
Abstract
Background
Multiple sclerosis (MS) is a multifactorial neurodegenerative autoimmune disease with a varied clinical course and presentation, which is more frequent than ever in the Middle East. The aim of this work is to investigate potential predictors of MS progression in order to help in early diagnose and predict progressive course of the disease.
Results
This is a retrospective case–control study conducted on a group of multiple sclerosis (MS) patients who developed secondary progression of the disease course (SPMS). The cases were matched with control MS patients who did not develop any disease progression (relapsing remitting MS (RRMS)). The matching was done for sex, and age with a ratio 1:1, total of 150 patients were included as cases and were matched with 150 control patients. Significant associations between MS progression and smoking, vitamin D deficiency, disease duration, delay in MS diagnosis, unemployment, site and number of lesions, and number of black holes were reported. About half of SPMS patients (53.3%) had 3 or more spinal lesions compared to only 1.4% of RRMS patients (p < 0.001). Moreover, about 76% of RRMS patients had no black holes in their radiological finding, while it was found that 35.3% of the SPMS patients had more than 5 black holes, compared to 8% of RRMS patients. Additionally, juxta-cortical site lesions were more frequent in SPMS than that in RRMS in a percentage 72.7 and 46%, respectively. Also, infra-tentorial lesions were found to be more frequent in SPMS group rather than RRMS group 92% and 78.7%, respectively.
On the other hand, a lower SDMT scale was associated with a shorter time to SPMS diagnosis in the multivariate Cox regression analysis adjusted to baseline factors and 25-FWT (HR: 0.928, 95% CI: 0.906–0.95).
Conclusions
MS secondary progression can be predicted among MS patients in routine practice comprising exposure history, clinical assessment, laboratory findings, and radiological examinations.
Similar content being viewed by others
Background
Multiple sclerosis (MS) is a chronic, seriously debilitating condition that has a significant social and economic impact. In young adults, it is the main contributor of non-traumatic impairment [1]. The most prevalent form of MS at disease onset, particularly in young patients, is RRMS. It is characterized by distinct attacks with complete or partial recovery (also known as relapses, flares, or exacerbations). There is little disease progression between relapses, while the relapses themselves may occasionally result in significant residual disability [2]. An initial RRMS disease course, followed by gradual worsening with or without sporadic relapses, small remissions, and plateaus, defines SPMS. SPMS is diagnosed retrospectively, and there are no recognized criteria to determine when RRMS transforms into it [3]. Secondary progressive multiple sclerosis was reported to occur in about 50% with 15 years [4] and roughly 80% within 20 years among people with RRMS that may be lower with newer disease-modifying drugs [5]. Because of the heterogeneity associated with the clinical presentation of SPMS, establishing a precise diagnosis is challenging as it is hindered by the lack of precise clinical, radiological, immunologic or pathologic criteria to determine the transition to SPMS [6]. Therefore, SPMS diagnosis is entirely based on clinical judgment which is done retrospectively and delayed up to 3 years due to several patient- and clinician-related factors [7]. However, the definition of secondary progression is not always easy to apply in clinical practice because of its wide spectrum including deterioration independent of relapses for more than 6 months following an initial RRMS. On the other hand, the optimal time after RRMS onset to assess for the secondary progression has not been exactly determined. The mean duration of progression to SPMS was 2.9 ± 0.8 years after reviewing 123 patients with RRMS in one study [8]. Another study reported an average time of 23.3 ± 1.23 months to secondary progression [9]. In investigating the potential risk factors of secondary progression of MS, some studies found associations with age at MS onset, disease-modifying drugs (DMD) [9], and first-recorded Expanded Disability Status Scale (EDSS) score [10]. It is important to establish a diagnosis criteria of SPMS through investigating sociodemographic, exposure historical, clinical, and radiological data. The present study aimed to evaluate many potential factors associated with the development of SPMS among RRMS patients.
Methods
It is a retrospective case–control study during the period from November to 2020 May 2022. Cases were selected as a consecutive sample who fulfilled the inclusion criteria comprising MS diagnosed according to McDonald criteria 2017 [11], aged more than 18 years, and clinically diagnosed with SPMS. Control patients were selected with 1:1 ratio who matched the cases for sex and age, diagnosed with MS according to McDonald criteria 2017, and clinically diagnosed with RRMS [11]. Our study adopted the definition of secondary progressive patients as any increase in EDSS by 1.5 points if the last EDSS before conversion to SPMS was 0, or increase by 1 point if the EDSS was between 1 and 5.5, or an increase by 0.5 points if the EDSS was above 5.5, if these changes occur this means that patient is stepping into the secondary progressive phase over a period of 6 months [12].
