
Abstract
Coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome corona virus-2 (SARS-CoV-2) appeared in early 2019 and swiftly became a pandemic causing extensive morbidity and mortality. Many studies have recognized the neuropathological changes in the brain and hypothesized the possible link with cognitive dysfunction, neuropsychiatric symptoms and behavioral disturbances. Potential biological mechanisms may include direct neuronal micro-invasion, disturbances in the neuro-immuno-endocrine system and possibly alteration of neuronal excitability. SARS-CoV-2 facilitates down-regulation of the ACE2 (Angiotensin-2) receptors which could alter inflammatory response through various cellular and neurophysiological systems leading to disturbance in the hypo-thalamopituitary–adrenal (HPA) axis, escalation of the oxidative stress and disruption of the homeostasis of the neurotransmitter system, including serotonin, dopamine and GABA (gamma-aminobutyric acid), eventually resulting in the emergence of neuropsychiatric symptoms. Psychiatric symptoms that emerged are many, some of which may be unique to SARS-CoV-2 infection. These neuropsychiatric symptoms are acute or chronic with possibly distinct etiopathogenesis. This article discusses the possible biological correlates and neurobiology of the psychiatric symptoms of SARS-CoV-2 and their impact on the brain and behavior.
Similar content being viewed by others


Introduction
SARS-CoV-2 (Severe Acute Respiratory Syndrome Corona Virus-2) causes coronavirus disease 2019 (COVID-19) and related medical complications. There is growing evidence for the neurotropic and neuro-invasive properties of SARS-CoV-2 and its ability to cause central nervous system (CNS) injury [1, 2]. SARS-CoV-2 affects neuropathogenesis due to its predilection for brain tissue besides pulmonary tissues. For example, SARS-CoV-2 may cause impairment in the brainstem structure, such as locus coeruleus in the pons, a major source of noradrenaline [3]. The neuro-cellular injuries associated with COVID-19 are mostly immune-mediated in addition to associated hypoxic–ischemic damage, which may play a role in the emergence of COVID-19 associated psychiatric conditions [4]. The pathogenesis of COVID-19 might vary or overlap between acute and chronic neuropsychiatric symptoms. The most common neuropsychiatric symptoms associated with COVID-19 infection are delirium, insomnia, fatigue, anxiety, post-traumatic disorder, psychosis, cognitive impairment, and mood disorders [5]. It has been suggested that many factors could be contributing to the pathophysiology of these symptoms including direct and indirect effects of the viral infection on the brain cells, cerebrovascular events due to hypercoagulable states, the impact of hypoxia and resultant anoxic brain injury, excessive inflammation secondary to altered immunological response, medical interventions, in addition to severe psychological and social stress associated with SARS-CoV-2 pandemic [6]. The etiology of psychiatric symptoms in COVID-19 survivors is likely not entirely attributable to neuropathological processes, as psychosocial factors also play a vital role. It is however beyond the scope of this review to discuss the etiological role of psychosocial factors. So, this narrative review highlights the available evidence for the possible biological mechanisms that may contribute to the development of neuropsychiatric symptoms.
Classification and etiology of neuropsychiatric symptoms of COVID-19
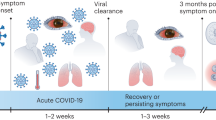
Acute and chronic neuropsychiatric symptoms in COVID-19 infection potentially differ or even overlap with the etiology of neurobiological signs and symptoms. Multiple etiologies contribute to the neuropsychiatric symptoms in acute SAR-CoV-2 infection, the most important being viral invasions of brain tissue and cytokine-induced immune disturbances. Chronic symptoms related to biological consequences of initial infection include neuronal/glial death, immune dysregulation, and virus reactivation [5]. In addition, psychosocial stressors inherent to the COVID-19 pandemic can further add to the pathology of neuropsychiatric symptoms. Unfortunately, due to methodological differences in studies assessing neuropsychiatric manifestations of COVID-19, there is also wide variation in the prevalence of acute and chronic neuropsychiatric symptoms reported. The chronic neuropsychiatric symptoms could be part of “Post COVID syndrome” or “Long COVID symptoms”. Still, it remains a dilemma in the classification of chronicity. In most classifications, including CDC and NICE guidelines, the chronicity of symptoms is usually new and/or persistent after 4–12 weeks [7].
Acute neuropsychiatric symptoms
Delirium (42%) is the most common acute neuropsychiatric syndrome [8]. In older people, delirium might be the only presenting symptom and is often seen without other typical signs or symptoms [9]. Other symptoms during acute infection include insomnia, cognitive impairment, and mood disorders [5]. Psychosis seems to be limited to the acute stage of illness as well, and new-onset psychosis has been reported in several studies [5]. A large study reviewing electronic medical record data found that of 40,469 COVID-19-positive individuals, 22.5% had neuropsychiatric manifestations. The most common psychiatric manifestations included anxiety and other related disorders (4.6%), mood disorders (3.8%), and sleep disorders (3.4%), while 0.2% of patients had suicidal ideation [10]. Also, in a large metanalysis, delirium, agitation were 65% and 69%, respectively, in intensive care unit patients and psychotic spectrum disorders range from 0.9 to 4% [6, 11]. In fact, SARS-CoV-2 has demonstrated an association with delirium in a significant proportion of patients in the acute stage of the disease [11]. Emerging data also indicate rising cases of catatonia, especially the akinetic variant in COVID-19 patients [12].
Chronic neuropsychiatric symptoms
An estimated probability of having been newly diagnosed with a psychiatric illness at 3 months after COVID-19 diagnosis was 5.8% [13]. A metanalysis of 51 studies (n = 18 917 patients) reports that most prevalent neuropsychiatric symptom was sleep disturbance (27.4%), fatigue (24.4%), objective cognitive impairment (20.2%), anxiety (19.1%) and 15.7% experience post-traumatic stress [14]. More specifically, within or after 6 months from the onset of acute COVID-19, 26% of patients may experience anxiety, 40% may experience depression and post-traumatic stress disorder (PTSD) has been shown to be found in up to 43% of all recovered patients [15]. In a one-month follow-up study 402 (psychiatric assessment was performed 31.29 ± 15.7 days after discharge, or 28.56 ± 11.73 days after emergency department visit) COVID-19 positive patients in Milan, self-rated psychopathology assessment showed evidence of PTSD (28%), depression (31%), anxiety (42%), obsessive compulsive symptoms (20%), and insomnia (40%) [16]. Importantly, the baseline systemic immune-inflammation index (SII), which reflects the immune response and systemic inflammation, is positively associated with scores of depressions and anxiety at follow-up [16]. In another study, short-term memory, attention, and concentration were particularly affected by COVID-19. Screening results did not correlate with hospitalization, treatment, viremia, or acute inflammation [17]. In another study assessing medium-term effects followed patients at 2–3 months from disease-onset, 55% reported fatigue. Patients exhibited changes in the thalamus, posterior thalamic radiations, and sagittal stratum on brain MRI and demonstrated impaired cognitive performance, specifically in the executive and visuospatial domains. In comparison to the controls, these patients reported a greater number of symptoms associated with depression and suffered notable limitations across all aspects of their quality of life [18].
