
Abstract
Background
Airguns with the energy of ejected pellets below 17 J are not considered weapons in Poland, can be purchased without permission, and do not require registration. The mere possession of this kind of airgun does not entail any legal consequences, unless it is used for an unauthorized purpose. Sports and recreational shooting do not have to take place within shooting ranges. However, the improper use of this type of weapon can lead to serious injuries and death. In addition, the impact of high blood alcohol content on pain perception can lead to a lack of awareness of the gunshot.
Case presentation
A 36-year-old woman died a few hours after a head injury inflicted by a 5.50-mm caliber pellet fired from an air gun. The first pellet penetrated perpendicularly through the left temporal bone to the brain. The gunshot tract of this head wound was 6 cm long and ran horizontally and perpendicularly to the surface of the squamous part of the temporal bone. The tract ran through the skin of the skull, the left temporal muscle, and the squamous part of the temporal bone (where the bone was only 1.5 mm thick). The pellet then penetrated the cerebral dura mater, cerebral pia mater on the borderline of the left temporal and frontal lobes, and left lateral wall of the sphenoidal sinus. The victim did not complain of pain due to a high level of alcohol intoxication (0.35 blood alcohol content). The pellet from the second shot (on the foot) penetrated the right foot and was inflicted by the victim.
Conclusion
The victim died not earlier than 3 h after being shot as a result of intracranial injuries that caused hemorrhage. The outcomes of this study indicated that high alcohol content resulted in reduced awareness of the victim and no apparent symptoms of developing intracranial injuries.
Highlights
• People should not underestimate the injury caused by an air weapon
• A small external wound is often misleading
• Highly intoxicated with alcohol may alter the perception of pain
• A victim may not be aware of the damage to brain structures and die after a while
Similar content being viewed by others

Background
According to the Weapons and Ammunition Act of May 21, 1999 (Journal of Laws No. 53/1999, item 549, as amended), airguns with the energy of ejected pellets below 17 J are not considered weapons in Poland (Ustawa o broni i amunicji 1999). Airguns can be purchased without permission and do not require registration. The mere possession of airguns with an energy below 17 J does not entail any legal consequences unless it is used for an unauthorized purpose. Sports and recreational shooting do not have to take place on shooting ranges. They may occur outside shooting ranges, but special care must be taken (Smędra-Kaźmirska et al. 2010). In most cases, airguns are used to shoot metallic projectiles called pellets. These are considered low velocities and are generally regarded as safe (Mishra and Satwinder 2014). Pneumatic weapons use compressed air to propel projectiles. These can be classified by the type of projectile they propel, propulsion mechanism, and caliber (Fig.1).

a KANDAR B3-3 airgun. b Diabolo pellet and metal box with 5.5-mm pellets
The standard calibers for airguns in Poland are 4.5 mm (0.177 in) and 5.5 mm (0.22 in). Depending on the pellet material, they can be made of steel, lead, copper, or plastic. Lead is the most frequently used material in Poland for pellets. The pellet weight was dependent on the pellet brand. Different nose shapes are used for pellets. These are axisymmetric projectiles of three basic types: wadcutter, sharp-pointed, and spherical. The round-nose pellet in a variable range of Mach numbers showed the best aerodynamic and dynamic behaviors in comparison with other pellets. From aerodynamic and dynamic viewpoints, sharp-pointed pellets would have been preferred if all the shaped pellets had the same weight (Rafeie and Teymourtash 2016). Moreover, a more aerodynamically shaped projectile exhibits a slower decline in velocity and kinetic energy owing to air resistance (Khan 2017). Ladomatos came to the opposite conclusion in his research (Ladommatos 2019). According to the presented results, the geometry of the front face has a weak influence on the drag acting on the pellet base. Flat, sharp-pointed, and cavity-head pellets had higher overall drag coefficients than a spherical pellet. Because of their extremely lightweight, pellets lose velocity rapidly and become harmless at less than 100 m (DiMaio 1999).
