
Abstract
Background
Parkinson's disease (PD) is the most common degenerative movement disorder. It is featured by motor manifestations and up till now the clinical diagnosis is based on them. Since the progress in the symptomatic treatment of PD and the longer survival of patients, non-motor manifestations (NMM) were more recognized and considered to be significant. The importance of NMM is that they reflect the more diffuse pathology of PD and may represent an opportunity of earlier diagnosis and treatment. Here in this cross-sectional study, we try to estimate the frequency of such manifestations in PD patients in the country. Using slightly modified PD non-motor (28 of 30 responses) questionnaire (NMS Quest), we studied the incidence of NMM in 100 PD patients attending one major teaching hospital and compared their occurrence in 130 age- and gender-matched non-PD controls.
Results
Out of 100 PD patients (40% females) mean age 67.4 ± 12 with disease duration of 7.3 ± 5.8, range < 1–33.2 years), and 130 control subjects (48.5% females), mean age 65.0 ± 7.0. PD patients had 8.6 ± 5.3 NMM while controls had 3.4 ± 3.3 NMM, respectively (p < 0.00001 t test). Constipation, urgency, insomnia, sad feeling, panic, light headedness and recent memory impairment were the most prevalent NMM in PD compared to controls, while nocturia, restless legs, encopresis and falling were not different in the two groups. The number of NMM ranged from 0 to 21 in PD patients with 50% having ≥ 8 manifestations. The number of NMM did not correlate with age, gender, or disease duration as defined by the classical motor symptoms. Frequency of 23 of these 28 manifestations differed significantly in PD patients compared to controls.
Conclusions
This study confirms that NMM in Jordanian PD patients are very common as reported in other populations. This signifies the universal prevalence of such NMM reflecting their important impact on their daily life and their relevant contribution to better understanding of this disease.
Similar content being viewed by others

Background
Parkinson disease (PD) is a complex neurodegenerative disorder that progresses over time. PD is associated with a range of clinical manifestations involving multiple neurotransmitter pathways within the brain [1,2,3]. Ever since PD has been first described up till many years later, it has been recognized as a motor disorder, yet this might be considered a one-dimensional view of the diverse clinical spectrum of this disease. Along with the motor cardinal features, rigidity, bradykinesia and resting tremor [1, 4,5,6], non-motor symptoms (NMS) almost inevitably emerge with disease progression, and they dominate the clinical picture of advanced PD. NMS such as hyposmia, rapid eye movement sleep behavioral disorder (RBD), depression and constipation present early in the disease [2, 7]. On the other hand, deterioration of global cognition and short-term memory correlate with the disease severity, in which they present in advanced stages reflecting the disease progression [3]. Other NMS include psychosis and hallucinations, autonomic dysfunction, sensory symptoms, and other sleep disorders [8].
Despite the emphasis on motor symptoms, several studies have shown that non-motor symptoms commonly present in PD patients, affecting more than 50% of patients [7, 9,10,11]. There has been evidence suggesting the presence NMM preceding the classical rigidity bradykinetic symptoms including autonomic, olfactory [12] and pathological evidence based on the presence of alpha synuclein in ascending order from the medulla up to the cortex [13]. Since the non-invasive stimulation of the brain tissue (NIBS) by magnetic or electric stimulation has been shown to be feasible and helpful to understand the mechanism of response to different stimuli [14] and to be of possible therapeutic effect of psychiatric symptoms [15] and such symptoms in PD patients [16] the detection of NMM of PD may be important as they may be amenable to such interventions. The pathogenesis of PD is quite complex and may involve the contribution of microorganisms including the microbiota in our intestines [17] as well as the possible role of cyanotoxins related to cyanobacteria [18] or the role of slow chronic inflammatory process and impaired bioactive kynurenines [19] and the role of indolamine single nucleotide polymorphism on the age onset of PD as an important factor in kynurenine pathway of tryptophan metabolism these patients [20]. There has been significant progress in understanding the relationship of gut microbiota regulation and neurodegenerative disease [21], their role in misfolding proteins like alpha synuclein in PD [22]. The finding of peripheral biomarkers for neurodegenerative disorders [23] and the relevant experimental models like the unilateral intralesional 6 hydroxydopamine lesions in mice [24] that showed evidence for non-motor manifestations in this PD model will advance our knowledge in this field. In addition to this, the ongoing efforts to reach personalized medical care based on certain markers in Alzheimer disease and PD [25] will lead to better understanding of the pathophysiology of degenerative neurological disorder and better avenues for new prophylactic and therapeutic options.
