
Abstract
Background
The investigation into sudden unexpected and unnatural deaths supports criminal justice, aids in litigation, and provides important information for public health including surveillance, epidemiology, and prevention programs. The use of mortality data to convey trends can inform policy development and resource allocations. Hence, data practices/management systems in Forensic Medicine are critical. This study scoped literature and described the body of knowledge on data management and practice systems in Forensic Medicine.
Methods
Five steps of the methodological framework of Arksey and O’Malley guided this scoping review. A combination of keywords, Boolean terms, and Medical Subject Headings was used to search PubMed, EBSCOhost (CINAHL with full text and Health Sources), Cochrane Library, Scopus, Web of Science, Science Direct, WorldCat, and Google Scholar from the 18th to 24th of June 2020 and updated in November 2021 for peer review papers. This study included articles involving unnatural deaths, focused on data practice or data management systems, relating to Forensic Medicine, all study designs, and published in English. Screening and selection and data extraction were conducted by two reviews. Thematic analysis was conducted, and the results were reported using both quantitatively and qualitatively.
Results
Of the 23,059 articles, 16 met this study’s inclusion criteria. The included articles were published between 2008 and 2019. Eight of the 16 articles were published between 2017 and 2019. Most of the included studies were conducted in the USA (5) and Australia/New Zealand (4). Only two publications were from lower- and middle-income countries (Nigeria, Mexico), and the remaining 14 were from high-income countries (Italy, Denmark, USA, Australia, and New Zealand, Japan, Switzerland, Canada). The data management systems found in this study were as follows: Virtopsy, Canadian Coroner and Medical Examiner Database, Infant Injury Database, Fatal injury surveillance system, Medical Examiners and Coroners Alert System, National Violent Deaths Reporting System, AM/PM Database, Tokyo CDISC/ODM, and National Coronial Information System.
Conclusions
This study’s results revealed limited articles relating to data management and practice systems in Forensic Medicine, particularly in LMICs through literature indicating there is a prevalence of unnatural deaths in LMICs. This study, therefore, recommends research on data management and practice systems relating to forensic medicine in LMICs to inform policy decisions.
Similar content being viewed by others
Background
The global burden of trauma, particularly in low- and middle-income countries places a large strain on resources, and therefore, the diagnostic value of autopsies must be reiterated (Salona Prahladh 2018). The use of autopsies remains the gold standard in assessing standards of medical care. There is a concerning decline in autopsies even though its value to the medical fraternity is acknowledged (Aase 2013; Bagher et al. 2015). Forensic Medicine and Forensic Pathology apply scientific and medical knowledge to inquests, and the autopsy is frequently regarded as the focus of the death investigation. The investigation into sudden unexpected and unnatural deaths supports criminal justice, aids in litigation, and provides important information for public health including surveillance, epidemiology, and prevention programs (Bagher et al. 2015; Tseng et al. 2018; Barbería et al. 2018; Pan et al. 2019; Soto Martinez et al. 2019). The evidence serves to inform policy not only for injury prevention and control but also to prevent suicide, violence, or substance abuse (Barbería et al. 2018; Pan et al. 2019; Rao et al. 2005; Grills et al. 2011; Prinsloo 2019; Willcox et al. 2020).
Globally, death investigations are conducted according to prevailing legislation which differs from country to country. Historically, the coroner system was formalized into law by England’s King Richard I in 1194 with the first coroners being knights (Koehler 2016). The coroner system from England was introduced in the 1600 s by American colonists to become an important part of the death investigation system in what would become the USA, but later, the role of the office was reduced to the medicolegal examination of a body and the determination of the cause and manner of death (Koehler 2016). Throughout the middle ages, the functions of the coroner included conducting inquests, attending to and inspecting the dead, and investigating suspicious deaths.
