
Abstract
Background
Human face is complex and intricate structure, with several features that are unique to each individual and can be taken as an identity pass in this mortal world. The facial profile of an individual holds materialistic value and is crucial for human identification. Present study aims to investigate the influence of sex and age of an individual on the soft tissue thicknesses (FSTT) at midline facial landmarks estimated on MRI scans.
Methods
Facial soft tissue thickness was estimated at 20 midline landmarks on the MRI scans of 120 (57 male; 63 female) anatomically normal Northwest Indian adult subjects (18–70 + years age-group). Age and sex dependent variations in tissue thicknesses at different landmarks were estimated using statistical software IBM SPSS Statistics 23.
Results
The results of the study yielded that most of the midline landmarks had higher values in males than in females indicating observable sexual dimorphism in FSTT values in this facial region, statistically significant differences were also noted in soft tissue thickness estimates of different age-groups, showing increasing or decreasing trend with age. The mid-facial landmarks like mid-philtrum, supra-dentale, incisor superius, and labile inferius displayed highly significant p values.
Conclusions
Present study results were in tandem with the findings of previous studies; males and younger age-group individuals were having higher tissue thickness values than the females and older individuals, respectively. The highest soft tissue estimates were obtained for the middle age subjects and the most aged individuals had the least midline soft tissue thickness values. These results can have significant forensic anthropological repercussions in attempting facial approximations on unknown skulls and identification of unknown individuals from still images, photographs or videos.
Similar content being viewed by others


Background
The human face, the key aspect of an individual’s identity, has long captivated the imagination of forensic investigators. Face prediction from an unknown skull is a widely accepted forensic investigation tool, used in situations when identification of skeletonized human remains from other means becomes very difficult (if not impossible). Facial approximation is a method to recreate likeness of an individualistic face based on application/knowledge of tissue thicknesses, cranial dimensions, musculature design, and the overlying skin layers. Forensic anthropologists utilize the standard methods and techniques formulated/developed in physical anthropology for the identification of such unidentified human remains (Ubelaker et al. 2019). Over time, the role of forensic anthropologists has become crucial in identification of deceased from the sites of mass disasters, natural calamities, war or war-related conflicts, terrorist massacres, or political genocide etc., where heaps of unidentified cadavers or skeletal remains have been reported (Krogman and Iscan 1986). Forensic anthropologists utilize a variety of methods from their armament towards human identification strategies, especially when the primary identification methods like dactyloscopy, odontological comparisons, and DNA profiling fail to identify individuals, either due to lack of antemortem information or inability to perform DNA analysis owing to contamination and severe putrefaction of the body (De Greef et al. 2006; Starbuck and Ward 2007). Under all such circumstances, forensic facial approximation comes to the rescue of forensic anthropologists to prevent the inadequacy among the league of conventional methods (Wilkinson 2008).
Facial approximation technique relies upon the anatomical knowledge about one of the most important biological structures of the human body, i.e., face. Forensic anthropologists need to have an understanding of various cranial characteristics and average facial soft tissue thickness values to obtain accurate facial approximations. Facial features of the individuals belonging to a particular region are considered to be the manifestations of interactions between genetical and environmental characteristics available to them (Wilkinson et al. 2006).
The study of facial soft tissue thickness becomes an important aspect that aids in the understanding of craniofacial characteristics of various populations and contributes to the accuracy of the resultant facial approximation models (Panenkova et al. 2012; Lodha et al. 2016). To achieve more accurate facial appearance, a link is established between facial soft tissue, starting from the surface of the skin to the most superficial surface of the underlying bone using predefined anthropological landmarks. Factors such as age, sex, BMI, ponderal status, population of origin, corpulence, dietary status, disease condition, physical activity, obesity status, as well as ecological, geographical, racial, and habitual conditions of an individual can significantly influence the facial soft tissue estimates and the complex anatomy of facial skeleton (Rhine and Campbell 1980; Wilkinson 2005; De Greef et al. 2006; Domaracki and Stephan 2006; Ruiz 2013). These differences necessitate the establishment of normative values of tissue depth standards for the individuals of two sexes and belonging to different population and age-groups to enable efficient forensic facial approximations.
In the contemporary world, every other person is adamant about becoming a part of the latest facial aesthetic trend. The lack of definitive facial beauty standards around the globe demands an in-depth facial analysis for undertaking simple orthodontic treatments to special reconstructive procedures of the face (Bazmi and Zahir 2013). Professionals preoccupied with facial aesthetics are concerned with different diagnostic and treatment planning. But greater reliance and emphasis on soft tissue estimates remain the same among orthodontists to maxillofacial surgeons (Auger and Turley 1999; Bashour 2006; Naini et al. 2006; Bazmi and Zahir 2013). Having access to reference data can have a beneficial influence on multiple disciplines. From plastic surgeons treating craniofacial deformities to forensic scientists undertaking the task of facial reconstruction. The knowledge of facial soft tissue thickness can also be useful for accurate portraying of the historically significant figures or d remodelling the archaeological samples for the purpose of facial approximation of the such unidentified individuals (Lee and Shin 2020; Lee et al. 2020). Facial soft tissue thickness data along with virtual anthropology tools can help locate the missing data for approximation and the process of human facial recognition (Guyomarc'h et al. 2018; Coutinho-Nogueira et al. 2019; de Moraes et al. 2022). The knowledge of facial soft tissue thickness is not only useful for developing facial recognition systems but it is also useful for locating in-depth penetration of malignant or non-malignant facial tumors, non-ablative dermal laser therapy, and establishment of dento-facial physiognomies. The FSTT estimations are crucially useful not only for forensic anthropologists performing craniofacial identifications but also to the experts of diverse medical and dental disciplines like maxillofacial surgeons, orthodontists, plastic surgeons, anatomists, orthopedicians, ophthalmologists, otolaryngologists, and dermatologists who work with facial anatomies of their subjects on almost daily basis (Kaur et al. 2017).
