
Abstract
Background
Although there is a striking impact of epilepsy on sexual functions, this issue is avoided by the patients, because they consider it as a taboo that brings much shame to the complainer and also largely ignored by physicians and neurologists who involved in epileptic patient management. Our aim was to investigate the prevalence and forms of sexual dysfunction (SD) in Egyptian men with epilepsy and relating this dysfunction to the type of epilepsy and the existing sex hormone disturbance.
Methods
We recruited seventy male epileptic patients on anti-seizure medications and seventy healthy males aged-matched control subjects. We assessed their sexual functions using IIEF-15.
Results
The prevalence of SD in epileptic patients in our study was as follows: erectile function (64.3%), sexual desire (45.7%), intercourse satisfaction (37.2%) and orgasmic function (15.7%). We found statistically significant lower IIEF scores in uncontrolled versus controlled epileptic patients, in spite that total and free testosterone were not statistically significantly different between the two groups. Although a lower IIEF score in focal versus generalized epilepsy was noticed, but only orgasmic function achieved statistical significance (P = 0.049). Our results exhibited no statistically significant difference as regard treatment therapy in relation to sexual function and hormonal plasma level.
Conclusions
A higher prevalence of sexual dysfunction was observed in the epileptic patients especially in those with uncontrolled seizures. For that reason, the issues related to sexual activity should be clarified by physicians how are involved in managing the patients suffering from epilepsy.
Similar content being viewed by others


Background
The Quality of Live (QoL) is of paramount importance for human feeling of wellness and health. Different Aspects of QoL—such as psychological health, sexual satisfaction, functional and social achievements are—definitely—affected by diverse spectrum of chronic medical derangements. Undoubtedly, these aspects are closely inter-connected, so that each of them reflects considerably on the others. One common example of these medical disorders which can harm QoL is epilepsy [1, 2].
Although there is a striking impact of epilepsy on sexual functions, this issue is largely ignored by those physicians who involved in epileptic patient management [3]. For long time, merely a discussion of sexual dysfunction (SD) and related sexual practice problems was considered as a taboo that brings much shame to the complainer. However, by the current time, one of the clear faces of the recent advanced technology such as wide availability of social media raised the awareness of SD and crushed the boundaries that circled it for long time.
In general population, SD is variable and found to affect 10–25% of males and 25–63% of females [4]. This wide variation could be attributed to presence of different definitions for sexual problems, variation in study methods, sample size, diverse cultural and socioeconomic states among different studies [3, 5,6,7].
It was noted that, many previous studies documented marked effect of epilepsy on sexual functions in males when compared with healthy non epileptic volunteers (63% and 10%, respectively) [4, 5, 8].
Obviously, there is no single etiological explanation for the occurrence of SD in epilepsy. Actually, there are many factors related to epilepsy and could harm—by a mean or other—the healthy sexual life of epileptics. Suggested etiologies for this problem may include epilepsy by itself, other comorbid neurological disorders, accompanying circulatory disturbance, psychological drawbacks and associated psychiatric disorders, inconvenient interpersonal and social associations, endocrinal derangement beside iatrogenic factors related to anti-seizure medications (ASM) [9, 10].
The pathophysiological effects of epileptic seizures may produce obvious impact on endocrine reproductive system [10], in addition to the complicated interconnection between the hypothalamic–pituitary axis (HPA) and the limbic system that can modify key traits in sex hormone discharging [11]. This is why the link between SD and epilepsy is complicated and mostly mutually related [12].
The aim of this study was to investigate the prevalence and forms of sexual dysfunction in Egyptian men with epilepsy and relating this disturbance to the type of epilepsy and the existing sex hormone disturbance.
