
Abstract
Background
Due to its disturbance in schizophrenic patients, mismatch negativity (MMN) generation is believed to be a potential biomarker for recognizing primary impairments in auditory sensory processing during the course of the disease. However, great controversy exists regarding the type and onset of MMN-related impairments, with the deficits to frequency deviants is more debatable. This cross-sectional, case–control study was conducted to assess the cognitive functions among 33 eligible Egyptian schizophrenics (15 early and 18 chronic), and 30 matched healthy controls by assessing their psychometric tests and correlating them to the coexisting frequency deviant MMN responses (using both tone and speech stimuli).
Results
Deficits in frequency MMN and neuropsychological tests were evident among early and chronic schizophrenics compared to their matched control counterparts, and also between early versus chronic schizophrenia in favor of the later. MMN deficits to speech stimuli were more elicited than tone stimuli among schizophrenics. Moreover, significant correlations were identified between MMN parameters and the results of psychiatric cognitive scales.
Conclusions
We demonstrated that frequency-deviant MMN deficits are evident feature among the enrolled Egyptian schizophrenics. The cognitive functions as indexed by MMN seem affected early, with the striking decrease of MMN amplitude and delay of latency point towards the progression of the illness. The normal lateralization of MMN was absent in chronic schizophrenia. These findings could be helpful in using the MMN as an additional objective tool for confirming cognitive impairments among schizophrenics and to differentiate between early- and chronic-schizophrenic patients for medico-legal purposes and clinical implication for medications.
Similar content being viewed by others

Background
Schizophrenia is a complex functionally debilitating mental disorder, with diverse genetic and neuro-biological backgrounds, leading to deficits in the neural circuits that triggered psychotic symptoms by adolescence and early adulthood. Various theories have emerged in the pathogenesis of schizophrenia including neurodegenerative hypothesis, neurodevelopment theory, neurochemical imbalance, endocannabinoid system dysfunction, atypical mitochondrial dynamics, brain networks dysfunction, triggered immune system and inflammation [1,2,3,4,5,6,7].
Beside the clinical psychotic symptoms, cognitive impairment is a core feature of schizophrenia which is usually present at/or even predate the onset of illness and is closely linked to functional outcomes [8,9,10,11,12]. Psychometric testing is one of the commonly used methods to evaluate the cognitive functions in patients with psychosis [10, 13, 14], but factors such as test anxiety, dishonest candidate or untrained psychologist can create misjudgment and false negative results. There can be also minor discrepancies in psychometric reliability due to individual variation in feelings or thoughts at different times leading to variance in scores. For this reason, a wide spectrum of modern laboratory-, neurroimaging- and neurophysiological-biomarkers have been recently suggested as objective tools for early cognitive impairment of schizophrenia.
Among the emerged laboratory markers, disturbed serum/CSF levels of Kynurenines and pro-inflammatory cytokines have been detected in schizophrenics and were linked extensively to cognitive/psychiatric symptoms in first episode and chronic schizophrenia. However, the results across studies are divergent, as well, these biomarkers are greatly overlapping between cardiovascular, autoimmune and other neuropsychiatric diseases [5, 15,16,17]. Regarding the advanced neuro-imaging technology, diffusion tensor and functional magnetic resonance imaging (static and dynamic) offer a strong insight for detecting morphological and functional brain changes among schizophrenics, as altered white matter integrity was recognized and correlated with cognitive performance, such as poor processing speed, working memory, and executive functioning [18,19,20,21]. Nevertheless, beside the imaging’s high costs, there have also been conflicting findings, probably due to the wide heterogeneity across study populations and in the imaging methodologies applied.
MMN is another attractive, available, and cost-effective neurophysiological tool that has been introduced as a “breakthrough biomarker” indexing early auditory processing, generated by a fronto-temporal network associated with pre-attentive sensory processing, and has a vital role in establishing learning and memory [22,23,24,25,26]. It is evoked when a sequence of identical auditory stimuli is infrequently interrupted. This occurs by a deviated stimulus from the preceding standard ones along one or more dimensions, such as pitch, intensity, frequency, or duration [22,23,24,25,26]. In schizophrenic patients, it has been suggested that glutamate/N-methyl-D-aspartate (NMDA) system dysfunctions at this network could trigger MMN deficits [27, 28].
Although there is a growing evidence highlighting on MMN amplitude attenuation in schizophrenia, there is yet quite inconsistency among studies [29], with the frequency deviants MMN (fMMN), in particular, in early schizophrenia is more debatable. Whereas several studies [30,31,32] detected no fMMN deficits in early phases of psychosis, others [33,34,35,36], however, elicited evident early deficits.
MMN latency is measured by the time at which the deviant stimulus can be differentiated from the preceding standard one. Reviews of the MMN literature in schizophrenia do not underscore reliable latency dissimilarity between patients and matched controls. Some researchers reported prolonged latency [37,38,39], while others showed significant shortening [40,41,42].
Another point of controversy is related to the relation of MMN deficits to neuropsychological tests. It has become increasingly obvious over recent years that MMN deficits correlate significantly with impaired cognitive performance in schizophrenia, which, in turn, forecast limited functional outcomes [38, 43, 44]. On the other hand, Li and colleagues [39] pointed out the lack of close association between MMN indices and neuropsychological parameters. It is thus still unclear whether MMN deficits specify a stable trait of the illness, or if it follow a progressive course.
Owing to the aforementioned discrepant results, no conclusions can so far be universally outlined regarding the MMN-related issues in schizophrenia. Therefore, the current study was designed to assess selected psychiatric cognitive scales in a cohort of Egyptian schizophrenics and to verify whether is it possible to replicate the literature findings of MMN parameters (amplitude and latency) using speech and tone stimuli, and then to examine whether the underlying MMN impairments are connected exclusively with any cognitive domains among our schizophrenics. The literature pertaining the correlations between psychometric testing and MMN findings among the Egyptian schizophrenic population is scarce.
Methods
The current study was approved by the Research Ethics Committee of Tanta University on May 2019 with an approval code 32974/03/19. Sixty-three eligible subjects were enrolled in this cross-sectional, case–control study within 1 year after approval. Participants were divided into 2 main groups for analysis and comparison: Group I included 30 healthy control adults, while Group II included 33 adult schizophrenic patients who admitted to the Neuropsychiatry Department, Tanta University Hospitals and fulfilled the criteria of the Diagnostic and statistical manual of mental Disorders fifth edition (DSM-5) [45]. Patients (Group II) were subdivided into 2 subgroups according to the duration of illness: Subgroup (IIa) included 15 patients with early schizophrenia (duration of illness ≤ 2 years), while Subgroup (IIb) included 18 patients with chronic schizophrenia (duration of illness > 2 years). Control group (Group I) was also subdivided into 2 subgroups to match the above-mentioned patients' groups in their age and gender for comparison: subgroup (Ia) included 15 younger control participants and subgroup (Ib) included 15 older ones.