Owing to technological advancements over the past few decades, numerous techniques have been devised to measure facial soft tissue thickness. Different techniques have come into the picture which may vary from direct measurement methods like knife puncture and needle puncture to indirect measurement methods involving digital imaging techniques such as radiographs, ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), and cone-beam computed tomography (CBCT) (Guyomarc’h et al. 2012; Sipahiolu et al. 2012; De Donno et al. 2019; Gietzen et al. 2019; Meundi and David 2019). However, all methods used for estimating soft tissue thickness have a fair share of advantages and disadvantages. While invasive and earlier techniques like needle puncture are better suited for measuring cadavers whereas modern non-invasive techniques provide in vivo consistent and robust facial soft tissue thickness data.
To avoid the risk of radiation exposure, non-ionizing imaging techniques such as ultrasound and magnetic resonance imaging (MRI) provide a safer alternative for obtaining soft tissue estimates. Although in ultrasound, tissue compression is possible and difficulties in scanning a surface parallel to a skeletal surface can pose a challenge in visualizing a surface.
Many studies reported that the greater accuracy offered by MRI makes it a promising technique for determining facial soft tissue depths measurements as compared to other methods (Sahni et al. 2002, 2008). MRI is one such modality that is not only being widely used for clinal diagnosis but also offers a wide range of applications for forensic purposes. It can be used for forensic anthropological identifications, craniofacial trauma analyses, facial soft tissue depth estimations, and post-mortem MRI (PMMR) to name a few (Bolliger and Thali 2015).
MRI-based soft tissue estimates with reproducible, accurate, and hazardless characteristics involve the possibility of creating large soft tissue datasets (Hillewig et al. 2013). Besides, MRI offers a high spatial resolution of soft tissues with good contrast and non-compression of soft tissues during measurement. For evaluation of facial soft tissue estimates, among the non-invasive and no-contact methods, the use of MRI was specifically initiated in forensics to do away with the shortcomings of CT (Khatri et al. 2017). As MRI offers a greater accuracy factor than CT images for obtaining soft tissue depths (Aulsebrook et al. 1995). Besides, a detailed depiction of muscular atrophies and soft tissue with structural features can be generated through MRI. As a radiological modality, MRI allows for greater virtual- manipulation, simulation, and segmentation of the bone whilst preservation. Key favourable features like lack of direct contact and no risk of radiation exposure make MRI a promising tool for carrying out the daunting task of forensic identification. Thus, making the images ethically acceptable for determining the soft tissue depths.
Globally, numerous studies have been conducted to create a soft tissue thickness database for different ethnicities. Traces of population-specific identities are manifested in soft and hard tissues as anthropological differences (Gupta et al. 2015). Hence, facial soft tissue estimates play an instrumental role for both clinical and scientific purposes. But for the purpose of craniofacial approximation soft tissue estimates present an instrumental role. The present study will contribute to the development of a more standardized approach for undertaking forensic facial approximation with greater accuracy and reliability in forensic investigations.
Therefore, the study of age and sex-dependent variation in midline facial soft tissue thickness estimates measured on MRI scans of Northwest Indian subjects have a consequential impact for the purpose of craniofacial approximation. The present study sample has a diverse population background and aims to establish normative values for the midline facial soft tissue thickness estimates for both the sexes. The use of MRI scans as the radiologic modality in the study provides allows for establishing an accurate and comprehensive method for understanding the variation in facial soft tissue thickness in the population under study. The study aims to contribute to the knowledge pool of human facial soft tissue depth standards by investigating the Northwest Indian population for different midline anatomical landmarks in both sexes using MRI scans. The main objectives of the study included:
-
To estimate age and sex-dependent variations among different midline facial soft tissue estimates.
-
To highlight age-related changes (facial aging) in soft tissue thickness at various midline facial landmarks.
-
To compare the results of the present study with other national and international studies.
Methods
Sampling strategy
The present study was conducted to estimate the average values of facial soft tissue thickness at universally defined twenty mid-line facial landmarks of Northwest Indian adult individuals with a purpose to quantify age- and sex-related differences in the tissue thicknesses at these landmarks. For this purpose, present study considered the MRI scans of 120 Northwest Indian (57 males and 63 females) adults between the age range of 18–70 + years.
The individuals included in present study were referred by their doctors for MRI scanning of the brain/head region due to certain diagnostic and therapeutic reasons like prolonged headache or migraine as the causal concerns. For this purpose, the consultant radiologists at the Atulya Healthcares and Radiodiagnostic Center, Chandigarh (India), helped in recruiting the ‘anatomically normal’ individuals for this study prior to their MRI scan, through their voluntary participation in the study who reported to the diagnostic centre at their own for scanning of their head/face region as advised by their treating physician. The radiologist helped in reviewing the MRI records of the potential participants and excluded any case that did not meet the inclusion criteria of the present study and it was continued until a sample size of 120 MRI scans of anatomically normal individuals was obtained.