Methods
This cohort study was carried out in the period from December 2020 to October 2021 in outpatient clinics of university hospital with approval from Research Ethical Committee (REC) for human and animal research at the faculty of medicine, university (serial: 73-2020). Written consent was obtained from all participants prior to inclusion in our study. The study enrolled 70 patients diagnosed with epilepsy and 70 age matched married men as healthy control subjects. The inclusion criteria included being: male, married, age range from 18 to 50 years, sexually active, epileptic (diagnosis of epilepsy was based on clinical evaluation, brain magnetic resonance imaging (MRI) and electroencephalography (EEG) findings), receiving anti-seizure medications (ASM) for at least 6 months before participation in our study. Excluded from our study, patients with other neurological diseases, presence of well-established endocrine disorders, such as diabetes mellitus, thyroid dysfunction, major depressive disorder or other psychiatric disorders, anatomical defects in external genitalia that can cause sexual dysfunction by itself, such as micropenis and ambiguous genitalia, history of hormone therapy, any other systemic disorders that may affect sexual function, such as hypertension, advanced liver disease, cardiovascular diseases, underlying urogenital diseases, impaired general health status and patient who was not able to fill questionnaires. In addition, excluded from our study, patients under current or recent treatment of erectile dysfunction with intra-corporeal injection or application of vasoactive drugs or drug history of any medication that can cause sexual dysfunction in the past 3 months, such as anti-androgens.
All patients diagnosed with epilepsy by two consultant neurology more than 20 year experience were subjected to thorough history taking and full clinical and neurological examination with focusing on epilepsy type, duration of illness, seizure control (controlled versus non controlled) and antiepileptic drug therapy (type and duration). Seizure types were diagnosed according to the International League Against Epilepsy (ILAE) [13].
General and local Genital examination by a consultant andrologist co-author visiting the outpatient clinic at Helwan University regularly during the study period to apply inclusion and exclusion criteria, evaluate different aspects of sexual function of epileptic patients and to help them in filling the questionnaire Assessment of sexual function by the self-administered questionnaire of the International Index of Erectile Function-15 (IIEF-15). that addresses the relevant domains of male sexual Function (Arabic Version) was done [14].
All enrolled subjects were performed Hamilton Rating scale for depression (HRDS) (Arabic version) [15]. Laboratory investigations including liver, renal and thyroid function tests, complete blood picture, HbA1c, and plasma levels of total and free testosterone, estradiol (E2) and prolactin were performed.
The International Index of Erectile Function (IIEF-15): a reliable, multidimensional, brief, standard, self-administrated questionnaire that address the relevant 5 central domains of men sexual function used in both research and clinical setting all over the world. The scale consists of fifteen items: 6 items assessing erectile function (EF), 2 items for sexual desire, 2 items for assessing orgasmic function (OF), 3 items for intercourse satisfaction (IS), while overall satisfaction (OS) included two items [14]. Erectile dysfunction further categorized into 5 categories: no erectile dysfunction (score from 22 to 25), mild erectile dysfunction (score from 17 to 21), mild to moderate erectile dysfunction (score from 12 to 16), moderate erectile dysfunction (score from 8 to 11) and finally severe erectile dysfunction (score from 5 to 7) [16].
Hormonal assessment: plasma levels of total and free testosterone, E2 and prolactin were calculated by collecting Samples of 5 ml of blood using venipuncture technique and kept in a plain tube for 10–15 min till complete clotting, sample had been centrifuged 3000RPM for 5 min then serum separated in special tube (Eppendorf) and kept frozen (− 18 °C) till the time of assay. Detection of total and free testosterone, E2 and prolactin had been done by chemiluminescence technique using Mindray 960 cli (china) machine and kit.
Statistical analysis: data were entered and analyzed using IBM-SPSS software (IBM Corp. Released 2019. IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp.). Qualitative data were expressed as N (%). Quantitative data were initially tested for normality using Shapiro–Wilk’s test with data being normally distributed if p > 0.050. The presence of significant outliers was tested by inspecting boxplots. Quantitative data were expressed as median (Q1–Q3). Chi-square was used to compare categorical data. Quantitative data between two groups were compared by Mann–Whitney U test. Spearman’s correlation was used to assess the direction and magnitude of association between two quantitative variables. For any of the used tests, results were considered as statistically significant if p value ≤ 0.050. Appropriate charts were used to graphically present the results whenever needed.
Results
This study involved 140 Egyptian participants divided into two groups:
-
Group 1: This group involved 70 male epileptic patients with median age (years), and marriage duration (years) of 35.5, and 6 years, respectively.
