
Abstract
Background
A wide variety of factors have been reported to influence stroke prognosis. Quality indicators serve as standards of care. The aim of this study is to assess the clinical and demographic characteristics of patients with stroke and to measure quality indicators in relation to stroke early outcome. We analyzed a prospective hospital-based data. All patients with acute stroke admitted to Kasr-al-ainy stroke unit over a 1-year period were included. Clinical variables and quality indicators were studied in relation to early outcome which was measured by both disability at discharge assessed by modified Rankin score (mRS) and in-hospital death.
Results
We studied 242 patients with acute stroke, 145 patients (59.9%) had poor outcome at discharge [mRS 3–6]. There were 36 (14.9%) in-hospital deaths. High mRS and National institute of health stroke scale (NIHSS) at stroke onset, low Gugging swallowing scale (GUSS) score and hypertension (HTN) were independent predictors for more disability on discharge. Chest infection, bed sores, high mRS at stroke onset and hemorrhagic transformation were independent predictors for in-hospital mortality. Receiving recombinant tissue plasminogen activator (rtPA) showed significant association with good outcome. Mean door to needle time (DNT) was 50.6 min. Low GUSS score was associated with increased risk of chest infection.
Conclusions
Stroke severity, potentially modifiable risk factors and complications are associated with an increased risk of poor early outcome. Dysphagia screening using GUSS scale can predict patients with higher risk of aspiration pneumonia after stroke. DNT needs to be improved.
Similar content being viewed by others

Background
After stroke, Clinicians are often asked to predict outcome by the patient, family, other healthcare workers, and insurance providers. A wide variety of factors have been reported to influence stroke prognosis, including age, stroke severity, stroke mechanism, infarct location, comorbid conditions, clinical findings, and related complications. In addition, interventions such as thrombolysis, stroke unit care, can play a major role in the outcome of stroke [1].
Clinical guidelines were written to promote diagnostic or therapeutic interventions applicable to the majority of patients in most circumstances. However, the use of guideline recommendations for individual patients has traditionally been left to the discretion of individual clinicians [2].
A recognized approach to assist the translation of research evidence into clinical practice is to monitor the key performance indicators (KPIs) which are standards of care implying that health care professionals are providing inadequate care if eligible patients do not receive that standard of care [2].
The mRS is a clinician-reported measure of global disability after stroke and used as a primary end point in randomized clinical trials (RCTs) of stroke treatments. Extensive evidence on the validity, reliability and sensitivity of the mRS exists across literature [3].
Determining an individual patient's risk of mortality at admission could aid clinical care by identifying those at high risk for poor outcomes who may require more intensive resources [4].
The aims of this study are measuring quality indicators together with identification of characteristics of stroke patients and the relation of both to early outcome of stroke units.
Methods
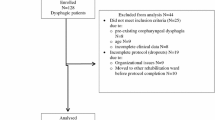
This was an observational prospective cohort hospital-based study involving all acute stroke patients (242) of both sexes aging above 12 years who were admitted to the stroke unit in Kasr-al-ainy hospital through 1 year from 1st of October 2019 to 30th of September 2020.
All Patients were subjected to medical history (including detailed history of possible stroke risk factors), neurological and neurovascular examination including dysphagia screening using GUSS scale [5], computed tomography (CT) brain using 16-slice CT scanner (Siemens, Somatom go.Top, Germany) and\or Magnetic resonance imaging (MRI) brain using MRI scanner (Philips, achieva 1.5T, Netherland), laboratory investigations including workup for stroke risk factors, Electrocardiogram(ECG) ± Echocardiography using ultrasound machine (Philips, HDI 5000, USA) ± Carotid and vertebrobasilar duplex ± transcranial duplex using ultrasound machine (philips, IU22, USA) ± CT angiography using the above mentioned CT scanner or Magnetic resonance angiography (MRA) using the above mentioned MRI scanner.
Clinical evaluation: we used Oxford community stroke project classification of clinically identifiable cerebral stroke subtypes to classify our patients [6]. Regarding stroke etiology: we used TOAST (trial of ORG 10172 in acute stroke treatment) classification [7] to classify ischemic patients. Regarding hemorrhagic stroke, it includes parenchymal hemorrhage, subarachnoid hemorrhage, intraventricular hemorrhage. Other etiological types include transient ischemic attack, sinus thrombosis and venous infarctions. NIHSS [8] and mRS [9] were used for assessment of stroke severity.