All participants in the present study were adults with bilateral normal peripheral hearing and bilateral normal middle ear functions which were prerequisites for the inclusion in this work. In addition, all patients were selected to be in remission or partial remission (not suffering from severe disruptive psychotic symptoms that compromised their communication), and had been taking their prescribed treatment regularly (on the same medical treatment for at least 1 month). Exclusion criteria included the followings: illiterates, elderly, participants not fitting the above-mentioned inclusion criteria, patients with other psychiatric disorders, history of psychotropic medications/electroconvulsive therapy in the previous 6 months, history of traumatic brain injury and existence of any serious medical condition that could affect cognitive function. Regarding controls, they were also excluded if they had: current or past history of mental disorders, neurological or general medical illnesses, or mental disorders in their first-degree relatives.
Psychiatric evaluation was conducted for all participants using the Arabic Version of Mini International Neuropsychiatric Interview for detailed history and mental state examination [46]. In addition, they all subjected to psychometric evaluation using the Arabic form of Mini-Mental state examination (MMSE) for measuring global cognition [47].Distinctive cognitive domains (attention, working memory, perceptual-motor and executive functions) were estimated by selective subtests of Wechsler Adult Intelligence Scale (WAIS-IV) in its Arabic version [48] including: Digit span (Ds), and Digit symbol (Dsy) scales as well as the Arabic form of Trail making test (TMT)[49].
Regarding the audiological assessment, all subjects of the current study were subjected to full audiological history taking, thorough otological examination and basic audiological assessment consisting of pure tone audiometry for the frequency range 250e8000 Hz and speech audiometry (using GSI-61 audiometer) and immittancemetry (using Zodiac-Madsen). MMN was carried out in the oddball paradigm using two kinds of stimuli (tone and speech) that were displayed in two paradigms. In the first paradigm, 1000 Hz and 1050 Hz were used as the standard and deviant stimuli, respectively, while in the second one, /da/ stimuli was used as a standard stimulus and /ga/stimuli was used as the deviant stimulus. The duration of tone and speech stimuli was approximately 150 ms and 200 ms, respectively. Both types of stimuli were presented at 1/s repetition rate, 15% deviant probability at 75 dB SPL using insert phone monaurally.
Once the test has been completed, offline manipulation of the traces was performed starting with N100 identification as the negativity occurring at about 80e120ms after stimulus presentation. MMN was measured in the difference waveform in accordance with manual specification of Smart-IHS. This was carried out by subtracting the traces occurring in response to both the deviant and the standard stimuli. MMN was identified visually as the most prominent negativity following N100 occurring between 150 and 300 ms. In each paradigm, both MMN parameters (latency and amplitude), were calculated.
Statistical analysis
All data were analyzed using the Statistical Package for Social Sciences (SPSS) version 21. Qualitative data were presented using number and percent, while the quantitative ones were displayed as mean and standard deviation (SD). Independent sample t test was applied for comparing two independent means. For categorical variables, Chi-square test was applied for analysis. Correlations between different variables were presented using Pearson correlation coefficients with p value < 0.05 was adopt as the level of significance. The sample size and power analysis was calculated using Epi-Info software statistical package created by World Health organization and center for Disease Control and Prevention, Atlanta, Georgia, USA version 2002. The sample size was calculated at N > 14 for each study-subgroup based on 95% confidence limit and 80% power of the study.
Results
In the present work the mean age of the younger controls (subgroup Ia) and the older controls (subgroup Ib) were 22.9 ± 3.6 years and 33.0 ± 3.1 years, respectively, that was matched with the age of early (subgroup IIa) and chronic (subgroup IIb) schizophrenic subgroups (24.1 ± 8.4 years and 33.9 ± 5.7 years, respectively). In comparing the disease duration between the 2 patients subgroups, the mean ± SD were 1.2 ± 0.3 and 17 ± 4.8 for early and chronic schizophrenic subgroups, respectively (P = 0.001).
Regarding the results of the investigated psychometric scales, there were statistically significant differences (p = 0.001) between early and chronic schizophrenic subgroups, as well as, between schizophrenics and their matched control counterparts, as shown in Table 1.
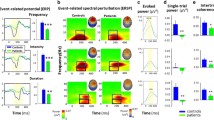
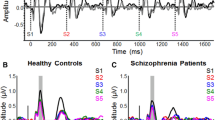
MMN responses were recorded in all subjects of control groups using both tone and speech stimuli (Fig. 1). Results of this work showed that 14 cases (93.3%) of the early schizophrenic subgroup (IIa) showed MMN response in both ears to both types of stimuli, while only one case showed no MMN response in both ears for the two stimuli (Fig. 2). MMN response in chronic schizophrenic subgroup was more absent when using speech stimuli than tone stimuli as the delectability of MMN response was 88.9% when using tone stimuli, while it was 72.2% on using speech stimuli (Fig. 3).

Traces of standard, deviant and MMN response using tone and speech stimuli of one of the controls

Abscece of N1 in one case of early schizophrenic patients

Presence of MMN response when using tone stimuli and their absence when using speech stimuli in chronic schizophrenic patient
Comparing the MMN latency responses between younger controls (Ia) and early schizophrenics (IIa), showed no statistically significant difference (P > 0.05) in both right and left ears after applying tone stimuli. Whereas on using speech stimuli, there was significant earlier latencies (p = 0.001) among subgroup Ia in MMN latency response in both ears. Regarding the MMN amplitude responses, comparison between the younger controls (Ia) and early schizophrenics (IIa) revealed significantly higher responses among the former in right and left ears when using both types of stimuli. The differences between all MMN parameters (latency and amplitude) in older control subgroup (Ib) and chronic schizophrenic subgroup (IIb) as well as between early (IIa) and chronic (IIb) schizophrenic subgroups when using both types of stimuli were statistically significant (p < 0.05) in both ears (Table 2). The latency was significantly delayed and the amplitude was lower in chronic schizophrenics in comparison to the older controls and also in early schizophrenics when using both types of stimuli (Table 2).