-
Group 2: This group involved 70 male healthy participants with median age (years), and marriage duration (years) of 38, and 10 years, respectively.
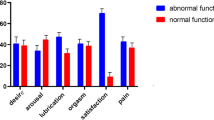
The prevalence of sexual dysfunction in our study was as follows erectile function was (64.3%), sexual desire (45.7%), intercourse satisfaction (37.2%) orgasmic function (15.7%).
Table 1 shows statistically significantly lower scores for erectile function, orgasmic function, sexual desire, and overall satisfaction, as well as total score in group 1 versus group 2, but statistically insignificant difference was noted in intercourse satisfaction score.
Table 2 shows a statistically significant higher proportion of sexual erectile dysfunction (ED) in male epileptic patients versus control with score of 16 or less (severe ED) in 47.1%, and 5.7%, respectively, while mild-to-moderate ED was observed in 17.1% and 7.1%, respectively. Multiple z tests shows a statistically significantly higher EF score ≤ 16 points, and a statistically significantly lower EF score ≥ 22 points in group 1 (epileptic) versus group 2 (control).
Table 3 shows a statistically significant negative correlation between both age and marriage duration with IIEF scores. This association was of mild strength for age with OF, and marriage duration with EF, OF, and SD, and of moderate strength for others. Subgroup analysis revealed that all 5 domains and total score had a statistically significant negative correlation with age and marriage duration except OF with age and sexual desire with marriage duration in control subjects only.
Table 4 shows a statistically significant all 6 lower IIEF scores, prolactin and estradiol younger age, short marriage and disease duration in uncontrolled versus controlled. Total and free testosterone were not statistically significantly different between the two groups.
Table 5 shows lower scores in focal versus generalized epilepsy, but only orgasmic function achieved statistical significance.
0Table 6 shows no statistically significant difference as regard treatment therapy in relation to sexual function and hormonal plasma level.
Discussion
Sexual functions including sexual desire, orgasm, erection and ejaculation are primary mediated by interaction between autonomic and somatic nervous systems that operate at the peripheral and central levels. Any disturbance of hormonal, vascular or neural response as a results of several medical illnesses including epilepsy will lead to disruption of sexual function with significant affection of QoL [17].
In our study that included seventy epileptic male married patients and seventy healthy married males as an age matched control group, we did not found any statistical significant differences between both groups as regard age and duration of marriage.
As regard prevelences of SD in our epileptic patients, the study exhibits the erectile dysfunction was notably high, while the least affected domain of sexual function was related to orgasmic achievement.
When comparing different sexual functions using IIEF-15 between both groups, we found statistically significant lower scores in epileptic patient as regard erectile function, orgasm, sexual desire, overall satisfaction and total score (P < 0.001, P < 0.001, P < 0.001, P < 0.001 and P < 0.001, respectively) but no statistical significant difference as regard intercourse satisfaction between both groups (P = 0.098).
One of the widely accepted mechanisms that can explain sexual dysfunction in those epileptic patients is that the epilepsy may have a negative effect on activation of the paralimbic and limbic regions that responsible for motor, emotional and sexual responses [18].
As regard erectile dysfunction in our study, we found similarity with Henning and his colleagues 2019 who found that the erectile function was significantly affected in epileptic patients when compared with normal population and also consistent with other several researches [8, 19,20,21].
But there was dissimilarity with Calabro and his colleagues who found that no difference was found in sexual function in epileptic versus general populations [22].This dissimilarity may be explained by different cultural backgrounds in the studied group in addition to difference in sample size and the methods of applying the questionnaire.
Our study revealed that score of orgasmic function was low (6 ranging between 3 and 8) when compared with score of control healthy non epileptic individuals (9 ranging between 8 and 9) with statistically significant difference between the two groups (P < 0.001). This was in agreement with Pavone and his colleagues 2017 who found that orgasmic dysfunction was high in epileptic patients and came next to erectile dysfunction [23].
We found in this research that the sexual desire score was markedly decreased in epileptic patients (7 ranging between 3 and 8.25) when compared with score of healthy subjects (8 ranging between 8 and 9) with statistically significant difference in between the two groups (P < 0.001) using IIEF questionnaire. This results were concordant with Rathore and his colleagues who found that decreased sexual desire was significantly high in epileptic patients when compared with general populations [24].