Cellular entry, mode of spread and dissemination to CNS
There are four important proteins identified in the SARS-CoV-2 virus, 1. nucleoprotein (N); 2. spike glycoprotein (S) at the receptor-binding site: serves as the entry point for the virus; 3. small envelope glycoprotein (E) and 4. membrane glycoprotein (M). The spike proteins have two subunits, S1 (responsible for binding to receptors on the host) and S2 (responsible for fusion with the host cell membrane for cellular entry) [19]. SARS CoV-2 enters the host cells by binding to the S-proteins and subsequently on the host cellular ACE2 (angiotensin converting enzyme-2) receptors; this leads to membrane fusion and endocytosis [19]. The S1 and S2 subunits are cleaved by transmembrane serine protease 2 (TMPRSS2) or the lysosomal/endosomal cathepsin, a cysteine protease. The above process occurs at specific furin cleavage sites, allowing for the dissociation of the S1 subunit and exposure of the fusion peptide [19]. Conformational changes within the activated S2 subunit propel the hydrophobic fusion peptide toward the host cell membrane, resulting in disruption of the host cell lipid-bilayer and fusion of the viral and host cell membranes, allowing for the release of the viral RNA genome into the host cell [19]. After infecting the epithelial cells in the respiratory tract, the SARS-CoV-2 virus enters the bloodstream and spreads to other organs, including the brain [20]. The spike protein of SARS-CoV-2 is purported to interact with ACE2 expressed in the capillary endothelium resulting in damage to the blood–brain barrier (BBB), which then helps it enter into the CNS [21] (Fig. 1). Interestingly, the virus can also spread to the CNS through neuronal dissemination by active retrograde axonal transport from peripheral nerves such as the olfactory nerve [20]. Meinhardt et al. have identified the presence of intact SARS-CoV-2 particles and RNAs in the olfactory mucosa and in the neuroanatomical areas that receive olfactory tract projections. The above research findings provide early evidence for the use of axonal transport by the virus to find the trans-mucosal entry to the CNS via the regional nervous structures in the neural–mucosal interface [22, 23]. Other factors, such as systemic inflammation associated with COVID-19 infection, disrupt/weaken the BBB, which helps with easy entry into CNS cells. The SARS-CoV-2 virus in brain tissues is equivocal in patients presenting with neurological/neuropsychiatric symptoms. In a large study of 43 samples of postpartum brains of COVID-19 patients, neuropathology showed that only 53% of the brain tissue sample was positive for SARS-CoV-2 [24]. Another study, which analyzed cerebrospinal fluid of 7 patients with COVID-19 encephalopathy, found no traces of SARS-CoV-2 in the CSF in any patient but instead noted an increased CSF/serum quotient of albumin in 6/7 patients, suggestive of blood–brain barrier disruption. The authors suggest that COVID-19 encephalopathy may be due to indirect (or inflammatory) effects of the virus resulting in disturbed brain homeostasis and vascular dysfunction consistent with SARS‐CoV‐2‐induced endothelialitis [25].

Mechanisms of SARS-CoV-2 CNS dissemination. SARS-CoV-2 particles are first inhaled into the nasal cavity and begins CNS spread through active retrograde axonal transport along the sensory and olfactory nerves. The virus then enters systemic circulatory system and travel to the brain where the BBB prevents entry. Here the virus employs a combination of the three mechanisms to gain entry. Transcellular migration allows for the invasion of endothelial cells through interactions with the ACE2 receptors (A). The virus can also infect the tight junction for entry via paracellular transport (B). Lastly, the virus may also enter via a “Trojan horse” where viral particle becomes engulfed by a host phagocytic cell (C) [26]
Cytokine network dysregulation and inflammatory systemic manifestation
In SARS-CoV-2 infection, inflammatory cytokines are overproduced by various tissues and immune cells due to the loss of negative feedback to the immune system [27]. The feedback failure leads to a hyper-reactive immune response and elevated levels of inflammatory cytokines, referred to as a "cytokine storm", a major hallmark of severe COVID-19 infections [28]. The disrupted inflammatory system causes an increased influx of neutrophils, macrophages, and T cells, causing damaging effects on the surrounding tissues at the site of infection. Current evidence supports the cytokine storm as the main pathological process causing lung injury, multiple organ failure, and ARDS [29]. Cytokines are produced when pattern recognition receptors (PRRs) recognize different surface molecules unique to each virus, known as pathogen-associated molecular patterns (PAMPs). This binding between PRRs and PAMPs initiates a series of events through downstream signaling pathways that activate transcription factors responsible for upregulating many immune molecules and pro-inflammatory cytokines. Different cells, such as tissue macrophages, mast cells, endothelial and epithelial cells, are major contributors to the production of pro-inflammatory cytokines such as IL-1, IL-6, and TNF-a [28]. Patients with SARS-CoV-2 exhibit significantly higher levels of IL-10 (anti-inflammatory cytokine) [30], potentially moderating the severe inflammatory response in COVID-19 patients. The contradictory argument is that the persistent elevation of IL-10 in severe viral infections may be harmful, as IL-10 has been shown to induce anergy of both CD4 + and CD8 + T cells, resulting in impaired humoral immunity (that is, inability to kill virus-infected cells) [30]. Clinical analysis and comparisons between COVID-19 patients admitted to the ICU versus those placed in the general ward have demonstrated that serum levels of IL-2R, IL-4, IL-6, IL-8, IL-10, ESR, CRP, Serum ferritin, PCT, IP-10, MCP-1, and TGF-B are correlated with the severity of the disease (see Table 1) [30,31,32,33]. It is noteworthy that IL-6 has always been an important central factor in "cytokine storm" and induces the differentiation of CD8 + T cells into cytotoxic T cells, which eliminate viruses by lysing the infected cells [27]. The utilization of cytotoxic T cells may cause a decrease in lymphocytes in most patients with COVID-19. Another recently conducted study collected plasma from 24 individuals follow-up at 1 and 3 months after the initial infection identified increased plasma cytokine IL-4 levels in all patients. The study also collected neuronal-enriched extracellular vesicles and demonstrated elevated levels of inflammatory and neurodegenerative proteins. In addition, in those volunteers who self-reported neurological problems, a positive correlation was observed between IL-6 and the severity of the different neurological sequelae. As a result, it was suggested that COVID-19 might cause ongoing peripheral and neuro-inflammation that may contribute to the onset of many neurological sequelae, which are discussed in detail in the next sections [34]. The typical serum profile of cytokines derangements in SARS-CoV-2 Infection are inappropriately elevated levels of TNF-α, IL-6, IL-1β, IL-2R, IL-8, IL-17, GM-CSF, inducible protein (IP)-10, d-dimer, CRP, and ferritin, which culminate as a cytokine storm [29, 35,36,37,38,39,40]. Ortelli et al. conducted a study on COVID-19 recovered patients and noted hyperinflammatory reaction to the virus as confirmed by elevated serum levels of C-reactive protein (CRP) and interleukin-6 (IL-6) during the acute phase of the infection. In addition, they found that compared to the healthy controls, these patients had significantly higher scores on the fatigue severity scale (FSS), poorer performance in the Montreal Cognitive Assessment (MoCA) battery, decreased motor speed, and increased reaction time to the computerized cognitive tasks (such as Vigilance Task, Stroop Interference Task, and Navon Task, a test for visual neglect). These findings elucidate the presence of long-term neuropsychiatric effects caused by COVID-19 [41] possibly mediated by the severe inflammatory response.