The selection criteria focused on including MRI scans of only those individuals who were interpreted as anatomically ‘normal’. The term ‘anatomically normal’ means those individuals who having normal facial contour/anatomy, having no major facial anomalies or deformities that could affect the facial soft tissue thickness estimations. The exclusion criteria focused on identifying individuals having any gross maxillo-facial disfigurements, post-operative head or orthodontic injuries, skin oedema, soft tissue masses, soft tissue trauma. congenital or pathological abnormal face profile or having some facial metallic implants (surgical) were ignored for inclusion in this study. Besides, individuals associated with certain occupation or anything leading to gross facial disfigurement were not included in this study. Such cases were continuously excluded according to the exclusion criteria until the targeted sample size of 120 MRI scans was fulfilled Table 1.
Imaging and data analysis process
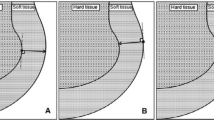
For each participant, a similar pre-structured proforma was maintained consisting of age, sex, and midline facial soft tissue thickness estimates at pre-defined facial landmarks. These soft tissue thickness estimates were measured as the distance between specific landmarks on the bone relative to the surface of the soft tissue part visible on each scan. As the hard tissue is visible as a thin dark line and the overlying soft tissue appears bright, making the task of measuring the superficial soft tissue thickness possible by differentiating between them.
The T1-weighted sagittal images were used to measure the 20 craniofacial midline landmarks on the MRI scans of each subject. MPR sequence was used for this purpose, as it shows good anatomical details and fat tissue. These T1 weighted images were obtained in Digital Imaging and Communications in Medicine (DICOM) format for each participant. The tissue thickness estimates were obtained using Osirix software. The positioning of the midline landmarks was selected on MRI scans of each subject on the basis of the standard definitions as listed in Table 2. (Kolar and Salter 1997; Frakas 1981; Buikstra and Ubelaker 1994; Farkas et al. 2002; Wilkinson 2004). Subject positioning can impact the imaging process as the position of the head and body of subjects can have direct bearing on the MRI scans which can in turn effect the soft tissue thickness values. Therefore, all the MRI scans obtained for this study were taken in the supine position. The subjects were lying on their backs with their heads oriented in in such a way that they were looking straight up so that their Frankfurt horizontal plane (FH plane) was oriented approximately vertically. Such a positioning ensured that the facial soft tissue thickness don’t get distorted under the influence of gravity. The subjects were also instructed to maintain a relaxed facial expression with eyes and mouth naturally closed during the imaging process.
Measurement process
During the analysis, measurements on about 20 midline points were taken on the mid-sagittal plane. As mentioned earlier, FSTT is the distance between the landmarks on the bone relative to the surface of the soft tissue. The required bony landmark is located on the hard tissue and then a perpendicular line from the bony landmark is extended outwards to meet the corresponding facial skin surface. The length of the perpendicular line from the bone to the junction with the skin surface will be regarded as the equivalent FSTT of that landmark. The FSTT value recorded is the Euclidean distance between the bony landmark and its homologous cutaneous landmark (Sandamini et al. 2018). In case of landmarks where it was difficult to take measurements perpendicular to bone, the direct method was used, i.e., it measures a distance between one point on bone and the other point on skin. The midline facial landmarks were selected keeping in mind the facial mid-sagittal section and the reliable positioning of these chosen landmarks on the MRI scans. Furthermore, the midline landmarks were selected based on the previous facial radio-imaging studies. The MRI scans of the subjects were later on divided by sex into four age groups as group 1 (18 to 34 years), group 2 (35 to 45 years), group 3 (46 to 55 years), and group 4 (56 years and above).
Imaging specifications
The MRI scans of the subjects were obtained on Siemens Espree 1.5 T wide bore whole body MR Scanner, ‘Magnetom Espree’ with the FoV (Field of view) = 230–250, TR (Total resolution) = 1390–10,000 ms, Matrix = 256 × 256, Slice thickness = 1 mm, TE (total enhancement) = 219 ms, Slabs = 70–90, slices/slab = 75 to 90, Distance factor (difference between per slab) = 50% (MRI Scanner) Somatom Definitions 64 Dual Source.
Statistical analysis
The data obtained from 120 MRI scans were organized in an excel spreadsheet and descriptive statistical analysis was performed like mean, standard deviation, independent t-test for establishing a reliability level of 95% using IBM SPSS Statistics 23. ANOVA was used to compare the mean values between sexes and age groups. Pearson correlation coefficient ‘r’ was computed to determine the effect size of the sample. Inter and intra observer error was calculated for each midline facial soft tissue estimate. This paper attempts to present a table of average facial soft tissue thickness as measured using MRI images along with age-related changes and sexual differences. Although, an attempt has been made to determine the relationship between age and sexual dimorphism with facial parameters.