In the USA, coroners are generally public officials with minimal to no medical training. Some coroners only serve part-time capacities, and they also had other full-time employment. The medical examiner system was introduced due to public dissatisfaction, accusations of corruption, and an increased need to have highly trained personnel in the death investigation (Koehler 2016). This led to the emergence of a separate discipline of Forensic Medicine that began in the seventeenth century (Choo and Choi 2012). The first medical examiner system was introduced in Massachusetts in 1877. In 1959, the medical subspecialty of Forensic Pathology was formally certified and medical examiners were trained in Pathology. Forensic Pathology is viewed as subspecialty in Anatomical Pathology in countries such as Canada and the UK. In countries such as South Africa and Australia, you may do training solely in Forensic Pathology for a minimum of a year (usually more) with training in Anatomical Pathology. In South Africa, the medicolegal death investigation is conducted primarily in terms of the Inquests Act (Act 58 of 1959). The medicolegal autopsies are performed by medical practitioners, but due to the large annual number of unnatural deaths and the small number of qualified Forensic Pathologists in South Africa, a large number of these autopsies are performed by colleagues with limited formal training in performing autopsies (du Toit-Prinsloo and Saayman 2012).
The fundamental essence of Forensic Pathologists’ work is to investigate and report the cause of death. The importance of reporting the cause of death is reiterated and forms the basis of The Global Burden of Disease Study (Roth et al. 2018). This comprehensive worldwide observational epidemiological describes mortality and morbidity from major diseases, injuries, and risk factors to health at global, national, and regional levels. Mortality reporting systems can help to prioritize health system investments, track progress towards global development goals, and guide scientific research (Roth et al. 2018). The Global Burden of Disease study acknowledges the need for wider adoption and improvement of these systems because continuous reporting of cause-specific mortality in many countries represents a success for global health.
Information derived from autopsies has historically been paper-documented, filed, and archived. With the current age of technology, this information can be stored and managed electronically to ensure reporting that is current, relevant, and contributory to training and service delivery, policy implementation, and social interventions. The current coronavirus pandemic has accentuated the importance of wireless technology and the use of the Internet to transcend normal communications. Due to safety reasons, much work has to be conducted remotely in many business sectors including the medical sector. General practitioners conducted consultations virtually to adhere to social distancing and safety measures, and telephonic communication and telemedicine became a necessity due to the pandemic. At this current point in time, we are forced to be open-minded to integrate technology into our daily work lives.
This scoping review was conducted to map the evidence on data management and practice systems, their use, benefits, and challenges in Forensic Medicine. The information gained on the use and availability of digital technologies and their strengths and limitations to collect autopsy data can inform models to suit similar purposes in Forensic Medicine in lower- and middle-income countries.
Methods
This study’s protocol was developed a priori and published (Prahladh and van Wyk 2020). This study used the Arksey and O’Malley framework to conduct a scoping review which includes the following: (i) the research question was identified, (ii) relevant studies were identified, (iii) eligible studies were selected, (iv) the data was charted, and (v) the results were collated and summarized (Arksey and O'Malley 2005; PRISMA 2018).
Identifying the research question
The main research question was “In the last 10 years, what evidence on data management and practice systems and their benefits and challenges in forensic medicine exist globally? This study’s population, concept, and context were sudden/unnatural deaths, data practices, and forensic medicine (autopsies or post-mortem examinations) globally, respectively. The research sub-questions were as follows:
-
1.
What evidence exists on data management and practice systems in forensic medicine?
-
2.
What are the reported benefits and challenges of the data management and practice systems used in forensic medicine?
Identifying relevant studies
A systematic search of both gray literature and published literature was done to retrieve articles relating to data practice, use, benefits, and challenges in forensic medicine internationally. A combination of keywords, Boolean terms, and Medical Subject Headings was used to search PubMed, EBSCOhost (Academic Search Complete, CINAHL with full text, and Health Sources), Cochrane Library, Scopus, Web of Science, Science Direct, WorldCat, and Google Scholar from the 18th to 24th of June 2020 and updated in November 2021 for peer review papers in English. Study design limitations were removed. The search strategy was piloted to check the appropriateness of keywords and databases. The results were reviewed by the research team to ensure the validity of the search strategy in PubMed. A hand search was conducted of the references of the included studies and the World Health Organization (WHO) website. Each search was adequately documented as illustrated in supplementary file 1. The Peer Review of Electronic Search Strategies (PRESS) statement guided this study’s electronic search strategy (McGowan et al. 2016). All citations were managed using the EndNote X9 reference manager.