Although these symptoms are substantially prevalent in all stages of the disease, most of physicians and researchers’ attention is focused on the motor symptoms. Consequently, this results in missing some pieces of the full picture of the disease and thus, lack of reporting, diagnosis, and management of these NMS. Even though PD is a motor disorder, some of the NMS occur in the very early stages of the disease, preceding the motor triad. These mostly include olfactory dysfunction and RBD [1, 9, 10]. These contribute to the complexity of the range of clinical manifestations in PD including motor, non-motor, and neuropsychiatric features. NMS have been perceived as a crucial determinant of the quality of life of PD patients [10, 12, 13]. Therefore, negligence of such treatable symptoms and potential treatment of some cognitive and psychiatric symptoms in PD patients with NIBS [16]leads to significant deterioration in the patient’s life, in addition to increase in morbidity and mortality rates [28,29,30,31].
Multiple tools have been established for the purpose of NMS assessment. Those include the non-motor symptom scale (NMSS) [26, 27, 32], the scales for outcomes in PD-Sleep (SCOPA-S) [33] Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) [34]. We have used the self-completed non-motor symptoms questionnaire for Parkinson's disease: the (NMS Quest) which has been validated in other study [35].
Others have used diaries based on daily activities [36]
The purpose of this study is to find the prevalence of NMS of PD among patients in the country. Furthermore, to evaluate the pattern of occurrence and frequency of each symptom. This study will shed light on the significance of NMS so that their impact on the patient’s quality of life and progression of PD will be better appreciated. Accordingly, this will encourage physicians and researchers to spend more time and effort on the management of NMS and understanding their pathophysiology, particularly with the lack of research around this topic in the country.
Methods
The current study was held at one major teaching hospital. The study was conducted between November 2019 and December 2020. The study was designed as a cross-sectional case control study, with a review through clinical records of 659 patients who have been diagnosed with Parkinson's disease at specialty neurology clinics. Among these sample, 152 patients could not be reached; 120 patients did not complete the interview; 281 refused to participate in the study; and 6 were excluded because they had been diagnosed with non-idiopathic Parkinson disease (drug-induced Parkinsonism); 100 patients completed the interview and fulfilled the criteria to be a case for this study (Fig. 1). To qualify as a case, the diagnosis "Parkinson" must be clearly documented and signed by a consultant neurologist in the clinical record. Moreover, control was defined as a patient who has not been diagnosed previously with PD but follows up at different medical (except neurology) clinics and were seen in the same period as PD patients. 130 non-PD patients were randomly selected and in total 230 patients and controls were interviewed through phone calls. A questionnaire of demographic variables (age, gender, marital status, and date and place of diagnosis). A slightly modified version of NMS QUEST which is the most widely used measure of the non-motor symptoms of PD, with well-established reliability and validity [32]. It consists of 30 questions each asks about experiencing one of the non-motor symptoms. The answer is considered “Yes” if the patient has experienced it during the past month. And it is considered “No” If they have not experienced it in the past month. 28 out of the 30 questions were included in the questionnaire. Some of the studied manifestations are defined as follows. Constipation (defined as less than 3 bowel movements a week or having to strain to pass a stool). Urinary urgency (defined as a sense of urgency to pass urine makes you rush to the toilet). Insomnia (defined as difficulty getting to sleep at night or staying asleep at night. Feeling sad (defined as feeling sad, ‘low’ or ‘blue’). Feeling panicky (defined as feeling anxious, frightened, or panicky). Recent memory impairment (defined as problems remembering things that have happened recently or forgetting to do things. Poor concentration (defined as difficulty concentrating or staying focused). Lack of interest (defined as loss of interest in what is happening around you or doing things. Hallucinations (defined as seeing or hearing things that you know or are told are not there). Delusions (defined as believing things are happening to you that other people say are not true). Nightmares (defined as intense, vivid dreams or frightening dreams). Hypersomnolence (defined as finding it difficult to stay awake during activities such as working, driving, or eating. REM sleep disorders (defined as talking or moving about in your sleep as if you are ‘acting’ out a dream). Dysphagia (defined as difficulty swallowing food or drink or problems with choking). Dysgeusia and anosmia (defined as loss or change in your ability to taste or smell). Sialorrhea (defined as dribbling of saliva during the daytime). Weight change (defined as unexplained change in weight, not due to change in diet. Lightheadedness (defined as feeling lightheaded, dizzy, or weak standing from sitting or lying). The 2 questions asking about sexual desire and difficulties were not included. Furthermore, questions about the duration and onset of experiencing each symptom were added to assess the relationship between motor and non-motor manifestations.

