
Abstract
Background
Stabbing is a relatively uncommon method of suicide. Typical suicide is usually associated with tentative wounds. Self-stabbing using two sharp weapons to produce two stab wounds without tentative marks is an uncommon incidence.
Case presentation
A 42-year-old Austronesian descent male with a history of family troubles was found dead by his friend inside a clothing store; two kitchen knives were present on both sides of the body. There were two stab wounds in the chest and the abdomen without any superficial hesitation cuts. At the crime scene, there were two blood pools.
Conclusion
The number of injuries with the absence of hesitation injuries raised suspicions of an atypical case of suicide that necessitated further forensic investigations. However, the circumstantial evidence and autopsy findings demonstrated that suicide was the cause of death.
Similar content being viewed by others


Background
Suicidal stab wounds are occasionally seen in less than 1% of all suicidal deaths (Kaliszan et al., 2010). A Saudi study showed that self-stabbing accounts for 8.2% of all suicide cases that were more prevalent among Indian residents (Issa et al., 2016).
Complex suicide is discussed in the literature and is classified into planned and unplanned groups. Planned groups employ multiple methods simultaneously, including intoxication and cutting. Due to the failure of the initial suicide attempt, victims in unplanned groups use alternative methods, such as shooting, stabbing, and jumping from a height (Hösükler et al., 2022; Parroni et al., 2002; Zengın Eroglu et al., 2017).
An isolated stab wound with the presence of tentative wounds is usually self-inflicted. Nevertheless, there are known cases in which a victim self-inflicted multiple stab wounds to various body parts without tentative wound infliction (Kaliszan et al., 2010; Patil et al., 2016). In these cases, precise forensic investigations are needed to determine whether the manner of death was suicidal or homicidal.
General prosecutor’s investigations, scene investigations, forensic description of the external and internal injuries, and determination of mental and substance abuse disorders can determine the manner of death (Rockett et al., 2018).
Case presentation
A 42-year-old man of Austronesian descent with no history of psychiatric illness or suicide attempts was discovered, by a friend, stabbed to death in the early morning hours inside a clothing store. The footage recorded by closed-circuit television cameras spotted that the victim had arrived at the clothing store early in the morning then entered its store and did not emerge from it.
The body was discovered in a semi-sitting position on the floor, surrounded by two pools of blood, fully dressed in an opened shirt and raised T-shirt on the abdomen. The forensic authority was called to investigate the death scene. There were two stab wounds to the front of the chest and abdomen. Two blood-stained kitchen knives were lying in his proximity to his hands (Fig. 1).

The position of the victim at the death scene where the body was seen seated on the floor in a semi-sitting position surrounded by two pools of the blood, fully dressed in the opened shirt and raised T-shirt on the abdomen
A letter was found in his bag, in which the victim apologized for being a burden and cheating on his wife. Neither tentative nor defensive wounds were identified.
The period between the time of death and forensic scene investigation was approximately 8 (±2) hours, which corresponded well with the extent of hypostasis, muscular rigidity, and cooling rate.
Autopsy finding
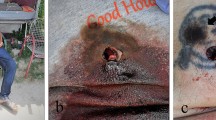
Upon postmortem examination, two stab wounds were discovered, as demonstrated in Fig. 2. The upper one was located in the left lower region of the chest, 52cm below hair line, and 4cm to the left of the anterior midline measuring 2.7cm in length. The lower one was present in the right lumbar region of the abdomen, 69cm below the hair line, and 4cm to the right of the anterior midline measuring 2.5cm in length.

The location of the chest and abdominal stab wounds where the upper one was present in the left lower region of the chest, measuring 2.7cm in length, while the lower one was present in the right lumbar region of the abdomen, measuring 2.5cm in length
The two stab wounds had a single pointed end with a unilateral “fish-tail” sign on the opposite end, caused by the knife blade, and had the same backward direction. However, the pointed edge of the chest wound was directed toward the right side, whereas the abdominal wound was directed toward the left side of the body. These characteristics were consistent with the knives that were discovered. The toxicological screening’s results were negative for the presence of basic and acidic drugs, amphetamine and its related compounds, sedatives, cannabinoids, opiates, and their related derivatives in the postmortem blood and urine samples
The chest stab wound penetrated the heart; ran through the right ventricle, interventricular septum, and left ventricle; and resulted in a penetrating wound in the posterior wall of the left ventricle (Fig. 3), accompanied by hemorrhage into the pericardial cavity, where nearly 350 mL of the blood was found. In contrast, the abdominal wound penetrated through the peritoneum into the small intestine with non-obvious peritoneal hemorrhage (Fig. 4). The cause of death was severe blood loss due to cardiac injuries.