However, our results are non-concordant with Henning and his colleagues 2019 who found that the lack of sexual desire did not significantly differ between general populations and epileptic patients [20].
As regard overall satisfaction, we found, significant decreased score in epileptic patients [6 ranging between 3 and 8] in comparing with control subjects (8 ranging between 8 and 9) (P < 0.001) This was in agreement with Owczarek and his colleagues who found that 57.4% of epileptic patients in their study exhibit either less satisfaction in sexual life [25], When we compared total score of IIEF between epileptic versus control groups we found statistically significant low score in epileptic patients (P < 0.001).
Erectile dysfunction categorization into five categories in our study revealed statistically significant higher proportion of sexual erectile dysfunction in male epileptic patients versus control (P < 0.001).
When we studied correlation between age and marriage duration in relation to IIEF for all participants we found that there was statistically significant negative correlation between both age and duration of marriage in years with erectile function (P < 0.001 and P < 0.001, respectively), this was consistent with Aliakbari and his colleagues who found strong inverse relation between age and erectile function considering the presence of other influencing factors, such as educational level, unemployment and other chronic diseases [26], while Pasha and his colleagues 2020 did not found any significant relation between duration of marriage and erectile dysfunction in there study [27].
In our study, we found a negative statistically significant correlation between both age and duration of marriage in years with orgasmic function (P = 0.012 and P = 0.010, respectively), this was consistent with Dawson and his colleagues who found marked decrease in orgasmic function in men with epilepsy when assessing sexual function using IIEF tool [28].
In our research, we found that there was statistically significant negative correlation between both age and duration of marriage in years with the following items: sexual desire (P < 0.001 and P < 0.001, respectively), intercourse satisfaction (P < 0.001 and P < 0.001, respectively), overall satisfaction (P < 0.001 and P < 0.001, respectively) and total score using IIEF scale. This was in agreement with Dawson and his colleagues 2019 who found marked affection of intercourse satisfaction, sexual desire and overall satisfaction in their study [28].
When we compare between controlled and uncontrolled epileptic patients we found statistically significant older age in controlled patients (P = 0.002). This can be explained by non-compliance for treatment in younger age, we also found statistically significant short disease duration in uncontrolled patients (P < 0.001).
As regard sexual function when assessed by IIEF, we found statistically significant low erectile function score in uncontrolled patients (P < 0.001), this was in concordant with Rathore and his colleagues 2019 as they documented that erectile dysfunction was significantly high in uncontrolled epileptic than controlled patients [24] but non concordant with Nikoobakht and his colleagues 2007 who found the prevalence of erectile dysfunction did not differ between controlled and uncontrolled patients. However, epileptic seizure frequency prior to initiating anti-seizure medication was correlated with erectile function scores [29].
We found in our study statistically significant low scores in uncontrolled epileptic group when compared with controlled group as regard orgasmic function, sexual desire, intercourse satisfaction, overall satisfaction and total score (P < 0.001, P < 0.001, P < 0.001, P < 0.001 and P < 0.001, respectively). This was consistent with Tao and his colleagues 2018., and Rathore and his colleagues 2019 who found high prevalence of sexual dysfunction among uncontrolled epileptic versus controlled epileptic patients [21, 24].
As regard the difference of sexual hormonal levels between controlled and uncontrolled epileptic patients, we found statistically significant high estradiol and prolactin levels in controlled versus uncontrolled patients (P = 0.013 and P = 0.001, respectively). This was consistent with Ke and his colleagues 2023 who found that increased level of estradiol reduce the risk of epileptic seizures in male [30] and also with Hamed and his colleagues 2013 who found that the disturbance in hormonal function was associated with seizure intractability [31]. However, there was no consensus about the swinging of prolactin level in epileptic patients in which there was a transient elevation of serum prolactin levels after seizing that commonly used in differentiation between true and pseudo-seizures [32, 33]. In addition, we did not find any significant difference in total and free testosterone level between controlled and uncontrolled epileptic patients. This was not consistent with some other researches [31].
