
Abstract
Background
Accumulating data have suggested that vitamin D receptor (VDR) gene is a pretender gene for vulnerability to Parkinson disease (PD). This study aimed to assess the relationship of VDR gene polymorphisms (FokI and ApaI) with PD. Fifty patients suffering from PD and 50 age- and sex-matched healthy controls were included. Unified Parkinson Disease Rating Scale (UPDRS) was done to assess disease severity. Genetic testing for VDR gene single nucleotide polymorphisms (FokI and ApaI) was done using real time polymerase chain reaction (PCR) technique.
Results
Concerning frequency of genes and alleles for vitamin D receptor gene polymorphisms (FokI and ApaI), no statistically significant difference was found between PD patients and controls. AC genotype was associated with younger age and younger age at onset of disease compared to CC and AA genotypes of ApaI gene polymorphisms. CC genotype was significantly positively correlated with fatigue and urine incontinence. VDR gene polymorphisms were not found to be independent predictors for severity of PD after adjustment for possible confounders.
Conclusion
VDR gene polymorphisms are related to the clinical manifestations rather than etiology or severity of idiopathic PD.
Similar content being viewed by others


Background
Genetic studies on vitamin D receptor (VDR) polymorphisms have proposed contribution of VDR to several neurodegenerative disorders, including multiple sclerosis, Alzheimer disease, and Parkinson disease (PD) [1].
VDR gene is located on the long arm of chromosome 12 region. Genetic polymorphisms describe the inter-individual, functionally silent differences in deoxy ribonucleic acid sequence that make each human genome unique. More than 60 VDR polymorphisms have been discovered. These polymorphisms are located in the promoter, in and around exons 2–9 and in the 3′untranslated region [2].
Vitamin D functions are modulated by VDR. It is activated upon binding to the active form of vitamin D. It interacts with vitamin D response elements in the promoters of vitamin D target genes to regulate their expression. Remarkably, VDR is greatly expressed in dopaminergic neurons of the substantia nigra suggesting its role in the pathophysiology of PD [3].
Prior researchers have reported associations between severity and clinical manifestations of PD and VDR gene polymorphisms [4,5,6,7,8,9].
The present study aimed to study the relation between VDR gene polymorphisms (FokI and ApaI) and PD, and to examine their relation to clinical presentation and disease severity.
Methods
This is a case control study conducted on 50 Egyptian patients diagnosed as idiopathic Parkinson disease and 50 age- and sex-matched healthy controls, in the period from April 2017 to May 2018.
The study proposal was approved by the ethical committee of department of Neurology. The aim, procedures of the study, the data confidentiality was explained to every participant. Informed consent was obtained before patients were enrolled in the study.
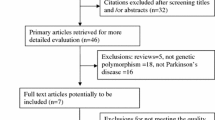
Patients with PD diagnosed according to MDS clinical diagnostic criteria for Parkinson's disease, 2015 [10] were included. Their age ranged between 45 and 70 years old.
Excluded from this study
Patients with diseases that may disturb cognitive functions, such as, diabetes mellitus, renal, hepatic diseases, or thyroid dysfunction and patients with brain magnetic resonance imaging showing structural lesions.
Patients were submitted to comprehensive neurological evaluation. Unified Parkinson Disease Rating Scale (UPDRS) [11] was done to assess disease severity. VDR-ApaI SNP (rs7975232) and VDR-FokI SNP (rs 2228570) gene polymorphisms were tested using PCR. SNP genotyping of VDR gene was performed with the Type-it Fast SNP Probe Kit (Qiagen) according to the manufacturer’s instructions using validated TaqMan ® SNP genotyping primers and probe (Applied Biosystems, Foster City, CA, USA).
Statistical analysis
The collected data were coded, tabulated, and statistically analyzed using IBM SPSS statistics (Statistical Package for Social Sciences) software version 22.0, IBM Corp., Chicago, USA, 2013. Data was summarized using mean, standard deviation, median, minimum and maximum in quantitative data and using frequency (count) and relative frequency (percentage). Comparisons between quantitative variables were done using the non-parametric Kruskal-Wallis and Mann-Whitney tests. Chi square (χ2) test was performed for categorical data. Exact test was used when the expected frequency is less than 5. Correlations between quantitative variables were done using Spearman correlation coefficient. Genotype and allele frequencies were compared between patients and control groups using logistic regression. Odds ratio (OR) with 95% confidence intervals was calculated. Linear regression analysis was done to predict total severity scores using VDR polymorphisms. Logistic regression was done to detect independent predictors of severity. P values less than 0.05 were considered as statistically significant.