Selection of articles and eligibility criteria
The principal investigator conducted the database searches and title screening using this study’s eligibility criteria. The search strategy and screening tools were piloted to calibrate operators and increase consistency and fine-tune the methods. A second reviewer reviewed the retrieved titles to ensure completeness before the abstract screening. Subsequently, the cleaned EndNote library was shared among the review team after the removal of duplicate titles. Using an electronic screening tool developed in Google forms, two reviewers independently screened the abstracts and full texts and categorized them into “include” or “exclude” categories based on this study’s eligibility criteria. The review team met throughout the screening process and resolved the discrepancies between the two reviewers at the abstract screening stage through discussions until a consensus was reached even though there were no significant disagreements among the reviewers. It was decided that the articles will be selected on a minimum agreement of at least 50% between the two reviewers due to the complex and specialized field the review would entail. The second reviewer, however, resolved the discrepancies between the principal investigator and the third reviewer at the full-text screening phase. The PRISMA flow diagram was used to account for all the articles. This study’s eligibility criteria used are outlined below:
Inclusion criteria
-
Studies that involved unnatural deaths
-
Studies that focused on Forensic Medicine (autopsies/post-mortem)
-
Articles that reported data practices such as use, benefits, and challenges
-
Published from 2008 to 2021
-
Published in the English language
-
All study designs
Exclusion criteria
-
Articles that do not involve Forensic Medicine/Pathology and/or autopsies
-
Studies with no clear targeted population
-
Studies where full-text articles could not be obtained
-
Articles reporting photo capture/imaging programs
-
Non-English publications
Charting the data
The data for this study were collected using a spreadsheet comprising of the following: bibliographic details, publication year, study design, study setting, data practices relating to Forensic Medicine, uses, benefits, challenges, and conclusion and recommendations. The form was pilot tested by two reviewers independently, and all discrepancies were resolved before its usage. Finally, two reviewers performed the data extraction using both inductive and deductive approaches. Subsequent discrepancies were resolved through discussion by the review team.
Collating, summarizing, and reporting the results
Thematic content analysis was conducted for this study. The emerging themes and subthemes relating to data practices in Forensic Medicine were collated, summarized, and reported narratively. However, the bibliographic details of the included studies such as design and publication year were reported quantitatively and presented as percentages.
Results
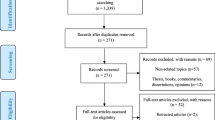
Of the total of 23,059 search yields, 144 were deemed relevant from the title screening phase based on this study’s eligibility criteria. Of the of 144 titles, 43 duplicates identified were removed, and then, 74 and 16 articles were removed at the abstract and full-text screening phases, respectively. The 16 articles removed at the full-text screening phase focused on software for clinical forensic medicine, and graph-based document representation models and others did not report the data storage method. Therefore 15 articles were finally deemed eligible for inclusion for data extraction (Fig. 1). Following reviewer indication, an additional article was added to the results after the full-text screening for a total of 16 articles to be included in the study.

PRISMA 2009 flow diagram
Characteristics of included publications
Table 1provides a summary of the main characteristics of the articles included. The included articles were published between 2008 and 2019. Eight of the 16 articles were published between 2017 and 2019 (Soto Martinez et al. 2019; Dunstan 2019; Fowler et al. 2018; Hargrove et al. 2018; Dennis et al. 2018; Saar et al. 2017; Hofmeister et al. 2017; Ottaviani et al. 2017). Most of the studies were published in the USA (Soto Martinez et al. 2019; Fowler et al. 2018; Hargrove et al. 2018; Levy 2015; Blair et al. 2016)and Australia/New Zealand (Willcox et al. 2020; Dunstan 2019; Saar et al. 2017; Lyndal et al. 2016; Pearse 2012) and three from European countries. Two publications were from LMIC (Nigeria, Mexico), and the remaining were from high-income countries (Italy, Denmark, USA, Australia, and New Zealand, Japan, Switzerland, Canada (Fig.1). The article types included brief communication (Ottaviani et al. 2017; Kiuchi et al. 2013), original studies (Dunstan 2019; Saar et al. 2017; Hofmeister et al. 2017; Levy 2015; Aghayev et al. 2008), author manuscript (preprint) (Blair et al. 2016), retrospective descriptive studies (Soto Martinez et al. 2019; Fowler et al. 2018; Hargrove et al. 2018; Dennis et al. 2018; Kipsaina et al. 2015; Colville-Ebeling et al. 2014), a single systematic review (Lyndal et al. 2016), and an annual/government report (Canada 2012).