Along with this plethora of pro-inflammatory cytokines, patients with SARS-CoV-2 infection also express elevated expression of multiple chemokines and their receptors; most notable are the upregulation of neutrophil (CXCL17, CXCL8, CXCL1, and CXCL2) and monocyte (CCL2, CCL3, CCL7) chemo-attractants [35, 37, 44], which may lead to shock and tissue damage in the heart, liver, kidney, and progress to multiple organ failure [35]. The multi-systemic manifestations of COVID-19 are illustrated in Fig. 2.

Part of Fig. 2 is adapted from Burkert et al. [45]
SARS-Cov-2 related organic brain damage
As discussed above, multiple pathological processes can weaken the integrity of the blood–brain barrier and trigger an immune response with over-production of IL-6 (pro-inflammatory) and, in severe cases, cytokine storm (particularly IL-6). The subsequent increase in pro-inflammatory cytokines in the brain and a rise in IL‐6 may be a useful marker for severe disease onset [46]. IL-6 can induce a hypercoagulable state [47] that paves the way for acute necrotizing encephalopathy (ANE) [46, 48]. Such CNS-related pathological changes may be the cause of symptoms, including loss of smell (37.9%), loss of taste (41.37%), nausea/vomiting (31%), are of central origin and have been reported in more than one-third of COVID-19-positive patients [49, 50]. The evidences from studies on other SARS groups viruses, potentially SARS-CoV-2 infection of the CNS affects the brainstem (example, locus coeruleus) and the medullary structures involved in respiration (example, solitary tract nucleus, nucleus ambiguus), and has been speculated to partially mediate the high incidence of respiratory failure currently seen in COVID-19 [51]. Interestingly, dopaminergic neurons are particularly susceptible to SARS-CoV-2 infection [52,53,54], which may account for neuropsychiatric symptoms like brain fog, mild cognitive impairments (MCI), and lethargy that develop in the aftermath of COVID-19 infection. In addition, neurons and glial cells also express ACE2, which is the key receptor that SARS-CoV-2 exploits for intracellular invasion. Previous experimental studies of intranasally inoculated other strains of SARS-CoV Infection in ACE2 transgenic mice demonstrated neuronal death and upregulation of pro-inflammatory cytokine secretion (example, TNF-α, IL-1-β, IL-6) by neurons and astrocytes [55]. Even in the absence of SARS-CoV-2 infiltration into the CNS, peripheral cytokines involved in the host antiviral response may elicit neuropsychiatric symptoms by precipitating neuroinflammatory responses and/or compromised blood–brain interface (BBI) integrity, leading to peripheral immune cell transmigration into the CNS and disruption of neurotransmission [56]. Another important aspect of pathology is the COVID-19 downregulation of ACE 2 leads to excessive production of angiotensin II which can cause severe endothelial damage and dysfunction as well as oxidative stress and enhances thrombosis that may be one of the possible explanations of stroke occurrence which can increase the risk of psychiatric disorder such a depression and anxiety [57].
Role of SARS-CoV-2 on dopamine, serotonin, norepinephrine, and GABAergic pathway
It has been postulated that COVID-19 infections alter dopamine and serotonin synthetic pathways and might be involved in the development of neuropsychiatric symptoms [52]. DOPA decarboxylase (DDC) is a major enzyme in both the dopamine and serotonin synthesis pathways. It converts L‐3,4‐dihydroxyphenylalanine (L‐DOPA) into dopamine and L‐5‐hydroxytryptophan (L-5-HT) into serotonin (5-HT). In fact, ACE2 and DDC co-express, suggesting that the defective expression of ACE2 induced by SARS-CoV-2 might impact DDC function and consequently alter levels of monoamine neurotransmitters such as DA and 5-HT [58], potentially playing an important role in etiology of neuropsychiatric disorders in SARS-CoV-2 infected patients. It is important to recognize that SARS-CoV-2 has demonstrated an impact on microglia and dopaminergic neurons in the CNS [52, 53, 59]. A prior in vitro study has shown midbrain dopamine (DA) neurons derived from human pluripotent stem cells (hPSCs) are selectively permissive to SARS-CoV-2 infection [60]. Parallelly, ACE2 receptors are highly expressed in dopamine neurons. SARS-CoV-2-related brain penetration and downregulation of ACE2, may cause additional harm and further alter dopamine levels and serotonin functioning [61]. This is evident in animal models with hypo-expression of ACE2, where decreased serotonin synthesis is observed [62] leading to an increased risk of depression and anxiety. Indeed, the downregulation of the ACE-2 receptor in COVID-19 also plays a crucial role in the pathological process in the body. It causes serious diseases [63] and also induces vulnerability to stressful conditions by influencing the neurotransmitter pathways as mentioned above [64]. Studies have shown that mice with downregulated ACE-2 expression demonstrate increased sympathetic activity [65] and decreased tryptophan uptake [66], which can lead to reduced brain 5-HT levels [62] and increased vulnerability to stress [67]. ACE-2 also acts as a neuroprotective factor and its downregulation by SARS-COV-2 has been speculated to be involved in neurodegeneration [68]. Moreover, SARS-CoV-2 induced hypercoagulable state, vasculitis, and micro-thrombosis in brain vessels locally exacerbate hypoxemia and hypoperfusion. These in turn increase oxidative stress and could lead to an elevated risk of cognitive impairment [69]. In addition, dopaminergic receptors modulate the innate immune response to a viral infection and some viruses even utilize the dopaminergic signal transduction pathway to increase neuronal susceptibility to infection [53, 70]. Since dopamine may downregulate the immune response during infection, increasing the life cycle of the virus, therapies targeting dopamine receptors may mitigate COVID-19 infection [53].
In SARS-CoV-2 infection, a high proportion of patients (up to 53.1%) experience mental and physical fatigue [41] frequently associated with executive dysfunction mainly involving attention deficits and impaired cognitive control [41]. In this context, it is noteworthy that the brain expresses ACE2 receptors on glial cells and neurons most prominently in the brainstem, paraventricular nucleus (PVN), nucleus tractus solitarius (NTS), and the rostral ventrolateral medulla [71]. Consequently, ACE2 downregulation in COVID-19 infection may contribute to impairments in cognitive functions, which is possibly mediated by the associated enhanced oxidative stress and a decrease in the concentrations of the BDNF [72]. Being that depigmentation also occurs in the substantia nigra, it is reasonable to speculate that COVID-19 infection might affect dopamine (DA) levels in the CNS [73]. Based on the above evidence, it is logical to hypothesize that the predilection of SARS-CoV-2 for these key brain structures implicated in dopaminergic and noradrenergic homeostasis may result in pathologic alterations which may explain reported symptoms such as “brain fog”, cognitive impairment, deficits of the executive functions (example, working memory, attention, concentration, and language tasks such as word-finding difficulties), confusion, sleep disturbances, mood instability, and lethargy. It is intriguing because these neuropsychiatric sequelae are seen in patients who demonstrated a mild form of COVID-19 and many were asymptomatic [74]. Furthermore, a study conducted by Versace et al. suggested a GABAergic mechanism by which COVID-19 might affect the CNS. They utilized trans-cranial magnetic stimulation (TMS) to investigate the integrity of intracortical GABAergic inhibitory circuits in the motor cortex in patients who have recovered from COVID-19 but had persistent fatigue and executive dysfunctions. They concluded that compared to healthy subjects, post-COVID-19 patients exhibited reduced inhibition of the motor cortex (M1) upon TMS application as evidenced by significant reductions of their short-interval intracortical inhibition (SICI) and long-interval intracortical inhibition (LICI) [75]. Of note, both SICI and LICI are paired-pulse mechanisms for modulating cortical excitability; they play an important role in the modulation of neural function during skill acquisition and prevention of neuronal fatigue during repeated stimulation [76]. SICI and LICI are conventionally measured as the relative reductions in the amplitudes of the motor evoked potentials (MEPs) in the hand muscle by the subthreshold conditioning stimuli. The GABAA receptors mediate SICI and the GABAB receptors mediate LICI. These impaired GABAergic mechanisms seen in post-COVID-19 patients may be attributed to the symptoms such as fatigue and cognitive dysfunctions. Ortelli and colleagues. (2021) conducted another study that reaffirmed the presence of dysregulated cortical GABAergic circuits, as evidenced by a decreased duration of the cortical silent period (CSP, another measure of intracortical inhibition that is mediated by the cortical GABAergic neurons) in post-COVID-19 patients compared to controls, thus alluding to impairments of the corticomotor GABAergic neurons [41]. A long-term follow-up study reported a greater reduction in grey matter thickness and tissue contrast in the orbitofrontal cortex and parahippocampal gyrus and a greater reduction in global brain size in the SARS-CoV-2 cases. The participants who were infected with SARS-CoV-2 also showed on average a greater cognitive decline [77]. Thus, many of the long-term symptoms of COVID-19 (‘long-COVID syndrome’), namely fatigue, cognition, apathy, and executive function, may be due to cortical impairments of the GABAergic neurotransmission.
