
Abstract
Background
There is increasing evidence that prolonged or recurrent seizures can cause or exacerbate cognitive impairment (CI) in memory, attention, orientation, and visuospatial and abstraction disabilities, all of which can jeopardize educational progress and achievement throughout life. The objectives of our study are to assess the cognitive functions in people with epilepsy (PwE) using P300 event-related potentials (ERPs), and correlate each P300 components with six explanatory variables (epilepsy type, seizure type, NHS3 score- seizure severity, disease duration, age at first seizure, and the number of anticonvulsant medications).
Methods
One hundred and two PwE [52 with focal epilepsy and 50 with generalized epilepsy, as classified by the International League Against Epilepsy in 2017]. They underwent electroencephalography (EEG) and P300. The Montreal Cognitive Assessment (MoCA) scale was used to assess baseline cognitive functions.
Results
Epileptic patients showed significant latency prolongation and amplitude reduction of P300 as compared to non-epileptic population. Longer P300 latency and lower amplitude were seen in patients with abnormal EEG records. P300 latency was longer in patients using poly-therapy. P300 components correlated well with age at presentation and disease duration but not with NHS3. According to epilepsy type, 50.98% of PwE had focal epilepsy and 49.02% had generalized epilepsy, 85.29% of them had abnormal EEG recording. Considering seizure type, 47.06% had a generalized tonic–clonic seizure, 38.24% had a focal to bilateral tonic–clonic seizure, 20.59% had a myoclonic seizure, 12.75% had a focal with impaired awareness seizure, 3.92% had a focal aware seizure, and 2.94% had an absence seizure. Seventy-seven PwE had one type of seizure, while 25 had more than one type of seizure. The NHS3 score was higher in those with a single seizure type than in those with multiple seizure types.
Conclusion
All seizure types had an abnormal P300 component, indicating cognitive function deficits. P300 may be a promising objective method for assessing cognitive function in PwE. The number of antiepileptic drugs used, the presence of EEG abnormalities, the age at presentation, and the duration of the disease are the factors that best correlate with cognitive impairment (CI).
Similar content being viewed by others


Introduction
For many patients and families, the burden of the epilepsy is largely caused by comorbid conditions, including behavioral changes and cognitive impairment (CI), such as memory, attention, processing difficulties or learning disabilities, and mental health disorders, such as depression and anxiety, attention-deficit hyperactivity disorder, intellectual disability, and autism; and somatic co-morbidities, such as sleep disorders and migraines [1].
These comorbidities, previously considered to be secondary to uncontrolled seizures or medication adverse effects, are now recognized as an integral part of the disorder, sometimes even preceding the seizures and attributable to an underlying disorder of neuronal networks [2].
In people with epilepsy (PwE), CI may present at the onset of epilepsy [3]. These can have a significant impact on several day-to-day functions, such as schoolwork in children and driving ability in adults [4]. Epilepsy can also further impair already compromised cognitive function, for example in elderly people [5]. Some patients find these cognitive consequences more debilitating than the actual seizures [6].
Because early seizures can induce permanent deficits and increase seizure susceptibility and that prolonged exposure to abnormal neural activity during a critical period of cerebral maturation may disrupt the structural and functional changes in the brain, thus diffuse CI are more often documented in children with additional troubles [7].
Severity and chronicity are the major sources of CI [8]. Some studies showed that in newly diagnosed and untreated epileptic patients, CI are already present [9, 10] in more than 50% of patients.
Electroencephalography (EEG) is one of the most effective electrophysiological examining techniques for understanding neurobiological dysregulation. The time-locked activity of EEG, known as event-related potential (ERP), is a small voltages generated in the brain structures in response to sensory, cognitive, or motor processes [11].
Event-related potentials have been linked with different cognitive functions, such as attention, concentration, memory, and decision-making. Therefore, they are considered as a clinically important tool for evaluating CI in various neurological disorders, including Alzheimer’s, Parkinson’s disease, epilepsy, schizophrenia, and stroke [12, 13].