On comparing focal and generalized seizures in relation to sexual functions, we found low scores in focal versus generalized seizures as regard erectile function, sexual desire, intercourse satisfaction, and total score without statistically significant differences except for orgasmic function (P = 0.049). No statistically significant differences as regard age of patients, duration of marriage, total and free testosterone, estradiol and prolactin levels between both groups.
In our study, we did not find any statistically significant differences in sexual function in patients using different antiepileptic drugs, for example, sodium valoperate, carbamazepine and levetiracetam. This was not in agreement with Calabrò 2016 who found that antiepileptic medications especially liver enzyme inducers such as carbamazepine can lead to sexual dysfunctions by lowering bioactive testosterone, fastening the metabolism of sexual hormone and stimulating the hormone binding globulin production. However, the mechanism by which the levetiracetam as a relatively new antiepileptic medication causing sexual dysfunction still poorly understood [34].
Limitations of our study: number of patients was rather small and needed to increased but in our study this was unfortunately applicable due to limited self-funding. Besides, this study was done in only one locality and was better to recruit patients from multiple urban and rural localities, but obtaining multiple approval from different hospitals in Egypt for multicenter study was extremely difficult.
Conclusion
A higher prevalence of sexual dysfunction was observed in the epileptic patients especially in those with uncontrolled seizures. For that reason, the issues related to sexual activity should be clarified by physicians how are involved in managing the patients suffering from epilepsy.
Availability of data and materials
The data supporting the results of this article are included within the article.
Abbreviations
- ASM:
-
Anti-seizure medication
- E2:
-
Estradiol
- EF:
-
Erectile function
- Hb A1c:
-
Hemoglobin A1c
- HPA:
-
The hypothalamic–pituitary axis
- HRDS:
-
Hamilton Rating scale for depression
- IIEF-15:
-
International Index of Erectile Function-15
- ILAE:
-
International League Against Epilepsy
- IS:
-
Intercourse satisfaction
- OF:
-
Orgasmic function
- OS:
-
Overall satisfaction
- QOL:
-
The quality of live
- SD:
-
Sexual dysfunction
References
Karakis I, Boualam N, Moura LM, Howard DH. Quality of life and functional limitations in persons with epilepsy. Epilepsy Res. 2023;190: 107084.
Davison SL, Bell RJ, LaChina M, Holden SL, Davis SR. The relationship between self-reported sexual satisfaction and general well-being in women. J Sex Med. 2009;6(10):2690–7.
Kaufman KR, Wong S, Sivaraaman K, Anim C, Delatte D. Epilepsy and AED-induced decreased libido—the unasked psychosocial comorbidity. Epilepsy Behav. 2015;52(Pt A):236–8. https://doi.org/10.1016/j.yebeh.2015.09.015.
Shifren JL, Monz BU, Russo PA, Segreti A, Johannes CB. Sexual problems and distress in United States women: prevalence and correlates. Obstet Gynecol. 2008;112(5):970–8. https://doi.org/10.1097/AOG.0b013e3181898cdb.
Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C, Moreira E, et al. Sexual problems among women and men aged 40–80 y: prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res. 2005;17(1):39–57. https://doi.org/10.1038/sj.ijir.3901250.
Ejigu AK, Zewlde KH, Muluneh NY, Seraj ZR, GebreLibanos MW, Bezabih YH. Sexual dysfunction and associated factors among patients with epilepsy at Amanuel Mental Specialty Hospital, Addis Ababa—Ethiopia. BMC Neurol. 2019;19(1):255. https://doi.org/10.1186/s12883-019-1432-1.PMID:31656168;PMCID:PMC6816149.
Zhao S, Tang Z, Xie Q, Wang J, Luo L, Liu Y, Zhu Z, Luo J, Zhao Z. Association between epilepsy and risk of sexual dysfunction: a meta-analysis. Seizure. 2019;65:80–8. https://doi.org/10.1016/j.seizure.2019.01.004.
Henning OJ, Nakken KO, Træen B, Mowinckel P, Lossius M. Sexual problems in people with refractory epilepsy. Epilepsy Behav. 2016;61:174–9. https://doi.org/10.1016/j.yebeh.2016.05.038.