SARS-CoV-2 and inflammatory hypothesis for depressive disorders
In SARS-CoV-2 infected patients, pro-inflammatory cytokines such as TNF-alpha and IL-6 in the plasma are significantly elevated. Of note, as proposed by the inflammatory hypothesis of depression, many of these pro-inflammatory cytokines are also implicated in major depressive disorder (MDD), especially treatment-resistant depression [78]. In a study, Taquet et al., reported that even after six months of a diagnosis of COVID-19, patients were still at high risk for developing psychiatric symptoms and neurological diagnoses [79]. Such risk of developing psychiatric disorders was even higher for those who had a severe and critical illness, required medical hospitalization, were admitted to the intensive care units, and had developed encephalopathy. These findings were consistent with a 3-month outcome, in the same retrospective cohort of COVID-19 positive patients [13]. COVID-19 infection undoubtedly acts as an etiological source of psychiatric symptoms. Furthermore, when compared to other acute health events, COVID-19 was found to have higher hazard ratios, indicating that it had a greater impact on mental health [11]. Although the etiology of these psychiatric outcomes is most likely to be multifactorial, a direct link to the viral infection may exist given the neurobiological mechanisms elaborated upon in the previous sections. In a prospective study by Mazza et al., the authors examined the mental state of COVID-19 survivors at one month and three months after their discharge from the hospital. The 3-month cohort demonstrated disorders in at least one psychopathological sphere in 35.8% of the respondents and a correlation was observed between COVID-19-associated inflammation and depression, in addition to other neurocognitive disorders [80].
Another immune molecule of interest is the C-reactive protein (CRP), a protein produced during an acute-phase response that is activated by infections/injuries. In the liver, hepatocytes recognize and bind to IL-6, leading to the secretion of acute-phase proteins (APP), particularly CRP. CRP levels act as an indicator of peripheral inflammation and correlate positively with the PHQ-9 total score of patients who presented symptoms of depression. This suggests a potential inflammatory pathway underlying these symptoms [81]. Although elevated levels of CRP are not normally described in viral respiratory infections, a significant increase of this protein has been reported in COVID-19 patients by several studies and suggests that CRP could potentially be used as an early prognostic biomarker for disease severity [82]. Similarly, MDD has been shown to have both cross-sectional and longitudinal associations with inflammatory markers including, CRP and IL-6 [83]. While studies have monitored the levels of these inflammatory biomarkers in the early and late phase of COVID-19 infection, no studies have evaluated these biomarkers in post-COVID, and more importantly, the relation of these biomarkers to severity of related psychiatric sequelae.
As discussed in earlier sections, COVID-19 can induce microglial activation as well as increase macrophage recruitment within the CNS; similar changes are also seen in the brains of depressed patients with completed suicide [84]. In addition, the activated microglia secrete inflammatory mediators, including glutamate, quinolinic acid, ILs, complement proteins, and TNF-α. Increased quinolinic acid results in higher glutamate and upregulation of NMDA receptors, possibly inducing altered learning, distorted memory, impaired neuroplasticity, hallucinatory experiences, and nightmares [85]. Historically, it has been found that central administration of IL-1 β and TNF-α to rats and mice will induce a full spectrum of behavioral changes and cause a depression-like “sickness behavior”. Those mice/rats that were injected showed little interest in their physical and social environments while demonstrating decreased motor activity, and altered cognition [56]. More recently, it was discovered that the increase in pro-inflammatory cytokines could reduce the number of monoamines available in the synapse. This is in keeping with the monoamine hypothesis of depression that suggests that the underlying pathophysiologic mechanism of MDD is due to reduced levels of serotonin, norepinephrine, and /or dopamine in the central nervous system [86]. More specifically, elevated levels of IL-1β and TNF-α in the brain can stimulate the p38 mitogen-activated protein kinase (MAPK) and increase the activity of the serotonin transporter (SERT). Increased activity of this transporter effectively reduces the amount of serotonin in the synapse and leads to depression-like behavior in animal models [87]. The increase in expression and function of the transporter is dependent on the expression of IL-1R as immobility was not observed in IL-1R knockout mice who received the same cytokine-inducer lipopolysaccharide (LPS) dosage [87]. Findings from similar studies are consistent with these results as injection of IL-1R antagonists blocked the effects of LPS [88]. Although these changes in SERT due to pro-inflammatory cytokines alone could not amount to the full spectrum of depression traits, it provides an interesting avenue for future research and a potential therapeutic target.
Impact of COVID-19 associated psychosocial stressors on neurobiology
Social factors also play an important role in the development of depression and other mood disorders. Due to the rapid spread of the virus, many safety measures were implemented in an attempt to decrease the rate of spread. These lockdowns and curfews that were implemented had an impact on both infected and uninfected individuals. The fear of infection with a potentially fatal new virus while being in lockdown may lead to feelings of anger, loneliness, and boredom. Social distancing measures have also been found to lead to frustration, aggression, mood disorders, insomnia, and psychosis. In addition, the presentation of mortality counts each day also has traumatizing effects on one’s mental health [89, 90].
