
Abstract
Background
Stroke is a neurological disorder resulting from a sudden decline in blood flow to a localized area of the brain. It is the second most common cause of death and the third most common cause of disability worldwide. Quality of life (QOL) is increasingly being used as an outcome measure designed to evaluate the quality of care for patients with stroke.
Objective
The study aims to assess the quality of life of cerebrovascular stroke patients in Alexandria, Egypt.
Methods
A descriptive crossover study was held on 80 adult cerebrovascular stroke patients admitted to the stroke unit at (Elhadra) University Hospital, Neuropsychiatry Department, and the outpatient clinics at the Main University Hospital.
Result
The main result of study revealed that there was a highly significant relation between socio-demographic characteristics and the patient’s quality of life (QOL), especially age, employment status, and the monthly income, the overall QOL (P < 0.05).
Recommendation
The study recommended that design health education program to raise stroke patient QOL, design program to improve care giver attitude toward stroke patient, collaborative efforts among the governmental agencies to improve the educational level of the citizens, further studies to examine QOL on larger group of patients to generalize the results.
Similar content being viewed by others

Introduction
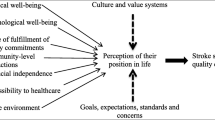
QOL is an important aspect of health outcome, along with duration of life, and it is of interest as a determinant of outcome as well. Reduction of life quality was reported even in patients with minimal consequences of stroke [1, 2].
Primary stroke prevention is focused mainly on control of the blood pressure (hypertension) as high blood pressure is a major stroke risk factor if left untreated. Also, smoking, and high cholesterol levels double the risk of stroke as it damages blood vessel walls, speed up artery clogging and raise blood pressure. Stroke risk could be increased by 500% because of atrial fibrillation (AF) [3, 4]. Reducing alcohol consumption, obesity as well as regular physical exercise are recommended both for prevention and in the recovery in the post stroke period [5, 6].
The role of the health care provider, especially the nursing team, is to be aware that stroke may lead to limitations in mobility such as requiring a wheelchair, communication difficulties, or functional disability to perform the activities of daily living, including self-care. Individually, the physical and social dimensions of stroke are central to the production of individuals’ suffering [7].
Nurses usually outnumber other health professionals and play a critical role in providing health care not only in traditional settings such as hospitals and long-term care institutions, but also increasingly in home care settings and primary care especially for the chronically ill [8]. Therefore, there is a felt need to assess QOL of patients with cerebrovascular stroke. This study aimed at assessing QOL and observing the impact of stroke on the self-care, mobility, upper extremity function, language, vision, work/productivity, thinking, family roles, social roles, personality, mood, and energy of stroke patients. As of this day, we could not find any study describing the quality of life of stroke patients in Alexandria stroke unit.
Aim of the study
To assess the quality of life of cerebrovascular stroke patients in Alexandria, Egypt.
Methods
Setting
The study was conducted at the stroke unit of EL-Hadra University Hospital, Neuropsychiatry Department, and the outpatient clinics in the Main University Hospital, in Alexandria governorate. The study site is chosen because the majority of stroke patients who are diagnosed are referred to this clinic for follow-up.
A convenience sample of 80 adult patients who attend the previously mentioned setting and meet the following criteria: age group (21–60) years old, able to communicate verbally, willing to participate, and first visit to the outpatient clinic after the stroke.
Tool of the study
Stroke-specific quality of life scale (SS-QOL). This tool was developed by Williams and Weinberger, (1999) to measure health-related quality of life (HRQOL) and was adopted by the researcher as a translated and validated version to suit the language of the study sample [9, 10]. It is a five Likert scale, and consists of 12 domains, ranging from total help to could not do it at all. The 12 domains consist of 49 items related to: self-care, mobility, upper extremity function, language, vision, work/productivity, thinking, social roles, personality, mood, and energy.
Preparation of study tools
The study tool was adopted and translated into Arabic to suit the language of the study subjects. The tool’s content validity was examined by a jury composed of five experts in the field of medical surgical nursing and then modifications were made accordingly, and the examination revealed that the tool was valid. Reliability of the tool was done on 15 patients by using Cronbach’s alpha, which proved it to be reliable (r = 0.931).
A pilot study was carried out on 10% of the subject of study (8 patients) to test the feasibility and applicability of the tool and to identify the obstacles that may be faced during data collection. The result of the pilot study revealed that the tool was clear and applicable. The pilot study subjects were excluded from the sample for testing.
Full clinical interview was carried out in the clinic in addition to using the Stroke Specific Quality of Life Scale (SS-QOL) tool for related quality of life. All data collected were revised, coded, and fed to statistical software SPSS version 16.
The following statistical tests were used:
-
1.