Results
The facial soft tissue thickness was measured at well-defined midline facial landmarks on the MRI scans (Fig. 1 generated using Radiant Viewer Software). The results of the present study are presented in Tables 3, 4, 5, 6, 7, and 8 and diagrammatically represented in Figs. 2, 3, and 4. The results presented in Table 4 show the mean tissue thickness estimated in two sexes from midline landmarks using MRI scan as the imaging modality. It was found that almost all craniofacial variables showcased evidently visible sexual dimorphism. General descriptive statistics were computed for each landmark, and the differences between mean values for males and females were compared using an independent t test. Among all the variables considered, statistically significant sex-specific differences were found in tissue thickness measurements in pooled aged groups at 17 anatomical points on MRI images. Majority of these mid-facial landmarks displayed highly significant sexual dimorphism between the sexes. On average, male subjects had greater soft-tissue thickness at almost all points which can be attributed to the inherent difference in the skull morphology between both the sexes. Each measurement was repeated three times and their average value was taken as the FSTT value. For estimating the inter and intra observer errors, the tissue thickness values were estimated at different times, respectively. No significant error was found in any of these two types of observations. The MRI scans taken from the single instrument were used for estimating the facial soft tissue thickness estimates. The Pearson correlation coefficient ‘r’ was computed to determine the effect size of the samples with respect to the relationship between different facial soft tissue thickness estimates (Table 9). The correlations were moderate to strong when it came to most of the midline facial landmarks. But relatively lower correlations were mainly found in the mid-facial region suggesting relative ambiguity in the soft tissue thickness in these regions. The results suggest that facial soft tissue thickness generally are influenced by similar types of genetic or environmental factors.

Facial soft tissue thickness measured at different anatomical landmarks on the midsagittal section of MRI scan of 68 years old male subject

Tissue depth mean values for males and females: a between males and females

One-way ANOVA analysis of facial soft tissue variation between four-age groups of females

One-way ANOVA analysis of facial soft tissue variation between four-age groups of males
The midline facial soft tissue thickness values of 120 individuals of both sexes were categorized into four age groups based on their midline values. The calculated mean, standard deviation, maximum, minimum, and ranges of the estimated midline points are shown in Tables 10, and 11, 12. It is evident from these tables that the average midline soft tissue thickness estimates for both males and females are greater in groups 1 and 3. Group 4 estimates of midline soft tissue thickness, however, justifies that with increasing age the soft tissue thickness values shows a decreasing trend. Furthermore, it is evident from the current data that the facial soft tissue thickness estimates for the mid-face region are greater than those for the upper face. The alternating increasing and decreasing pattern with facial soft tissue thickness estimates among the four-age groups could be due to the variation in deposition of fat with aging.
To compare the estimates of midline soft tissue thickness between the four age groups, a one-way ANOVA test was conducted on both sexes. These results indicate that there is a direct correlation between the midline facial soft tissue estimates and increasing age in females. Especially, as displayed by mid-facial midline landmarks like mid-philtrum, supra-dentale, incisor superius, labile superius and labile inferius with significant p-values. In males, except for six, significant p-values were obtained for the majority of midline landmarks. Despite this, only pronasale landmark displayed a highly significant result.
In the present study, it was possible to identify age-related differences that were consistent across male and female age groups. Female facial soft tissue values tend to exhibit an alternating increasing and decreasing pattern with age. Except for landmarks like subnasale and mid-philtrum, the majority of the midfacial landmarks exhibited alternatingly increasing FSTT values, with group 4 exhibiting the lowest mean values. On the other hand, in case of males, the mean values for most of the midline facial soft tissue thickness tended to thicken with age and then decrease for the samples of group 4. For both male and female subjects, group 3 had the thickest values for the majority of landmarks, indicating that middle-aged people have the thickest FSST values. In contrast, group 4 had the lowest values, indicating that the majority of midline landmarks tend to thin with age. These differences could not be directly correlated with age but perhaps be an impact of BMI-related changes.
Discussion
The creation of a facial soft tissue database offers a wide range of practical applications beyond the expertise of forensic anthropologists. Having access to such a database can have a multitude of applications for biological and medical fields such as forensic, anthropology, archaeology, cosmetic surgery, oral medicine, orthodontic treatment, and various other diagnostic purposes (Wang et al. 2016). Facial soft tissue thickness varies due to number of factors like age, sex, ancestry, nutritional status, BMI, etc. In the present study, the focus was on determining the effect of age and sex on the midline facial soft tissue thickness of the Northwest Indian subjects. Our facial morphology is an amalgamation of complex interaction between the inherited and environmental factors. Considering the diverse background of India and its population, numerous variations can be seen among the people belonging to different regions of the country.
The FSTT values obtained in the present study were compared with other studies conducted on different populations as well as a similar population sample. Due to the difference in ethnicity, the data obtained from other international studies cannot be used for forensic facial approximation purpose of the native Indian population. However, the technique employed and data classification method are significant. Comparing the Northwest Indian population of the past with that of the present generates useful information due to the similarity of the two populations. The prevalence of higher FSTT values in males compared to females was the prevalent finding across all studies compared to the results of the present study. This sexual dimorphism was verified with the presence of statistically significant difference between the midline facial soft tissue thickness values of the present study as well.
Two MRI studies on the same heterogeneous populations sample of Northwest Indian subjects have been reported (Sahni et al. 2002, 2008). In a preliminary MRI-based study of 60 Northwest Indian subjects, Sahni et al. (2002) discovered statistically significant sex and side differences in facial tissue thickness at specific landmarks. In 2008, Sahni et al. measured FSTT at 29 standard anthropological landmarks of 300 MRI scans (173 males and 127 female) and found a significant correlation between body mass index (BMI) and FSTT in both sexes. When the midline values of the present study were compared to the previous Northwest Indian study, the mid-philtrum proved to be the distinguishing factor between the two. Previous Northwest Indian study produced higher values for mid-philtrum, supragnathion, and gnathion midline landmarks in both sexes. Among females, however, there were additional exceptions for the soft tissue values of the nasion, mid-philtrum, labile superius, and labile inferious. Sahni et al (2008) reported a significant correlation between BMI and FSTT values among the individuals of two sexes belonging to the geographical area considered in present study. Such a correlation was also investigated among the individuals of present study; however, its discussion is beyond the scope of this article and will be communicated later on separately.