Result
The age of patients ranged from 45 to 70 years with a mean of 60.8 ± 5 years whereas, the age of controls ranged from 46 to 68 years with a mean of 61.4 ± 5.7 years. The patients group included 34 males (68%) and 16 females (32%). The control group included 32 males (64%) and 18 females (36%). Patients and controls were matched regarding mean age and sex distribution (p = 0.5, 0.7 respectively).
The age at onset of the disease ranged from 40 to 69 years with a mean 57.32 ± 6.40 years, while disease duration ranged from 1 to 10 years with a mean 3.42 ± 2.35 years. Six patients (12%) had positive family history of PD.
Forty patients (80%) presented with tremor dominant phenotype while, 10 patients (20%) presented with postural instability gait difficulty phenotype.
Constipation was found in 28 (56%) patients, memory impairment in 15 (30%) patients, visual problems in 13 (26%) patients, sleep behavior disorder (REM) in 12 (24%) patients, depression in 9 (18%) patients, erectile dysfunction in 3 (6%) patients , insomnia in 3 (6%) patients, and fatigue in 1 (2%) patient.
Scores of UPDRS were as follows: mentation, behavior, and mood section UPDRS score ranged from 0 to 7 with median 1, activities of daily living (ADL) section score ranged from 1 to 33 with median 19 and, motor section score ranged from 12 to 47 with median 28.
According to H and Y staging, 20 patients (40%) had stage 1, 11 patients (22%) had stage 1.5, 9 patients (18%) had stage 2, 4 patients (8%) had stage 2.5, 4 patients (8%) had stage 3, and 2 patients (4%) had stage 4.
For statistical reasons, we added the AA and AG genotypes in FokI polymorphism as AA genotype was found only in one patient. No statistically significant difference was found between the studied groups concerning the distribution of VDR genotypes and alleles (p > 0.05) (Table 1).
In SNP FokI, no statistically significant difference was detected between distribution of different genotypes AA, AG, and AG (P value = 0.480). While SNP ApaI showed a statistically significant difference between distribution of CC, AC, and AA genotypes (P value = 0.002). Pairwise comparison revealed that AC was significantly present compared to CC and AA (p < 0.001) and AA was significantly present compared to CC (P = 0.008). This indicates that among PD patients, AC genotype was the most common and the CC was the least frequent genotype (Table 2).
There is a tendency towards significant preponderance of male sex in FokI GG genotype (p = 0.068). A statistically significant difference was found in VDR gene rs7975232 (ApaI) polymorphisms regarding mean age and age at onset of disease (p = 0.005 and 0.012, respectively). Post hoc test revealed a statistically significant difference between AA and AC in the mean age and age at onset of disease (P = 0.004 and 0.009, respectively). AC genotype was associated with younger age and younger age at onset of disease compared to CC and AA genotypes (Figs. 1 and 2).

Relation between VDR gene ApaI polymorphism and age of patients. VDR: vitamin D receptor

Relation between VDR gene ApaI polymorphism and age at onset of the disease. VDR: vitamin D receptor
However, there was no statistically significant difference between ApaI polymorphisms in the mean duration of disease. Also, there was no statistically significant difference in VDR gene rs2228570 (FokI) polymorphisms regarding mean age, age at onset of disease, or duration of disease (P = 0.179, 0.170, and 0.578, respectively).
Regarding VDR gene ApaI polymorphisms, CC genotype was significantly positively correlated with fatigue and urine incontinence (r = 0.32, P = 0.02). However, there was no statistically significant difference between FokI and ApaI VDR gene polymorphisms regarding starting motor symptom.
VDR gene FokI and ApaI polymorphisms were not significantly correlated with scores of UPDRS or H and Y staging (p > 0.05).
Linear regression analysis was done between UPDRS-I scores, activity of daily living, and motor examination as dependent factors and VDR polymorphisms as independent factor. Logistic regression analysis was also done between modified H and Y scale as dependent factor and VDR polymorphisms as independent factor. We found that P value was not significant after adjustment for age, sex, age at onset of disease, and disease duration. This points to that VDR gene polymorphisms were not independent predictors for UPDRS scores or H and Y staging (Tables 3 and 4).