The aims of our study are to evaluate the cognitive functions in PwE using the P300 ERPs, and to correlate P300 components with certain characteristics of those patients like epilepsy type, seizure type, seizure severity, duration of the disease, age at first presentation of epilepsy, and the number of anticonvulsant medications.
Methods
This is a two-center case-control study conducted in the Neurophysiology Department of Al-Imammian Al- Kadhimiyain Medical City and Baghdad Teaching Hospital in Baghdad from Jan. 2020. to Dec. 2021. The study was approved by the Iraqi Board for Medical Specialties (Decision No. 291; Date 21/1/2021).
One hundred and two PwE comprised 52 with focal epilepsy and 50 with generalized epilepsy classified according to the 2017 classification of ILAE for types of seizures and type of epilepsy. Age of the patient was between 12 and 40 years. All the patients can read and write. Patients with history of impaired hearing, diagnosed psychiatric disorder or abnormal brain MRI were excluded from the study. Another 50 ages and sex-matched healthy subjects serve as the control group.
Clinical and neurophysiologic assessment
All patients enrolled in the study were examined by consultant neurologists to determine the semiology of the events, which were assisted by routine EEG, brain magnetic resonance imaging (epilepsy protocol), home videos, and video EEG recording.
The National Hospital Seizure Severity Scale (NHS3), which includes seven seizure-related factors and generates a score ranging from 1 to 27, was used to assess seizure severity in patients who had one or more seizures within the previous 12 months [14]. Patients with an NHS3 score of 15 or higher were classified as having severe seizure attacks, while those with a score of 15 or less were classified as having mild seizure attacks [15], unless they had more than 10 seizures in the previous 12 months, in which case they were classified as having severe seizure attacks. We excluded all patients who were seizure free for the last 12 months from our study. The test was approved for children and adolescents [16].
Electroencephalography
Clinical diagnosis of epilepsy was evident with routine and long- term EEG. The EEGs were received from the hospital's epilepsy clinic, where they were performed by the same technician and reviewed by the same neurophysiologist to lower inter-rater variability. We looked for positive EEG findings such as focal or generalized epileptiform discharges, sharp waves, poly spikes, spike wave activities, and slow wave activities.
Montreal cognitive assessment test
Cognitive functions of all participants were assessed using the Montreal Cognitive Assessment (MoCA) test scale version 8.3. The test validity for young adults and adolescents aged 14–21 for detecting cognitive deficits was approved [17]. MoCA consists of 30 items divided into the domains of attention, language, memory, visuospatial, executive functions, and orientation and scored accordingly from 0 to 30 with a cutoff value of 26. A score of 26 or above was considered normal [18]. Accordingly, MoCA score ranges from 14 to 25 refers to impaired cognition, and from 27 to 30 goes with intact cognition [19].
P300 event-related potentials
In a silent room, P300 was elicited using a Cadwell electromyography machine (Kennewick, WA99336, USA) using an auditory "oddball" paradigm. In accordance with the 10–20 International System, standard Ag/AgCl electrodes positioned at Cz, referenced at the mastoid process, and a forehead ground were used.
Subjects were instructed to mentally count rare tones while lying comfortably on the couch with their eyes closed, and they were then asked to report the number of rare tones counted at the end of each run. To determine performance accuracy, each patient's count was compared to the actual number of target tones provided at the end of each session. Two or three trials were conducted to ensure the consistency of the waveform, with each trial lasting until 200 artifact-free infrequent stimuli responses were recorded and averaged. The P300's latencies and amplitudes were measured.
The impedance was kept at 5 K or less, the band pass filter was set between 1 and 30 Hz, and the analysis time was set at 1024 ms with a pre-stimulus baseline record of 100 ms.
Statistical analysis
All statistical analyses were performed using statistical package of social sciences (SPSS software version 25.0, Chicago, USA). Continuous data were presented as mean ± SD and analyzed with Student t test. Categorical variables were expressed as number and percentage. Pearson’s correlation test was used to explore the possible correlation of neurophysiological parameters with age, disease duration and NHS3. A p- value less than 0.05 were considered to indicate a statistically significant difference.