Chen et al. (2011) estimated craniofacial soft tissue thickness and nasal profile of 425 Chinese adults of the Han population between the age range of 17–60 years using MRI scans. In the upright position (following the Frankfurt Horizontal plane), MRI images were acquired at 31 anatomical landmarks and 4 nasal profile parameters. The study revealed that males had significantly higher FSTT values than females at the majority of landmarks. Males and females exhibited a highly significant correlation between nasal profile and nasal measurements. Both characteristics demonstrated a significant correlation with age, which has important implications for forensic identification. In both the sexes, the average values of soft tissue thickness at almost all the points in the Chinese Han population were found to be lower than the present study. Except for midfacial landmarks like subnasale, labile superius, labile inferius, and supramentale where Han population exhibited greater values in comparison to present study. In females, additional exceptions were demonstrated by the rhinion landmark, where both populations displayed equal values, and the mid-philtrum, where Han values were higher than present study values.
Eftekhari-Moghadham et al. (2020) investigated the facial soft tissue thickness estimates of the Lur and Arab population of southwest Iran. This cross-sectional study was conducted on 100 Iranian adults between the ages of 18 and 50. Using certain sagittal, axial, and coronal sections of the MRI images, soft tissue thickness estimates were calculated. Utilizing Stata 14 software, the statistical analysis was evaluated. This study revealed a significant correlation between estimates of soft tissue thickness and other parameters such as gender, BMI, and ethnicity in Southwest Iran. This study also identifies the Mid-philtrum (MID) as a distinguishing feature of the male sex. In addition, when the results of South-west Iranian samples were compared to those of the present study, with the exception of mid-philtrum, labile superius, labile inferius, supramentale, and supragnathion, all other FSTT values were higher in the present study sample.
Sipahiolu et al. (Sipahioğlu et al. 2012) measured nine midline points to determine the age-related variation in the soft tissue thickness values of both sexes. The measurement analysis revealed that age-related changes were observed at four midline points in males. Age-related thickening of soft tissues in females was only statistically significant at the mental eminence. In addition, the Turkish population with varying BMIs has statistically significant thicknesses at four midline facial points, namely the glabella, nasal end, mental eminence, and beneath the chin.
Johari et al. (2017) investigated the facial soft tissue thickness estimations of Iranian adults aged 18 to 76 years. They measured 12 landmark points in the midline region of 179 participants. These statistically significant differences were examined using the Mann–Whitney and Kruskal-Willis tests. According to the study, for the majority of landmarks, males tend to have greater soft tissue thickness values than females. It was found that in normal-weight and overweight groups, a significant difference was found in all landmarks as soft tissue thickness displayed a positive correlation with BMI. The rise in BMI values in Iranian population was linked with subsequent increase in soft tissue thickness values indicating a significant relationship between the soft tissue thickness values and BMI.
Sandamini et al. (2018) measured 23 anthropological landmarks on adult Sri Lankans using MRI images. For this study, 223 MRIs and 20 MRIs of volume were collected from subjects aged 20 to 59. The gender-based analysis of this study revealed that men have higher FSTT values than women in the midline region. However, the area around the cheeks shows comparatively higher soft tissue values in young women than in young men.
It is pertinent to state that all the studies included in the present research focused on scanning the subjects in the supine position. Although, much research has been conducted with the subjects in the supine position, we cannot deny the affect it has on the facial soft tissues due to the gravity. To justify this statement, a few different lines of evidence need to be considered. Among these, the anatomical reasons happen to be the foremost important which suggests that gravity could have an impact on facial tissues during scanning. In upright or standing position, facial soft tissue thickness is oriented under the impact of gravity in a particular direction. However, in supine position, the direction of gravity has the potential to shift the tissue or settle them in a different direction. Some researchers have investigated the impact of body position on facial appearance and a few of them have been listed.
Bulut et al. (2017) compared the facial morphology of live subjects obtained with the help of 3D scanners in upright and supine positions. Data of 3D face scans were collected using 3D Laser scanner in upright and supine position from 44 volunteers aged 22–49 years with normal BMI index. Volumetric analysis of the obtained face scan was done by 3D morphometric surface comparison between upright and supine position. Keeping upright position as reference frame surface to surface comparison was performed which resulted in a continuous color map. The study showed that change in pose produces 2–10 mm soft tissue thickness variations around the buccal region, masseteric region and the nasolabial region of the face. Finally concluding that 84% of the face being within ± 2 mm of error between the supine and upright 3D surfaces and thereby the data collected in supine positions are acceptable within minimal error.