We have used a previously designed quality indicators to measure performance of management of stroke patients. We selected these indicators from last version of Get With The Guidelines (GWTG) Stroke, a performance improvement program for hospitals that use a stroke registry to support its aims [10].
Both mRS on discharge and in-hospital mortality were used to assess early stroke outcome. We grouped patients regarding mRS on discharge into 2 categories: good outcome: mRS 0–2 and poor outcome: mRS 3–6.
The association of demographics, clinical characteristics, complications, management and compliance to quality indicators with early outcome was assessed.
Data were coded and entered using the statistical package for the Social Sciences (SPSS) version 26. Data were summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage) for categorical data. Comparisons between quantitative variables were done using the non-parametric Kruskal–Wallis and Mann–Whitney tests for non-normally distributed date and t test for normally distributed data. For comparing categorical data, Chi square (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5. Multivariate logistic regression was done to detect independent predictors of mortality and bad mRS on discharge. P values less than 0.05 were considered as statistically significant.
The institutional review board of faculty of medicine, Cairo University approved this study. All methods were carried out in accordance with relevant guidelines and Declaration of Helsinki.
Results
Two hundred and forty-two acute stroke patients were enrolled in our study; out of them, 186 had ischemic stroke. Age of patients ranges from 25 to 87 years with mean of 59.3 ± 13.1, 155 (64%) were males, while 87 (36%) were females. The prevalence of stroke risk factors, stroke subtypes, etiology and complications are illustrated in Table 1.
Regarding stroke severity on admission, mRS ranged from 0 to 5 with mean of 3.5 ± 1, while NIHSS ranged from zero to 31 with a median of 10. Thirteen (5.4%) patients had NIHSS zero, 33 patients (13.6%) had minor stroke (NIHSS 1–4), 166 (68.6%) had moderate stroke (NIHSS 5–15) and 30 patients (12.4%) had severe stroke (NIHSS > 15).
Patients' hospital stays ranged from 1 day to 105 days, with a median of 8 days.
Regarding Quality indicators, out of 77 patients who arrived at the hospital within 4.5 h, 75 received rtPA, while two patients did not; one received low molecular weight heparin before presentation to us, while the other was subjected to mechanical thrombectomy directly. GUSS score was done for all patients on admission (n = 242), ranging 0 to 20 with a mean of 14.62 ± 7.1. It was done also for all patients on discharge apart from those who died at hospital (n = 206), ranging from 2 to 20 with a mean of 18.69 ± 3.8. Patients complicated with chest infection had significantly lower GUSS scores at stroke onset (median of 6, range from 0 to 20) compared to those not complicated with chest infection (median of 20, range from 0 to 20), P < 0.001. The mean onset-to-door time ranged from 60 to 230 min, with a median of 150 and a mean of 151.93 ± 45.43 min, while the mean door-to-needle time ranged from 20 to 60 min, with a median of 50 and a mean of 50.6 ± 9.04 min. Regarding onset-to-needle time, it ranged from 110 to 270 min, with a median of 210 and a mean of 202.5 ± 42.4 min. The mRS at discharge (including patients who died in hospital) ranged from 0 to 6 with a median of 3. Out of 242 patients, 36 died in hospital (14.9%) due to stroke and its complications. Other quality indicators are summarized in Table 2.
On comparing outcome groups depending on mRS on discharge; the presence of HTN, stroke complicated by chest infection, bed sores, or sepsis, posterior circulation infarct stroke, cardioembolic stroke, large artery stroke, not receiving rtPA, older age, higher NIHSS, and lower GUSS score on admission are significantly associated with bad mRS on discharge, as illustrated in Tables 3 and 4.
Results of multivariate logistic regression analysis for prediction of having bad mRS on discharge (utilizing significant variables in Tables 3 and 4) showed a significant regression, P < 0.001 and R2 = 0.38. The risk of having bad mRS on discharge is more than the double when the patient is hypertensive (OR = 2.6, CI 1.24–5.44, P value = 0.01). Similar results were found regarding lower GUSS on admission and higher both mRS on and NIHSS on admission (Table 5).
On comparing between patients discharged alive and dead groups: older age, posterior circulation infarction (POCI) stroke, cardio embolic stroke, large artery stroke, stroke complicated by hemorrhagic transformation, chest infection, bed sores or sepsis, admission in ICU, higher NIHSS and mRS and lower GUSS scores on admission are associated with higher in-hospital mortality, while small artery infarction was associated with lower mortality as shown in Tables 3 and 4.