Results
Table 1 shows the demographic information for the study population. The age, gender, and educational level of the PwE and control groups were not significantly different (p = 0.370; p = 0.425; p = 0.160, respectively). The majority of the PwE (85.29%) have abnormal EEG records while 15 (14.71%) have normal EEG records. Fifty-two PwE (50.98%) had focal epilepsy whereas 50 (49.02%) had generalized epilepsy.
According to the seizure type, 48 PwE (47.06%) had generalized tonic clonic seizures, 39 (38.24%) had focal to bilateral tonic clonic seizures, 21 (20.59%) had myoclonic seizures, 13 (12.75%) had focal with impaired awareness seizures, 4 (3.92%) had focal aware seizure, and 3 (2.94%) had absence seizures.
The majority of PwE (75.49%) had one seizure type while 25 (24.51%) had more than one seizure type. In terms of the NHS3, those with one seizure type received a score of 15.46 ± 4.39, while those with more than one seizure type received a score of 5.46 ± 5.67.
Table 2 displays the data from the P300 ERPs of the study population. The latency in PwE was 330.12 ± 30.23 ms which is significantly longer (p < 0.001) than 294.87 ± 9.5 ms in the control group. On the contrary, the amplitude in PwE was 10.68 ± 1.85 µV which is significantly lower (p = 0.005) than the 11.55 ± 1.59 µV in the control group.
Table 3 illustrates the possible relationship (if any) between P300 parameters and various demographic and clinical data of PwE. There was no significant relationship between gender and P300 latency or amplitude. Patients suffering from focal epilepsy have longer latencies than those suffering from generalized epilepsy (p < 0.001).
The P300 latency was longer (p = 0.001) and the amplitude was lower (p = 0.019) in PwE with abnormal compared to those with normal EEG records. Moreover, the P300 latency but not the amplitude was significantly different (longer) in PwE receiving polytherapy versus those receiving monotherapy (p = 0.001). Furthermore, neither the latency nor the amplitude of the P300 were associated with the presence of one or more seizure types.
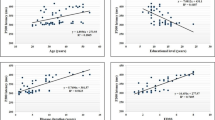
The P300 latency was found to be negatively related to age at onset (r = − 0.293; p = 0.003) and positively related to disease duration r = 0.470; p < 0.001). On the contrary, the amplitude was positively correlated with age at onset (r = 0.270; p = 0.006) and negatively correlated with disease duration (r = − 0.328; p = 0.001) as shown in Table 4 and Fig. 1.

Scatter plot and regression line between age at onset and P300 latency (upper right) and P300 amplitude (upper left), disease duration and P300 latency (lower right), and P300 amplitude (lower left) in PwE
Discussion
The P300 has been widely used for evaluating cognitive functions in various neurophysiological disorders due to its very stable latency in normal controls [20, 21]. Epilepsy is one of the major causes of central auditory disorders among the various neurological disorders [22].
Our study indicates a prolonged P300 latency and attenuated amplitude in PwE. These changes are indicative of impaired cognitive processing because this component provides information about various cognitive processes, such as memory, attention, auditory discrimination, processing of sequential information, and decision making [22, 23]. This is further supported by the fact that in normal subjects, P300 latency is negatively associated with cognitive functions, with shorter latencies associated with excellent cognitive performance [24, 25].
Significant changes in this long-latency component of ERPs have been linked to hippocampus damage in PwE due to its possible involvement in ERP generation. It is thought that the involvement of mesencephalic reticular formation and the sum of the activities of various areas, including cortical and subcortical structures, are involved in its generation [26, 27]. Furthermore, according to Musiek et al. [28], the decrease in P300 amplitude in these subjects could indicate that fewer neurons were functioning or that the intensity of neural firing was reduced.
Many studies have examined CI in PwE using ERP analysis. The outcomes are diverse and frequently contentious. While many studies [29,30,31,32,33] reached similar conclusions to ours, others found no differences [34,35,36], whereas, the P300 in PwE was shorter than in controls in other studies [37, 38].
These controversies in the aforementioned studies could be attributed to a variety of factors that varied greatly between studies, including sample size, patient age, location of P300 recording, recording electrodes, frequent/rare stimulus in hertz, stimulus intensity in decibels, type of epilepsy, disease duration, seizure severity, epileptogenesis process itself, the frequency of seizures, lesions, and anti-epileptic treatments used [23, 32].