Research on airgun injuries has been conducted for several years (Mallozzi 2008). Milroy et al. described the characteristics of a series of people accidentally or deliberately killed by air-powered weapons (Milroy et al. 1998). Various studies have indicated that injuries are predominat in school-aged patients and male adolescents. This is because the use and manufacture of this type of weapon are aimed at this population (Naude and Bongard 1996; Chhetri and Shapiro 2004). Bakovic described a case of suicide in a young female who used an air rifle (Bakovic et al. 2014).
Abad et al. reported that the critical velocity required for the penetration of human skin by an airgun pellet is approximately 38–70 m/s (Abad et al. 2009). The skin thickness and subcutaneous tissue affect the degree of penetration. DiMaio et al. established that skin penetration of the human lower extremities occurs at 101 m/s for a 4.57 mm, (0.18 in.) 0.54 g pellet, and 75 m/s for a 1.07 g, 5.59 mm (0.22 in.) pellet (DiMaio et al. 1982). Skurczyński demonstrated that air rifles can produce enough power to cause projectiles to penetrate the skull, depending on the distance between the weapon and penetrated tissue (Skurczyński 1965). The pellets typically enter transnasally, transocularly, or transtemporally. In these regions, the bone is the thinnest (Ford et al. 1990). Keten presented the problem of fatal internal organ injuries from close-range air gunshots (Keten et al. 2016). A 6-year-old boy was injured by an air gun. The pellet entered the chest cavity and injured the lung and aorta, causing the death pf the boy as a result of bleeding.
People may put themselves or others at risk of air gun injury by inappropriately consuming alcohol in situations where firearms are present. Thus, alcohol consumption is seen as a contributing factor to the occurrence of firearm injuries. Research on this subject has been conducted for many years. For example, Branas reported that over one-quarter of these decedents in the USA (homicides and suicides) had consumed alcohol heavily before their death (Branas et al. 2016). The consumption of alcohol in large doses (BAC - blood alcohol content, 0.25–0.45%) leads to a condition called Stupor-Coma. These stages can be dangerous and even fatal if a person is critically injured. A person in the coma stage is at risk of death. Alcohol has been found to alleviate physical pain, but requires doses consistent with binge drinking to do so. Thompson et al. suggested that a BAC of 0.08% produces a small increase in the pain threshold, a reduction in pain intensity, and a moderate to large reduction in pain intensity ratings (Thompson et al. 2017). Thus, alcohol is an effective analgesic that delivers a clinically relevant reduction in pain intensity ratings. Horn-Hofman et al. indicated that alcohol does, in fact, have pain-dampening effects (Horn-Hofmann et al. 2015).
Case presentation
In the early hours of the morning, in a flat town in Poland, an ambulance crew member called for intervention and reported the death of a 36-year-old woman. The body, already showing early signs of death (livores mortis), was kept in a room. On the left temple of the deceased, an injury initially described as epidermal abrasion was found, which raised concerns of the medical staff and was the reason why police officers were called to the site. During the emergency procedure, the woman’s glucose level, 7.8 mmol/L, was measured. The owner explained that the victim was a friend and asked him to stay overnight the previous evening. After drinking alcohol (beer and vodka) together, they went to bed before midnight, each in a different room. He found the body of his deceased friend the next day, when he was ready for work. The victim then sat on the floor, with her abdomen resting on a soft bed. In his opinion, she was already dead by then, but nevertheless, he put her on the floor and tried to help.
A detailed visual inspection of the body location was conducted. On top of the cupboard, there was a wooden board leaning against the wall, with targets inside it. The targets had holes in them. Numerous signs of damage caused by airgun pellets were identified on the furniture and on the walls of the flat. During the preliminary external examination of the corpse, small wounds were found in the left temporal area and right foot. The injuries had tracts, classified as gunshot wounds.