Flowchart showing PD patient selection
The statistical analysis was performed using the statistical package for social sciences IBM SPSS version 22, 2020 (SPSS Inc., Chicago, IL, USA). For continuous variables t test was used and for categorical variable cross-tables with Chi-square calculated for significance between the two groups. p value of < 0.05 was significant. Pearson correlation was calculated to assess relationship between NMM, age, gender and duration of PD based on motor diagnosis.
Results
Table 1 shows demographic characteristics of PD patients and controls as well as the frequencies of the 28 NMM. We included 100 patients of PD including 60 males (60%) and 40 females (40%) and the mean age of 67.4 ± 12 years and mean disease duration of 7.3 ± 5.8, range < 1–33.2 years. Meanwhile, there were 130 non-PD control subjects, 67 males (51.5%) and 63 females (48.5%) and a mean age of 65.0 ± 7.0 years. There was no significant difference in the age (p = 0.08) or gender (p = 0.85) between the two groups (Table 1). Overall findings of NMM in PD and control groups: frequency of 23 of the 28 studied manifestation differed significantly in PD patients compared to controls with prevalence ranging from 12 to 66% in PD patients, 0.8 to 39.2% in controls. The other five NMM (nocturia, restless legs, incomplete fecal evacuation, encopresis, and fainting) were not statistically different in the two groups (Table 2). The number of NMM per patient ranged from 0 to 21 in PD patients with 50% having ≥ 8 manifestations. The most common NMM, constipation, nocturia, urinary urgency, insomnia, sad feelings, panic, and vertigo/light headedness occurred each occurred in ≥ 40% of PD patients, while 22 out of the 28 NMM each occurred in ≥ 20% of these patients. While in the control group only one NMM, nocturia occurred in ≥ 40%, and 5 NMM occurred in ≥ 20%. The most common NMM in control group were nocturia, urinary urgency, insomnia, unexplained pain, and recent memory impairment each occurring in ≥ 20%. Frequencies are described in more detail in Table 2 and the Fig. 2. The most common manifestations in PD were gastrointestinal and urinary symptoms, namely, constipation followed by urinary urgency with frequencies in PD, controls of 66%, 15.4% (p = 0.000), and 53%,39.2% (p = 0.031), respectively. These were followed by sleep and neuropsychiatric manifestations, namely, insomnia, feeling sad, and feeling panicky with frequencies in PD, controls of 49%, 23.1% (p < 0.00001), 47%, 16.2% (p = 0.000), and 47%, 17.7% (p = 0.001), respectively. Other neuropsychiatric manifestations ranked less in the frequency in PD patients with recent memory impairment along with poor concentration, both showing higher prevalence among PD patients with frequencies of 39% and 28% in PD patients, 21.5% and 16.9% in controls (p = 0.004, 0.043), respectively. Lack of interest was more frequent in PD patients with a frequency of 36%, 16.2% in controls (p = 0.001). Hallucinations and delusions were also more common in PD patients rather than controls (19% and 13%, 0.2.3% and 1.5%, respectively. p = 0.000). Other sleep disturbances were also more common in PD patients including nightmares, hypersomnolence, and REM sleep disorders, with frequencies of 33%, 31%, and 26%, 10.8%, 3.1%, and 5.4%, respectively (p < 0.00001). Although encopresis and fecal incontinence did not show statistically significant difference between the two groups, other gastrointestinal manifestations did. Dysphagia, dysgeusia and anosmia, sialorrhea, weight change, and nausea and vomiting were more common in PD patients (35%, 28%, 27%, 26%, and 12%, 3.1%, 1.5%, 0.8%, 6.2, and 3.1%, respectively, p < 0.05). Lightheadedness, unexplained pain, LL edema, hyperhidrosis and diplopia were also more common in PD patients. The onset of NMM varied from one manifestation to another. The relationship between the onset of NMM and the classical motor based clinical diagnosis varied also markedly with a minimum mean of almost 5 years prior to diagnosis (− 4 0.9 ± 7.2). Of the 28 NMM only 5 were reported to occur after the motor onset (nausea/vomiting, visual hallucinations, syncope, lower limb edema and delusions) while all other 23 manifestations could precede or follow the motor manifestations.

The frequencies of non-motor manifestations in Parkinson’s disease patients and control group. * Indicates p < 0.05. Only 5 out of 28 features were not more prevalent in PD compared to controls
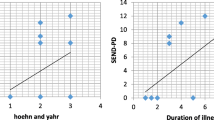