Gender does not appear to be a significant variable in this study of P300 latency and amplitude. A finding that is consistent with other research [39, 40].
Event related potential changes occur in a variety of epilepsy types, including temporal lobe epilepsy, idiopathic generalized epilepsy, and benign childhood epilepsy with centrotemporal spikes [22]. The effect of epilepsy type on P300 responses was discovered in our study. Patients with focal epilepsy have the longest delay, which can be explained by structural etiologies such as cortical dysplasia or tumors, mesial temporal sclerosis, and migrational disorders.
Clinically, these children may experience frequent seizures with auras and impaired consciousness [41, 42]. Their seizures frequently become resistant to high doses of drugs, necessitating surgical procedures [43, 44]. Moreover, their abnormal discharges frequently occur exactly where the auditory pathway ends, resulting in neural network impairment and extratemporal abnormalities, which are associated with language impairment and auditory processing deficits [23, 45]. Similar studies, which agree with our findings, report longer P300 latency and lower amplitude in those with temporal lobe epilepsy than in those with idiopathic generalized epilepsy [27, 46, 47].
The P300 in PwE with and without epileptiform EEG discharges was assessed in this study, and patients with normal EEG performed better in cognitive function tests (P300) than patients with abnormal EEG. This suggests that in this study, epileptiform discharges had an additional effect on cognitive function. It is unclear why epileptiform EEG discharges affect cognitive functioning, but some of these discharges appear to disrupt central information processing in the same way that seizures do. In addition, this could be related to the fact that epileptiform discharges generating neurons showed liability to premature death [48].
Several studies have found a sudden and unexpected drop in school performance in children with interictal EEG discharges [49], as well as a drop in intelligence quotient scores in epileptic children with frequent episodes of epileptiform EEG discharges [50].
There is little data on the relationship between P300 latency and EEG findings in PwE. In line with this study, Triantafyllou et al. [46] discovered that epileptic patients with abnormal EEGs had significantly longer P300 latencies than those with normal EEGs. However, Naganuma et al. [25] and Ozmenek et al. [30] claim that the presence of EEG abnormalities has little effect on cognitive function. Furthermore, Gotman and Marciani discovered that the number of paroxysmal discharges does not always correspond to the severity of epileptic activity [51].
The current study found that those on polytherapy had more CI than those on monotherapy. This finding is consistent with those of Park and Kwon [52] and Witt and Helmstaedter [53]. While AEDs can have a negative impact on cognitive function by suppressing neuronal excitability or increasing inhibitory neurotransmission [52], they are rarely the sole cause of cognitive deficits in certain patients. AEDs affect cognitive functioning in a dose-dependent manner, which can be exacerbated by AED polytherapy.
Attention/vigilance, psychomotor speed, and secondary involvement of other cognitive functions (e.g., memory) are the main cognitive effects of AEDs [54]. Furthermore, in monotherapy and when the AED is present at therapeutic serum concentrations, the magnitude of AED-related cognitive dysfunction is generally modest [52] shifting therapy from polytherapy to monotherapy improved cognition. Many theories have been proposed to explain the link between polytherapy and CI. One theory is based on the fact that pharmacodynamic interactions with negative cognitive effects are likely to occur during a polytherapy regimen [55].
The P300 was found to be significantly correlated with disease duration and age at onset in the current study. These findings suggest that uncontrolled seizures impair cognitive function, with the effects being most severe in infancy and diminishing with increasing age at onset. While studies found that the prolonged P300 latency was significantly correlated with epilepsy duration, age at onset, seizure frequency, and antiepileptic treatment, other studies found conflicting results [37, 56, 57]. Other studies found no link between latency prolongation and seizure frequency, seizure type, seizure duration, or cerebral imaging pathologies [25, 29, 58].