Findings
Table 2 present a summary of these findings. A brief narrative of the finding is reported under the following main themes: data management and practice systems, benefits/uses of the data management and practice systems, and challenges/limitations of the data management and practice systems.
Types of data management and practice systems
All the reviewed studies described the use of electronic-based systems which ranged in complexity from a simplified Excel spreadsheet (Kipsaina et al. 2015)to a more complex system based on the use of a web portal (Kiuchi et al. 2013)and use at the state level and national levels, the National Violent Death Reporting System ((Blair et al. 2016), and the National Coronial Information System systems (Dunstan 2019; Saar et al. 2017; Lyndal et al. 2016). The national system received full technical support. In some cases, such as mentioned in the Nigerian study, data was collected by a single user and was based on tools developed by WHO-Monash University fatal injury surveillance manual (2012). It was found to be acceptable and timely with good data quality which was representative and specific due to a single experienced user. Other systems sourced data from multiple users and departments such as the Forensic Medicine Department, Police, Psychologist. Many of the systems were consolidated centralized systems that were used in the Forensic Medicine Departments (n= 10; 62.5%) (Dunstan 2019; Saar et al. 2017; Hofmeister et al. 2017; Ottaviani et al. 2017; Blair et al. 2016; Lyndal et al. 2016; Pearse 2012; Aghayev et al. 2008; Canada 2012). Access to all the systems was strictly controlled either through single/multiple user authorization (Dunstan 2019; Hofmeister et al. 2017; Lyndal et al. 2016; Kiuchi et al. 2013; Aghayev et al. 2008; Colville-Ebeling et al. 2014), or data are captured in a spreadsheet created in Excel (Kipsaina et al. 2015). The articles based on systems that reported the best utility were those that allowed greater flexibility and lend themselves to state-based use (Fowler et al. 2018; Blair et al. 2016). In these cases, the systems received government funding and technical support (Hofmeister et al. 2017; Blair et al. 2016; Lyndal et al. 2016; Aghayev et al. 2008; Colville-Ebeling et al. 2014; Canada 2012).
Benefits/uses of the reported data management and practice systems
In 9 (56%) of the articles, the wide coverage of cases increased the value of the system for those who used the data (Dunstan 2019; Fowler et al. 2018; Hargrove et al. 2018; Saar et al. 2017; Hofmeister et al. 2017; Ottaviani et al. 2017; Blair et al. 2016; Colville-Ebeling et al. 2014; Canada 2012). The benefits reported included the use to formulate injury prevention policies and enhance epidemiological studies (n= 10; 62.5%) (Dunstan 2019; Fowler et al. 2018; Hargrove et al. 2018; Saar et al. 2017; Ottaviani et al. 2017; Levy 2015; Blair et al. 2016; Lyndal et al. 2016; Colville-Ebeling et al. 2014; Canada 2012). Many of the cited systems contributed and supported research (n= 10; 62.5%) (Arksey and O'Malley 2005; Dunstan 2019; Fowler et al. 2018; Saar et al. 2017; Ottaviani et al. 2017; Levy 2015; Blair et al. 2016; Lyndal et al. 2016; Colville-Ebeling et al. 2014; Canada 2012). Although only a few systems had standardization of data as an attribute (n= 4; 27%) (Fowler et al. 2018; Hofmeister et al. 2017; Aghayev et al. 2008; Kipsaina et al. 2015), two reported the benefits of information security (n= 2; 13%) (Kiuchi et al. 2013; Colville-Ebeling et al. 2014)and 3 (20%) included the anonymization of data as a characteristic (Kiuchi et al. 2013; Aghayev et al. 2008; Colville-Ebeling et al. 2014). Some of the systems mentioned the use of their own data quality control measures (n= 7; 47%) (Dunstan 2019; Hargrove et al. 2018; Saar et al. 2017; Blair et al. 2016; Lyndal et al. 2016; Kiuchi et al. 2013; Canada 2012). Only six (37.5%) of the reported systems allowed for ease of data sharing/information exchange for the research and policy implementation (Dunstan 2019; Saar et al. 2017; Blair et al. 2016; Lyndal et al. 2016; Aghayev et al. 2008).