Relation of symptoms to patient characteristics: the number of NMM did not correlate with age, gender, or disease duration (r = − 0.16, 0.07, 0.17 and p = 0.12, 0.52 and 0.0.09, respectively). We did not assess disease severity in this study as this was a questionnaire study and we did not have well documented data of the severity or stage of the disease in each patient.
Discussion
In this first study about PD patients in Jordan, we have confirmed what has been shown in other studies coming from different parts of the world indicating the high prevalence of NMM in PD patients [27, 29, 38,39,40,41,42] in addition to 3 studies from Egypt [43,44,45] using the validated NMS QUEST questionnaire. As we compared our patients to an age- and gender-matched group, we found that the frequency and distribution of these NMM differed significantly in PD patients reflecting that PD pathology would mandate what manifestation will be more prevalent. Most of the studied NMM 23/28 were significantly more prevalent in PD patients and these manifestations reflect the well-known diffuse pathology of PD which is much beyond the substantia nigra and involves areas related to affect, sleep, pain, autonomic and cognitive functions [2, 6, 41]. The number of these NMM did not correlate with age, gender, or duration of disease based on clinical motor diagnosis. This may indicate that these NMM are integral and independent part of this disease with different pathophysiology and time course independent of the motor manifestations. Of the common NMM nocturia did not differ significantly between the 2 groups perhaps reflecting the age-related lower urinary tract dysfunction that is quite common, and age related [37]. Fainting and RLS also did not differ in the two groups due the increased prevalence of both symptoms with age [46,47,48]. Encopresis almost reached statistical significance occurring more in PD patients 9.0% compared to 3.1% (p = 0.054) and this could have been significant if we had a larger sample size. Most studies found it was the least reported NMM or not significantly different from control group [27, 38]. The onset of 22 out of the 28 manifestations were reported by some of these patients to occur before the motor onset by variable time (-4.9 ± 7.2 years). This is important as clinicians do not consider PD as a differential diagnosis in those who present with these NMM. If for example we consider a scoring system for patients who present with the most common NMM before their clinical PD diagnosis, excluding those symptoms that are also known to be common in a matched control group, these patients perhaps can be followed for possible future conversion to clinical PD. So, in our study if we consider someone who presents with constipation, urinary urgency, insomnia, depression, and unexplained chronic pain then such a patient may be having the prodrome or preclinical PD as we know it with its motor manifestations. This group of patients may then be chosen with a control group to undergo more advance evaluation for possible PD like dopa PET scan [37], and then be considered for a disease-modifying investigational drug trial. On the other hand, these NMM regardless of their time relationship to the motor signs, have been shown to have significant impact on patients’ daily activities and function and need to be addressed and managed [5, 6, 28, 40, 48]. There are still further issues that need to be studied in PD patients including studies to assess modulation of autonomic nervous system for behavioral regulation as manifested by response to interpersonal space (IPS) changes by methods like skin conductance response (SCR) which was quite sensitive in normal persons [49, 50]. Finally, we recognize the limitations of our study. First, it is one center rather than representative of Jordan. Since our facility is in the heart of the capital city and we have patients coming from all over the country, we can say it may reflect partially the PD population in the country. Second the number of patients was relatively small, and the control subjects were matched only for gender and age, and we did not look for other confounding factors like smoking, diet habits, atherosclerotic risk factors. This may give this study less weight regarding its conclusions and we may need to study these PD patients with better matched controls. Also, we did not attempt to correlate the findings with the severity of the disease for the reason discussed above.