Calabrò RS, Cerasa A. Drug-induced sexual dysfunction in individuals with epilepsy: beyond antiepileptic compounds. Medicines (Basel). 2022;9(3):23. https://doi.org/10.3390/medicines9030023.
Scharfman HE, Kim M, Hintz TM, MacLusky NJ. Seizures and reproductive function: insights from female rats with epilepsy. Ann Neurol. 2008;64(6):687–97. https://doi.org/10.1002/ana.21518.
Herzog AG, Seibel MM, Schomer DL, Vaitukaitis JL, Geschwind N. Reproductive endocrine disorders in women with partial seizures of temporal lobe origin. Arch Neurol. 1986;43(4):341–6. https://doi.org/10.1001/archneur.1986.00520040029014.
Atif M, Sarwar MR, Scahill S. The relationship between epilepsy and sexual dysfunction: a review of the literature. Springerplus. 2016;5(1):2070. https://doi.org/10.1186/s40064-016-3753-5.
Proposal for revised clinical and electroencephalographic classification of epileptic seizures. From the Commission on Classification and Terminology of the International League Against Epilepsy. Epilepsia. 1981; 22 (4):489–501.
Quinta Gomes AL, Nobre P. The international index of erectile function (IIEF-15): psychometric properties of the Portuguese version. J Sex Med. 2012;9(1):180–7. https://doi.org/10.1111/j.1743-6109.2011.02467.x.
Alhadi AN, Alarabi MA, Alshomrani AT, Shuqdar RM, Alsuwaidan MT, McIntyre RS. Arabic translation, validation and cultural adaptation of the 7-item hamilton depression rating scale in two community samples. Sultan Qaboos Univ Med J. 2018;18(2):e167–72. https://doi.org/10.18295/squmj.2018.18.02.008.
Rosen RC, Cappelleri JC, Gendrano N 3rd. The International Index of Erectile Function (IIEF): a state-of-the-science review. Int J Impot Res. 2002;14(4):226–44. https://doi.org/10.1038/sj.ijir.3900857.
Calabrò RS, Cacciola A, Bruschetta D, Milardi D, Quattrini F, Sciarrone F, et al. Neuroanatomy and function of human sexual behavior: a neglected or unknown issue? Brain Behav. 2019;9(12):e01389. https://doi.org/10.1002/brb3.1389.
Rees PM, Fowler CJ, Maas CP. Sexual function in men and women with neurological disorders. Lancet. 2007;369(9560):512–25. https://doi.org/10.1016/S0140-6736(07)60238-4.
Ureka RK, Gaur V, Purohit G, Gupta M. Sexual Dysfunction in Male Patients with Idiopathic Generalized Tonic Clonic Seizures. Ann Indian Acad Neurol. 2021;24(5):726–31. https://doi.org/10.4103/aian.AIAN_1023_20.
Henning O, Johannessen Landmark C, Traeen B, Svendsen T, Farmen A, Nakken KO, et al. Sexual function in people with epilepsy: similarities and differences with the general population. Epilepsia. 2019;60(9):1984–92. https://doi.org/10.1111/epi.16311.
Tao L, Zhang X, Duan Z, Wang Y, Liu J, Hou H, et al. Sexual dysfunction and associated factors in Chinese Han women with epilepsy. Epilepsy Behav. 2018;85:150–6. https://doi.org/10.1016/j.yebeh.2018.06.003.
Calabrò RS, Grisolaghi J, Quattrini F, Bramanti P, Magaudda A. Prevalence and clinical features of sexual dysfunction in male with epilepsy: the first southern Italy hospital-based study. Int J Neurosci. 2013;123(10):732–7. https://doi.org/10.3109/00207454.2013.798783.
Pavone C, Giacalone N, Vella M, Urso L, Zummo L, Fierro B. Relation between sexual dysfunctions and epilepsy, type of epilepsy, type of antiepileptic drugs: a prospective study. Urologia. 2017;84(2):88–92. https://doi.org/10.5301/uro.5000222.
Rathore C, Henning OJ, Luef G, Radhakrishnan K. Sexual dysfunction in people with epilepsy. Epilepsy Behav. 2019;100:106495. https://doi.org/10.1016/j.yebeh.2019.106495.