The owner of the flat was interrogated as a suspect in connection with the suspicion that the woman had died by unlawful killing. He explained that the previous night, he and the woman had been drinking alcohol and shooting from a distance with an airgun at targets in the corridor (Fig. 2a). Sitting on a couch in one of the rooms, they took turns shooting at two targets glued to a board set in the hallway on a cupboard. The woman was probably already drunk to such an extent that she was unable to load the air gun with the pellet. As the man fired a shot, the woman, sitting on his right, leaned over to reach for a glass of vodka or beer on the coffee table in front of the couch. Her head was on the shooting line of the airgun held by the man, approximately 20–50 cm from the barrel. As the suspect was shooting, at that very moment the woman was accidentally shot in the temporal part of her left head. The perpetrator assumed that the shot ricocheted from the head. Only slight bleeding abrasion of the epidermis was visible on the temple, while the victim did not complain of any significant ailments. They then continued to consume alcohol and shoot at the targets in the hallway. At one point, the man went to another room from where he heard a shot. At that time, the woman shot herself from the airgun onto her right foot. Upon returning to the room, the man noticed a wound on the victim’s foot, so he hid the airgun and went to sleep in another room. In the morning, while the man was preparing for work, he noticed that the woman was dead.
In this case, a shooting incident reconstruction was performed, during which the suspect presented circumstances in which he was supposed to have accidentally shot the victim on his flat. In particular, the exact positions of the airgun, the victim’s head, and the targets placed in the hallway at the time of the accidental shooting were indicated (Fig. 2b).

Site of the incident and a reconstruction scheme: a targets used for aiming the airgun and b scheme of the incident and accidental shooting in the temporal region of the head in the victim reaching for a glass on the coffee table
During the course of the investigation, an examination of the secured air gun was performed, and a forensic autopsy was performed on the deceased’s body. A gunshot wound on the head was found, starting with an entrance wound (Ø 5 mm) in the left temporal-epidural region (Fig. 3a). The wound had a tract that ran through the skin of the skull, left temporal muscle, and squamous part of the temporal bone. The wound tract ran through the dura mater and pia mater on the borderline of the left temporal and frontal lobes (where a massive diffuse subarachnoid hematoma was also found) and the left lateral wall of the sphenoidal sinus (with the hematoma in its lumen and secondary massive blood aspiration to the lower airways) (Fig. 3b). In this case, the pellet entered transtemporally, where the bone was the thinnest (1.5 mm on autopsy). The gunshot tract of the head wound was 6 cm long in total. Although no exit wounds were found on the scalp, no pellets were found inside the cranial cavity. However, an autopsy revealed that after turning the victim’s corpse sideways, the pellet, together with the blood, flowed out of her body through the nasal canals (cranial cavity → sinus cavity → nasal cavity). Diabolo pellets retrieved from the skull and foot are presented in Fig. 4.

Entrance wound and trajectory a left cranial entrance wound, b trajectory of airgun pellet in the skull, c right foot entrance wound, d left temporal muscle hematoma with the entrance wound, e basal of the cranium (the arrow indicates wound entering cranial cavity), f massive diffuse subarachnoid hematoma (the arrow indicates arachnoid laceration on the borderline od left temporal and frontal lobes)

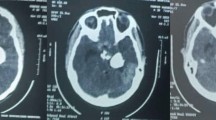
Diabolo pellet a schematic representation of “route” using an example CT scan (cranial cavity → sinus cavity → nasal cavity). b Pellet retrieved from the patient (two side views): c pellet from the skull and from the foot
The entrance wound on the right foot was 6 × 3 mm and was surrounded by a 1-mm wide margin of abraded epidermis, with a rounded posterior end and a pointed anterior end (Fig. 3c). It was located within a diffuse dark-red bruise measuring 80×70 mm. The gunshot tract was 60 mm long and ran under the skin above the dorsal side of the 2nd metatarsal bone towards the base of the second toe.
During the autopsy, the blood and urine samples were collected from the corpse for toxicological tests. The tests showed the presence of 0.34% ethyl alcohol in the blood and 0.46% in the urine.