Results of multivariate logistic regression analysis for prediction of in-hospital mortality (utilizing significant variables in Tables 3 and 4) showed a significant regression, P < 0.001 and R2 = 0.34. The risk of in-hospital mortality is more than seven times higher when the patient developed hemorrhagic transformation (OR = 7.39, CI 1.97–27.7, P value = 0.003). Similar results were found regarding chest infection, bed sores, mRS on admission (Table 5).
Discussion
The current study stated that advanced age correlates significantly with poor mRS on discharge and in-hospital mortality, but not an independent predictor of either in multivariate analysis. These findings are consistent with other studies, which stated that the association between age and early stroke disability and in-hospital mortality may be better explained by the coexistence of other factors, such as the severity of neurological impairment on admission [11,12,13]. However, other studies have found that age is a predictor for disability and mortality [14,15,16].The population of these studies is only of ischemic stroke.
In the present work, no statistically significant difference was found between males and females regarding mortality or disability. The existence of gender differences in stroke outcome is controversial in previous studies; some previous studies reported that females had worse functional outcome and more in-hospital mortality after stroke [14, 17, 18], while other studies have stated that male sex is associated with more in-hospital mortality [19, 20]. Some more studies argued that gender has no effect on stroke outcome [21,22,23].
The present results did not show any significant relation between any of the studied risk factors and outcome, except for hypertension which was associated with disability and found to be a predictor of it. This comes in agreement with previous studies [17, 24, 25]. Other studies have found that, in addition to hypertension, diabetes, atrial fibrillation, history of previous stroke, and ischemic heart disease are associated with an increased risk of poor outcome and mortality following stroke [14, 15, 26]. On the other hand, other studies have stated that the presence of common stroke risk factors was not associated with poor functional outcome or mortality [18, 27].
In our study, stroke initial clinical severity was significantly associated with disability and mortality; however, it was an independent predictor only for disability. Previous studies reported that stroke severity as measured by the NIHSS is an important factor determining outcome after stroke [1, 14] and predicting in-hospital mortality [17, 28]; these studies used NIHSS categorization in relation to mortality. The non-categorization of NIHSS in our study may explain why NIHSS is not a predictor for mortality.
The current work showed that large artery and cardioembolic strokes were associated with poorer mRS on discharge compared to other stroke subtypes; however, neither was an independent predictor for it. This agrees with previous studies [29, 30]. Other studies showed that they were associated with higher disability and in-hospital mortality [15, 26].
Our study showed that partial anterior circulation infarction (PACI) was associated with poorer mRS on discharge compared to other stroke subtypes, but was not an independent predictor for it. On the other hand, POCI was associated with significantly higher in-hospital mortality, while lacunar infarction (LACI) was associated with lower in-hospital mortality, but not an independent predictor for it. Previous studies had found similar results [12, 15, 28]. Other studies has reported no significant difference in outcome between anterior and posterior circulation strokes [22].
Medical and neurological complications occur after stroke and can affect outcome. Our study found that chest infection and bed sores were associated with poor outcome and were independent predictors for mortality. The same was found in previous studies [27, 28, 31]. On the other hand, another study has stated that post-stroke complications, including bronchopneumonia, urinary tract infection, bedsore, deep venous thrombosis, seizures, and others, were not associated with poor outcome at discharge. They considered all complications as one item and did not consider each as a separate entity. That could be an explanation for the discrepancy in results [32].
Regarding treatment with rtPA, our results showed that it is significantly associated with better outcomes regarding disability at discharge, but is not an independent predictor. Regarding in-hospital mortality, our results showed no significant difference between rtPA and non-rtPA treated patients. This come in agreement with other results [22, 27].
Moreover, our results showed that time to treatment (onset to treatment) was not significantly related to outcomes.rtPA was associated with better outcome in a time-dependent pattern, while mortality did not vary up to 4.5 h in one study [33]. In addition, treatment within 60 min, compared with treatment within 61 to 270 min, was associated with increased odds of discharge to home, independent ambulation at discharge, and freedom from disability (mRS 0–1) on discharge, without increased hemorrhagic complications or in-hospital mortality in another study [34].