Comparing the MMN response parameters between right and left ears in the study demonstrated that the only significant difference was noticed in the amplitude as the MMN amplitude elicited by the right ears was higher than those of the left ones. When using tone stimuli, the results were significantly higher (P = 0.023) in the right ears in comparison to the left ears among control group and also in early schizophrenic subgroup only. On the other hand, when using speech stimuli, the results showed a significantly higher (P = 0.001) amplitude in the right ear in comparison to left ears only in chronic schizophrenic subgroup.
As regards to the correlations between the investigated psychometric tests and MMN results of the right and left ears among early schizophrenic patients, significant correlations were detected between MMN latency and each of MMSE and DS scores when using speech stimuli. In addition, there were significant correlations between these scores and MMN amplitude when using both types of stimuli (Table 3). Regarding the chronic schizophrenics, each of the MMSE, DS, and DSY scales revealed significant correlations with the elicited MMN parameters on using both types of stimuli in the right and left ears. As well, there was a negative correlation between duration of illness and MMN amplitude when using both types of stimuli in the right ear, while there was positive correlation between duration of illness and MMN latency when using tone stimuli only in the left ear (Table 4).
Discussion
One of the characteristic features of schizophrenia is the impairments across a broad array of cognitive domains, including both higher order tasks such as global cognitive functioning, memory, executive functions, attention, verbal fluency, learning and social cognition, as well as essential sensory functions such as auditory and visual processing [8,9,10,11,12,13,14, 50]. The interplay between these cognitive dysfunctions and poor motor functioning are the grounds of the diverse presentations of the illness as well as the impairment of daily living activity and social/occupational functioning [12, 51, 52].
Brain Morphological and functional studies indicated that different brain regions are implicated in schizophrenia-related cognitive dysfunctions including prefrontal cortex (associated with executive functioning), basal ganglia (reinforces behavior patterns), limbic system (implicated in learning, memory storage/recalling, and emotional processing), cerebellum (beside motor coordination, implicated in attention, working memory and sensory discrimination) and brainstem, with functional deterioration of the brain due to abnormal interactions between differentiated connecting networks [7, 21, 53, 54]. From the neuro-chemical viewpoint, the deregulations of dopaminergic, serotonergic, GABAergic and/or glutamatergic neurons reduce the effectiveness of context information and flexible updating of stored information (cognitive symptoms) [2].
MMN generation test has been acknowledged as one of the attractive, potential biomarkers of cognitive dysfunctions among schizophrenics. Deficits in MMN generation in schizophrenia are linked to impaired activation of superior temporal auditory cortex, prefrontal cortex and a salience network as well as other subcortical regions, such as inferior colliculus and thalamus [22, 23, 26, 55,56,57]. MMN deficits have been identified in patients with first-episode and chronic schizophrenia as well as in clinical high risk patients [58, 59]. Notably, MMN is obtained pre-attentively permitting the evaluation of auditory processing impairments in psychiatric disorders away from the confounding impact of motivation and attention related to higher order cognitive tasks [60].
The current research was conducted to evaluate the cognitive functions in patients with early and chronic schizophrenia using MMN (as elicited by tone and speech stimuli) and selected neuropsychological tests. Our findings revealed a statistically significant difference in psychometric MMSE scores between schizophrenic patients and their matched controls, and also between early and chronic schizophrenic subgroups. The current results are in agreement with previous researches [61, 62] that highlighted that MMSE is a valid tool to screen for cognitive impairment and to estimate the severity of cognitive changes overtime. The meta-analysis conducted by Maltais and his colleagues [62] has documented that the decline of MMSE scores in schizophrenics was proportional with the chronicity of illness.
Parallel to our findings, Perry and colleagues [63] found a significant difference between schizophrenics and healthy group in assessing of DS scores. Patients with schizophrenia had impairment of both the forward DS test as an indicator of the general attention, and the backward DS test for measuring the verbal working memory [64]. Working memory deficits in schizophrenia may have crucial implications both for the localization of underlying impairment and for explanations of different cognitive deficits associated with this disorder [65]. Our results also support the literature findings that processing speed, as measured by the Dsy test, is consider to be a critically impaired cognitive ability in schizophrenia [66]. Similarly, Reichenberg and Harvey [67] have advocated that the deficit in attention, processing speed, memory, working memory, and executive functions have all been always encountered in schizophrenia. This aspect is further underlined by the established correlations of processing speed with the risk of schizophrenia and the severity/disability of the illness [68, 69].
As regard to TMT scores, our findings were in line with a previous meta-analytic work [70] which approved similar deficits in the TMT results among patients with schizophrenia. As well, Toulopoulou and colleagues [71] reported that cognitive dysfunctions in schizophrenic patients appeared to be most severe in episodic memory and executive processes as assessed by TMT. In the present article, the impairment of different cognitive functions illustrated in the psychiatric scales supports the concomitant abnormal MMN responses in our included schizophrenic patients.
This study revealed a significantly prolonged MMN latency among early schizophrenic subgroup as compared to younger controls when using speech stimuli only. This agreed with the outcomes of other authors [35, 37,38,39] who demonstrated longer latencies among their early schizophrenics compared to controls on using speech and non-speech stimuli, whereas others [72] failed to find significant group differences, or else they [40,41,42] reported a shortened MMN latency in their patients. In one hand, prolonged latency may be expected to emerge from the compromised neuroanatomy and/or neurological function in schizophrenia. On the other hand, it is proposed that a shortened MMN latency in schizophrenia may reflect spontaneous, dysfunctional-premature stimulus processing [73]. Another speculation is that the diversity between the standard and deviant tone events may not precisely registered and their expression consequently largely overlapping [74]. Furthermore, the contradicted latency results may be allied to the discrepancy in many patient- and stimulus-related confounders across studies. Sampling differences regarding age of onset, IQ scoring, level of learning, and illness severity may explain these conflicting results. It may also be due to the dissimilarity between the specific sounds used in speech stimuli, as some speech stimuli were not cognitively taxing enough, and, therefore, not able to explain the subtle cognitive dysfunctions present early in schizophrenia. As well, a shorten MMN latency may be pronounced by applying complex multi-deviant stimuli, elevated stimulus magnitude/rate, and increased number of standards foregoing a deviant stimulus [75,76,77,78,79].