Conclusions
In summary, we presented here data showing that NMM were quite prevalent in PD patients in Jordan. The significance of this study is that it confirmed findings of other studies done in different parts of the world including the three studies from Egypt (43, 44, 45), though it is the first in Jordan. This subject needs further study in well controlled PD cohorts to better understand the frequency and effect of such manifestations on the life and disease progression in this disease. These manifestations reflect the widespread pathology of PD reflecting its systemic rather than restricted nature. Looking for and understanding the pathophysiology of such manifestations may allow better knowledge of the natural progression of such chronic degenerative disorders and may represent an opportunity to study such a disease before its relentless progressive motor signs taking advantage of our current understanding of the possible role of infectious, inflammatory, genetic, and environmental factors associated with these diseases. This will help in finding better ways of prevention and treatment of such disorders.
Availability of data and materials
The data set used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Abbreviations
- PD:
-
Parkinson’s disease
- NMM:
-
Non-motor manifestations
- NMS Quest:
-
Non-motor symptoms questionnaire
- NMS:
-
Non-motor symptoms
- NIBS:
-
Non-invasive stimulation of the brain tissue
- RBD:
-
REM sleep behavioral disorder
- NMSS:
-
Non-motor symptom scale
- SCOPA-S:
-
Scales for outcomes in PD-Sleep
- MDS-UPDRS:
-
Movement Disorder Society Unified Parkinson Disease Rating Scale
- IBM SPSS:
-
Statistical Package of Social Sciences
References
Langston JW. The Parkinson’s complex: parkinsonism is just the tip of the iceberg. Ann Neurol. 2006;59(4):591–6.
Lee HM, Koh SB. Many faces of Parkinson’s disease: non-motor symptoms of Parkinson’s disease. J of Mov Disord. 2015;8(2):92–7.
Schapira AHV, Chaudhuri KR, Jenner P. Non-motor features of Parkinson disease. Nat Rev Neurosci. 2017;18(7):435–50.
Lim S, Fox SH, Lang AE. Overview of the extranigral aspects of Parkinson disease. Arch Neurol. 2009;66(2):167–72.
Barone P, Antonini A, Colosimo C, Marconi R, Morgante L, Avarello TP, et al. The PRIAMO study: a multicenter assessment of nonmotor symptoms and their impact on quality of life in Parkinson’s disease. Mov Disord. 2009;24(11):1641–9.
Lyons KE, Pahwa R. The impact and management of nonmotor symptoms of Parkinson’s disease. Am J Manag Care. 2011;17(Suppl 12):S308–14.
Shulman LM, Taback RL, Rabinstein AA, Weiner WJ. Non-recognition of depression and other non-motor symptoms in Parkinson’s disease. Parkinsonism Relat Disord. 2002;8(3):193–7.
Chaudhuri KR, Healy DG, Schapira AH. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol. 2006;5(3):235–45.