Patients with any other autoimmune disease were excluded from cases and control. For sample size calculation, we were planning a study of matched sets of cases and controls with 1 matched control per case. Prior data indicated that the probability of exposure among controls was 0.4 [14]. If the true odds ratio for disease in exposed subjects relative to unexposed subjects is 2, we would need to study 99 SPMS patients with 1:1 matched control per case to be able to reject the null hypothesis that this odds ratio equals 1 with power of 0.8. The Type I error probability associated with this test of this null hypothesis is 0.05.
Sociodemographic data, exposure history, clinical assessments, laboratory data and radiological findings were obtained from medical records. Sociodemographic data included weight, height, education level, and employment status. Comorbidities included diabetes mellitus (DM), hypertension, hypo- and hyperthyroidism, epilepsy, and deep venous thrombosis (DVT). Exposure history included smoking status, drugs, and food intake. Clinical assessments included neurological examination, MS diagnosis, assessment for deterioration, 25-feet timed walk test (25-FWT), and simple digit modalities test (SDMT). Radiological assessments included magnetic resonance imaging (MRI) of brain and spine. Patients and their relatives were contacted for any missed data.
Qualitative data were analyzed using the appropriate Chi-square or Fisher exact tests. The Chi-square test was used when at least 80% of the expected values of cells were 5 or greater. Alternatively, Fisher’s exact test was used. Numerical data were analyzed using independent samples t-test or Mann–Whitney U test as appropriate. Time analysis using multivariate Cox regression was used including all baseline data to obtain the adjusted relationship between 25-FWT and SDMT and the diagnosis time of SPMS. A receiver operating characteristic (ROC) curve was used to optimize a cutoff point for better sensitivity and specificity for either SDMT or 25-FWT. R version 4.1.1 (2021-08-10) and RStudio 2021.09.0 + 351 were used. All tests were two-tailed and conducted at a 0.05 level of significance.
Results
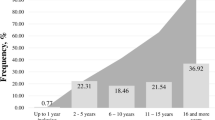
There were 150 patients diagnosed with SPMS group and 150 patients diagnosed with RRMS who served as control. The distribution of sex and age did not show significant differences between the groups. The sociodemographic and historical comparison showed that onset age was slightly higher among SPMS but insignificant. However, disease duration and time before diagnosis years were longer among SPMS compared to RRMS (p < 0.05). Additionally, more frequent diabetes, vitamin D deficiency, and smoking, less frequent employment, and higher mean BMI were reported among SPMS compared to RRMS patients (p < 0.05), as shown in Table 1.
Type and number of relapses before starting any DMD comparison showed that SPMS patients were more likely to have cerebral lesions (48%) or spinal lesions (65.3%) compared to RRMS patients. On the other hand, RRMS were more likely to have motor relapse (40.7%) compared to SPMS patients. However, brainstem, sensory and vision relapse did not differ between the groups. Number of relapses before starting DMD were higher among SPMS compared to RRMS patients with mean ± SD of (3.13 ± 2.1), respectively, as shown in Table 2.
Patients with more than 10 lesions were more frequent in SPMS group compared to RRMS group (58.7%). Additionally, juxta-cortical (72.7%) and infra-tentorial lesions (92.7%) were more frequently reported among SPMS compared to RRMS patients. Spinal lesions number more than 3 were found only in SPMS patients with 23.6% compared to 0% in RRMS group (p < 0.05). Black holes number ≥ 3 holes were more frequent in SPMS compared to RRMS group (66%) oligoclonal bands (OCB) showed larger median in SPMS that that was reported in RRMS (5) with IRQ of (2–10).
Simple digit modality test showed lower mean ± SD among SPMS patients compared to those with RRMS at the time of first diagnosis (30 ± 9.13) and at the time of the study (20.23 ± 7.6). Additionally, 25-FWT showed higher mean ± SD among SPMS patients compared to those with RRMS at the time of first diagnosis (11.83 ± 2.23) and at the time of the study (26 ± 16.86) (Table 3).