Our study showed a statistically significant difference in MMN amplitude between controls and early schizophrenic subgroup on using both types of stimuli in both ears. This was in agreement with the results of other researchers [59] who reported comparable findings when using tone stimuli. In the same line, previous studies [80, 81] have established a significant lower MMN amplitude in early schizophrenic patients compared to healthy controls. It can be speculated that the normal MMN declines over time in patients with schizophrenia, reflecting some ongoing neuro-chemical changes such as glutamate-mediated excitotoxic decrease of dendritic fields. This was also confirmed by Javitt and colleagues [82] who concluded that within 3 years of their first episode, schizophrenic patients had marginally diminished MMN to pitch deviants. In the contrary, Fisher and colleagues [83] did not get any statistically significant differences regarding the MMN parameters between early schizophrenic and their controls. This variation in the results between studies may be due to the difference in methodology and in the duration of illness between different series.
It is worth mentioning that MMN amplitude decrement among schizophrenics varies with the nature of stimulus deviance. Though the MMN decline to duration- and intensity-deviant tones have been detected from early stages of illness, those to frequency deviant tones may emerge with time during the course of the disease which thought to reflect illness chronicity [30,31,32, 84, 85]. However, this view is contradicted by our results as fMMN was elicited in both schizophrenic subgroups. Parallel to our findings, fMMN tones have been previously elicited among early schizophrenics, and even during the prodromal stage preceding psychosis onset [33,34,35,36, 86]. These controversies may be driven, at least partly, by the discrepancy in type of oddball paradigm and the types/characteristics of deviant stimuli applied to elicit MMN response, as different types of deviances may propagate at multiple levels of the neural axis (cortical versus subcortical). Individual variations may also play a crucial role in this regard. Furthermore, the heterogeneity between included schizophrenic samples and the method of recruiting the patients (inpatients versus outpatients) may also contribute to these conflicting results.
The chronic schizophrenic subgroup in the present study showed lower amplitude and longer latencies compared to their matched controls and also in comparison to early schizophrenic subgroup when using both types of stimuli. Parallel to these results, Horton [87] recognized that patients with chronic schizophrenia exhibited reduced amplitudes and longer latencies than controls to all frequency changes (5%, 10% and 20%). Moreover, other studies [23, 59, 83] reported significant reduction of MMN amplitude in chronic schizophrenics when compared to healthy control group and first episodic schizophrenics when using tone stimuli to fMMN and duration deviants MMN (dMMN). Our results, therefore, support the existence of a potential role of disease duration on simple auditory processing in patients with schizophrenia and is compatible with the glutamatergic dysfunction hypothesis [88]. The considerable difference in MMN decline between early and chronic schizophrenics may also be secondary to the impact of long-term neuroleptic medication. The noteworthy correlations between the duration of illness with each of the impaired MMN responses and worsen psychometric tests among our patients may indicate ongoing neuropathological changes in schizophrenia, which may support the neurodegenerative hypothesis of schizophrenia [1]; however, longitudinal studies will be more appropriate to confirm this issue.
Up till now, an extensive literature has built up regarding the MMN to pitch deviance and dMMN in schizophrenics and high risk patients relative to healthy controls. On the contrary, less data is existing regarding other deviant stimuli, in particular, frequency and location (the difference between both ears) MMN types. These stimuli depend chiefly upon accurate processing within midbrain regions and offer a quick and robust reorientation of attention. In the present study, the right ears had a statistically significant higher MMN amplitude than the left ears when using tone stimuli in early schizophrenic subgroup and also in their matched controls. This was concordant with the normal expected lateral distribution of MMN. This normal lateralization of MMN was absent in chronic schizophrenia after using tone stimuli. This coincided with previous studies that pointed to the long-term disturbed normal hemispheric asymmetry among schizophrenic populations [89].
Regarding the response to speech stimuli, the amplitude was significantly higher in right ears compared to left ones in chronic schizophrenic subgroup. This supports the findings of Razafimandimby and colleagues [90] who documented that in schizophrenics, the leftward functional language asymmetry indices were significantly decreased as compared to healthy controls. Consequently, these findings support Crow's hypothesis of a reduced hemispheric specialization in schizophrenics.
The results of our work showed that the MMN responses in chronic schizophrenic patients were more absent when using speech stimuli than tone stimuli (72.2% versus 88.9%, respectively). Besides, reduction of MMN amplitude was more observed in the former, with a significant difference in amplitude results in favor of the left ears. Moreover, latencies of MMN elicited by speech stimuli were longer than those elicited by tone ones. This might be related to the more complexity of speech syllables. There is a general concept that deficit in perceptual processing probably affects cognitive and social behavior. For example, difficulty in decoding modulation in speech can cause impaired social cognition owing to failure to understand emotional cues. Similarly, failure to parse perceptual objects into larger meaningful groups may undermine the cognition needed to navigate the social environment [91]. This supports our results which showed there were more deficits of MMN responses when using speech stimuli.
It is noteworthy that the relationship between neuropsychological tests and MMN latency has hardly ever been established in schizophrenia. In the current study, early schizophrenics displayed a statistically significant correlation between MMN latency and both psychometric MMSE and DS scores on using speech stimuli only. In addition, the reduction of MMN amplitude was correlated with worsen psychometric test-scores on using either types of stimuli. In the chronic schizophrenic subgroup, there was a positive correlation between MMN latency and illness duration on using tone stimuli in both ears. While on using speech stimuli there was positive correlation between MMN latency and duration of illness in right ears only. The MMN latency significantly increases and the amplitude decreases as MMSE, DS, Dsy and TMT scores worsen on using either type of stimuli. Our findings reveal that better neurophysiological test results, in the form of shorter latencies and higher amplitudes, are obtained with shorter duration of illness and better scores of cognitive scales (higher MMSE, DS, and Dsy, and lesser TMT scores).
The aforementioned results were in line with those obtained by prior researchers [42] who recognized an inverse correlation between MMN amplitude and duration of illness in patients with schizophrenia. They also studied the relation of fMMN and dMMN parameters and cognitive function in schizophrenia using neuropsychological test battery including TMT, Dsy and the DS. They found that MMN latency to fMMN was significantly correlated with neuropsychological tests. In addition, reduced MMN amplitude to fMMN was significantly correlated with a higher PANNS positive score in schizophrenics [38, 92]. Baldeweg and colleague [43] also delineated a significant association regarding the drop of MMN amplitude measures with duration deviant stimuli and several cognitive domains including verbal fluency, executive function and episodic memory. In the same line, Toyomaki and colleague [38] stated that tone dMMN deficits predict impairment of executive functioning in schizophrenia as represented by WCST, Stroop Test and TMT. Comparable findings have been replicated exclusively for selective cognitive domains, such as verbal fluency [93] and executive tasks [36]. Relations between MMN amplitude to duration deviants and measures of visual attention [94] and social cognition [95] have also been documented previously. More recently, Nakajima 2021 [44] shed light on the potential value of MMN amplitude as a biomarker for predicting symptomatic remission and upgrading of both cognitive and social abilities in first episode schizophrenia. However, the later-mentioned issues were not evaluated in our study.