The important component in the perpetuation of the anxiety orchestra in the brain is the amygdala-mediated negative valence systems, which are particularly present in the limbic system, and are primarily responsible for responses to aversive situations or context, such as fear, anxiety, and loss [91]. The stress and anxiety during the COVID-19 pandemic resulted from imposed social isolation, resultant fear, loss, loneliness, and a negative impact on daily living [92]. The prolonged course of the COVID-19 illness may lead to chronic stress in turn causing strain on the limbic system [91]. The limbic region is quite sensitive to inflammatory processes (the various mechanisms of which are described below), and subsequently alters the neural circuits and regions associated with symptoms of generalized anxiety [93]. Also, acute fear/phasic anxiety is mediated by the amygdala, which releases corticotropin-releasing hormone (CRH), a stress hormone that acts on receptors on the bed nucleus of the stria terminalis (BNST), also called ‘extended amygdala.’ The BNST is an important structure of the limbic system sensitive to inflammatory process and it is implicated in chronic anxiety. The BNST also plays a pivotal role in the circuit from the hippocampus to the paraventricular nucleus of the hypothalamus. The paraventricular nucleus also releases CRH leading to downstream glucocorticoid release while also acting as a positive-feedback loop on the BNST, thus perpetuating the stress response leading to long-lasting anxiety. This circuit is known to play a crucial role in the stimulation of the hypothalamic–pituitary–adrenal (HPA) axis [92, 94]. From the pieces of evidence presented earlier, ACE2 receptors are expressed on glial cells and neurons within the brain, especially in the paraventricular nucleus of the hypothalamus [71]. In animal models, upregulation of ACE2 suppresses CRH synthesis, which alters the central processing of psychogenic stress, thereby blunting HPA axis activation and attenuating anxiety-like behavior. However, in COVID-19 the downregulation of the ACE2 receptor alters the corticosterone and HPA axis activation worsening anxiety-like behavior [95]. Moreover, the inflammatory cytokines from stress can specifically activate the anterior cingulate cortex (ACC) producing anxiety symptoms [93] while associated hypoactivity in the vmPFC results in impaired top-down regulation and hyperactivity of the amygdala; another mechanism of causing anxiety symptoms [93, 96]. In addition, insulin resistance disrupts the dopamine system which causes a cognitive decline, decrease in synaptic plasticity, decrease in neuronal survival, increase in cerebral degeneration, disruption of the HPA axis, and impairment of physiological mechanisms of reward, learning, and mood [97, 98]. From published evidence, one can hypothesize that stress associated with COVID infection can trigger a cascade of stress-triggered events resulting in stress-induced hypoglycemia-mediated insulin resistance, neuro-inflammation, and oxidative stress [97, 98].
Medical treatments in COVID-19 infection and neuropsychiatric symptoms
Although there are currently no specific medications with proven efficacy in treating the SARS-CoV-2 infection, some medications such as remdesivir, steroids, and other medications seem to have potential in SARS-CoV2, which has led to their off-label use. Corticosteroids are used in severe and critical SARS-CoV2 infections to control the hyperinflammatory responses. The intensity of the neuropsychiatric manifestations as side effects of corticosteroids is dependent on the dose and duration of the treatment. For example, steroids can cause mania, psychosis, delirium, depression, and cognitive impairment, especially in the elderly population [99]. However, authors recognize that the duration of corticosteroid treatment in COVID-19 infection is short and it is less likely an important cause of neuropsychiatric symptoms. Tocilizumab, a humanized monoclonal antibody that causes IL-6 blockade, seems to have preventive effects on the cytokine storm. Inhibition of IL-6 has been shown to have beneficial effects in the treatment of rheumatoid arthritis [100] as well as for the cognitive symptoms in schizophrenia [101]. Remdesivir, an intravenously administered nucleotide prodrug of an adenosine analog that binds to the viral RNA-dependent RNA polymerase and inhibits viral replication through premature termination of RNA transcription, is proposed to reduce the viral load and thus the downstream effects of the virus; and as of yet, no neuropsychiatric side effects have been reported [102]. Immune checkpoint inhibition, such as PD-1 (such as nivolumab, pembrolizumab, cemiplimab) and CTLA-4 (such as Ipilimumab, tremelimumab) monoclonal antibodies, commonly used in the treatment of various malignancies, is another area being researched due to their potential to interrupt T cell exhaustion and depletion, thus improving lymphopenia and augmenting the humoral immune response to COVID-19 infection [103]. Though it must be noted there may also be an increased risk of cytokine release syndrome [103] as well as CNS side effects including fatigue, cognitive dysfunction, and memory loss [104]. The other antiviral medications molnupiravir and paxlovid (nirmatrelvir and ritonavir), have no reported psychiatric side effects. Other recent strains of the evolving SARS-CoV-2 viruses have variable neuropsychiatric disease outcomes but seem to have less severe post-COVID neuropsychiatric symptoms. It might logical to hypothesize such milder course could be due to the availability of the vaccine and/or new treatments ameliorating SARS-CoV-2 infection, though this needs to be evaluated further from the objective studies.
Conclusion
SARS-CoV-2 infection most important biological factor might be the virus’s affinity and ability to downregulate the ACE-2 receptor to induce inflammation and cause direct damage to the various cellular systems, eventually causing the derangement of multiple neurophysiological systems. The impaired allostatic mechanism subsequently affects the early return of homeostasis within the neurotransmitter system, further increasing the risk of mental illness. Moreover, ongoing research evidence supports that SARS-CoV-2 infection compromises the HPA axis, induces oxidative stress, and skews the immune system by stimulating several excessive pro-inflammatory factors. Such diverse pathological processes of the COVID-19 infection may also indirectly alter the serotonin, dopamine, and GABAergic systems and lead to the manifestation of various psychiatric disorders. This interplay of various bio-psycho-social factors is critical in disrupting the neurophysiological system homeostasis, causing distinct neuropsychiatric symptoms that may be unique to the SARS-CoV-2 infections. Though SARS-CoV-2 is a novel disease, new strains of the virus are forming rapidly even before the emergence of research evidence. The above summary of evidence linking SARS-CoV-2 to psychiatric illness might be the tip of the iceberg representing the underlying viral neuropathology caused by SARS-CoV-2 infections.
Availability of data and materials
Not applicable.
Abbreviations
- SARS- CoV-2:
-
Severe acute respiratory syndrome corona virus-2
- COVID-19:
-
Coronavirus Disease 2019
- CNS:
-
Central nervous system
- CDC:
-
Center for disease control
- NICE:
-
National Institute Clinical Excellence
- PTSD:
-
Post-traumatic stress disorder
- MRI:
-
Magnetic resonance imaging
- ACE2:
-
Angiotensin converting enzyme-2
- TMPRSS2:
-
Transmembrane serine protease 2
- ARDS:
-
Acute distress respiratory syndrome (29).
- PRR:
-
Pattern recognition receptors
- PAMPs:
-
Pathogen-associated molecular patterns
- IL:
-
Interleukin
- ESR:
-
Erythrocyte sedimentation rate
- CRP:
-
C-reactive protein
- TNF-a:
-
Tumor necrosis factor-alpha
- PCT:
-
Procalcitonin
- IP10:
-
Interferon-inducible protein-10,
- MCP1:
-
Monocyte chemoattractant protein-1
- TGF-B:
-
Transforming growth factor-beta
- GM-CSF:
-
Granulocyte macrophage-colony stimulating factor
- CCL:
-
Chemokine ligand
- CXCL:
-
Motif chemokine ligand
- ANE:
-
Acute necrotizing encephalopathy
- MCI:
-
Mild cognitive impairments
- BBi:
-
Blood–brain-interface
- hPSCs:
-
Human pluripotent stem cells
- DDC:
-
Dopamine decarboxylase
- l-5-HT:
-
l‐5‐hydroxytryptophan
- l‐DOPA:
-
l‐3,4‐dihydroxyphenylalanine
- 5-HT:
-
5‐Hydroxytryptophan
- NE:
-
Norepinephrine
- FSS:
-
Fatigue severity scale
- MoCA:
-
Montreal cognitive assessment
- TMS:
-
Trans-cranial magnetic stimulation
- GABA:
-
Gamma amino butyric acid
- SICI:
-
Short-interval intracortical inhibition
- LICI:
-
Long-interval intracortical inhibition
- MEP:
-
Motor evoked potentials
- MDD:
-
Major depressive disorder
- PHQ-9:
-
Physical Health Questionnaire-9
- APP:
-
Acute-phase proteins
- MAPK:
-
Mitogen-activated protein kinase
- LPS:
-
Lipopolysaccharide
- CRH:
-
Corticotropin-releasing hormone
- BNST:
-
Bed nucleus of the stria terminalis
- HPA:
-
Hypothalamic–pituitary–adrenal axis
References
Borah P, Deb PK, Chandrasekaran B, Goyal M, Bansal M, Hussain S, et al. Neurological consequences of SARS-CoV-2 infection and concurrence of treatment-induced neuropsychiatric adverse events in COVID-19 patients: navigating the Uncharted. Front Mol Biosci. 2021;8: 627723.
