rate of corticosteroid-induced mood changes in patients with inflammatory bowel disease: a prospective study. J Can Assoc Gastroenterol. 2018;1:99–106.
Nonino F, Baldin E, Ridley B, Casetta I, Iuliano G, Filippini G. Azathioprine for people with multiple sclerosis. Cochrane Database Syst Rev. 2021;2021(7): CD015005.
Massacesi L, Tramacere I, Amoroso S, Battaglia MA, Benedetti MD, Filippini G, et al. Azathioprine versus beta interferons for relapsing-remitting multiple sclerosis: a multicentre randomized non-inferiority trial. PLoS ONE. 2014;9: e113371.
Acknowledgements
Not applicable.
Funding
No funds, grants, or other support was received.
Author information
Authors and Affiliations
Contributions
O.E.S. contributed to conceptualization, study design, and data collection. A.I. contributed to conceptualization, supervision, study design, data analysis and interpretation, editing, and critical revision of the manuscript. S.H.M. participated in literature reviewing, data presentation, comment on original manuscript, reviewing, and improving the final layout of the manuscript. A.S.A. contributed to drafting and reviewing the original manuscript. O.B. participated in reviewing, and critical evaluation of the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval was granted by the Ethics Committee of University of Khartoum, Faculty of Pharmacy, Research Board (No. KH-15-25-3-2019), and from the Ministry of Health, Research Department. Permission was also granted by the authorities of the neurology clinic at each participating hospital. The study was performed in line with the principles of the 1964 Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study after explaining the rationale behind the research. Voluntary participation was assured and confidentiality and anonymity of participants' information were ensured by using a coded data collection sheet.
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Omar, E.S., Suliman, H.M., Osman, B. et al. Disease-modifying therapies as positive predictors of quality of life for Sudanese patients with multiple sclerosis: a cross-sectional study. Egypt J Neurol Psychiatry Neurosurg 60, 77 (2024). https://doi.org/10.1186/s41983-024-00855-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-024-00855-3