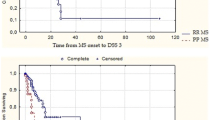
In the multivariate Cox regression analysis using, lower SDMT scale at the time of SPMS diagnosis was associated with greater hazard of progression (HR, 95% CI; 0.928, 0.906–0.95). However, the 25-FWT was not associated with SPMS diagnosis (HR, 95% CI; 1.005, 0.994–1.015) (Fig. 1). In the diagnostic accuracy analysis, a cutoff ≤ 29.5 for the SDMT scale showed a sensitivity and specificity of 96% and 88.7%, respectively, as shown in the ROC curve (Fig. 2).

Multivariate Cox regression of time to reach EDSS = 3 among MS patients

Area under the ROC curve for SDMT in the diagnosis of SPMS
Discussion
As long as the diagnosis of SPMS is challenging, the present study provides the literature with an objective tool to help in the prediction and diagnosis of secondary progressive form of MS comprising prognostic and diagnostic elements. We found in this matched case–control study that smoking, vitamin D deficiency, longer disease duration, longer time before diagnosis, unemployment, and larger BMI were associated with secondary progression among MS patients. Consistently, a retrospective study conducted on 400 MS patients of registry database in Iran found that smoking was an independent risk factor for SPMS with hazard ratio (HR) and 95% CI of 2.43 (1.28–4.6) [13]. In contrast, a survey study conducted on 364 patients with MS reported that smoking has no effect on the clinical course of the disease in multiple sclerosis [14]. Since immune cells and bodily fluids of smokers typically have greater amounts of numerous matrix metalloproteinases, upregulating these enzymes is one possible way that smoking impacts MS. The increased expression of matrix metalloproteinases in smokers may make it easier for immune cells to enter the parenchyma of the central nervous system [15]. Another cohort study using the NARCOMS Registry found that MS patients with vascular comorbidities at any time during their disease course progressed to an EDSS score of 6 on average 6 years faster than MS patients without a vascular comorbidity [16].
Vitamin D deficiency has been also reported as an environmental risk factor for secondary progression of MS. A total of 465 MS patients in a large clinical trial had a serial measures of serum 25(OH)D concentrations. The study found that lower 25(OH) vitamin D levels significantly predicted rate of secondary progression and MS activity [17]. Another study included 137 MS patients and 218 MS-free controls. The study reported that vitamin D deficiency was associated with secondary progression and disability of MS [18]. Noteworthy, vitamin D supplementation role in reducing rate of MS progression has been studied. An under power study could not prove benefits in decreasing MS progression after vitamin D supplementation with 20,000 IU vitamin D3 weekly to 35 patients [19]. The effects of vitamin D supplementation in MS are recommended to be further studied in bigger clinical trials with chosen patient groups, preferably clinically isolated syndrome patients and young patients at the time of diagnosis, using vitamin D3 supplements to obtain a 100 nmol/l level [20]. Moreover, fatigue, muscle weakness, or urinary dysfunction are symptoms of vitamin D poisoning that may resemble the progression of MS in its normal state. Given these restrictions, vitamin D supplementation in MS is a delicate task that requires medical supervision [21]. The possible underlying mechanism of vitamin D is that vitamin D also influences the development of CD4 + T helper cells, resulting in decreased production of pro-inflammatory Th1 and Th17 cells and increased production of Th2 cells, which helps to lessen the pro-inflammatory state characteristic of MS [17].
Regarding MS disease duration, the period effect, it had an impact on the entire severity spectrum and second progression. Nevertheless, the time to secondary progression could be longer with DMD [22]. Another study reported that disease duration was an independent risk factor for progression in step-wise regression analysis [23]. Relapses type and number could predict secondary prognosis of MS in the present study, whereas cerebral and spinal lesions with more than 10 relapses before starting DMD were strongly associated with SPMS. Consistent with our findings, a cross-sectional study was conducted on 113 patients involving 30 controls. The study found that the fractional anisotropy, mean diffusivity, and radial diffusivity in the grey matter and posterior columns of spinal cord were all substantially higher in SPMS than RRMS [24].