Wu Y, Xu X, Chen Z, Duan J, Hashimoto K, Yang L, et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav Immun. 2020;87:18–22.
Hugon J, Queneau M, Sanchez Ortiz M, Msika EF, Farid K, Paquet C. Cognitive decline and brainstem hypometabolism in long COVID: a case series. Brain Behav. 2022;12(4): e2513.
Bodnar B, Patel K, Ho W, Luo JJ, Hu W. Cellular mechanisms underlying neurological/neuropsychiatric manifestations of COVID-19. J Med Virol. 2021;93(4):1983–98.
Smith CJ, Renshaw P, Yurgelun-Todd D, Sheth C. Acute and chronic neuropsychiatric symptoms in novel coronavirus disease 2019 (COVID-19) patients: a qualitative review. Front Public Health. 2022;10: 772335.
Dinakaran D, Manjunatha N, Naveen Kumar C, Suresh BM. Neuropsychiatric aspects of COVID-19 pandemic: a selective review. Asian J Psychiatry. 2020;53: 102188.
Shah W, Hillman T, Playford ED, Hishmeh L. Managing the long term effects of covid-19: summary of NICE, SIGN, and RCGP rapid guideline. BMJ. 2021;372: n136.
McLoughlin BC, Miles A, Webb TE, Knopp P, Eyres C, Fabbri A, et al. Functional and cognitive outcomes after COVID-19 delirium. Eur Geriatr Med. 2020;11(5):857–62.
Kennedy M, Helfand BKI, Gou RY, Gartaganis SL, Webb M, Moccia JM, et al. Delirium in older patients with COVID-19 presenting to the Emergency Department. JAMA Netw Open. 2020;3(11): e2029540.
Nalleballe K, Reddy Onteddu S, Sharma R, Dandu V, Brown A, Jasti M, et al. Spectrum of neuropsychiatric manifestations in COVID-19. Brain Behav Immun. 2020;88:71–4.
Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020;7(7):611–27.
Scheiner NS, Smith AK, Wohlleber M, Malone C, Schwartz AC. COVID-19 and catatonia: a case series and systematic review of existing literature. J Acad Consult Liaison Psychiatry. 2021;62(6):645–56.
Taquet M, Luciano S, Geddes JR, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry. 2021;8(2):130–40.
Badenoch JB, Rengasamy ER, Watson C, Jansen K, Chakraborty S, Sundaram RD, et al. Persistent neuropsychiatric symptoms after COVID-19: a systematic review and meta-analysis. Brain Commun. 2021;4(1).
Batiha GE-S, Al-kuraishy HM, Al-Gareeb AI, Welson NN. Pathophysiology of post-COVID syndromes: a new perspective. Virol J. 2022;19(1):158.
Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, et al. Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain Behav Immun. 2020;89:594–600.
Woo MS, Malsy J, Pöttgen J, SeddiqZai S, Ufer F, Hadjilaou A, et al. Frequent neurocognitive deficits after recovery from mild COVID-19. Brain Commun. 2020;2(2):fcaa205.
Raman B, Cassar MP, Tunnicliffe EM, Filippini N, Griffanti L, Alfaro-Almagro F, et al. Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine. 2021;31: 100683.
Jackson CB, Farzan M, Chen B, Choe H. Mechanisms of SARS-CoV-2 entry into cells. Nat Rev Mol Cell Biol. 2022;23(1):3–20.
Desforges M, Le Coupanec A, Dubeau P, Bourgouin A, Lajoie L, Dubé M, et al. Human coronaviruses and other respiratory viruses: underestimated opportunistic pathogens of the central nervous system? Viruses. 2020;12(1):14.
Baig AM, Khaleeq A, Ali U, Syeda H. Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host–virus interaction, and proposed neurotropic mechanisms. ACS Chem Neurosci. 2020;11(7):995–8.
Achar A, Ghosh C. COVID-19-associated neurological disorders: the potential route of CNS invasion and blood–brain relevance. Cells. 2020;9(11):2360.
Meinhardt J, Radke J, Dittmayer C, Franz J, Thomas C, Mothes R, et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat Neurosci. 2021;24(2):168–75.
Matschke J, Lütgehetmann M, Hagel C, Sperhake JP, Schröder AS, Edler C, et al. Neuropathology of patients with COVID-19 in Germany: a post-mortem case series. Lancet Neurol. 2020;19(11):919–29.
Uginet M, Breville G, Assal F, Lövblad KO, Vargas MI, Pugin J, et al. COVID-19 encephalopathy: clinical and neurobiological features. J Med Virol. 2021;93(7):4374–81.
Shehata GA, Lord KC, Grudzinski MC, Elsayed M, Abdelnaby R, Elshabrawy HA. Neurological complications of COVID-19: underlying mechanisms and management. Int J Mol Sci. 2021;22(8):4081.
Song P, Li W, Xie J, Hou Y, You C. Cytokine storm induced by SARS-CoV-2. Clin Chim Acta. 2020;509:280–7.
Ragab D, Salah Eldin H, Taeimah M, Khattab R, Salem R. The COVID-19 cytokine storm; what we know so far. Front Immunol. 2020;11:1446.
Chen G, Wu D, Guo W, Cao Y, Huang D, Wang H, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest. 2020;130(5):2620–9.
Zawawi A, Naser AY, Alwafi H, Minshawi F. Profile of circulatory cytokines and chemokines in human coronaviruses: a systematic review and meta-analysis. Front Immunol. 2021;12:666223.
Akbari H, Tabrizi R, Lankarani KB, Aria H, Vakili S, Asadian F, et al. The role of cytokine profile and lymphocyte subsets in the severity of coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis. Life Sci. 2020;258:118167.
Henry BM, de Oliveira MHS, Benoit S, Plebani M, Lippi G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. 2020;58(7):1021–8.
Ling L, Chen Z, Lui G, Wong CK, Wong WT, Ng RWY, et al. Longitudinal cytokine profile in patients with mild to critical COVID-19. Front Immunol. 2021;12:763292.
Sun B, Tang N, Peluso MJ, Iyer NS, Torres L, Donatelli JL, et al. Characterization and biomarker analyses of post-COVID-19 complications and neurological manifestations. Cells. 2021;10(2):386.
Cao X. COVID-19: immunopathology and its implications for therapy. Nat Rev Immunol. 2020;20(5):269–70.
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506.
Costiniuk CT, Jenabian M-A. Acute inflammation and pathogenesis of SARS-CoV-2 infection: cannabidiol as a potential anti-inflammatory treatment? Cytokine Growth Factor Rev. 2020;53:63–5.