The chest wound: penetrating the heart ran through the right ventricle, interventricular septum, and left ventricle

Abdominal wound: penetrating peritoneum into the small intestine with non-obvious bleeding
Discussion
A body with multiple stab wounds can raise suspicions of homicide; however, these suspicions can be dispelled by a thorough analysis of the scene investigations and forensic examination results (Brunel et al., 2010; Burke et al., 2018).
A single-stab wound was identified in 29% of the sharp-force suicidal fatalities (Brunel et al., 2010). In addition, single-stab homicidal injuries were detected in 78.8% of the sharp force fatalities (Burke et al., 2018). Furthermore, multiple stab injuries and complex suicides could be detectable in suicidal deaths. Indeed, medicolegal differentiation between suicide and homicide is required in these cases (Kaliszan et al., 2010; Hösükler et al., 2022; Zengın Eroglu et al., 2017; Kranioti et al., 2017).
The planned complex suicides were commonly inflicted using two methods and mainly involved male victims in their resident area (Kaliszan et al., 2010; Hösükler et al., 2022; Zengın Eroglu et al., 2017; Kranioti et al., 2017). As an example of a complex suicide involving two knife-related stabs, the proximity of the two knives in the present case suggests that the victim inflicted injuries sequentially with the two sharp objects. He attempted suicide by stabbing himself in the abdomen and heart. In complex suicides, less lethal methods are typically employed prior to more fatal ones (Zengın Eroglu et al., 2017).
Homicidal sharp object wounds were mainly identified in the front of the neck, chest, and abdomen (Issa et al., 2016), whereas suicidal ones primarily targeted the wrist, neck, pericardium at the intercostal and subcostal spaces, and epigastrium (Kaliszan et al., 2010; Hösükler et al., 2022; Patil et al., 2016). This finding is consistent with our case in which the lethal stab wound was discovered in the left subcostal region.
Using two opposed knives in suicidal stabbing could result in wounds with the same trajectory alongside different orientations as the victim’s position was not changed. However, homicidal stabbing wounds had different trajectories depending on the body’s position during the fighting and escaping (Kaliszan et al., 2010; Patil et al., 2016; Phoenix & Indiana, 2017).
As in most suicides, the victim unbuttoned his shirt and lifted his T-shirt to explore the stabbing area (Issa et al., 2016; Burke et al., 2018; Kranioti et al., 2017; Phoenix & Indiana, 2017). However, the tentative wounds were not identified.
Tentative wounds are superficial sharp object wounds confined to the skin layers. They are useful predictive signs of suicides, as their presence with the absence of defensive wounds and the cloth tears can differentiate suicide from homicide (Rockett et al., 2018; Kranioti et al., 2017). As tentative wounds could be observed in homicidal deaths (Kaliszan et al., 2010; Brunel et al., 2010; Phoenix & Indiana, 2017) but not in suicidal deaths, we could not distinguish suicide from homicide based solely on their presence (Patil et al., 2016).
The presence of suicidal letters and the absence of fight signs are related to the suicide phenomenon. According to the Interpersonal Theory of Suicide, Fernández-Cabana et al. (2015) stated that suicidal factors could be identified from suicidal notes, and both interpersonal risk factors, including the feeling of being a burden and lack of belonging to a group, were the most commonly detected factors (Fernández-Cabana et al., 2015).
In the present case, the distribution of the blood, the position of the body, and the proximity of the two knives assumed that the victim inflicted injuries himself using the found sharp objects. The sequence of wound infliction could be as follows: first, the victim inflicted the abdominal wound; nonetheless, the abdominal wall thickness and the penetration angle led to the non-fatal injury of the peritoneum without obvious bleeding (Phoenix & Indiana, 2017). Because of failing of this attempt, the victim inflicted a lethal cardiac wound with another weapon. The conversion from lesser to greater fatal techniques is typically seen in complex suicide cases (Hösükler et al., 2022; Parroni et al., 2002; Zengın Eroglu et al., 2017).