Descriptive statistics: including mean with standard deviation and percent to describe the scale and categorical data, respectively, while median was used for skewed data.
-
2.
Analysis of categorical data (Monte Carlo exact test and Fisher’s exact test): they are alternatives for the Pearson’s Chi-square test if there were many, small, expected values.
Results
With regard to age, 72.5% of the studied patients’ age ranged from 50 to 60 years old, 21.3% were aged from 40 to less than 50 years, 3.8% were aged between 30 and less than 40 years, while the least population were 2.5% aged from 21 to less than 30 years. Regarding gender, 68.8% of patients were males. 70% of our population were married. The rest were 15% widowed, and 15% were either divorced or single equally.
As for the occupation, only 32.2% were employed while the majority were unemployed (without a contract). While 15% were jobless, 41.3% had technical jobs, 18.8% had clerk jobs, 5% had manual jobs, and 20% were housewives.
For the educational level: 20% were illiterate and 23.8% could only read and write. 6.3%, 12.4%, 20% had primary, preparatory, and secondary school certificates, respectively. Finally, 17.5% had university education. As for residence areas, the majority of our sample (70%) lived in urban areas (Table 1).
QoL domains showed regarding the physical domains, self-care the minimum score was 5 and the maximum was 25 scores. As regards mobility, the minimum score was 6 and the maximum was 30 scores. For the upper extremity function the patients had 5 as minimum and 25 as maximum score. The patients’ language was affected by 5 as minimum and 25 for maximum scores. Minimum scores for vision and work productivity were 3 and maximum were 15 scores. The overall physical domain was 36 and 133 scores, respectively. Regarding psychological domain, thinking, family role, personality, and energy had a 3 for minimum scores and 15 for maximum for each. For social roles and mood, they were affected by a minimum of 5 scores and 25 scores as maximum.
For the physical QOL domain 38.8% of the study subjects had fair physical activity, while 25% of them had poor physical activity. As for psychological QOL domain 56.3% had a fair psychological state while only 8.8% had a good psychological state. The overall status of the patients was fair by 53.8% and good by 18.8% (Figure 1).

Distribution of physical and psychological QOL domain by the study subjects
Table 2 demonstrates the relation between the overall QOL and socio-demographic characteristics. Regarding age, there was significant difference between the overall QOL from good to fair and poor where P = 0.046*.
Regarding employment status, there was significant difference between the overall QOL from good to fair and poor where P = 0.025*. Regarding occupation there was significant difference between the overall QOL from good to fair and poor where P = 0.014*. As for the monthly income there was significant difference between the overall QOL from good to fair and poor where P = 0.022*. The same table showed that there was no statistical difference between the overall QOL, gender, marital status, educational level, and area of residence.
Discussion
Governments and those responsible for providing health care are increasingly aware of the impact that stroke has on the health of the population and the cost to the community [11]. The current study revealed that the age of the great majority of the studied group was above 55 years. The results of this study are in line with Wahab et al. (2011) who reviewed stroke admissions at a tertiary hospital in Nigeria and indicated that stroke incidence increases with age and the chance of having stroke approximately doubles for each decade of life after the age of 55 [12]. This finding is of special concern where more than the half of the subjects were males. In this regard, Joanna et al. (2009) and Morsy (2013) revealed that men had higher incidence of CVS than women, even after full risk factor adjustment [13, 14]. However, contradicted findings by Wahab et al. (2011) who showed dominance of women experiencing CVS in his sample [12].
Regarding educational background, the current study revealed illiteracy among fifth of the studied group and nearly quarter of the subjects knew how to read and write, Approximately the same findings were found by Leite, Nunes and Correa (2011) who found illiteracy among more than one-third of patients with stroke [13, 15].
With regard to residence, the majority of the studied group were from urban areas. This is unexpected as being from rural areas interferes with the access to health care facilities, is associated with lacking awareness of CVS warning signs, and interfere with compliance and follow-up unlike urban residents. This finding was in accordance with Tavangar et al., (2012) where they found that urban population had a higher probability of stroke, hypertension, ischemic heart disease and diabetes than rural population [16]. Additionally, Ennen (2004) reported the same findings in his study on stroke patients [17].
Half of the subjects of the study had low income, where their income did not cover their daily needs or their treatment. This may be due to their type of occupation as they worked manual, clerk work, technical work, or did not work altogether. This is aggravated by the expenses of health maintenance in chronically ill patients and can affect compliance. In this regard, Joanna et al. (2009) revealed that both lower income and wealth are associated with high incidence of CVS [13]. This is supported by Toivanen (2011) who revealed that risk of stroke mortality is high in the low-income group and with poverty among both women and men [18].