Conclusions
Our study concludes that abnormal P300 was observed across different types of seizures, indicating cognitive function deficits. As a result, the P300 may be a promising objective method for assessing cognitive function in PwE. The factors that best correlate and are associated with CI are epilepsy type, EEG abnormality, number of antiepileptic drugs, age at presentation, and disease duration. Thus, our findings show that screening for CI is critical in PwE, and that adequate epilepsy treatment should not focus solely on seizure control. We also recommend researching the effect of old versus new AEDs on cognitive functions, as well as the duration of AED treatment.
Availability of data and materials
All data generated or analyzed during this study are included in this published article. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AEDs:
-
Antiepileptic drug
- CI:
-
Cognitive impairment
- EEG:
-
Electroencephalography
- ERPs:
-
Event-related potentials
- NHS3:
-
National Hospital Seizure Severity Scale
- PwE:
-
People with epilepsy
References
Stafstrom CE, Carmant L. Seizures and epilepsy: an overview for neuroscientists. Cold Spring Harb Perspect Med. 2015;5: a022426.
Brooks-Kayal AR, Bath KG, Berg AT, et al. Issues related to symptomatic and disease-modifying treatments affecting cognitive and neuropsychiatric comorbidities of epilepsy. Epilepsia. 2013;54(suppl. 4):44–60.
Braun KP. Preventing cognitive impairment in children with epilepsy. Curr Opin Neurol. 2017;30(2):140–7.
van Rijckevorsel K. Cognitive problems related to epilepsy syndromes, especially malignant epilepsies. Seizure. 2006;15(4):227–34.
Lodhi S, Agrawal N. Neurocognitive problems in epilepsy. Adv Psychiat Treat. 2012;18(3):232–40.
Aldenkamp AP. Cognitive impairment in epilepsy: state of affairs and clinical relevance. Seizure. 2006;15:219–120.
Smith ML, Elliott IM, Lach L. Cognitive skills in children with intractable epilepsy: comparison of surgical and nonsurgical candidates. Epilepsia. 2002;43:631–7.
Bjørnaes H, Stabell K, Henrikesen O, et al. The effects of refractory epilepsy on intellectual function in children and adults. Seizure. 2001;10:250–9.
Austin JK, Dunn DW, Johnson CS, et al. Behavioral issues involving children and adolescents with epilepsy and the impact of their families: recent research data. Epilepsy Behav. 2004;5(S3):S33–41.
Fastenau PS, Shen J, Dunn DW, et al. Neuropsychological predictors of academic underachievement in pediatric epilepsy: moderating roles of demographic, seizure and psychosocial variables. Epilepsia. 2004;45:1261–72.
Patel SH, Azzam PN. Characterization of N200 and P300: selected studies of the event-related potential. Int J Med Sci. 2005;2:147–54.
Kaga Y, Kanemura H, Ishii S, et al. Event-related potentials for cognitive assessment of patients with epilepsy. Pediat Therapeut. 2013;3:161.
Tsolaki A, Kosmidou V, Hadjileontiadis L, et al. Brain source localization of MMN, P300 and N400: aging and gender differences. Brain Res. 2015;1603:32–49.
O’Donoghue MF, Duncan JS, Sander JWAS. The National hospital seizure severity scale: a further development of the Chalfont seizure severity scale. Epilepsia. 1996;37(6):563–71.
Moran N, Poole K, Bell G, Solomon J, Kendall S, McCarthy M, et al. Epilepsy in the United Kingdom: seizure frequency and severity, anti-epileptic drug utilization and impact on life in 1652 people with epilepsy. Seizure. 2004;13:425–33. https://doi.org/10.1016/j.seizure.2003.10.002.
Adedeji IA, Adamu AS, Bashir FM. Factors associated with seizure severity among children with epilepsy in Northern Nigeria, Ghana. Med J. 2022;56(1):23–7.
Pike NA, Poulsen MK, Woo MA. Validity of the Montreal Cognitive Assessment screener in adolescents and young adults with and without congenital heart disease. Nurs Res. 2017;66(3):222–30.
Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695–9.
Guo QH, Cao XY, Zhou Y, Zhao QH, Ding D, Hong Z. Application study of quick cognitive screening test in identifying mild cognitive impairment. Neurosci Bull. 2010;26(1):47–54.