The data management and practice systems serve as repositories for information to inform about international best practices and supported the development of diagnostic models (Soto Martinez et al. 2019; Levy 2015; Fowler et al. 2018). The systems were also seen as a conduit for information sharing once privacy challenges were tackled (Levy 2015; Colville-Ebeling et al. 2014; Aghayev et al. 2008; du Toit-Prinsloo and Saayman 2012). The provision of data for research was a large contribution to most of the databases establishment (Soto Martinez et al. 2019; du Toit-Prinsloo and Saayman 2012; Dennis et al. 2018; Dunstan 2019; Fowler et al. 2018; Lyndal et al. 2016; Saar et al. 2017; Levy 2015; Pearse 2012; Kiuchi et al. 2013; Aghayev et al. 2008; Kipsaina et al. 2015; Colville-Ebeling et al. 2014). The systems contributed to the institution of preventative measures by identifying risk factors and by predicting the possible outcomes by using the data available in the reporting systems (du Toit-Prinsloo and Saayman 2012; Fowler et al. 2018; Blair et al. 2016; Lyndal et al. 2016). Improvement of surveillance and statistics related to epidemiology was notable in some studies (Saar et al. 2017; Ottaviani et al. 2017; Blair et al. 2016), and this further informed policy changes, contributed to the institution of new policies, and the reformation of laws (Bagher et al. 2015; Lyndal et al. 2016; Saar et al. 2017; Blair et al. 2016; Pearse 2012).
Challenges/limitations of the data management and practice systems
In one of the systems included for review, the authors described that data were captured voluntarily. This however led to inconsistencies, underreporting and time lag that impacted the usability of the data for research and epidemiology (PRISMA 2018; Dunstan 2019; Fowler et al. 2018; Hofmeister et al. 2017; Kipsaina et al. 2015). Some of the other challenges reported (n= 8; 53%) in service work and research included underreporting, low-case numbers, or use of closed cases only which generally impacted on epidemiology and research (Soto Martinez et al. 2019; Hargrove et al. 2018; Dennis et al. 2018; Saar et al. 2017; Blair et al. 2016; Lyndal et al. 2016; Kipsaina et al. 2015; Canada 2012). In the articles that cited data quality and validity challenges (n= 8; 53%) missing information was also reported as a limitation (Dunstan 2019; Fowler et al. 2018; Saar et al. 2017; Levy 2015; Blair et al. 2016; Lyndal et al. 2016; Colville-Ebeling et al. 2014). Data exchange and entry limitations were also reported as an issue (n= 8; 53%) (Dunstan 2019; Fowler et al. 2018; Saar et al. 2017; Hofmeister et al. 2017; Levy 2015; Lyndal et al. 2016; Aghayev et al. 2008), and these barriers may be in part be due to an inability to institute standardization practices for data capturing (n= 5; 33%) (Fowler et al. 2018; Dennis et al. 2018; Hofmeister et al. 2017; Levy 2015; Blair et al. 2016). Ethical considerations such as consent for autopsy or submitting data for analysis and research also impacted the use of the systems (n= 2; 13%) (Ottaviani et al. 2017; Kiuchi et al. 2013). Factors such as case-reporting bias, reporting errors, and bias in case selection also impacted case numbers and research (n= 4; 27%) (Soto Martinez et al. 2019; Blair et al. 2016; Lyndal et al. 2016; Canada 2012).