In agreement with our results, one study found that early treatment with rtPA was not associated with an increased probability of having major neurologic improvement at 24 h after IV rt-PA administration. The mean time from symptom onset to treatment was 157 min (median 160 min). In the overall sample, only 4.1% of patients were treated within 90 min of stroke onset [35].
In our study, the mean onset to needle time was 202.5 min, and with more than half of the patients (58.7%) being injected after 3 h from stroke onset, this may explain the negative association between time to treatment and outcome in our study.
Our results showed that lower GUSS was significantly associated with disability, mortality, and developing chest infections. Moreover, in multivariate logistic regression, the GUSS score appears to be an independent predictor for disability. The same result was found in previous works [36, 37].
Conclusions
At the end of our discussion, we have to note that there is wide variability between studies regarding different variables in relation to stroke outcome. This could be explained the by different scores and variable systems used to evaluate the outcome, as well as the different used functional outcome measures among studies.
There were some limitations in this study. First, this study measured a very short-term outcome of acute stroke patients during hospital stay. A long-term study is required for further comments. Second, the study was conducted in a university hospital, which may include more severe and complicated stroke patients, and this may affect our results. Finally, a significant portion of our study occurred during the corona virus disease 2019(COVID-19) era which might affected the rate of patients admitted to the stroke unit and the quality of management.
We recommend including quality indicators as part of our stroke unit program to regularly assess our performance, so that we can improve it, which will have a beneficial effect on patients. Special attention should be taken to reduce "door to needle" time for intravenous thrombolysis. Dysphagia screening using a valid, reliable, and easy tool such as the GUSS scale is beneficial in predicting and thus preventing and managing aspiration pneumonia.
Availability of data and materials
The data sets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author on reasonable request.
Abbreviations
- mRS:
-
Modified Rankin scale
- NIHSS:
-
National institute of health stroke scale
- GUSS:
-
Gugging Swallowing Scale
- HTN:
-
Hypertension
- rtPA:
-
Recombinant tissue plasminogen activator
- DNT:
-
Door to needle
- KPIs:
-
Key performance indicators
- RCTs:
-
Randomized clinical trials
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- ECG:
-
Electrocardiogram
- MRA:
-
Magnetic resonance angiography
- TOAST:
-
Trial of ORG 10172 in acute stroke treatment
- GWTG:
-
Get With The Guidelines
- SPSS:
-
Statistical package for the Social Sciences
- REC:
-
Research Ethics Committee
- TACI:
-
Total anterior circulation infarction
- TACH:
-
Total anterior circulation hemorrhage
- PACI:
-
Partial anterior circulation infarction
- PACH:
-
Partial anterior circulation hemorrhage
- POCI:
-
Posterior circulation infarction
- POCH:
-
Posterior circulation hemorrhage
- LACI:
-
Lacunar infarction
- LACH:
-
Lacunar hemorrhage
- TIA:
-
Transient ischemic attack
- OCP:
-
Oral contraceptive pills
- CVS:
-
Cerebrovascular stroke
- UTI:
-
Urinary tract infection
- DVT:
-
Deep venous thrombosis
- SAH:
-
Sub arachnoid hemorrhage
- ICU:
-
Intensive care unit
- COVID-19:
-
Corona virus disease 2019
References
Wouters A, Nysten C, Thijs V, Lemmens R. Prediction of outcome in patients with acute ischemic stroke based on initial severity and improvement in the first 24 h. Front Neurol. 2018;9:308.
Urimubenshi G, Langhorne P, Cadilhac DA, Kagwiza JN, Wu O. Association between patient outcomes and key performance indicators of stroke care quality: a systematic review and meta-analysis. Eur Stroke J. 2017;2:287–307.
Broderick JP, Adeoye O, Elm J. Evolution of the modified rankin scale and its use in future stroke trials. Stroke. 2017;48:2007–12.
Herpich F, Rincon F. Management of acute ischemic stroke. Crit Care Med. 2020;48:1654–63.
Trapl M, Enderle P, Nowotny M, Teuschl Y, Matz K, Dachenhausen A, et al. Dysphagia bedside screening for acute-stroke patients: the Gugging Swallowing Screen. Stroke. 2007;38:2948–52.
Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet. 1991;337:1521–6.
Adams HP, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24:35–41.
Hinkle JL. Reliability and validity of the National Institutes of Health Stroke Scale for neuroscience nurses. Stroke. 2014;45:e32-34.