In the conclusions of the post-mortem report, a gunshot wound to the head with intracranial injuries and aspiration of the blood to the lower airways with subsequent asphyxiation was considered to be the direct cause of the woman’s death. The autopsy results did not contradict the suspect’s version of the possibility of accidental head injury with a pneumatic weapon in the victim. In addition, the victim was heavily intoxicated with alcohol which may have caused her to underestimate the effects of her head injury, and her reduced level of consciousness, which was already altered by previous alcohol consumption, masked the symptoms of developing intracranial injuries.
After a preliminary investigation, the suspect was accused of manslaughter by the public prosecutor.
Conclusions
Injuries to the skull, face, and neck caused by pneumatic weapon projectiles are most commonly reported, and some of these cases have fatal outcomes (Holland et al. 2004; Bratton et al. 1997). Much has been published on the fact that the head is the most common part of the body penetrated (Bowen and Magauran 1973; James 1962; Shaw and Galbraith 1977). Nonfatal injuries include brain damage and permanent impairment. This is because the human skull is vulnerable to penetration by airgun pellets.
Our case study highlights that skull penetration by air gun pellets can occur and lead to death. The depth of penetration and damage depends on the characteristics of the tissues on the trajectory of the projectile. The present case is interesting because the pellet went through the lateral wall of the sphenoidal sinus and leaked via the nasal canal with the blood, once the dead body was turned on the side. Moreover, the victim died not earlier than 3 h after being shot as a result of intracranial injuries that caused the hemorrhage. Aspiration of the blood into the lower airways resulted in the suffocation of the victim. High alcohol content resulted in reduced awareness of the victim and no apparent symptoms of developing intracranial injuries. If helped properly immediately after the shooting, the victim would have had a chance of survival.
Injuries inflicted by airguns are frequently underestimated, and airguns should not be played with, especially by people who are under the influence of alcohol. The public, as well as governments and legislatures, should be advised that air guns are not toys but dangerous weapons that may cause serious injuries and even death. This case report advocates for more rigorous regulations regarding air guns and safety standards, especially in Poland.
Availability of data and materials
25 November 2020.
Abbreviations
- BAC:
-
Blood alcohol content
References
Abad S, McHenry ID, Carter LM, Mitchell DA (2009) Carotid artery injury from an airgun pellet: a case report and review of the literature. Head Face Med. 5. https://doi.org/10.1186/1746-160X-5-3
Bakovic M, Petrovecki V, Strinovic D, Mayer D (2014) Shot through the heart-firepower and potential lethality of air weapons. J. Forensic Sci. 59:1658–1661. https://doi.org/10.1111/1556-4029.12486
Bowen D, Magauran D (1973) Ocular injuries caused by airgun pellets: an analysis of 105 cases. Br. Med. J. 1:333–337. https://doi.org/10.1136/bmj.1.5849.333
Branas CC, Han S, Wiebe DJ (2016) Alcohol use and firearm violence, epidemiol. Rev. 38:32–45. https://doi.org/10.1093/epirev/mxv010
Bratton S, Dowd M, Brogan T, Hegenbarth M (1997) Serious and fatal air gun injuries: more than meets the eye. Pediatrics. 100:609–612. https://doi.org/10.1542/peds.100.4.609
Chhetri D, Shapiro N (2004) A case of a BB-gun pellet injury to the ethmoid sinus in a child. Ear, Nose Throat J. 83:176–180. https://doi.org/10.1177/014556130408300313
DiMaio V (1999) Gunshot Wounds. Practical aspects of firearms, ballistics, and forensic techniques. CRC Press
DiMaio V, Copeland A, Besant-Matthews P, Fletcher L, Jones A (1982) Minimal velocities necessary for perforation of skin by air gun pellets and bullets. J. Forensic Sci. 27:894–898. https://doi.org/10.1520/jfs12207j