Discussion
This study sought to map the evidence on data management and practice systems in Forensic Medicine. The results show that several data management and practice systems exist. However, most of the existing systems were from high-income countries with few in LMICs based on this study’s eligibility criteria. This review was informed by the need to collect systematic evidence on the data management and practice systems being used in forensic medicine and the possible lessons and applicability to LMIC contexts where paper reporting is still being used. The lack of information on data management and practice systems is visible in that only two of the articles included for review reported on studies from the LMIC context. Half the publications (50%) were published during and after 2017. This trend may be due to the greater access, use, and reporting of electronic data reporting systems. The inclusion of Forensic Pathology reports on databases also captures information that is not routinely captured in vital registration statistics. The existing data management systems in forensic medicine reported in the included articles have several benefits. Nonetheless, the included articles also reported several challenges about those existing data management systems (see Fig. 2).

Countries where publications originated
To the best of our knowledge, this scoping review is the first present evidence on data management and practice systems in Forensic Medicine. Therefore, we cannot compare our findings. Nonetheless, the literature shows that electronic data reporting systems are relevant and were developed from the recognition of coronial data as not only a part of the death investigation but as a contributor to preventable death research and public health initiatives. For instance, in an article by Bruce Levy which discussed the United States of America systems currently in place to support Forensic Pathology and death investigation, the CDC implemented the National Violent death Reporting System in response to a report describing the need for a national fatal intentional injury surveillance system. Initially, the system started in six states but later was expanded to 18 states as stated in the publication (Fowler et al. 2018). According to the CDC website, and an article published in 2019 regarding its future directions, the program has now expanded to all 50 states and is constantly being updated and improved for data sharing (Blair et al. 2016; CDC, 2012). Other systems developed in the USA included a state-wide comprehensive multisource drug overdose fatality surveillance system in Kentucky (developed in response to drug overdoses cited as a public health crisis) and a database related to infant and child abuse (Soto Martinez et al. 2019; Hargrove et al. 2018). The burden of sudden infant death syndrome and the large number of cases that remain unexplained led to the passing of legislation in Italy (2006) that fetuses and infants, from 25 weeks of gestation to one postnatal year, who died suddenly and unexpectantly should be sent to the University of Milan, Italy, for a postmortem with parental consent (Ottaviani et al. 2017). An Italian research center developed a web portal for a national bank registry which has been set up to centralize records retrieved from regions across Italy which hopes to contribute data for epidemiology and study into risk factors for sudden unexpected death in infants. Canada instituted a National Coroner and Medical Examiner database to detect emerging trends and hazards for the prevention of avoidable deaths (Canada 2012). Tokyo is recognized as a technology hub, and the latest inclusion of a Legal Medicine Information System for forensic systems is discussed in an included article (Kiuchi et al. 2013). Using the information system, Forensic Pathologists and other staff can register and search for institutional autopsy information, print death certificates, and extract data for research and analysis. Switzerland created a tool called the Virtopsy-a centralized database in Forensic Medicine for analysis and comparison of radiological and autopsy findings (Aghayev et al. 2008). It is a database currently created but not in routine use as it has not been validated. The database compares autopsy and radiological data with photograph storage. In the Nigerian study, recognition of the poorly representative mortality injury surveillance system prompted the authors to institute an electronic injury surveillance system (Kipsaina et al. 2015). The system included features based on a South African initiative namely the National Injury Mortality Surveillance System (NIMSS) which due to logistical reasons and lack of funding was deemed unfeasible and discontinued (Prinsloo 2019). Articles related to NIMSS did not meet the inclusion criteria of the current study. Although the tools that were utilized were already existing making the system feasible and sustainable, but an appropriate infrastructure needs to be in place to maintain the system (Prinsloo 2019).