Duncan CC, Barry RJ, Connolly JF, et al. Event-related potentials in clinical research: guidelines for eliciting, recording, and quantifying mismatch negativity, P300, and N400. Clin Neurophysiol. 2009;120:1883–908.
Gokcay A, Celebisoy N, Gokcay F, et al. Cognitive functions evaluated by P300 and visual and auditory number assays in children with childhood epilepsy with occipital paroxysms (CEOP). Seizure. 2006;15:22–7.
Sowndhararajan K, Kim M, Deepa P, et al. Application of the P300 event-related potential in the diagnosis of epilepsy disorder: a review. Sci Pharm. 2018;86(2):10.
Casali RL, Ramos do Amaral MI, Boscariol M, et al. Comparison of auditory event-related potentials between children with benign childhood epilepsy with centrotemporal spikes and children with temporal lobe epilepsy. Epilepsy Behav. 2016;59:111–6.
Vecchio F, Maatta S. The use of auditory event-related potentials in Alzheimer’s disease diagnosis. Int J Alzheimer Dis. 2011;2011:653173–210.
Naganuma Y, Konishi T, Hongou K, et al. Epileptic seizures and event-related potentials (P300) in childhood partial epilepsies. Clin Electroencephalogr. 1997;28:106–11.
Sunaga Y, Hikima A, Otsuka T, et al. P300 event-related potentials in epileptic children. Clin Electroencephalogr. 1994;25:13–7.
Fukai M, Motomura N, Kobayashi S, et al. Event-related potential (P300) in epilepsy. Acta Neurol Scand. 1990;82:197–202.
Musiek FE, Baran J, Pinheiro M. P300 results in patients with lesions of the auditory areas of the cerebrum. J Am Acad Audiol. 1992;3:5–15.
Celebisoy N, Kisabay A, Gökçay F, et al. Evaluating cognitive functions with visual and auditory number assays and P300 in children with epilepsy. Brain Dev. 2005;27:253–8.
Ozmenek OA, Nazliel B, Leventoäÿlu A, et al. The role of event related potentials in evaluation of subclinical cognitive dysfunction in epileptic patients. Acta Neurol Belg. 2008;108:58–63.
Tandon OP, Duhan P. Event-related evoked potential responses in epileptic patients. Indian J Physiol Pharmacol. 2000;44:461–6.
Zhong R, Li M, Chen Q, et al. The P300 event-related potential component and cognitive impairment in epilepsy: a systematic review and meta-analysis. Front Neurol. 2019;10:943.
Gupta S, Prasad A, Singh R, et al. Auditory and visual P300 responses in early cognitive assessment of children and adolescents with epilepsy. J Pediatr Neurosci. 2020;15:9–14.
Katayama J, Polich J. P300, probability, and the three-tone paradigm. Electroencephalog Clin Neurophysiol. 1996;100:555–62. https://doi.org/10.1016/s0168-5597(96)95171-0.
Chayasirisobhon WV, Chayasirisobhon S, Tin SN, et al. Scalp-recorded auditory P300 event-related potentials in new-onset untreated temporal lobe epilepsy. Clin EEG Neurosci. 2007;38:168–71.
Boscariol M, Casali RL, Amaral MI, et al. Language and central temporal auditory processing in childhood epilepsies. Epilepsy Behav. 2015;53:180–3.
Sun W, Wang Y, Wang W, et al. Attention changes in epilepsy patients following 3-month topiramate or valproate treatment revealed by event-related potential. Int J Psychophysiol. 2008;68:235–41.
Duncan CC, Mirsky AF, Lovelace CT, et al. Assessment of the attention impairment in absence epilepsy: comparison of visual and auditory P300. Int J Psychophysiol. 2009;73:118–22.
Stenklev NC, Laukli E. Cortical cognitive potentials in elderly persons. J Am Acad Audiol. 2004;15(6):401–13.
Martin DA, Tremblay KL, Stapells DR. Principles and applications of cortical auditory evoked potentials. In: Burkard RF, Don M, Eggermont JJ, editors. Auditory evoked potentials: basic principles and clinical application. Baltimore: Lippincott Williams & Wilkins; 2007. p. 482–507.