Two knife-related stabs in one suicidal case have been infrequently described in literature, but feeling of guilt and inability to adapt to challenging situations can increase self-directed aggression (Kaliszan et al., 2010).
Conclusions
Stabbing is one of the least used methods detected in complex suicidal deaths. Homicidal deaths are associated with multiple sharp-force injuries; however, multiple sharp-force injuries have been described in atypical suicidal deaths. Detection of the cause and the manner of the atypical deaths need inter-disciplinary co-operation between medicolegal death investigators to interpret circumstantial pieces of evidence.
Availability of data and materials
All data is available in the manuscript.
Abbreviations
- Cm:
-
Centimeter
- mL:
-
milliliter
References
Brunel C, Fermanian C, Durigon M, de la Grandmaison GL (2010) Homicidal and suicidal sharp force fatalities: autopsy parameters in relation to the manner of death. Forensic Sci Int 198(1-3):150–154
Burke MP, Baber Y, Cheung Z, Fitzgerald M (2018) Single stab injuries. Forensic Sci Med Pathol 14(3):295–300
Fernández-Cabana M, Ceballos-Espinoza F, Mateos R, Alves-Pérez MT, García-Caballero AA (2015) Suicide notes: clinical and linguistic analysis from the perspective of the Interpersonal Theory of Suicide. Eur J Psychiatry 29(4):293–308
Hösükler E, Hösükler B, Çoban İ, Koç S (2022) Complex suicides: 21 cases and a review of the literature. Egypt J Forensic Sci 12(1):1–8
Issa SY, El Dossary M, Salam MA, Al Madani O, AlMazroua MK, Alsowayigh K et al (2016) Suicidal deaths in depth-Eastern Province-Saudi Arabia. Egypt J Forensic Sci 6(3):240–247
Kaliszan M, Kernbach-Wighton G, BouHaidar R (2010) Multiple self-inflicted stab wounds to neck, chest and abdomen as a unique manner of suicide. J Forensic Sci 55(3):822–825
Kranioti EF, Kastanaki AE, Nathena D, Papadomanolakis A (2017) Suicidal self-stabbing: a report of 12 cases from Crete, Greece. Med Sci Law 57(3):124–129
Parroni E, Caringi C, Ciallella C (2002) Suicide with two guns represents a special type of combined suicide. Am J Forensic Med Pathol 23(4):329–333
Patil SS, Deokar RB, Vidhate SG, Tyagi S (2016) An atypical case of suicidal cut throat injury. Egypt J Forensic Sci 6(4):492–495
Phoenix PV, Indiana U (2017) Multiple stab wounds: understanding the manner of death through the psychological autopsy. Clin Ter 168(4):e233–e239
Rockett IR, Caine ED, Stack S, Connery HS, Nolte KB, Lilly CL et al (2018) Method overtness, forensic autopsy, and the evidentiary suicide note: a multilevel National violent death reporting system analysis. PLoS One 13(5):e0197805
Zengın Eroglu M, Şahan E, Kıraz S (2017) An unusual case of unplanned complex suicide. Psychiatry Clin Psychopharmacol 27(4):406–408
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Abdurrab A.A. Kasim: practical part, research writing, and approval. Faisal M. Alzubaidi: practical part, research writing, and approval. Yahya H. Zakari: practical part, research writing, and approval. Almaha A.A. Shatwan: literature review and research writing. Sahar S. Mulla: literature review and research writing. Abdulaziz Alasmari: practical part, research writing, and approval. Samah F. Ibrahim research writing, institutional review board approval, and proofreading. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This manuscript has been approved by institutional review board, Princess Nourah bint Abdulrahman University.
Consent for publication
All authors agree to publish this research work.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kasim, A.A.A., Alzubaidi, F.M., Zakari, Y.H. et al. The manner of death in a case with two stab wounds caused by two weapons: case report. Egypt J Forensic Sci 12, 60 (2022). https://doi.org/10.1186/s41935-022-00316-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41935-022-00316-z