Owczarek K, Rozenek H, Jedrzejczak J, Rysz A, Blaszczyk B, Wlodaczyk D. Declared satisfaction with sexual life and quality of life in patient with epilepsy. Acta Neuropychologica. 2015;13(2):157–67.
Aliakbari F, Nematollahi S, Pestehei SK, Mogharabian N, Taghizabet N, Rezaei-Tazangi F, et al. The prevalence of erectile dysfunction among adult men: the results of a national survey on male morbidities. Nephro-Urol Mon. 2023;15(1): e127442.
Pasha H, Faramarzi M, Basirat Z, Kheirkha F, Shafee H. Evaluation of sexual dysfunction and its associated risk factors in the male partners of the infertile couples using International Index of Erectile Function. Turk J Obstet Gynecol. 2020;17(1):1–8. https://doi.org/10.4274/tjod.galenos.2019.89801.
Dawson E, Stutzman SE, Olson DM, Hays RS. Performance of the International Index of Erectile Function tool in men with epilepsy. Epilepsy Behav. 2019;94:78–81. https://doi.org/10.1016/j.yebeh.2019.01.044.
Nikoobakht M, Motamedi M, Orandi A, Meysamie A, Emamzadeh A. Sexual dysfunction in epileptic men. Urol J. 2007;4(2):111–7.
Ke B, Li C, Shang H. Sex hormones and risk of epilepsy: a bidirectional Mendelian randomization study. Front Mol Neurosci. 2023;16:1153907. https://doi.org/10.3389/fnmol.2023.1153907.
Hamed SA, Ahmad HK, Youssef AH, Metwaly NA, Hassan MM, Mohamad HO. Erectile function in men with epilepsy: relationship to psychosocial, hormonal, epilepsy and antiepileptic drugs related variables. J Neurol Neurosci. 2013;2:5. https://doi.org/10.3823/337.
Shukla G, Bhatia M, Vivekanandhan S, Gupta N, Tripathi M, Srivastava A, et al. Serum prolactin levels for differentiation of nonepileptic versus true seizures: limited utility. Epilepsy Behav. 2004;5(4):517–21. https://doi.org/10.1016/j.yebeh.2004.03.004.
Javali M, Acharya P, Shah S, Mahale R, Shetty P, Rangasetty S. Role of biomarkers in differentiating new-onset seizures from psychogenic nonepileptic seizures. J Neurosci Rural Pract. 2017;8(4):581–4. https://doi.org/10.4103/jnrp.jnrp_139_17.
Calabrò RS. Sexual dysfunction in patients with epilepsy: disentangling the pathogenic mechanisms! Epilepsy Behav. 2016;64:294. https://doi.org/10.1016/j.yebeh.2016.07.040.
Acknowledgements
The authors are grateful to all patients and control subjects for their willingness to participate in this study.
Funding
Self-funding by authors.
Author information
Authors and Affiliations
Contributions
AAM, SSS, TSS and AFI carried out the work. AAM performed the protocol, did the statistical analysis, was responsible for collecting the scientific data and writing the initial draft of the manuscript. SSS and TSS shared in collecting the scientific data, shared in statistical analysis and revision of manuscript, AFI was responsible for andrological examination of all patients, share in writing the manuscript and reply to reviewer if needed. All authors read and approved the final version to be published.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We obtained permission to conduct our study from Research Ethics Committee (REC) for Human Subject and animal Research at the Faculty of Medicine, Helwan University, Cairo, Egypt: (serial: 73-2020). All participants gave written informed consent. The procedures followed were in accordance with our protocol. We recruited 140 participants (70 patients and 70 controlled volunteers) who attended at neurology outpatient clinic of Badr University Hospital, Helwan university from December 2020 to October 2021.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abou Elmaaty, A.A., El Sherifi, S.S., Elserafy, T.S. et al. Prevalence and forms of sexual dysfunctions in Egyptian men with epilepsy in Helwan. Egypt J Neurol Psychiatry Neurosurg 59, 129 (2023). https://doi.org/10.1186/s41983-023-00729-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00729-0