Chaudhuri KR, Odin P, Antonini A, Martinez-Martin P. Parkinson’s disease: the non-motor issues. Parkinsonism Relat Disord. 2011;17(10):717–23.
Chaudhuri KR, Schapira AHV. Non-motor symptoms of Parkinson’s disease: dopaminergic pathophysiology and treatment. Lancet Neurol. 2009;8(5):464–74.
Bostantjopoulou S, Katsarou Z, Karakasis C, Peitsidou E, Milioni D, Rossopoulos N. Evaluation of non-motor symptoms in Parkinson’s Disease: an underestimated necessity. Hippokratia. 2013;17(3):214–9.
Palma JA, Kaufmann H. Autonomic disorders predicting Parkinson’s disease. Parkinsonism Relat Disord. 2014;20(1):94–8. https://doi.org/10.1016/S1353-8020(13)70024-5 (PMID: 24262198; PMCID: PMC4122262).
Braak H, Del Tredici K, Rub U, de Vos RA, Jansen Steur EN, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003;24:197–211 (PubMed: 12498954).
Borgomaneri S, Vitale F, Battaglia S, Avenanti A. Early right motor cortex response to happy and fearful facial expressions: a TMS motor-evoked potential study. Brain Sci. 2021;11:1203.
Terranova C, Rizzo V, Cacciola A, Chillemi G, Calamuneri A, Milardi D, Quartarone A. Is there a future for non-invasive brain stimulation as a therapeutic tool? Front Neurol. 2019;9:1146. https://doi.org/10.3389/fneur.2018.01146.
Dinkelbach L, Brambilla M, Manenti R, Brem AK. Non-invasive brain stimulation in Parkinson’s disease: exploiting crossroads of cognition and mood. Neurosci Biobehav Rev. 2017;75:407. https://doi.org/10.1016/j.neubiorev.2017.01.021.
Sini P, Dang TBC, Fais M, Galioto M, Padedda BM, Lugliè A, Iaccarino C, Crosio C. Cyanobacteria, cyanotoxins, and neurodegenerative diseases: dangerous liaisons. Int J Mol Sci. 2021;22(16):8726. https://doi.org/10.3390/ijms22168726.
Tanaka M, Toldi J, Vécsei L. Exploring the etiological links behind neurodegenerative diseases: inflammatory cytokines and bioactive kynurenines. Int J Mol Sci. 2020;21(7):2431. https://doi.org/10.3390/ijms21072431.
Török N, Maszlag-Török R, Molnár K, Szolnoki Z, Somogyvári F, Boda K, Tanaka M, Klivényi P, Vécsei L. Single nucleotide polymorphisms of indoleamine 2,3-dioxygenase 1 influenced the age onset of Parkinson’s disease. Preprints. 2020;2020:2020090470. https://doi.org/10.20944/preprints202009.0470.v1.
Cannon T, Gruenheid S. Microbes and Parkinson’s disease: from associations to mechanisms. Trends Microbiol. 2022;30:749–60. https://doi.org/10.1016/j.tim.2022.01.004.
Sun P, Su L, Zhu H, Li X, Guo Y, Du X, et al. Gut microbiota regulation and their implication in the development of neurodegenerative disease. Microorganisms. 2021;9:2281. https://doi.org/10.3390/microorganisms9112281.
González-Sanmiguel J, Schuh CMAP, Muñoz-Montesino C, Contreras-Kallens P, Aguayo LG, Aguayo S. Complex interaction between resident microbiota and misfolded proteins: role in neuroinflammation and neurodegeneration. Cells. 2020;9:2476. https://doi.org/10.3390/cells9112476.
Török N, Tanaka M, Vécsei L. Searching for peripheral biomarkers in neurodegenerative diseases: the tryptophan-kynurenine metabolic pathway. Int J Mol Sci. 2020;21:9338. https://doi.org/10.3390/ijms21249338.