Radiological assessments in the present study using MRI revealed that number of enhanced lesions, juxta-cortical lesions, infra-tentorial lesions, number of black holes, and OCB could have diagnostic values in the identifying of secondary progression in MS. In agreement with the present study findings, baseline gadolinium-enhancing lesions and spinal cord lesions were independently linked to secondary progressive multiple sclerosis (odds ratios of 3.16 and 4.71, respectively, P 0.05) [25]. Another study reported that cortical lesion volume was an independent risk factor for MS-related disability [26]. In a more recent study, black holes, infra-tentorial lesions, and higher baseline EDSS scores were found to be potential predictors of secondary progression by univariate analysis. However, only infra-tentorial lesions were the independent risk for SPMS [27]. OCB prediction value for disease progression has been studied with conflicting results. It was associated with 20% higher risk of conversion to SPMS which agreed with our results [28]. In contrast, OCB was not associated with disease progression in a Canadian study including 1200 MS patients [29]. Another study did not find difference in OCB between RRMS and SPMS including 149 MS patients [30].
SDMT and 25-FWT evaluation scores at baseline and at the time of SPMS diagnosis in the present study showed significant differences between RRMS and SPMS indicating their beneficial roles in prediction and diagnosis of secondary progression in MS. Noteworthy, the most common used reliable and sensitive test for measuring cognition in MS patients is the SDMT [31]. Additionally, as EDSS and SDMT cover different parts of secondary progression, and the combination of SDMT and EDSS led to increased sensitivity for progression and treatment outcomes [32]. Moreover, worsening in 5 years SDMT could be predicted by baseline SDMT, age, EDSS, and T2 lesion volume [33]. In contrast, using original trial data from the 2-year ASCEND trial, it was found that SDMT might not be a reliable outcome indicator of disease progression, whereas the gradual cognitive impairment that SPMS patients endure is not captured by the SDMT [34]. On the other hand, the 25-FWT is used to detect progression. A minimum of 20% deterioration on the 25-FWT confirmed after at least 6 months was utilized as the criteria for detecting progression [35]. Additionally, the 1-year reduction in 25-FWT or EDSS was considered an accepted treatment response for DMD [36].
Limitations
Some of the registry data were missing (could not give us full picture about the natural history of the disease, hence many patients were excluded from the study).
Many SPMS patients when interviewed at our clinic already had cognitive impairment that could affect history taking.
This study’s retrospective design inherently limits its ability to establish temporal relationships between variables, hindering the capacity to infer causation. Consequently, the absence of a prospective approach restricts the study’s ability to definitively identify risk factors, as it primarily relies on historical data without capturing dynamic changes over time. It is essential to acknowledge that the retrospective nature of the study confines the scope of conclusions regarding causal relationships and risk factor assessments.
Recommendation
Establishing multidimensional approach including clinical, laboratory, and MRI measures, available in routine follow-up, may be helpful in identifying patients with early unfavorable prognosis and help tailoring individualized treatment strategies for patients with RRMS.
Conclusions
Clinicians can prospectively diagnose patients at the transitioning phase of MS identifying who are the patients at risk for progression, then calculating the risk of future progression, close detailed clinical assessments on short time intervals, and finally making the diagnosis of confirmed disability progression early prior to reaching an irreversible stage of neurological damage, SDMT and 25 FWT scores can predict early conversion to SPMS. Variables that are associated with high risk of progression are smoking, employment state, number of relapses and relapse recovery, disease duration, number and site of lesions, DMDs used.
Availability of data and materials
The datasets are not publicly available due to institutional rules. The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- MS:
-
Multiple sclerosis
- SPMS:
-
Secondary progressive multiple sclerosis
- RRMS:
-
Relapsing remitting MS
- EDSS:
-
Expanded Disability Status Scale
- PPMS:
-
Primary progressive MS
- DMD:
-
Disease-modifying drugs
- DM:
-
Diabetes mellitus
- DVT:
-
Deep venous thrombosis
- 25-FWT:
-
25-Feet timed walk test
- MRI:
-
Magnetic resonance imaging
- SDMT:
-
Simple digit modalities test
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- BMI:
-
Body mass index
- OCB:
-
Oligoclonal bands
- HR:
-
Hazard ratio
References
Mirmosayyeb O, Brand S, Barzegar M, Afshari-Safavi A, Nehzat N, Shaygannejad V, et al. Clinical characteristics and disability progression of early-and late-onset multiple sclerosis compared to adult-onset multiple sclerosis. J Clin Med. 2020;9(5):1326.
Blair HA. Dimethyl fumarate: a review in relapsing-remitting MS. Drugs. 2019;79(18):1965–76.
Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sørensen PS, Thompson AJ, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278–86. https://doi.org/10.1212/wnl.0000000000000560.