The strength of the present research lies in its comparative nature; however, it has several limitations. One of them is the modest sample size, which could be attributed to the restricted selection criteria and limited study period. In addition, the study could be more informative if we could follow-up the cognitive functions and MMN responses among our schizophrenic cases. Another limitation was the lack of other comprehensive neuropsychological tests for precise assessment of cognitive abilities. However, such tests may be time-costly, not feasible and fatiguing for our patients. All the psychometric tests included in the present study depend on simple pen-and-paper tasks that are characterized by their briefness, easiness, and availability, which make them relatively tolerated by our schizophrenics and suitable to administrate in our busy university inpatient wards. As well, the selected tests could measure the different cognitive domains frequently affected in schizophrenics (as working memory, processing speed, attention, perceptual-motor and executive functions) making them potentially useful screening instruments for cognitive impairment in psychosis patients without the use of full-extensive battery.
An additional shortcoming of this work is that it did not include a measure for symptom severity of psychosis (such as PANSS). Nevertheless, our patients were selected to be stable inpatients (in remission or partial remission), had been taking their prescribed treatment regularly (for at least 1 month) and were not suffering from any serious disruptive symptoms that compromised their communication.
Future longitudinal multicentre studies using MMN to evaluate the auditory discrimination on a larger scale of schizophrenic patients, taking into consideration the symptom severity as a potential variable that could affect the patient's cognition while performing the tests, is strongly recommended to confirm the findings of this study. We also recommend conducting future studies pertaining MMN to evaluate the auditory working memory in schizophrenics treated with different medications.
Conclusions
This study replicates the literature evidence of reduced MMN amplitude and prolonged latency with regard to fMMN in a sample of schizophrenic Egyptian population, independent of early or chronic stages, with the deficits to speech stimuli are more elicited than to tone ones. Relating them to psychometric measures, more disturbed MMN responses were significantly associated with more severe cognitive decline, which reinforces the utility of MMN as a pre-attentive index of early auditory discrimination processing across the course of illness. The hallmark finding among our chronic schizophrenics is the absence of the normal lateralization of MMN when using tone stimuli. Therefore, our findings highlighted the value of using MMN as a supplementary objective tool, added to the conventional clinical psychiatric judgment, for early identification of cognitive impairments among schizophrenics, which may have the potential to limit substantial illness morbidity. This may also be helpful for the differentiation between early and chronic schizophrenia in favor of medico-legal purposes and clinical implication. This could aid in planning for precise therapeutic interventions and revealing functional improvements after cognitive therapy.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author, [Abeer Mamdouh Ali Mahmoud], upon reasonable request.
Abbreviations
- MMN:
-
Mismatch negativity
- DSM-5:
-
Diagnostic and statistical manual of mental disorders-fifth edition
- MMSE:
-
Mini-mental state examination
- WAIS-IV:
-
Wechsler Adult Intelligence Scale-fourth edition
- DS:
-
Digit span
- Dys:
-
Digit symbol
- TMT:
-
Trail making test
- fMMN:
-
Frequency deviant mismatch negativity
- dMMN:
-
Duration deviant mismatch negativity
References
Rund BR. Is schizophrenia a neurodegenerative disorder? Nord J Psychiatry. 2009;63(3):196–201.
Nikolaus S, Hautzel H, Müller HW. Neurochemical dysfunction in treated and nontreated schizophrenia—a retrospective analysis of in vivo imaging studies. Rev Neurosci. 2014;25(1):25–96.
Manseau MW, Goff DC. Cannabinoids and schizophrenia: risks and therapeutic potential. Neurotherapeutics. 2015;12(4):816–24.
Okusaga O, Fuchs D, Reeves G, Giegling I, Hartmann AM, Konte B, et al. Kynurenine and tryptophan levels in patients with schizophrenia and elevated antigliadin immunoglobulin G antibodies. Psychosom Med. 2016;78(8):931–9.
Tanaka M, Toldi J, Vécsei L. Exploring the etiological links behind neurodegenerative diseases: inflammatory cytokines and bioactive kynurenines. Int J Mol Sci. 2020;21(7):2431.
Tanaka M, Szabó Á, Spekker E, Polyák H, Tóth F, Vécsei L. Mitochondrial impairment: a common motif in neuropsychiatric presentation? The link to the tryptophan-kynurenine metabolic system. Cells. 2022;11(16):2607.
van den Heuvel MP, Fornito A. Brain networks in schizophrenia. Neuropsychol Rev. 2014;24(1):32–48.
Elvevåg B, Goldberg TE. Cognitive impairment in schizophrenia is the core of the disorder. Crit Rev Neurobiol. 2000;14(1):1–21.
Green MF, Kern RS, Heaton RK. Longitudinal studies of cognition and functional outcome in schizophrenia: implications for MATRICS. Schizophr Res. 2004;72(1):41–51.
Frommann I, Pukrop R, Brinkmeyer J, Bechdolf A, Ruhrmann S, Berning J, Decker P, Riedel M, Möller HJ, Wölwer W, Gaebel W, Klosterkötter J, Maier W, Wagner M. Neuropsychological profiles in different at-risk states of psychosis: executive control impairment in the early–and additional memory dysfunction in the late–prodromal state. Schizophr Bull. 2011;37(4):861–73.
Green MF, Horan WP, Lee J. Nonsocial and social cognition in schizophrenia: current evidence and future directions. World Psychiatry. 2019;18(2):146–61.
Harvey PD, Isner EC. Cognition, social cognition, and functional capacity in early-onset schizophrenia. Child Adolesc Psychiatr Clin N Am. 2020;29(1):171–82.
Lin YT, Liu CM, Chiu MJ, Liu CC, Chien YL, Hwang TJ, et al. Differentiation of schizophrenia patients from healthy subjects by mismatch negativity and neuropsychological tests. PLoS ONE. 2012;7(4): e34454.