As for quality of life of stroke patients, the current study revealed that approximately a quarter of the subjects had both poor physical and psychological QOL. The physical domain was poor in work productivity as they could not do daily work around the house as usual and could not complete a job they started or do any work they used to do. As for vision, they cannot see well as before, having trouble seeing the television well enough to enjoy a show, having trouble reaching things because of poor eyesight and having trouble seeing things off to one side. Also, self-care was affected as they became unable to perform their daily care as dressing, feeding, or toileting on their own that may be due to physical impairment resulting from stroke as upper extremity’s daily function, and mobility is affected and, in addition, they are unable to express their needs. Furthermore, psychological domain was found to be poor in family roles as participants with family activity, feeling that they are a burden on their family and physical condition interfering with personality life. As for energy, being tired most of the time, tired from resting for a long time during the day. As for mental disturbance, inability to concentrate, unable to remember things to do. As for personality change, being impatient, irritable, most of the time with others. This may be due to not knowing the importance of follow-up, especially in patients with recurrent stroke.
In the present study, the subjects showed a highly significant relation between QOL levels and their socio-demographic characteristics as high age, employment status, occupation, and low monthly income. More than third of patients above 50 years old (37.9%), scored poor results compared none from the groups under 50 years This finding was in accordance with Kilkenny et al., as they reported lower VAS score in older patients compared to younger ones [19]. Our data regarding sex differences are relatively similar, although it shows a slight deterioration in the female quality of life compared to the male counterpart. This fact was agreed upon in multiple studies as female gender is considered a risk factor for poor quality of life after stroke [20,21,22].
In our sample, married patients have by far the best quality score compared to other groups. This was the same conclusion of another study by Cenjing Zhu et al. showed deterioration of quality of life in single patients compared to married/with partners [23]. Our study showed worse quality of life in divorced followed by widowed patients.
36.4% of unemployed patients in our study had poor life quality compared to only 8% of our employed patients. In contradiction, a study by Singhpoo et al., showed their unemployed population to have a better outcome compared to their employed ones [24]. This contradiction could be due to the stress of a daily job on chronic patients, while our unemployed patients would suffer lower socioeconomic level causing their poor quality of life. This is confirmed as patients with higher income in our study scored higher quality of life. Finally, regarding educational lever, more than half of illiterate patients had poor quality of life score while those with higher educational lever scored higher scores. This was in accordance with the results of a study by Zalihić [25].
Conclusion
From the results of this study, it was concluded that there was a significant relation between socio-demographic characteristics and the patients QOL, especially age, employment status, and monthly income, the overall QOL (P < 0.05).
Availability of data and materials
The data are available upon request.
Abbreviations
- SS-QOL:
-
Stroke specific quality of life
- AF:
-
Atrial fibrillation
- HRQOL:
-
Health-related quality of life
References
Tonon G. Relevance of the use of qualitative methods in the study of quality of life. In: Tonon G, editor. Qualitative studies in quality of life. Cham: Springer; 2015. p. 3–21.
Alkadry M, Wilson C, Nicholas D. Stroke awareness among rural residents. Soc Work Health Care. 2006;42(2):73–92. https://doi.org/10.1300/J010v42n02_05.
National Stroke Association. Warning Signs of Stroke. 2010. Available at: www.stroke.org. Retrieved on: 9/25/2016.
Lindsay P, Kelloway L, McConnell H. Research to practice: nursing stroke assessment guidelines link to clinical performance indicators. Can Assoc Neurosci Nurses. 2005;26(4):22–7.
Centers for Disease Control and Prevention. Use of a registry to improve acute stroke care—Minnesota Department of Health. 2011. Retrieved on: 9/25/2016.
Minnesota Heart Disease and Stroke Prevention Plan. 2011–2020. Available at: www.health.state.mn.us/cvh. Retrieved on: 9/25/2016.
Health at a glance, OECD indicator. 2011. 74.
Swedish Association of Local Authorities and Regions and National Board of Health and Welfare (2010), Quality and Efficiency in Swedish Health Care—Regional Comparisons 2009, Stockholm.
Muus I, Williams LS, Ringsberg KC. Validation of the Stroke Specific Quality of Life Scale (SS-QOL): test of reliability and validity of the Danish version (SS-QOL-DK). Clin Rehabil. 2007;21(7):620–7.
Williams L, Weinverger M. Development of a stroke-Specific Quality of Life Scale. (1999): American Heart Association, Inc. Available at: http://www.strokeaha.org. Retrieved on: 8/25/2016.
Thom T, Haase N, Rosamond W. a report from the American heart association statistics committee and stroke statistics subcommittee. Heart Dis Stroke Stat. 2011;113:85–90.
Wahab KW, Desalu OO, Fawale B, Olarenwaju TO, Busari OA, Adekoya AO, Afolayan JO. A review of stroke admissions at a tertiary hospital in rural Southwestern Nigeria. Ann Afr Med. 2011;10(2):80–5.