Giamarellos-Bourboulis EJ, Netea MG, Rovina N, Akinosoglou K, Antoniadou A, Antonakos N, et al. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe. 2020;27(6):992-1000.e3.
Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, et al. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis. 2020;71(15):762–8.
Ghazavi A, Ganji A, Keshavarzian N, Rabiemajd S, Mosayebi G. Cytokine profile and disease severity in patients with COVID-19. Cytokine. 2021;137: 155323.
Ortelli P, Ferrazzoli D, Sebastianelli L, Engl M, Romanello R, Nardone R, et al. Neuropsychological and neurophysiological correlates of fatigue in post-acute patients with neurological manifestations of COVID-19: insights into a challenging symptom. J Neurol Sci. 2021;420: 117271.
Kovarik JJ, Kämpf AK, Gasser F, Herdina AN, Breuer M, Kaltenecker CC, et al. Identification of immune activation markers in the early onset of COVID-19 infection. Front Cell Infect Microbiol. 2021;11: 651484.
Zawawi A, Naser AY, Alwafi H, Minshawi F. Profile of circulatory cytokines and chemokines in human coronaviruses: a systematic review and meta-analysis. Front Immunol. 2021;12: 666223.
Zhou Z, Ren L, Zhang L, Zhong J, Xiao Y, Jia Z, et al. Heightened innate immune responses in the respiratory tract of COVID-19 patients. Cell Host Microbe. 2020;27(6):883-90.e2.
Burkert FR, Lanser L, Bellmann-Weiler R, Weiss G. Coronavirus disease 2019: clinics, treatment, and prevention. Front Microbiol. 2021;12: 761887.
Wang J, Jiang M, Chen X, Montaner LJ. Cytokine storm and leukocyte changes in mild versus severe SARS-CoV-2 infection: review of 3939 COVID-19 patients in China and emerging pathogenesis and therapy concepts. J Leukoc Biol. 2020;108(1):17–41.
Zhang C, Wu Z, Li JW, Zhao H, Wang GQ. Cytokine release syndrome in severe COVID-19: interleukin-6 receptor antagonist tocilizumab may be the key to reduce mortality. Int J Antimicrob Agents. 2020;55(5): 105954.
Poyiadji N, Shahin G, Noujaim D, Stone M, Patel S, Griffith B. COVID-19-associated acute hemorrhagic necrotizing encephalopathy: imaging features. Radiology. 2020;296(2):E119–20.
Canada.ca. COVID-19 signs, symptoms and severity of disease: A clinician guide—Canada.ca 2019 [Available from: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/signs-symptoms-severity.html.
Özçelik Korkmaz M, Eğilmez OK, Özçelik MA, Güven M. Otolaryngological manifestations of hospitalised patients with confirmed COVID-19 infection. Eur Arch Otorhinolaryngol. 2021;278(5):1675–85.
Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. 2020;92(6):552–5.
Nataf S. An alteration of the dopamine synthetic pathway is possibly involved in the pathophysiology of COVID-19. J Med Virol. 2020;92(10):1743–4.
Khalefah MM, Khalifah AM. Determining the relationship between SARS-CoV-2 infection, dopamine, and COVID-19 complications. J Taibah Univ Med Sci. 2020;15(6):550–3.
Yang L, Han Y, Nilsson-Payant BE, Gupta V, Wang P, Duan X, et al. A human pluripotent stem cell-based platform to study SARS-CoV-2 tropism and model virus infection in human cells and organoids. Cell Stem Cell. 2020;27(1):125-36.e7.
Netland J, Meyerholz DK, Moore S, Cassell M, Perlman S. Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J Virol. 2008;82(15):7264–75.
Dantzer R. Neuroimmune interactions: from the brain to the immune system and vice versa. Physiol Rev. 2018;98(1):477–504.
Roushdy T, Hamid E. A review on SARS-CoV-2 and stroke pathogenesis and outcome. Egypt J Neurol Psychiatr Neurosurg. 2021;57(1):63.
Attademo L, Bernardini F. Are dopamine and serotonin involved in COVID-19 pathophysiology? Eur J Psychiatry. 2021;35(1):62–3.
Crunfli F, Carregari VC, Veras FP, Silva LS, Nogueira MH, Antunes A, et al. Morphological, cellular, and molecular basis of brain infection in COVID-19 patients. Proc Natl Acad Sci USA. 2022;119(35): e2200960119.
Chen S, Han Y, Yang L, Kim T, Nair M, Harschnitz O, et al. SARS-CoV-2 infection causes dopaminergic neuron senescence. Res Sq. 2021.
Antonini A, Leta V, Teo J, Chaudhuri KR. Outcome of Parkinson’s disease patients affected by COVID-19. Mov Disord. 2020;35(6):905–8.
Klempin F, Mosienko V, Matthes S, Villela DC, Todiras M, Penninger JM, et al. Depletion of angiotensin-converting enzyme 2 reduces brain serotonin and impairs the running-induced neurogenic response. Cell Mol Life Sci. 2018;75(19):3625–34.
Cheng H, Wang Y, Wang GQ. Organ-protective effect of angiotensin-converting enzyme 2 and its effect on the prognosis of COVID-19. J Med Virol. 2020;92(7):726–30.
Jansen van Vuren E, Steyn SF, Brink CB, Möller M, Viljoen FP, Harvey BH. The neuropsychiatric manifestations of COVID-19: interactions with psychiatric illness and pharmacological treatment. Biomed Pharmacother. 2021;135:111200.
Xia H, Lazartigues E. Angiotensin-converting enzyme 2 in the brain: properties and future directions. J Neurochem. 2008;107(6):1482–94.
Hashimoto T, Perlot T, Rehman A, Trichereau J, Ishiguro H, Paolino M, et al. ACE2 links amino acid malnutrition to microbial ecology and intestinal inflammation. Nature. 2012;487(7408):477–81.
Bartolomucci A, Carola V, Pascucci T, Puglisi-Allegra S, Cabib S, Lesch K-P, et al. Increased vulnerability to psychosocial stress in heterozygous serotonin transporter knockout mice. Dis Model Mech. 2010;3(7–8):459–70.
Barzegar M, Vital S, Stokes KY, Wang Y, Yun JW, White LA, et al. Human placenta mesenchymal stem cell protection in ischemic stroke is Angiotensin converting enzyme-2 (ACE-2) and masR receptor dependent. Stem Cells. 2021;39:1225.
Dolatshahi M, Sabahi M, Aarabi MH. Pathophysiological clues to how the emergent SARS-CoV-2 can potentially increase the susceptibility to neurodegeneration. Mol Neurobiol. 2021;58(5):2379–94.
Simanjuntak Y, Liang J-J, Lee Y-L, Lin Y-L. Japanese encephalitis virus exploits dopamine D2 receptor-phospholipase C to target dopaminergic human neuronal cells. Front Microbiol. 2017;8:651.
Xia H, Lazartigues E. Angiotensin-converting enzyme 2: central regulator for cardiovascular function. Curr Hypertens Rep. 2010;12(3):170–5.
Wang X-L, Iwanami J, Min L-J, Tsukuda K, Nakaoka H, Bai H-Y, et al. Deficiency of angiotensin-converting enzyme 2 causes deterioration of cognitive function. NPJ Aging Mech Dis. 2016;2(1):16024.
Kantonen J, Mahzabin S, Mäyränpää MI, Tynninen O, Paetau A, Andersson N, et al. Neuropathologic features of four autopsied COVID-19 patients. Brain Pathol. 2020;30(6):1012–6.