Schulz SC, Murray A. Assessing cognitive impairment in patients with schizophrenia. J Clin Psychiatry. 2016;77(Suppl 2):3–7.
Wang AK, Miller BJ. Meta-analysis of cerebrospinal fluid cytokine and tryptophan catabolite alterations in psychiatric patients: comparisons between schizophrenia, bipolar disorder, and depression. Schizophr Bull. 2018;44(1):75–83.
Tanaka M, Tóth F, Polyák H, Szabó Á, Mándi Y, Vécsei L. Immune influencers in action: metabolites and enzymes of the tryptophan-kynurenine metabolic pathway. Biomedicines. 2021;9(7):734.
Koola MM, Raines JK, Hamilton RG, McMahon RP. Can anti-inflammatory medications improve symptoms and reduce mortality in schizophrenia? Curr Psychiatr. 2016;15(5):52–7.
Penadés R, Franck N, González-Vallespí L, Dekerle M. Neuroimaging studies of cognitive function in schizophrenia. Adv Exp Med Biol. 2019;1118:117–34.
Yang M, Gao S, Zhang X. Cognitive deficits and white matter abnormalities in never-treated first-episode schizophrenia. Transl Psychiatry. 2020;10(1):368.
Holleran L, Kelly S, Alloza C, Agartz BI, Andreassen OA, Arango C, et al. The relationship between white matter microstructure and general cognitive ability in patients with schizophrenia and healthy participants in the ENIGMA consortium. Am J Psychiatry. 2020;177(6):537–47.
Nyatega CO, Qiang L, Adamu MJ, Younis A, Kawuwa HB. Altered dynamic functional connectivity of cuneus in schizophrenia patients: a resting-state fMRI study. Appl Sci. 2021;11(23):11392.
Light GA, Swerdlow NR, Thomas ML, Calkins ME, Green MF, Greenwood TA, et al. Validation of mismatch negativity and P3a for use in multi-site studies of schizophrenia: characterization of demographic, clinical, cognitive, and functional correlates in COGS-2. Schizophr Res. 2015;163(1–3):63–72.
Erickson MA, Ruffle A, Gold JM. A meta-analysis of mismatch negativity in schizophrenia: from clinical risk to disease specificity and progression. Biol Psychiatry. 2016;79(12):980–7.
Vinogradov S, Nagarajan S. Association of sensory processing with higher-order cognition and functioning in schizophrenia: mapping the world. JAMA Psychiat. 2017;74(1):17–8.
Joshi YB, Breitenstein B, Tarasenko M, Thomas ML, Chang WL, Sprock J, Sharp RF, Light GA. Mismatch negativity impairment is associated with deficits in identifying real-world environmental sounds in schizophrenia. Schizophr Res. 2018;191:5–9.
Garrido MI, Kilner JM, Stephan KE, Friston KJ. The mismatch negativity: a review of underlying mechanisms. Clin Neurophysiol. 2009;120(3):453–63.
Michie PT, Malmierca MS, Harms L, Todd J. The neurobiology of MMN and implications for schizophrenia. Biol Psychol. 2016;116:90–7.
Avissar M, Javitt D. Mismatch negativity: a simple and useful biomarker of N-methyl-d-aspartate receptor (NMDAR)-type glutamate dysfunction in schizophrenia. Schizophr Res. 2018;191:1–4.
Umbricht D, Krljes S. Mismatch negativity in schizophrenia: a meta-analysis. Schizophr Res. 2005;76(1):1–23.
Näätänen R, Kähkönen S. Central auditory dysfunction in schizophrenia as revealed by the mismatch negativity (MMN) and its magnetic equivalent MMNm: a review. Int J Neuropsychopharmacol. 2009;12(1):125–35.
Bodatsch M, Ruhrmann S, Wagner M, Müller R, Schultze-Lutter F, Frommann I, et al. Prediction of psychosis by mismatch negativity. Biol Psychiatry. 2011;69(10):959–66.
Nagai T, Tada M, Kirihara K, Araki T, Jinde S, Kasai K. Mismatch negativity as a “translatable” brain marker toward early intervention for psychosis: a review. Front Psychiatry. 2013;23(4):115.
Nagai T, Tada M, Kirihara K, Yahata N, Hashimoto R, Araki T, et al. Auditory mismatch negativity and P3a in response to duration and frequency changes in the early stages of psychosis. Schizophr Res. 2013;150(2–3):547–54.
Perez VB, Woods SW, Roach BJ, Ford JM, McGlashan TH, Srihari VH, et al. Automatic auditory processing deficits in schizophrenia and clinical high-risk patients: forecasting psychosis risk with mismatch negativity. Biol Psychiatry. 2014;75(6):459–69.
Hay RA, Roach BJ, Srihari VH, Woods SW, Ford JM, Mathalon DH. Equivalent mismatch negativity deficits across deviant types in early illness schizophrenia-spectrum patients. Biol Psychol. 2015;105:130–7.
Rydkjær J, Møllegaard Jepsen JR, Pagsberg AK, Fagerlund B, Glenthøj BY, Oranje B. Mismatch negativity and P3a amplitude in young adolescents with first-episode psychosis: a comparison with ADHD. Psychol Med. 2017;47(2):377–88.
Kathmann N, Wagner M, Rendtorff N, Engel RR. Delayed peak latency of the mismatch negativity in schizophrenics and alcoholics. Biol Psychiatry. 1995;37(10):754–7.
Toyomaki A, Kusumi I, Matsuyama T, Kako Y, Ito K, Koyama T. Tone duration mismatch negativity deficits predict impairment of executive function in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(1):95–9.
Li Z, Zheng B, Deng W, Liu X, Zheng Z, Li T. Multi-components of evoked-brain potentials in deficit and nondeficit schizophrenia. Asia Pac Psychiatry. 2013;5(2):69–79.
Horton J, Millar A, Labelle A, Knott VJ. MMN responsivity to manipulations of frequency and duration deviants in chronic, clozapine-treated schizophrenia patients. Schizophr Res. 2011;126(1–3):202–11.
Domján N, Csifcsák G, Drótos G, Janka Z, Szendi I. Different patterns of auditory information processing deficits in chronic schizophrenia and bipolar disorder with psychotic features. Schizophr Res. 2012;139(1–3):253–9.
Kärgel C, Sartory G, Kariofillis D, Wiltfang J, Müller BW. Mismatch negativity latency and cognitive function in schizophrenia. PLoS ONE. 2014;9(4): e84536.