Discussion
In the current study, no statistically significant difference of genotypes or allele occurrence for VDR gene polymorphism (FokI and ApaI) between PD patients and healthy controls. This was in agreement with Petersen and colleagues. (2014) [12], who found no statistical significant difference between PD patients and controls regarding genotypes or allele frequency for VDR gene polymorphism ApaI. On the contrary, a Turkish study by Gezen and colleagues (2017) [13] reported that in ApaI polymorphism, allele C was expressively more in PD patients than controls and significantly increases the risk of developing PD irrespective of age and age at onset. Also, a previous study done on a Chinese cohort revealed that the frequency of FokI CC + CT genotypes was higher in PD patients compared to controls [14]. Another study done on Hungarian by Torok and colleagues (2013) [6] found that VDR FokI CC + CT genotypes were higher among PD patients compared to controls. The controversy between studies may be attributed to differences in sample size and ethnic backgrounds, which may have effect on the genetic map.
The present study revealed that ApaI AC genotype was associated with younger age and younger age at onset of disease compared to CC and AA genotypes. The neuroprotective theory of VDR gene in the pathophysiology of PD can provide some explanation to this finding. The younger age at disease onset in patients with AC genotype could lead to dopaminergic neuronal damage due to defective process of neuroprotection. The nigral dopaminergic neurons appear to be the first suffer from neuro-inflammation and decreased neuroprotection [14]. Also, Han and colleagues (2012) [14] found significant difference in FokI genotype distribution between early onset PD patients and healthy controls, as FokI CT + CC genotypes raised risk of early onset PD compared to FokI TT genotype. On contradistinction to this finding, Torok and colleagues (2013) [8] showed no significant association between VDR gene polymorphism FokI and ApaI and the age at onset of PD. The discrepancies between these studies could be explained by differences in ethnic backgrounds and difficulties in determining the actual age at onset of the disease
In the current study, a significant positive correlation was detected between fatigue and urine incontinence and CC genotype of VDR ApaI polymorphisms. To the best of our knowledge, no previous studies correlated VDR gene polymorphisms distribution and non-motor symptoms of PD. However, this study revealed no association between VDR gene polymorphisms and motor symptoms of PD, a finding which agreed with Gezen and colleagues (2017) [6] who reported no association between motor symptoms of PD patients and ApaI and FokI genotypes.
The present study showed no relation between severity of PD assessed by UPDRS and H and Y staging and VDR gene polymorphisms after adjustment for possible confounders. On the contrary, Suzuki and colleagues (2012) [15] reported that FokI CC genotype was significantly associated with lower H and Y stages. The discrepancy may be related to the inclusion of small sample size in this work compared to that of Suzuki and colleagues (137 patients). Moreover, most of our patients had H and Y staging less than 3.
Conclusion
It could be concluded that VDR FokI and ApaI genotypes are related to clinical presentations rather than etiology or severity of idiopathic PD. Future studies including larger sample size and different stages of PD are recommended for more clarification of the potential role of VDR polymorphisms in the pathogenesis and progression of PD, which may suggest new management strategies to slow the progression of the disease.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to current Cairo University regulations and Egyptian legislation but are available from the corresponding author on reasonable request and after institutional approval.
Abbreviations
- ADL:
-
Activities of daily living
- H and Y:
-
Hoehn and Yahr staging
- PCR:
-
Polymerase chain reaction
- PD:
-
Parkinson disease
- UPDRS:
-
Unified Parkinson Disease Rating Scale
- VDR:
-
Vitamin D receptor
References
Morello M, Pieri M, Zenobi R, Talamo A, Stephan D, Landel V, et al. The influence of vitamin D on neurodegeneration and neurological disorders: a rationale for its physio-pathological actions. Current pharmaceutical design. 2020;26(21):2475–91. https://doi.org/10.2174/1381612826666200316145725.
Taymans SE, Pack S, Pak E, Orban Z, Barsony J, Zhuang Z, et al. The Human vitamin D receptor gene (VDR) is localized to region 12cen-q12 by fluorescent in situ hybridization and radiation hybrid mapping: genetic and physical VDR map. J Bone Miner Res. 1999;14(7):1163–6. https://doi.org/10.1359/jbmr.1999.14.7.1163.