Ford E, Senac M, McGrath N (1990) It may be more significant than you think: BB air rifle injury to a child’s head. Pediatr. Emerg. Care. 6:278–279
Holland P, O’Brien D, May L (2004) Should air guns be banned? Br J Neurol. 18:124–129
Horn-Hofmann C, Büscher P, Lautenbacher S, Wolstein J (2015) The effect of nonrecurring alcohol administration on pain perception in humans: a systematic review. J. Pain Res. 8:175–187. https://doi.org/10.2147/JPR.S79618
James W (1962) A fatal air rifle pellet wound of the brain. Med. Sci. Law. 2:153–154. https://doi.org/10.1177/002580246200200210
Keten A, Avsar A, Karanfil R, Okdemir E (2016) Accidental Death by Air Rifle: A Case Report. Bull. Leg. Med. 21:50–51. https://doi.org/10.17986/blm.2016116602
Khan I (2017) Study of Internal & External Ballistics for .177 cal & .22 cal Projectile. Int. J. Sci. Res. Dev 5:78–82
Ladommatos N (2019) Influence of air rifle pellet geometryon aerodynamic drag. Proc. Inst. Mech. Eng. Part P J. Sport. Eng. Technol. https://doi.org/10.1177/1754337119831107
Mallozzi D (2008) Herida por proyectil de arma neumatica. Caso Clinico, AN ORL MEX. 53:182–185
Milroy C, Clark J, Carter N, Rutty G, Rooney N (1998) Air weapon fatalities. J. Clin. Pathol. 51:525–529. https://doi.org/10.1136/jcp.51.7.525
Mishra A, Satwinder P (2014) A rare case of deep penetration of skull base by an airgun pellet. Exp. 28:1973–1942
Naude G, Bongard F (1996) From deadly weapon to toy and back again: the danger of air rifles. J. Trauma - Inj. Infect. Crit. Care. 41:1039–1043. https://doi.org/10.1097/00005373-199612000-00017
Rafeie M, Teymourtash AR (2016) Aerodynamic and dynamic analyses of three common 4.5 mm-caliber pellets in a transonic flow. Sci. Iran. 23:1767–1776. https://doi.org/10.24200/sci.2016.3924
Shaw M, Galbraith S (1977) Penetrating airgun injuries of the head. Br J Surg. 64:221–224
Skurczyński W (1965) Air rifle gunshot wounds in the region of the neck and head. HNO. 13:223–226
Smędra-Kaźmirska A, Barzdo M, Kędzierski M, Szram S, Berent J (2010) Experimental effect of a shot caused by 4.5 mm cartridges fired from a Norica Dragon air-rifle and a Walther PPK/S air-pistol. Arch. Med. Sąd. Kryminol. LX 60:77–82
Thompson T, Oram C, Correll CU, Tsermentseli S, Stubbs B (2017) Analgesic effects of alcohol: a systematic review and meta-analysis of controlled experimental studies in healthy participants. J. Pain. 18. https://doi.org/10.1016/j.jpain.2016.11.009
Ustawa o broni i amunicji (Dz. U. nr 53/1999 poz. 549 z późn. zm), 1999. https://eli.gov.pl/api/acts/DU/1999/549/text/O/D19990549.pdf
Acknowledgements
We are most thankful to the District Court Szczecin-Prawobrzeże and the West in Szczecin, 7th VII Police Local Criminal Division (Poland), that has approved the publication of this case report.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conceptualization, S.G.; formal analysis, S.G.; methodology, S.G.and S.M.; project administration, S.G.; supervision, S.G.; validation, S.G; data curation, S.M. and B.P-B.; software, S.G.; visualization, S.G.; writing—original draft, S.G. and S.M.; writing—review and editing, S.G and B.P-B. The authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent for publication
The authors affirm that identifying details (name, date of birth, identity numbers, and other information) of the participant that were studied are not published in written descriptions, photographs, and genetics. The District Court Szczecin-Prawobrzeże and the West in Szczecin, 7th VII Police Local Criminal Division (Poland), has approved the publication of this case report.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Glowinski, S., Majdanik, S. & Potocka-Banaś, B. Alcohol and fatal penetration of the cranium by an airgun pellet—a case study from Poland. Egypt J Forensic Sci 13, 12 (2023). https://doi.org/10.1186/s41935-023-00332-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41935-023-00332-7