Augustin M, Schommers P, Stecher M, Dewald F, Gieselmann L, Gruell H, et al. Post-COVID syndrome in non-hospitalised patients with COVID-19: a longitudinal prospective cohort study. Lancet Reg Health Europe. 2021;6:100122.
Versace V, Sebastianelli L, Ferrazzoli D, Romanello R, Ortelli P, Saltuari L, et al. Intracortical GABAergic dysfunction in patients with fatigue and dysexecutive syndrome after COVID-19. Clin Neurophysiol. 2021;132(5):1138–43.
Ljubisavljevic M. Transcranial magnetic stimulation and the motor learning-associated cortical plasticity. Exp Brain Res. 2006;173(2):215–22.
Douaud G, Lee S, Alfaro-Almagro F, Arthofer C, Wang C, McCarthy P, et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature. 2022;604(7907):697–707.
Leighton S, Nerurkar L, Krishnadas R, Johnman C, Graham G, Cavanagh J. Chemokines in depression in health and in inflammatory illness: a systematic review and meta-analysis. Mol Psychiatry. 2018;23(1):48–58.
Taquet M, Geddes J, Husain M, Luciano S, Harrison P. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8:416.
Mazza MG, Palladini M, De Lorenzo R, Magnaghi C, Poletti S, Furlan R, et al. Persistent psychopathology and neurocognitive impairment in COVID-19 survivors: effect of inflammatory biomarkers at three-month follow-up. Brain Behav Immun. 2021;94:138–47.
Guo Q, Zheng Y, Shi J, Wang J, Li G, Li C, et al. Immediate psychological distress in quarantined patients with COVID-19 and its association with peripheral inflammation: a mixed-method study. Brain Behav Immun. 2020;88:17–27.
Jain S, Gautam V, Naseem S. Acute-phase proteins: as diagnostic tool. J Pharm Bioallied Sci. 2011;3(1):118–27.
Haapakoski R, Mathieu J, Ebmeier KP, Alenius H, Kivimäki M. Cumulative meta-analysis of interleukins 6 and 1β, tumour necrosis factor α and C-reactive protein in patients with major depressive disorder. Brain Behav Immun. 2015;49:206–15.
Torres-Platas SG, Cruceanu C, Chen GG, Turecki G, Mechawar N. Evidence for increased microglial priming and macrophage recruitment in the dorsal anterior cingulate white matter of depressed suicides. Brain Behav Immun. 2014;42:50–9.
Boldrini M, Canoll PD, Klein RS. How COVID-19 affects the brain. JAMA Psychiat. 2021;78(6):682–3.
Delgado PL. Depression: the case for a monoamine deficiency. J Clin Psychiatry. 2000;61(Suppl 6):7–11.
Zhu CB, Lindler KM, Owens AW, Daws LC, Blakely RD, Hewlett WA. Interleukin-1 receptor activation by systemic lipopolysaccharide induces behavioral despair linked to MAPK regulation of CNS serotonin transporters. Neuropsychopharmacology. 2010;35(13):2510–20.
Konsman JP, Veeneman J, Combe C, Poole S, Luheshi GN, Dantzer R. Central nervous action of interleukin-1 mediates activation of limbic structures and behavioural depression in response to peripheral administration of bacterial lipopolysaccharide. Eur J Neurosci. 2008;28(12):2499–510.
Roushdy T. SARS-CoV-2 and monkeypox: what is common and what is not in a present pandemic versus a potential one—a neuropsychiatric narrative review. Egypt J Neurol Psychiatry Neurosurg. 2022;58(1):127.
Xiang YT, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. 2020;7(3):228–9.
NIMH. NIMH (2021). Domain: Negative Valence Systems 2021. Available from: NIMH. (2021). Domain: Negative Valence Systems. Retrieved from https://www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/constructs/negative-valence-systems.
Wilkialis L, Rodrigues NB, Cha DS, Siegel A, Majeed A, Lui LMW, et al. Social isolation, loneliness and generalized anxiety: implications and associations during the COVID-19 quarantine. Brain Sci. 2021;11(12):1620.
Michopoulos V, Powers A, Gillespie CF, Ressler KJ, Jovanovic T. Inflammation in fear- and anxiety-based disorders: PTSD, GAD, and beyond. Neuropsychopharmacology. 2017;42(1):254–70.
Lebow MA, Chen A. Overshadowed by the amygdala: the bed nucleus of the stria terminalis emerges as key to psychiatric disorders. Mol Psychiatry. 2016;21(4):450–63.
Wang LA, de Kloet AD, Smeltzer MD, Cahill KM, Hiller H, Bruce EB, et al. Coupling corticotropin-releasing-hormone and angiotensin converting enzyme 2 dampens stress responsiveness in male mice. Neuropharmacology. 2018;133:85–93.
Motzkin JC, Philippi CL, Wolf RC, Baskaya MK, Koenigs M. Ventromedial prefrontal cortex is critical for the regulation of amygdala activity in humans. Biol Psychiat. 2015;77(3):276–84.
Kleinridders A, Pothos EN. Impact of brain insulin signaling on dopamine function, food intake, reward, and emotional behavior. Curr Nutr Reports. 2019;8(2):83–91.
Hamer JA, Testani D, Mansur RB, Lee Y, Subramaniapillai M, McIntyre RS. Brain insulin resistance: a treatment target for cognitive impairment and anhedonia in depression. Exp Neurol. 2019;315:1–8.
Fardet L, Flahault A, Kettaneh A, Tiev K-P, Généreau T, Tolédano C, et al. Corticosteroid-induced clinical adverse events: frequency, risk factors and patient’s opinion. Br J Dermatol. 2007;157(1):142–8.
Biggioggero M, Crotti C, Becciolini A, Favalli EG. Tocilizumab in the treatment of rheumatoid arthritis: an evidence-based review and patient selection. Drug Des Dev Ther. 2019;13:57.
Miller BJ, Dias JK, Lemos HP, Buckley PF. An open-label, pilot trial of adjunctive tocilizumab in schizophrenia. J Clin Psychiatry. 2016;77(2):275.
García CC, Sánchez EA, Huerta DH, Gómez-Arnau J. Covid-19 treatment-induced neuropsychiatric adverse effects. Gen Hosp Psychiatry. 2020;67:163.
Pezeshki PS, Rezaei N. Immune checkpoint inhibition in COVID-19: risks and benefits. Expert Opin Biol Ther. 2021;21(9):1173–9.
McGinnis GJ, Raber J. CNS side effects of immune checkpoint inhibitors: preclinical models, genetics and multimodality therapy. Immunotherapy. 2017;9(11):929–41.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from any funding agency in the public or commercial sector.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript. SMT: conceptualization, collected data, supervision, investigation, writing original draft, writing—review and editing. SM: writing, conceptualization, review and editing. ZHH: investigation on the topic, collected data, writing—review and editing. EG: investigation on the topic, collected data, writing—review and editing. BP: supervision, conceptualization, methodology, investigation, writing—review and editing, supervision.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mannekote Thippaiah, S., Amanullah, S., Huang, Z.H. et al. Biological correlates of the neuropsychiatric symptoms in SARS-CoV-2 infection: an updated review. Egypt J Neurol Psychiatry Neurosurg 59, 101 (2023). https://doi.org/10.1186/s41983-023-00705-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00705-8