Mendes-Pinheiro B, Soares-Cunha C, Marote A, Loureiro-Campos E, Campos J, Barata-Antunes S, et al. Unilateral intrastriatal 6-hydroxydopamine lesion in mice: a closer look into non-motor phenotype and glial response. Int J Mol Sci. 2021;22:11530. https://doi.org/10.3390/ijms222111530.
Lam S, Hartmann N, Benfeitas R, Zhang C, Arif M, Turkez H, et al. Systems analysis reveals ageing-related perturbations in retinoids and sex hormones in Alzheimer’s and Parkinson’s diseases. Biomedicines. 2021;9:1310. https://doi.org/10.3390/biomedicines9101310.
Chaudhuri KR, Martinez-Martin P, Brown RG, Sethi K, Stocchi F, Odin P. The metric properties of a novel non-motor symptoms scale for Parkinson’s disease: results from an international pilot study. Mov Disord. 2007;22(13):1901–11.
Sauerbier A, Jitkritsadakul O, Titova N, Klingelhoefer L, Tsuboi Y, Carr H, et al. Non-motor symptoms assessed by non-motor symptoms questionnaire and non-motor symptoms scale in Parkinson’s disease in selected Asian populations. Neuroepidemiology. 2017;49(1–2):1–17.
Martinez-Martin P, Rodriguez-Blazquez C, Monica M, Kurtis MM, Chaudhuri KR. The impact of non-motor symptoms on health-related quality of life of patients with Parkinson’s disease. Mov Disord. 2011;26(3):339–496.
Zis P, Erro R, Walton CC, Sauerbier A, Chaudhuri KR. The range and nature of non-motor symptoms in drug-naive Parkinson’s disease patients: a state-of-the-art systematic review. NPJ Parkinson’s Dis. 2015;1:15013. https://doi.org/10.1038/npjparkd.2015.13.
Global Parkinson's Disease Survey (GPDS) Steering Committee. Factors impacting on quality of life in Parkinson's disease: results from an international survey. Mov Disord. 2002;17(1):60–7.
Aarsland D, Larsen JP, Tandberg E, Laake K. Predictors of nursing home placement in Parkinson’s disease: a population-based, prospective study. J Am Geriatr Soc. 2000;48(8):938–42.
Chaudhuri KR, Martinez-Martin P, Schapira AH, Stocchi F, Sethi K, et al. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: the NMSQuest study. Mov Disord. 2006;21(7):916–23.
Marinus J, Visser M, van Hilten JJ, Lammers GJ, Stiggelbout AM. Assessment of sleep and sleepiness in Parkinson disease. Sleep. 2003;26(8):1049–54.
Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P, et al. Movement disorder society-sponsored revision of the unified Parkinson’s Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–70.
Romenets SR, Wolfson C, Galatas C, Pelletier A, Altman R, Wadup L, et al. Validation of the non-motor symptoms questionnaire (NMS-Quest). Parkinsonism Relat Disord. 2012;18(1):54–8.
Marinus J, Visser M, Stiggelbout AM, Rabey JM, Bonuccelli U, et al. Activity-based diary for Parkinson’s disease. Clin Neuropharmacol. 2002;25(1):43–50.
Zhong LL, Song YQ, Cao H, Ju KJ, Yu L. The non-motor symptoms of Parkinson’s disease of different motor types in early stage. Eur Rev Med Pharmacol Sci. 2017;21(24):5745–50.
Marisol SC, Alberto CJ, Noel P, Lilia N, Parménides G. Frequency and dynamics of non-motor symptoms presentation in Hispanic patients with Parkinson disease. Front Neurol. 2019. https://doi.org/10.3389/fneur.2019.01197.
Gulunay A, Cakmakli GY, Yon MI, Ulusoy EK, Karakoc M. Frequency of non-motor symptoms and their impact on the quality of life in patients with Parkinson’s disease: a prospective descriptive case series. Psychogeriatrics. 2020;20(2):206–11.
Mukhtar S, Imran R, Zaheer M, Tariq H. Frequency of non-motor symptoms in Parkinson’s disease presenting to tertiary care centre in Pakistan: an observational, cross-sectional study. BMJ Open. 2018;8(5):e019172.