Banks JL, Marotta CA. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38:1091–6.
Howard G, Schwamm LH, Donnelly JP, Howard VJ, Jasne A, Smith EE, et al. Participation in get with the guidelines-stroke and its association with quality of care for stroke. JAMA Neurol. 2018;75:1331–7.
Sumer MM, Ozdemir I, Tascilar N. Predictors of outcome after acute ischemic stroke. Acta Neurol Scand. 2003;107:276–80.
Payabvash S, Benson JC, Tyan AE, Taleb S, McKinney AM. Multivariate prognostic model of acute stroke combining admission infarct location and symptom severity: a proof-of-concept study. J Stroke Cerebrovasc Dis. 2018;27:936–44.
Namale G, Kamacooko O, Makhoba A, Mugabi T, Ndagire M, Ssanyu P, et al. Predictors of 30-day and 90-day mortality among hemorrhagic and ischemic stroke patients in urban Uganda: a prospective hospital-based cohort study. BMC Cardiovasc Disord. 2020;20:442.
Qawasmeh MA, Aldabbour B, Momani A, Obiedat D, Alhayek K, Kofahi R, et al. Epidemiology, risk factors, and predictors of disability in a cohort of Jordanian patients with the first ischemic stroke. Stroke Res Treat. 2020;2020:1920583.
Gattringer T, Posekany A, Niederkorn K, Knoflach M, Poltrum B, Mutzenbach S, Austrian Stroke Unit Registry Collaborators, et al. Predicting Early Mortality of Acute Ischemic Stroke. Stroke. 2019;50:349–56.
Panni P, Gory B, Xie Y, Consoli A, Desilles JP, Mazighi M, ETIS (Endovascular Treatment in Ischemic Stroke) Investigators, et al. Acute stroke with large ischemic core treated by thrombectomy. Stroke. 2019;50:1164–71.
Koennecke HC, Belz W, Berfelde D, Endres M, Fitzek S, Hamilton F, et al. Factors influencing in-hospital mortality and morbidity in patients treated on a stroke unit. Neurology. 2011;77:965–72.
Irie F, Kamouchi M, Hata J, Matsuo R, Wakisaka Y, Kuroda J, FSR Investigators, et al. Sex differences in short-term outcomes after acute ischemic stroke: the Fukuoka stroke registry. Stroke. 2015;46:471–6.
Alhazzani AA, Mahfouz AA, Abolyazid AY, Awadalla NJ, Katramiz K, Faraheen A, et al. In Hospital stroke mortality: rates and determinants in southwestern Saudi Arabia. Int J Environ Res Public Health. 2018;15:927.
Irie F, Matsuo R, Nakamura K, Wakisaka Y, Ago T, Kamouchi M, Fukuoka Stroke Registry Investigators Sex, et al. Differences in the risk of 30-day death after acute ischemic stroke. Neurol Clin Pract. 2021;11:e809–16.
Jeng JS, Huang SJ, Tang SC, Yip PK. Predictors of survival and functional outcome in acute stroke patients admitted to the stroke intensive care unit. J Neurol Sci. 2008;270:60–6.
Wollenweber FA, Tiedt S, Alegiani A, Alber B, Bangard C, Berrouschot J, et al. Functional outcome following stroke thrombectomy in clinical practice. Stroke. 2019;50:2500–6.
Abdu H, Seyoum G. Sex differences in stroke risk factors, clinical profiles, and in-hospital outcomes among stroke patients admitted to the medical ward of Dessie comprehensive specialized hospital, Northeast Ethiopia. Degener Neurol Neuromuscul Dis. 2022;12:133–44.
Nayak AR, Shekhawat SD, Lande NH, Kawle AP, Kabra DP, Chandak NH, et al. Incidence and clinical outcome of patients with hypertensive acute ischemic stroke: an update from tertiary care center of Central India. Basic Clin Neurosci. 2016;7:351–60.
Admas M, Teshome M, Petrucka P, Telayneh AT, Alamirew NM. In-hospital mortality and its predictors among adult stroke patients admitted in Debre Markos Comprehensive Specialized Hospital, Northwest Ethiopia. SAGE Open Med. 2022;10:20503121221122464.
Russell JBW, Charles E, Conteh V, Lisk DR. Risk factors, clinical outcomes and predictors of stroke mortality in Sierra Leoneans: a retrospective hospital cohort study. Ann Med Surg. 2020;60:293–300.