Joanna M, Bates LM, Mauricio A, Glymour MM. the intersection of sex, marital status, and cardiovascular risk factors in shaping stroke incidence: results from the health and retirement study. J Am Geriatrics Soc. 2009;12:2293–9.
Morsy W, Elfeky H. Cerebrovascular stroke recurrence among critically ill patients at a selected University Hospital in Egypt Journal of Biology. Agric Healthc. 2013;3(13):22–34.
Leite HR, Nunes AP, Correa CL. Epidemiological profile and quality of life of stroke survivors. Arquivos de Ciências da Saúde da UNIPAR. 2011;15(1):15–21.
Tavangar A, Shamsaee MH, Chitsaz A, Akbari M, Saadatnia M. Epidemiologic evaluation of stroke risk factors among rural–urban patients in Isfahan university hospitals, Iran. J Isfahan Med School. 2012;29:168.
Ennen KA. Knowledge of Stroke Warning Symptoms and Risk Factors: Variations by rural and urban categories, Proquest Dissertations and Theses, 2004;26: 376–9.
Toivanen S. Income differences in stroke mortality: a 12-year follow-up study of the Swedish working population. Scand J Public Health. 2011;8:797–804.
Kilkenny MF, Grimley R, Lannin NA. Quality of life and age following stroke. Aging. 2019;11(3):845–6. https://doi.org/10.18632/aging.101797.
Gray LJ, Sprigg N, Bath PM, Boysen G, De Deyn PP, Leys D, O’Neill D, Ringelstein EB, Investigators TAIST. Sex differences in quality of life in stroke survivors: data from the Tinzaparin in Acute Ischaemic Stroke Trial (TAIST). Stroke. 2007;38(11):2960–4. https://doi.org/10.1161/STROKEAHA.107.488304.
Bushnell CD, Reeves MJ, Zhao X, Pan W, Prvu-Bettger J, Zimmer L, Olson D, Peterson E. Sex differences in quality of life after ischemic stroke. Neurology. 2014;82(11):922–31. https://doi.org/10.1212/WNL.0000000000000208.
Phan HT, Gall SL, Blizzard CL, Lannin NA, Thrift AG, Anderson CS, Kim J, Grimley RS, Castley HC, Kilkenny MF, Cadilhac DA. Sex differences in quality of life after stroke were explained by patient factors, not clinical care: evidence from the Australian Stroke Clinical Registry. Eur J Neurol. 2021;28(2):469–78. https://doi.org/10.1111/ene.14531.
Zhu C, Tran PM, Leifheit EC, Spatz ES, Dreyer RP, Nyhan K, Wang SY, Goldstein LB, Lichtman JH. The association of marital/partner status with patient-reported health outcomes following acute myocardial infarction or stroke: protocol for a systematic review and meta-analysis. PLoS ONE. 2022;17(11):e0267771. https://doi.org/10.1371/journal.pone.0267771.
Singhpoo K, Charerntanyarak L, Ngamroop R, Hadee N, Chantachume W, Lekbunyasin O, Sawanyawisuth K, Tiamkao S. Factors related to quality of life of stroke survivors. J Stroke Cerebrovasc Dis. 2012;21(8):776–81. https://doi.org/10.1016/j.jstrokecerebrovasdis.2011.04.005.
Zalihic A. Differences in quality of life after stroke and myocardial infarction. Psychiatr Danub. 2010;22(2):241–8.
Acknowledgements
The authors are thankful to the Critical Care and Emergency Nursing Department, Faculty of nursing Alexandria University.
Funding
None.
Author information
Authors and Affiliations
Contributions
JM: participated in the idea conceptualization, patient recruitment, draft writing and critically reviewed the manuscript. AA: responsible for recruitment and management of patients. Participated in data collection and draft writing. FT: helped in conceptualization, patient selection and critically reviewed the manuscript. AR: helped in the idea conceptualization, draft writing and critically reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The current study procedure was revised and approved by the Ethical Committee of the Faculty of Nursing, Alexandria University. A written informed consent to participate in the study was obtained from the participants. Confidentiality and privacy of the study subjects were maintained. The Ethical Committee (EC) at Alexandria university faculty of medicine also approved the study.
Consent for publication
All authors approved the publication.
Competing interests
The authors have declared no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aziz, A.M., Rizian, A.E., Tawfik, F.M. et al. Determinants of the quality of life in Egyptian patients with cerebrovascular stroke by using the stroke specific QoL questionnaire. Egypt J Neurol Psychiatry Neurosurg 59, 22 (2023). https://doi.org/10.1186/s41983-023-00617-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-023-00617-7