Baldeweg T, Klugman A, Gruzelier J, Hirsch SR. Mismatch negativity potentials and cognitive impairment in schizophrenia. Schizophr Res. 2004;69(2–3):203–17.
Nakajima S, Higuchi Y, Tateno T, Sasabayashi D, Mizukami Y, Nishiyama S, Takahashi T, Suzuki M. Duration mismatch negativity predicts remission in first-episode schizophrenia patients. Front Psychiatry. 2021;25(12): 777378.
Association AP. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Publishing; 2013.
Sadek A. Mini international neuropsychiatric interview (MINI): the Arabic translation. Psychiatry Update, Institute of Psychiatry. 2000; 2:23–31
Albanna M, Yehya A, Khairi A, Dafeeah E, Elhadi A, Rezgui L, et al. Validation and cultural adaptation of the Arabic versions of the mini-mental status examination-2 and mini-cog test. Neuropsychiatr Dis Treat. 2017;13:793–801.
Abdelhamid GSM, Gómez-Benito J, Abdeltawwab ATM, Abu Bakr MHS, Kazem AM. Hierarchical structure of the wechsler adult intelligence scale–fourth edition with an Egyptian sample. J Psychoeduc Assess. 2019;37(3):395–404.
Stanczak DE, Stanczak EM, Awadalla AW. Development and initial validation of an Arabic version of the Expanded Trail Making Test: implications for cross-cultural assessment. Arch Clin Neuropsychol. 2001;16(2):141–9.
Guo JY, Ragland JD, Carter CS. Memory and cognition in schizophrenia. Mol Psychiatry. 2019;24(5):633–42.
Lepage M, Bodnar M, Bowie CR. Neurocognition: clinical and functional outcomes in schizophrenia. Can J Psychiatry. 2014;59(1):5–12.
Kar SK, Jain M. Current understandings about cognition and the neurobiological correlates in schizophrenia. J Neurosci Rural Pract. 2016;7:412–8.
Andreasen NC, Pierson R. The role of the cerebellum in schizophrenia. Biol Psychiatry. 2008;64(2):81–8.
Burke T, Gleeson C, Holleran L, Mothersill D, Holland J, Costello L, et al. Corpus callosum microstructural tract integrity relates to longer emotion recognition reaction time in people with schizophrenia. Brain Sci. 2022;12(9):1208.
Cacciaglia R, Escera C, Slabu L, Grimm S, Sanjuán A, Ventura-Campos N, et al. Involvement of the human midbrain and thalamus in auditory deviance detection. Neuropsychologia. 2015;68:51–8.
Gaebler AJ, Mathiak K, Koten JW Jr, König AA, Koush Y, Weyer D, et al. Auditory mismatch impairments are characterized by core neural dysfunctions in schizophrenia. Brain. 2015;138(Pt 5):1410–23.
Näätänen R, Paavilainen P, Rinne T, Alho K. The mismatch negativity (MMN) in basic research of central auditory processing: a review. Clin Neurophysiol. 2007;118(12):2544–90.
Näätänen R, Todd J, Schall U. Mismatch negativity (MMN) as biomarker predicting psychosis in clinically at-risk individuals. Biol Psychol. 2016;116:36–40.
Xiong YB, Bo QJ, Wang CM, Tian Q, Liu Y, Wang CY. Differential of frequency and duration mismatch negativity and theta power deficits in first-episode and chronic schizophrenia. Front Behav Neurosci. 2019;6(13):37.
Mathalon DH, Ford JM. Divergent approaches converge on frontal lobe dysfunction in schizophrenia. Am J Psychiatry. 2008;165(8):944–8.
Pangman VC, Sloan J, Guse L. An examination of psychometric properties of the mini-mental state examination and the standardized mini-mental state examination: implications for clinical practice. Appl Nurs Res. 2000;13(4):209–13.
Maltais JR, Gagnon G, Garant MP, Trudel JF. Correlation between age and MMSE in schizophrenia. Int Psychogeriatr. 2015;27(11):1769–75.
Perry Y, Henry JD, Grisham JR. The habitual use of emotion regulation strategies in schizophrenia. Br J Clin Psychol. 2011;50(2):217–22.
Conklin HM, Curtis CE, Katsanis J, Iacono WG. Verbal working memory impairment in schizophrenia patients and their first-degree relatives: evidence from the digit span task. Am J Psychiatry. 2000;157(2):275–7.
Goldman-Rakic PS, Selemon LD. Functional and anatomical aspects of prefrontal pathology in schizophrenia. Schizophr Bull. 1997;23(3):437–58.
Knowles EE, David AS, Reichenberg A. Processing speed deficits in schizophrenia: reexamining the evidence. Am J Psychiatry. 2010;167(7):828–35.
Reichenberg A, Harvey PD. Neuropsychological impairments in schizophrenia: integration of performance-based and brain imaging findings. Psychol Bull. 2007;133(5):833–58.
Reichenberg A, Caspi A, Harrington H, Houts R, Keefe RS, Murray RM, et al. Static and dynamic cognitive deficits in childhood preceding adult schizophrenia: a 30-year study. Am J Psychiatry. 2010;167(2):160–9.
Brekke JS, Hoe M, Long J, Green MF. How neurocognition and social cognition influence functional change during community-based psychosocial rehabilitation for individuals with schizophrenia. Schizophr Bull. 2007;33(5):1247–56.
Sitskoorn MM, Aleman A, Ebisch SJ, Appels MC, Kahn RS. Cognitive deficits in relatives of patients with schizophrenia: a meta-analysis. Schizophr Res. 2004;71(2–3):285–95.
Toulopoulou T, Goldberg TE, Mesa IR, Picchioni M, Rijsdijk F, Stahl D, et al. Impaired intellect and memory: a missing link between genetic risk and schizophrenia? Arch Gen Psychiatry. 2010;67(9):905–13.
Magno E, Yeap S, Thakore JH, Garavan H, De Sanctis P, Foxe JJ. Are auditory-evoked frequency and duration mismatch negativity deficits endophenotypic for schizophrenia? High-density electrical mapping in clinically unaffected first-degree relatives and first-episode and chronic schizophrenia. Biol Psychiatry. 2008;64(5):385–91.
Grzella I, Müller BW, Oades RD, Bender S, Schall U, Zerbin D, et al. Novelty-elicited mismatch negativity in patients with schizophrenia on admission and discharge. J Psychiatry Neurosci. 2001;26(3):235–46.