Stephan and Preisler, (2018) study provided the in vivo facial soft tissue standards for adult Australians of European origin. Facial soft tissue data was collected from 64 living adult Australians using B-mode ultrasound system at 14 anatomical landmarks along with details of height, weight, and BMI index. The data was further categorized into two sub groups, group one having 52 subjects aged 18–30 years (excluding one subject due to extremely large BMI) and group two having 11 subjects aged 37–74 years. The measurements were taken in both upright and supine positions. For reference 6, previous facial soft tissue thickness data sets of adult Australian cadavers were collected which were measured using needle-puncture method. The results showed that the in vivo ultrasound data are like needle puncture data on cadavers but high measurement errors in both the cases. Posture effect did not exist in terms of significance except only two landmarks which exhibited a > 1 mm change with highest variations in mid-ramus landmarks. The posture did not show the different between positions of data collection but the values vary with the method of measurement adopted.
Finally, it is worth mentioning that many imaging studies do take body position into account when analyzing facial soft tissue thickness estimates. But this impacts the facial asymmetry related features more which is beyond the scope of the present study. The studies mentioned above also indicate that error range between the supine and upright position is within the minimal error range.
The relationship between soft tissue thickness and skull size, has not been explored in the present study. But it is important to mention that few population-specific factors like hormonal, genetic, nutritional and environmental/climatic differences may affect the skull size in males and females differentially, along with the facial soft tissue thickness estimates in two sexes. Future research should focus on exploring the relationship between skull size and FSTT values in both the sexes.
Although MRI is a costly imaging modality, it provides excellent anatomical characteristics for distinguishing between the soft tissue and hard tissue details of various organs being imaged. MRI's use in obtaining a database based on the thickness of facial soft tissue is limited due to the time take procedure and high cost involved. All these factors contribute to the paucity of existing literature on facial soft tissue thickness databases based on MRI. In most forensic cases where only the skull is retrieved from the site, though MRI is not the technique that can be utilized for digitalising the bone, as CT scans or surface scanning (laser grammetry and photogrammetry) are the preferable and accurate techniques to undertake this task, however, it can contribute towards facial approximation of such unknown skull/s to provide investigative leads in the case. Secondly, MRI technique is costly one compared to other radio-diagnostic modalities and is used in some exceptional cases only.
Consequently, it can be concluded that the results of the present study are consistent with the findings of other studies indicating that the FSTT values of males tend to be higher than those of females at nearly all points. Rhinion yielded the thinnest values, whereas pogonion yielded the thickest values for both sexes. The present Northwest Indian samples had the thickest soft tissue measurement in the mid-face region. The absence of information regarding the subjects’ BMI is the only limitation of this study. Differences in the values of soft tissue thickness when compared to other studies can be attributed to the population-specific or secular changes that have occurred over time.
To successfully apply facial soft tissue thickness for facial recognition, population-specific tissue depth standards are required. Therefore, future research should include a larger sample size and take into account confounding factors such as BMI, bilateral landmarks, nutrition status, and facial skeletal type to determine the effect of these variables on facial soft tissue depth estimates.
Conclusions
With the development of technology, the forensic facial approximation techniques have also evolved overtime. The advent of newer radio-imaging techniques has made the task of estimating facial soft tissue thickness albeit a less tedious task than before. The present study was conducted with the aim of evaluating and determining the facial soft tissue thickness estimates of Northwest Indian population while highlighting the age-related and sex-related changes in the soft tissue thickness values. The results of the present study were in tandem with the findings of previous studies. It was observed from the present samples that males presented higher soft tissue estimates than females. Furthermore, highest soft tissue estimates were obtained for the middle age people. The group 4 cases, the most aged individuals group, had the least midline soft tissue thickness values.
The significance of such a database lies in understanding the facial characteristics of the Northwest Indian population and might be potentially helpful in the forensic facial approximation process. As a result of secular change over time, the midline facial landmarks estimated in the present study demonstrate greater tissue depth standards compared to previous research conducted on the same population pool. However, the role of other factors like changes in nutritional status, climatic factors, BMI and aesthetic treatments in the FSTT variations cannot be ruled out and thus needs to be further investigated with larger dataset.
In addition to forensic anthropology, the facial soft tissue thickness values obtained in the present study may have a variety of other applications. It may be useful not only for forensic anthropologists performing craniofacial identifications, but also for experts from a variety of medical and dental disciplines who interact with the facial anatomies of their subject on regular basis for delivering facial aesthetic or medical care to their subjects through the means of facial profile manipulation. The way forward is to conduct a comprehensive study based on facial soft tissue estimates for the Indian population. Hence, further research in the field must be encouraged so as to build database of soft tissue estimates that can be correlated with other radio-imaging modalities-based studies to develop acceptable standards.
Availability of data and materials
Data and material used in present manuscript are available with the corresponding author and can be obtained via email.