Inojosa H, Proschmann U, Akgün K, Ziemssen T. A focus on secondary progressive multiple sclerosis (SPMS): challenges in diagnosis and definition. J Neurol. 2021;268(4):1210–21. https://doi.org/10.1007/s00415-019-09489-5.
Cree BAC, Arnold DL, Chataway J, Chitnis T, Fox RJ, Pozo Ramajo A, et al. secondary progressive multiple sclerosis: new insights. Neurology. 2021;97(8):378–88. https://doi.org/10.1212/WNL.0000000000012323.
Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sørensen PS, Thompson AJ, et al. Defining the clinical course of multiple sclerosis. The 2013 revisions. Neurology. 2014;83(3):278–86. https://doi.org/10.1212/wnl.0000000000000560.
Ontaneda D, Fox RJ. Progressive multiple sclerosis. Curr Opin Neurol. 2015;28(3):237–43. https://doi.org/10.1097/wco.0000000000000195.
Katz Sand I, Krieger S, Farrell C, Miller AE. Diagnostic uncertainty during the transition to secondary progressive multiple sclerosis. Mult Scler. 2014;20(12):1654–7. https://doi.org/10.1177/1352458514521517.
Koch M, Uyttenboogaart M, van Harten A, De Keyser J. Factors associated with the risk of secondary progression in multiple sclerosis. Mult Scler. 2008;14(6):799–803.
Manouchehrinia A, Zhu F, Piani-Meier D, Lange M, Silva DG, Carruthers R, et al. Predicting risk of secondary progression in multiple sclerosis: a nomogram. Mult Scler. 2019;25(8):1102–12.
Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162–73.
Lorscheider J, Buzzard K, Jokubaitis V, Spelman T, Havrdova E, Horakova D, et al. Defining secondary progressive multiple sclerosis. Brain. 2016;139(Pt 9):2395–405.
Calabrese M, Filippi M, Gallo P. Cortical lesions in multiple sclerosis. Nat Rev Neurol. 2010;6(8):438–44.
Roudbari SA, Ansar MM, Yousefzad A. Smoking as a risk factor for development of secondary progressive multiple sclerosis: a study in IRAN, Guilan. J Neurol Sci. 2013;330(1–2):52–5.
Koch M, van Harten A, Uyttenboogaart M, De Keyser J. Cigarette smoking and progression in multiple sclerosis. Neurology. 2007;69(15):1515–20.
Marrie RA, Rudick R, Horwitz R, Cutter G, Tyry T, Campagnolo D, et al. Vascular comorbidity is associated with more rapid disability progression in multiple sclerosis. Neurology. 2010;74(13):1041–7.
Koch MW, Metz LM, Agrawal SM, Yong VW. Environmental factors and their regulation of immunity in multiple sclerosis. J Neurol Sci. 2013;324(1–2):10–6.
Ascherio A, Munger KL, White R, Köchert K, Simon KC, Polman CH, et al. Vitamin D as an early predictor of multiple sclerosis activity and progression. JAMA Neurol. 2014;71(3):306–14.
Oliveira SR, Simão AN, Alfieri DF, Flauzino T, Kallaur AP, Mezzaroba L, et al. Vitamin D deficiency is associated with disability and disease progression in multiple sclerosis patients independently of oxidative and nitrosative stress. J Neurol Sci. 2017;381:213–9.
Kampman MT, Steffensen LH, Mellgren SI, Jørgensen L. Effect of vitamin D3 supplementation on relapses, disease progression, and measures of function in persons with multiple sclerosis: exploratory outcomes from a double-blind randomised controlled trial. Mult Scler. 2012;18(8):1144–51.
Boltjes R, Knippenberg S, Gerlach O, Hupperts R, Damoiseaux J. Vitamin D supplementation in multiple sclerosis: an expert opinion based on the review of current evidence. Expert Rev Neurother. 2021;21(6):715–25.
Feige J, Moser T, Bieler L, Schwenker K, Hauer L, Sellner J. Vitamin D supplementation in multiple sclerosis: a critical analysis of potentials and threats. Nutrients. 2020;12(3):783.
Tedeholm H, Lycke J, Skoog B, Lisovskaja V, Hillert J, Dahle C, et al. Time to secondary progression in patients with multiple sclerosis who were treated with first generation immunomodulating drugs. Mult Scler. 2013;19(6):765–74.
Calabrese M, Poretto V, Favaretto A, Alessio S, Bernardi V, Romualdi C, et al. Cortical lesion load associates with progression of disability in multiple sclerosis. Brain. 2012;135(10):2952–61.