Durcan R, Wiblin L, Lawson RA, Khoo TK, Yarnall AJ, Duncan GW, ICICLE-PD Study Group, et al. Prevalence and duration of non-motor symptoms in prodromal Parkinson’s disease. Eur J Neurol. 2019;26(7):979–85.
Bliwise DL, Wagg A, Sand PK. Nocturia. A highly prevalent disorder with multifaceted consequences. Urology. 2019;133S:3–13. https://doi.org/10.1016/j.urology.2019.07.005.
Khedr EM, El Fetoh NA, Khalifa H, Ahmed MA, El Beh KM. Prevalence of non-motor features in a cohort of Parkinson’s disease patients. Clin Neurol Neurosurg. 2013;115(6):673–7.
Shalash AS, Hamid E, Elrassas H, Bahbah EI, Mansour AH, Mohamed H, et al. Non-motor symptoms in essential tremor, akinetic rigid and tremor-dominant subtypes of Parkinson’s disease. PLoS ONE. 2021;16(1): e0245918. https://doi.org/10.1371/journal.pone.0245918.
Shalash AS, Hamid E, Elrassas HH, Bedair AS, Abushouk AI, Khamis M, Hashim M, Ahmed NS, Ashour S, Elbalkimy M. Non-motor symptoms as predictors of quality of life in Egyptian patients with Parkinson’s disease: a cross-sectional study using a culturally adapted 39-Item Parkinson’s Disease Questionnaire. Front Neurol. 2018;24(9):357. https://doi.org/10.3389/fneur.2018.00357.PMID:29881368;PMCID:PMC5976737.
Hogan TM, Constantine ST, Crain AD. Evaluation of syncope in older adults. Emerg Med Clin North Am. 2016;34(3):601–27.
Peralta C, Biafore F, Depetris TS, Bastianello M. Recent advancement and clinical implications of 18FDG-PET in Parkinson’s disease, atypical Parkinsonisms, and other movement disorders. Curr Neurol Neurosci. 2019;19(8):56. https://doi.org/10.1007/s11910-019-0966-3 (PMID: 31256288).
Trenkwalder C, Allen R, Högl B, Clemens S, Patton S, Schormair B, et al. Comorbidities, treatment, and pathophysiology in restless legs syndrome. Lancet Neurol. 2018;17(11):994–1005.
Ellena G, Battaglia S, Làdavas E. The spatial effect of fearful faces in the autonomic response. Exp Brain Res. 2020;238:2009–18. https://doi.org/10.1007/s00221-020-05829-4.
Candini M, Battaglia S, Benassi M, di Pellegrino G, Frassinetti F. The physiological correlates of interpersonal space. Sci Rep. 2021;11:2611. https://doi.org/10.1038/s41598-021-82223-2.
Acknowledgements
Special thanks to all patients who agreed to participate in this study ant to Jordan university hospital medical records department head, Hasan Rihan and the staff.
Funding
Self-supported. No funding from any institute or person.
Author information
Authors and Affiliations
Contributions
SD: idea generation, data analysis and writing of the initial manuscript, revision, and acceptance of the final manuscript, MMr, LO, and NA, M Moh participated in idea generation, data collection and methods section writing. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Jordan university review board (IRB)/Faculty of medicine research committee decision #122/2021 its meeting #6/2021 on 30/03/2021. All patients gave an informed verbal consent as this was a retrospective study with interview of the patients and review of their medical file. No interventions were applied on the participants and the institution review board approved the study based on this informed verbal consent.
Consent for publications
Not applicable.
Competing interests
None for any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dahbour, S.S., Al Murr, M.J., Oweis, L.H. et al. Non-motor manifestation of Parkinson's disease: a cross-sectional study in a teaching hospital in Jordan. Egypt J Neurol Psychiatry Neurosurg 58, 148 (2022). https://doi.org/10.1186/s41983-022-00559-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-022-00559-6