Niu MY, Wang L, Xie AM. ApaI, BsmI, FokI, and TaqI polymorphisms in the vitamin D receptor gene and Parkinson’s disease. Chin Med J. 2015;128(13):1809–14. https://doi.org/10.4103/0366-6999.159358.
Butler MW, Burt A, Edwards TL, Zuchner S, Scott WK, Martin ER, et al. Vitamin D receptor gene as a candidate gene for Parkinson disease. Ann Hum Genet. 2011;75(2):201–10. https://doi.org/10.1111/j.1469-1809.2010.00631.x.
Lv Z, Tang B, Sun Q, Yan X, Guo J. Association study between vitamin d receptor gene polymorphisms and patients with Parkinson disease in Chinese Han population. Int J Neurosci. 2012;123(1):60–4. https://doi.org/10.3109/00207454.2012.726669.
Török R, Török N, Szalardy L, Plangar I, Szolnoki Z, Somogyvari F, et al. Association of vitamin D receptor gene polymorphisms and Parkinson's disease in Hungarians. Neurosci Lett. 2013;551:70–4. https://doi.org/10.1016/j.neulet.2013.07.014.
Lin CH, Chen KH, Chen ML, Lin HI, Wu RM. Vitamin D receptor genetic variants and Parkinson's disease in a Taiwanese population. Neurobiol Aging. 2014;35(5):1212–e11.
Lv L, Tan X, Peng X, Bai R, Xiao Q, Zou T, et al. The relationships of vitamin D, vitamin D receptor gene polymorphisms, and vitamin D supplementation with Parkinson’s disease. Transl Neurodegener. 2020;9(1):1–3.
Gao J, Teng J, Liu Z, Cai M, Xie A. Association between vitamin D receptor polymorphisms and susceptibility to Parkinson's disease: an updated meta-analysis. Neurosci Lett. 2020;720:134778. https://doi.org/10.1016/j.neulet.2020.134778.
Fahn S. Members of the UPDRS development committee. Unified Parkinson’s disease rating scale. Recent Dev Parkinson’s Dis. 1987;2:293–304.
Goetz CG, Tilley BC, Shaftman SR, Stebbins GT, Fahn S, Martinez-Martin P, et al. Movement Disorder Society- sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–70.
Petersen MS, Bech S, Christiansen DH, Schmedes AV, Halling J. The role of vitamin D levels and vitamin D receptor polymorphism on Parkinson's disease in the Faroe Islands. Neurosci Lett. 2014;561:74–9. https://doi.org/10.1016/j.neulet.2013.12.053.
Gezen-Ak D, Alaylıoğlu M, Genç G, Gündüz A, Candaş E, Bilgiç B, et al. GC and VDR SNPs and vitamin D levels in Parkinson’s disease: the relevance to clinical features. Neuromolecular Med. 2017;19(1):24–40. https://doi.org/10.1007/s12017-016-8415-9.
Han X, Xue L, Li Y, Chen B, Xie A. Vitamin D receptor gene polymorphism and its association with Parkinson's disease in Chinese Han population. Neurosci Lett. 2012;525(1):29–33. https://doi.org/10.1016/j.neulet.2012.07.033.
Suzuki M, Yoshioka M, Hashimoto M, Murakami M, Kawasaki K, Noya M, et al. 25hydroxyvitamin D, vitamin D receptor gene polymorphisms, and severity of Parkinson's disease. Mov Disord. 2012;27(2):264–71. https://doi.org/10.1002/mds.24016.
Acknowledgements
The authors acknowledge subjects for their participation and cooperation in this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
EMF: research idea and conception, data acquisition, data analysis and interpretation, and manuscript writing and reviewing. MEE: research idea, data acquisition, data analysis, and interpretation. SS: performing and reviewing the laboratory workup. SH: data acquisition, data analysis, and interpretation. RSI: data acquisition, data analysis and data interpretation, and manuscript writing and reviewing. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The aim and procedures of the study were explained to every participant and an informed written consent was obtained from all participants before being enrolled in the study. The study was approved by the ethical committee of the Neurology Department, Cairo University Hospitals (4/3/2017).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fahmy, E.M., Elawady, M.E., Sharaf, S. et al. Vitamin D receptor gene polymorphisms and idiopathic Parkinson disease: an Egyptian study. Egypt J Neurol Psychiatry Neurosurg 57, 102 (2021). https://doi.org/10.1186/s41983-021-00358-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-021-00358-5