Neshuku SN, Kirchner-Frankle J, Nangolo M, Moses M, Einbeck CO, Kumire P, et al. The burden and in-hospital mortality of stroke admissions at a tertiary level hospital in Namibia: a retrospective cohort study. Stroke Res Treat. 2023;2023:1978536.
Kortazar-Zubizarreta I, Pinedo-Brochado A, Azkune-Calle I, Aguirre-Larracoechea U, Gomez-Beldarrain M, Garcia-Monco JC. Predictors of in-hospital mortality after ischemic stroke: a prospective, single-center study. Health Sci Rep. 2019;2: e110.
Fuentes B, Martínez-Sánchez P, Alonso de Leciñana M, Egido J, Reig-Roselló G, Díaz-Otero F, et al. Efficacy of intravenous thrombolysis according to stroke subtypes: the Madrid Stroke Network data. Eur J Neurol. 2012;19:1568–74.
Mahmoud Fouad M, Mohamed Farag S, Hegazy MI, Abd Elalem Aziz M. Prediction of functional outcome in ischemic stroke patients: an observational study on Egyptian population. Cureus. 2017;9: e1392.
Ingeman A, Andersen G, Hundborg HH, Svendsen ML, Johnsen SP. In-hospital medical complications, length of stay, and mortality among stroke unit patients. Stroke. 2011;42:3214–8.
Mapoure NY, Tchaleu Nguenkam CB, Mbatchou Ngahane HB, Dzudie A, Coulibaly A, Mounjouopou NG, et al. Predictors of in-hospital mortality for stroke in Douala, Cameroon. Stroke Res Treat. 2014;2014: 681209.
Gumbinger C, Reuter B, Stock C, Sauer T, Wiethölter H, Bruder I, et al. Time to treatment with recombinant tissue plasminogen activator and outcome of stroke in clinical practice: retrospective analysis of hospital quality assurance data with comparison with results from randomised clinical trials. BMJ. 2014;348: g3429.
Kim JT, Fonarow GC, Smith EE, Reeves MJ, Navalkele DD, Grotta JC, et al. Treatment with tissue plasminogen activator in the golden hour and the shape of the 4.5-hour time-benefit curve in the National United States get with the guidelines-stroke population. Circulation. 2017;135:128–39.
Saposnik G, Di Legge S, Webster F, Hachinski V. Predictors of major neurologic improvement after thrombolysis in acute stroke. Neurology. 2005;65:1169–74.
Joundi RA, Martino R, Saposnik G, Giannakeas V, Fang J, Kapral MK. Predictors and outcomes of dysphagia screening after acute ischemic stroke. Stroke. 2017;48:900–6.
Dang PD, Nguyen MH, Mai XK, Pham DD, Dang MD, Nguyen DH, et al. A comparison of the national institutes of health stroke scale and the Gugging swallowing screen in predicting stroke-associated pneumonia. Ther Clin Risk Manag. 2020;16:445–50.
Acknowledgements
The authors would like to express their gratitude to the patients for their participation and cooperation in this study.
Funding
We did not receive any fund.
Author information
Authors and Affiliations
Contributions
MAZ was the idea founder, shared in the patient collection, and the supervisor in all the steps. AMA shared in the patient collection and supervision. HSM shared in the patient collection and supervision AAS shared in the patient collection, wrote and revised the manuscript. AMF did the data analysis, and he is the submitting and corresponding author. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate.
The institutional review board of faculty of medicine, Cairo University approved this study in 17-4-2018. Informed written consent was obtained from each participant or their relatives if they were unable to give the consent owing to their medical condition. All methods were carried out in accordance with relevant guidelines and Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Authors’ information
Maha Atef Zaki is a professor of neurology at Cairo University. Ahmed Mohamed Abdelalim is a professor of neurology at Cairo University. Husam Salah Mourad is a professor of neurology at Cairo University. Abdallah Adel Saad is an Assistant lecturer of neurology at Cairo University. Amr Mohamed Fouad is a lecturer of neurology at Cairo University.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zaki, M.A., Abdelalim, A.M., Mourad, H.S. et al. Quality indicators and patients' characteristics in relation to early outcome of Kasr-al-ainy stroke unit. Egypt J Neurol Psychiatry Neurosurg 59, 91 (2023). https://doi.org/10.1186/s41983-023-00691-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00691-x