Bourgeois BFD. Temporal lobe epilepsy in infants and children. Brain Dev. 1998;20:135–41.
Franzon RC, Guerreiro MM. Temporal lobe epilepsy in childhood: review article. J Epilepsy Clin Neurophysiol. 2006;12:26–31.
Hara K, Ohta K, Miyajima M, et al. Mismatch negativity for speech sounds in temporal lobe epilepsy. Epilepsy Behav. 2012;23(3):335–41.
Báez-Martín MM, Morales-Chacón LM, García-Maeso I, et al. Temporal lobe epilepsy surgery modulates the activity of auditory pathway. Epilepsy Res. 2014;108(4):748–54.
Guimaraes CA, Li LM, Rzezak P, et al. Temporal lobe epilepsy in childhood: comprehensive neuropsychological assessment. J Child Neurol. 2007;22:836–40.
Triantafyllou NI, Zalonis I, Kokotis P, et al. Cognition in epilepsy: a multichannel event related potential (P300) study. Acta Neurol Scand. 1992;86:462–5.
Chen Y, Chi Chow J, Lee I. Comparison the cognitive effect of anti-epileptic drugs in seizure-free children with epilepsy before and after drug withdrawal. Epilepsy Res. 2001;44:65–70.
Aldenkamp AP, Arends J. The relative influence of epileptic EEG discharges, short nonconvulsive seizures and type of epilepsy on cognitive function. Epilepsia. 2004;45:54–63.
Nicolai J, Ebus S, Biemans DPLJJG, et al. The cognitive effects of interictal epileptiform EEG discharges and short non-convulsive epileptic seizure. Epilepsia. 2012;53(6):1051–9.
Hewedi KM, Mohamed WO, Mostafa AA, et al. Effect of interictal epileptiform EEG discharges on cognitive functions in epileptic children. Egyptian J Hos Med (The). 2018;72(8):5130–6.
Gotman J, Marciani MG. Electroencephalographic spiking activity, drug levels and seizure occurrence in epileptic patients. Ann Neurol. 1985;17:597–603.
Park SP, Kwon SH. Cognitive effects of antiepileptic drugs. J Clin Neurol. 2008;4(3):99–106.
Witt JA, Helmstaedter C. Monitoring the cognitive effects of antiepileptic pharmacotherapy—approaching the individual patient. Epilepsy Behav. 2013;26(3):450–6.
Meador KJ. Cognitive outcomes and predictive factors in epilepsy. Neurology. 2002;58(8 Suppl 5):S21-26.
Thompson PJ, Trimble MR. Sodium valproate and cognitive functioning in normal volunteers. Br J Clin Pharmacol. 1981;12:819–24.
Caravaglios G, Natalè E, Ferraro G, et al. Auditory event-related potentials (P300) in epileptic patients. Neurophysiol Clin. 2001;31:121–9.
Berg AT, Zelko FA, Levy SR, Testa FM. Age at onset of epilepsy, pharmacoresistance, and cognitive outcomes: a prospective cohort study. Neurology. 2012;79(13):1384–91.
Soysal A, Atakli D, Atay T, et al. Auditory event-related potentials (P300) in partial and generalized epileptic patients. Seizure. 1999;8:107–10.
Acknowledgements
We thank assistant professor Dr. Qasim Al-Mayah from the Research Medical Unit / College of Medicine/Al-Nahrain University for helping in statistical analysis.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All the authors have directly participated in the preparation of this manuscript and have approved the final version submitted. ‘AA’ clinically examined and referring epileptic patients. ‘LH’ did the EEG and P300 ERP tests. ‘FH’ and ‘LH’ drafted the manuscript. ‘AA’, ‘LH’, and ‘FH’ conceived the study and participated in its design and interpretation. All the authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Iraqi Board for Medical Specialization (Decision No. 291; Date 21/1/2021). Written consent for participation from all subjects was ensured.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hasan, L.A., Hamdan, F.B. & Al-Mahdawi, A. P300 event-related potentials in people with epilepsy: clinico-neurophysiologic study. Egypt J Neurol Psychiatry Neurosurg 59, 93 (2023). https://doi.org/10.1186/s41983-023-00700-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00700-z