Kearney H, Schneider T, Yiannakas M, Altmann D, Wheeler-Kingshott C, Ciccarelli O, et al. Spinal cord grey matter abnormalities are associated with secondary progression and physical disability in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2015;86(6):608–14.
Brownlee WJ, Altmann DR, Prados F, Miszkiel KA, Eshaghi A, Gandini Wheeler-Kingshott CAM, et al. Early imaging predictors of long-term outcomes in relapse-onset multiple sclerosis. Brain. 2019;142(8):2276–87. https://doi.org/10.1093/brain/awz156.
Hamdy SM, Abdel-Naseer M, Shalaby NM, Elmazny AN, Nemr AA, Hassan A, et al. Characteristics and predictors of progression in an Egyptian multiple sclerosis cohort: a multicenter registry study. Neuropsychiatr Dis Treat. 2017;13:1895–903. https://doi.org/10.2147/NDT.S140869.
Karrenbauer VD, Bedri SK, Hillert J, Manouchehrinia A. Cerebrospinal fluid oligoclonal immunoglobulin gamma bands and long-term disability progression in multiple sclerosis: a retrospective cohort study. Sci Rep. 2021;11(1):14987.
Lourenco P, Shirani A, Saeedi J, Oger J, Schreiber WE, Tremlett H. Oligoclonal bands and cerebrospinal fluid markers in multiple sclerosis: associations with disease course and progression. Mult Scler. 2013;19(5):577–84.
Koch M, Heersema D, Mostert J, Teelken A, Keyser JD. Cerebrospinal fluid oligoclonal bands and progression of disability in multiple sclerosis. Eur J Neurol. 2007;14(7):797–800.
Buyukturkoglu K, Zeng D, Bharadwaj S, Tozlu C, Mormina E, Igwe KC, et al. Classifying multiple sclerosis patients on the basis of SDMT performance using machine learning. Mult Scler. 2021;27(1):107–16.
Goldman MD, LaRocca NG, Rudick RA, Hudson LD, Chin PS, Francis GS, et al. Multiple Sclerosis Outcome Assessments Consortium. Evaluation of multiple sclerosis disability outcome measures using pooled clinical trial data. Neurology. 2019;93(21):e1921–e1931. https://doi.org/10.1212/WNL.0000000000008519. Erratum in: Neurology. 20219;96(10):504–505.
Jacobsen C, Zivadinov R, Myhr K-M, Dalaker TO, Dalen I, Benedict RH, et al. Brain atrophy and clinical characteristics predicting SDMT performance in multiple sclerosis: a 10-year follow-up study. Mult Scler J Exp Transl Clin. 2021;7(1):2055217321992394.
Koch MW, Mostert J, Repovic P, Bowen JD, Uitdehaag B, Cutter G. Is the symbol digit modalities test a useful outcome in secondary progressive multiple sclerosis? Eu Eur J Neurol. 2021;28(6):2115–20.
Wolinsky JS, Montalban X, Hauser SL, Giovannoni G, Vermersch P, Bernasconi C, et al. Evaluation of no evidence of progression or active disease (NEPAD) in patients with primary progressive multiple sclerosis in the ORATORIO trial. Ann Neurol. 2018;84(4):527–36.
Collongues N, Kuhle J, Tsagkas C, Lamy J, Meyer N, Barro C, et al. Biomarkers of treatment response in patients with progressive multiple sclerosis treated with high-dose pharmaceutical-grade biotin (MD1003). Brain Behav. 2021;11(2): e01998.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
All authors (MS, TM, ES, MR) contributed equally to this work.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional review board (IRB), Nasser institute hospital at 20 December 2020. Written informed consent was waived by the committee because of the observational nature of the study.
Informed consent
Prior to the start of study, informed written consent was obtained from the patients, participants were provided detailed information regarding the study including the title, objective and procedures as well as assurance of the participants data confidentiality and anonymity with data never to be used for purposes other than scientific research. Participation in the present study was completely voluntary and study participants were free to withdraw at any time.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shawky, M.A., Menecie, T.I., Saif El Deen, E.M. et al. Predictors of progression of multiple sclerosis in a sample of Egyptian patients. Egypt J Neurol Psychiatry Neurosurg 60, 1 (2024). https://doi.org/10.1186/s41983-023-00779-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00779-4