Abbreviations
- BMI:
-
Body mass index
- CT:
-
Computed tomography
- CBCT:
-
Cone-beam computed tomography
- DICOM:
-
Digital Imaging and Communications in Medicine
- FoV:
-
Field of view
- FSST:
-
Facial soft tissue-thickness
- MID:
-
Mid-philtrum
- MRI:
-
Magnetic resonance imaging
- PMMR:
-
Post-mortem MRI
- TR:
-
Total resolution
References
Auger TA, Turley PK (1999) The female soft tissue profile as presented in fashion magazines during the 1900s: a photographic analysis. Int J Adult Orthodon Orthognath Surg 14(1):7–18
Aulsebrook WA (1995) Superimposition and reconstruction in forensic facial identification: a survey. Forensic Sci Int 75:101–120
Bashour M (2006) History and current concepts in the analysis of facial attractiveness. Plast Reconstr Surg 118(3):741–756
Bazmi B, Zahir S (2013) A cross-sectional study of soft tissue facial morphometry in children of West Bengal. ContempClin Dentistry 4(1):42–47. https://doi.org/10.4103/0976-237X.111613
Bolliger SA, Thali MJ (2015) Imaging and virtual autopsy: looking back and forward. Philos Transact R Soc B: Biol Sci 370(1674):20140253
Buikstra JE, Ubelaker DH (1994) Standards for Data Collection from Human Skeletal Remains, Proceedings of a Seminar at The Field Museum of Natural History (Arkansas Archeological Survey Research Series No. 44). Spiral ed. Arkansas Archeological Survey, Fayetteville
Bulut O, Liu C-YJ, Koca F, Wilkinson C (2017) Comparison of three-dimensional facial morphology between upright and supine positions employing three-dimensional scanner from live subjects. Leg Med 27:32–37
Chen F, Chen Y, Yu Y, Qiang Y, Liu M, Fulton D, Chen T (2011) Age and sex related measurement of craniofacial soft tissue thickness and nasal profile in the Chinese population. Forensic Sci Int 212(1–3):272.e1–272.e6. https://doi.org/10.1016/j.forsciint.2011.05.027
Coutinho Nogueira D, Dutailly B, Comte F, Vasil’iev A, Khokhlov A, Shvedchikova T, Berezina N, Buzhilova A, Dutour O, Coqueugniot H (2019) “Gueule cassée”(facial injuries): a 3D paleotraumatology study and facial approximation of a Napoleonic soldier who died in 1812 at Königsberg during the Russian Campaign. Int J Osteoarchaeol 29(2):191–197
De Donno A, Sablone S, Lauretti C, Mele F, Martini A, Introna F, Santoro V (2019) Facial approximation: Soft tissue thickness values for Caucasian males using cone beam computer tomography. Leg Med 37:49–53
De Greef S, Claes P, Vandermeulen D, Mollemans W, Suetens P, Willems G (2006) Large-scale in-vivo Caucasian facial soft tissue thickness database for craniofacial reconstruction. Forensic Sci Int. 159(1). https://doi.org/10.1016/j.forsciint.2006.02.034
de Moraes JK, Baldasso RP, Gonçalves ÁP, Beux L, Fernandes MM, Strapasson RAP (2022) Two-dimensional facial approximation: facial composite and digital 3D facial approximation techniques applied on cone-beam tomography. Conjecturas 22(7):183–199
Domaracki M, Stephan CN (2006) Facial soft tissue thicknesses in Australian adult cadavers. J Forensic Sci 51(1):5–10
Eftekhari-Moghadam AR, Latifi SM, Nazifi HR, Rezaian J (2020) Influence of sex and body mass index on facial soft tissue thickness measurements in an adult population of southwest of Iran. Surg Radiol Anat 42(5):627–633
Farkas LG, Tompson BD, Katic MJ, Forrest CR (2002) Differences between direct (anthropometric) and indirect (cephalometric) measurements of the skull. J Craniofac Surg 13(1):105–108
Frakas LG (1981) Anthropometry of the head and face in medicine. Elsevier, New York, p 1981
Gietzen T, Brylka R, Achenbach J, Zum Hebel K, Schömer E, Botsch M, Schwanecke U, Schulze R (2019) A method for automatic forensic facial reconstruction based on dense statistics of soft tissue thickness. PLoS One 14(1):e0210257
Gupta S, Gupta V, Vij H, Vij R, Tyagi N (2015) Forensic facial reconstruction: The final frontier. J Clin Diagnostic Res 9(9):ZE26
Guyomarc’h P, Santos F, Dutailly B, Desbarats P, Bou C, Coqueugniot H (2012) Three-dimensional computer-assisted craniometrics: a comparison of the uncertainty in measurement induced by surface reconstruction performed by two computer programs. Forensic Sci Int 219(1–3):221–227
Guyomarc’h P, Velemínský P, Brůžek J, Lynnerup N, Horák M, Kučera J, Rasmussen KL, Podliska J, Dragoun Z, Smolik J (2018) Facial approximation of Tycho Brahe’s partial skull based on estimated data with TIVMI-AFA3D. Forensic Sci Int 292:131–137
Hillewig E, Degroote J, Van Der Paelt T, Visscher A, Vandemaele P, Lutin B, D’Hooghe L, Vandriessche V, Piette M, Verstraete K (2013) Magnetic resonance imaging of the sternal extremity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med 127(3):677–689. https://doi.org/10.1007/s00414-012-0798-z
Johari M, Esmaeili F, Hamidi H (2017) Suppl-1, M6: facial soft tissue thickness of midline in an Iranian sample: MRI study. Open Dent J 11:375
Kaur K, Sehrawat JS, Bahadur R (2017) Sex dependent variations in craniofacial soft-tissue thicknesses estimated from Sex dependent variations in craniofacial soft-tissue thicknesses estimated from MRI and CT scans: A pilot study based on northwest Indian subjects. Int J Diagn Imaging 4:47
Khatri M, Misra D, Rai S, Misra A (2017) Unfolding the mysterious path of forensic facial reconstruction: Review of different imaging modalities. MAMC J Med Sci 3(3):120