Todd J, Michie PT, Schall U, Ward PB, Catts SV. Mismatch negativity (MMN) reduction in schizophrenia-impaired prediction–error generation, estimation or salience? Int J Psychophysiol. 2012;83(2):222–31.
Tiitinen H, May P, Näätänen R. The transient 40-Hz response, mismatch negativity, and attentional processes in humans. Prog Neuropsychopharmacol Biol Psychiatry. 1997;21(5):751–71.
Oades RD, Wild-Wall N, Juran SA, Sachsse J, Oknina LB, Röpcke B. Auditory change detection in schizophrenia: sources of activity, related neuropsychological function and symptoms in patients with a first episode in adolescence, and patients 14 years after an adolescent illness-onset. BMC Psychiatry. 2006;8(6):7.
Jakoby H, Goldstein A, Faust M. Electrophysiological correlates of speech perception mechanisms and individual differences in second language attainment. Psychophysiology. 2011;48(11):1517–31.
De Pascalis V, Varriale V. Intelligence and information processing: A mismatch negativity analysis using a passive auditory backward-masking task. J INDIVID DIFFER. 2012;33(2):101–8.
Haigh SM, Coffman BA, Murphy TK, Butera CD, Salisbury DF. Abnormal auditory pattern perception in schizophrenia. Schizophr Res. 2016;176(2–3):473–9.
Oranje B, Aggernaes B, Rasmussen H, Ebdrup BH, Glenthøj BY. Selective attention and mismatch negativity in antipsychotic-naïve, first-episode schizophrenia patients before and after 6 months of antipsychotic monotherapy. Psychol Med. 2017;47(12):2155–65.
Olney JW, Farber NB, Wozniak DF, Jevtovic-Todorovic V, Ikonomidou C. Environmental agents that have the potential to trigger massive apoptotic neurodegeneration in the developing brain. Environ Health Perspect. 2000;108(Suppl 3):383–8.
Javitt DC, Shelley AM, Silipo G, Lieberman JA. Deficits in auditory and visual context-dependent processing in schizophrenia: defining the pattern. Arch Gen Psychiatry. 2000;57(12):1131–7.
Fisher DJ, Rudolph ED, Ells EML, Knott VJ, Labelle A, Tibbo PG. Mismatch negativity-indexed auditory change detection of speech sounds in early and chronic schizophrenia. Psychiatry Res Neuroimaging. 2019;30(287):1–9.
Todd J, Michie PT, Schall U, Karayanidis F, Yabe H, Näätänen R. Deviant matters: duration, frequency, and intensity deviants reveal different patterns of mismatch negativity reduction in early and late schizophrenia. Biol Psychiatry. 2008;63(1):58–64.
Salisbury DF, Kuroki N, Kasai K, Shenton ME, McCarley RW. Progressive and interrelated functional and structural evidence of post-onset brain reduction in schizophrenia. Arch Gen Psychiatry. 2007;64(5):521–9.
Oknina LB, Wild-Wall N, Oades RD, Juran SA, Röpcke B, Pfueller U, et al. Frontal and temporal sources of mismatch negativity in healthy controls, patients at onset of schizophrenia in adolescence and others at 15 years after onset. Schizophr Res. 2005;76(1):25–41.
Horton HK. Linguistic ability and mental health outcomes among deaf people with schizophrenia. J Nerv Ment Dis. 2010;198(9):634–42.
Harms L, Fulham WR, Todd J, Meehan C, Schall U, Hodgson DM, et al. Late deviance detection in rats is reduced, while early deviance detection is augmented by the NMDA receptor antagonist MK-801. Schizophr Res. 2018;191:43–50.
Youn T, Park HJ, Kim JJ, Kim MS, Kwon JS. Altered hemispheric asymmetry and positive symptoms in schizophrenia: equivalent current dipole of auditory mismatch negativity. Schizophr Res. 2003;59(2–3):253–60.
Razafimandimby A, Maïza O, Hervé PY, Lecardeur L, Delamillieure P, Brazo P, et al. Stability of functional language lateralization over time in schizophrenia patients. Schizophr Res. 2007;94(1–3):197–206.
Javitt DC. When doors of perception close: bottom-up models of disrupted cognition in schizophrenia. Annu Rev Clin Psychol. 2009;5:249–75.
Kawakubo Y, Kamio S, Nose T, Iwanami A, Nakagome K, Fukuda M, et al. Phonetic mismatch negativity predicts social skills acquisition in schizophrenia. Psychiatry Res. 2007;152(2–3):261–5.
Higuchi Y, Sumiyoshi T, Seo T, Miyanishi T, Kawasaki Y, Suzuki M. Mismatch negativity and cognitive performance for the prediction of psychosis in subjects with at-risk mental state. PLoS ONE. 2013;8(1): e54080.
Hermens DF, Ward PB, Hodge MA, Kaur M, Naismith SL, Hickie IB. Impaired MMN/P3a complex in first-episode psychosis: cognitive and psychosocial associations. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(6):822–9.
Wynn JK, Sugar C, Horan WP, Kern R, Green MF. Mismatch negativity, social cognition, and functioning in schizophrenia patients. Biol Psychiatry. 2010;67(10):940–7.
Acknowledgements
All authors thank the staff members of Tanta University Audio-Vestibular unit and neuropsychiatry centre for their support and help in this study.
Funding
The research was self-funded, and no grants were obtained.
Author information
Authors and Affiliations
Contributions
AM: contributed to collection and interpretation of the data, statistical analysis of the results, drafting of the work, references collection, and writing of the manuscript. ME: participated in the study's design, psychiatric data interpretation, manuscript revision. MK: participated in the study's design, material preparation, audiological data interpretation, references collection, manuscript writing. RA: participated in the study's design, material preparation, patients' psychometric assessment, reference collection, manuscript writing. EK: Conception and design of the work, interpretation of data and critical revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study has been approved by The Research Ethical Committee and Quality Assurance Unit, Faculty of Medicine, Tanta on May 2019 with an approval code 32974/03/19 and with the Helsinki Declaration. Informed consent was obtained from all patients before contribution to this study.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mahmoud, A.M.A., Eissa, M.AE., Kolkaila, E.A. et al. Mismatch negativity as an early biomarker of cognitive impairment in schizophrenia. Egypt J Neurol Psychiatry Neurosurg 59, 24 (2023). https://doi.org/10.1186/s41983-023-00627-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00627-5