Kolar JC, Salter EM (1997) Craniofacial anthropometry: practical measurement of the head and face for clinical, surgical, and research use. Springfield, Ill., U.S.A: C.C. Thomas
Krogman WM, Isçan MY (1986) The human skeleton in forensic medicine, Charles C. Thomas, Springfield, IL 15(2):202–208
Lee WJ, Shinde V, Kim YJ, Woo EJ, Jadhav N, Waghmare P, Yadav Y, Munshi A, Panyam A, Chatterjee M (2020) Craniofacial reconstruction of the Indus Valley Civilization individuals found at 4500-year-old Rakhigarhi cemetery. Anat Sci Int 95:286–292
Lee WJ, Shin DH (2020) Craniofacial Reconstruction in Mummy Studies. The Handbook of Mummy Studies: New Frontiers in Scientific and Cultural Perspectives. pp 1–14
Lodha A, Mehta M, Patel MN, Menon SK (2016) Facial soft tissue thickness database of Gujarati population for forensic craniofacial reconstruction. Egypt J Forensic Sci 6(2):126–134
Meundi MA, David CM (2019) Application of cone beam computed tomography in facial soft tissue thickness measurements for craniofacial reconstruction. J Oral Maxillofac Pathol 23(1):114
Naini FB, Moss JP, Gill DS (2006) The enigma of facial beauty: Esthetics, proportions, deformity, and controversy. Am J Orthod Dentofac Orthop 130(3):277–282. https://doi.org/10.1016/j.ajodo.2005.09.027
Panenková P, Beňuš R, Masnicová S, Obertová Z, Grunt J (2012) Facial soft tissue thicknesses of the mid-face for Slovak population. Forensic Sci Int 220(1–3):293–e1
Rhine JS, Campbell HR (1980) Thickness of facial tissues in American blacks. J Forensic Sci 25(4):847–858
Ruiz NAP (2013) Facial soft tissue thickness of Colombian adults. Forensic Sci Int 229(1–3). https://doi.org/10.1016/j.forsciint.2013.03.017
Sahni D, Sanjeev SG, Jit I, Singh P (2008) Facial soft tissue thickness in northwest Indian adults. Forensic Sci Int 176(2–3):137–146. https://doi.org/10.1016/j.forsciint.2007.07.012
Sahni D, Jit I, Gupta M, Singh P, Suri S, Kaur H (2002) Preliminary study on facial soft tissue thickness by magnetic resonance imaging in Northwest Indians. Forensic Sci Commun 4(1). https://archives.fbi.gov/archives/about-us/lab/forensic-science-communications/fsc/jan2002/sahni.htm.
Sandamini H, Jayawardena A, Batuwitage L, Rajapakse R, Karunaratna D, Vidanapathirana M, Pallewatte A (2018) Facial soft tissue thickness trends for selected age groups of Sri Lankan adult population. Forensic Sci Int 293(102):e1–102.e11. https://doi.org/10.1016/j.forsciint.2018.10.001
Sipahioğlu S, Ulubay H, Diren HB (2012) Midline facial soft tissue thickness database of Turkish population: MRI study. Forensic Sci Int 219(1–3):282–e1
Starbuck JM, Ward RE (2007) The affect of tissue depth variation on craniofacial reconstructions. Forensic Sci Int 172(2–3):130–136
Stephan CN, Preisler R (2018) In vivo facial soft tissue thicknesses of adult Australians. Forensic Sci Int 282:220–e1
Ubelaker DH, Shamlou A, Kunkle A (2019) Contributions of forensic anthropology to positive scientific identification: a critical review. Forensic Sci Res 4(1):45–50
Wang J, Zhao X, Mi C, Raza I (2016) The study on facial soft tissue thickness using Han population in Xinjiang. Forensic Sci Int 266:585.e1–585.e5. https://doi.org/10.1016/j.forsciint.2016.04.032
Wilkinson C (2005) Computerized forensic facial reconstruction: a review of current systems. Forensic Sci Med Pathol 1(3):173–177. https://doi.org/10.1385/FSMP:1:3:173
Wilkinson C, Rynn C, Peters H, Taister M, Kau CH, Richmond S (2006) A blind accuracy assessment of computer-modeled forensic facial reconstruction using computed tomography data from live subjects. Forensic Sci Med Pathol 2(3):179–187
Wilkinson CM (2004) Forensic Facial Reconstruction. Cambridge: Cambridge University Press
Wilkinson CM (2008) The facial reconstruction of ancient Egyptians. In Egyptian Mummies and Modern Science (ed R David), Chapter 11, pp. 162–180, Cambridge: Cambridge University Press
Acknowledgements
Authors would like to thank all individuals whose scans were used in this study. We would also like to thank tricity radiographers to help in data collection.
Funding
NA.
Author information
Authors and Affiliations
Contributions
JSS conceptualized the manuscript, helped in location of facial landmarks on MRI scans, data analysis, interpretation and tabulation, and wrote original draft of the manuscript, revised the previous version of the manuscript. ST collected data, made figures, ran statistical analyses, reviewed, and corrected the original manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Necessary permissions for data collection and consent to participation have been obtained.
Consent for publication
Both the authors have consented to submit this work to Egyptian Journal of Forensic Sciences for consideration of publication.
All authors have agreed to the submission to the journal and declare that the manuscript is not currently under submission to any other journal.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thakur, S., Sehrawat, J.S. Age and sex dependent differences in midline facial soft tissue thicknesses measured on MRI scans of Northwest Indian subjects: a forensic anthropological study. Egypt J Forensic Sci 13, 38 (2023). https://doi.org/10.1186/s41935-023-00356-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41935-023-00356-z