The recognition and understanding of violent deaths require the collection of accurate, timely, and comprehensive surveillance data to implement preventative measures (du Toit-Prinsloo and Saayman 2012; Prinsloo 2019; Saar et al. 2017; Blair et al. 2016; Pearse 2012). The wealth of information collected by Forensic Pathologists can be effectively used in public health and safety initiatives, policies, and legislation (Dunstan 2019; Fowler et al. 2018; Blair et al. 2016). The databases have been credited as an evidence base for awareness-raising and death prevention initiatives informing research, policy development, and coronial investigation (Dunstan 2019; Blair et al. 2016). It encourages information exchange, standardization, and implementation of investigation protocols, and research. It has contributed to the publication of more than a hundred articles in a broad range of journals (Blair et al. 2016; Lyndal et al. 2016). Access, tracking, and centralization of data can result in the improvement of scientific and investigative processes with the implementation of international standards and best practices (Fowler et al. 2018; Saar et al. 2017; Blair et al. 2016; Kiuchi et al. 2013). The implementation of the system improved the quality of the surveillance data and the standardization of data. Furthermore, using and linking multiple sources of data-enabled valuable information to be extracted and translated for the identification of vulnerable populations at risk and provided evidence to implement a new legislature (Fowler et al. 2018; Levy 2015). It can be cost-effective and impact public health to reduce waste of resources and improve public initiatives. This data can further be used to develop diagnostic models to better inform clinical decision-making (Soto Martinez et al. 2019). It was recognized that the tool used must be comprehensive and adaptable as data management systems are indispensable as part of forensic investigations (Hofmeister et al. 2017; Levy 2015). It can be remodeled to an online platform that simplified system operations and management, improved timeliness of reporting, and increased adaptability which creates an opportunity for expansion to multiple sites.
There were several limitations discussed which primarily involved feasibility of the system, accuracy, availability, and completeness of data, involvement of relevant stakeholders, and the absence of morbidity data (Lyndal et al. 2016). Collaboration may address challenges of sharing and merging and analyzing of data. Developing policies regarding storage, quality review, and access of the data for analysis may address privacy challenges. Important issues discussed included the protection of data privacy which can be overcome by anonymization of data on the central server and the case sensitive information can be stored on the local server (Kiuchi et al. 2013; Aghayev et al. 2008). The use of the Internet can be a cost-effective solution whereas more sophisticated databases require time and resources and a necessary framework that involves policies, staff, training, quality control, and support. The issues relating to the systems are the limited resources for death investigations (both human factors and technology). The involvement of various stakeholders to support data-sharing programs in Forensic Pathology can relieve the financial strain (Dunstan 2019; Fowler et al. 2018; Hargrove et al. 2018; Dennis et al. 2018; Saar et al. 2017; Hofmeister et al. 2017; Ottaviani et al. 2017; Levy 2015). The Forensic Medicine Departments can utilize simple and available tools that can advance standardization of data collection, storage, and reporting because of the central role they play in reporting provincial/national data (Kipsaina et al. 2015). The reviewed articles included a great variety of systems that could lend themselves to use in LMIC contexts. Apart from its limitations, the autopsy/coronial data reporting systems are recognized as an essential tool for monitoring the prevalence and incidence of violence related to fatal injuries.
Strengths and limitations
This study is the first scoping review that systematically mapped literature relating to data practices in Forensic Medicine globally. A major strength of our study method is that it permits the inclusion of all study designs and the development of a protocol that ensures reproducibility. Moreover, we conducted a thorough search using a comprehensive search strategy which enabled us to capture the most relevant articles to answer the review question. However, the articles selected were limited to Forensic Medicine, keywords, and its data collection methods of autopsy records; therefore, articles that entail electronic methods for the data collection in other medical departments were excluded. The limitation was due to the focus of the study being on the value of these systems to preventative programs rather than treatment. The keywords to be used in the search strategy are broad and may not identify specialized studies in data management. Only articles in English will be used. Nonetheless, the finding produced by this study is useful to inform further research, particularly LMICs.
Recommendations
The general consensus from the articles is that a data management and practice system containing coronial/medical examiner/Forensic Pathology data is beneficial for research, policymaking, prevention strategies, and information exchange for education. Due to resource limitations in some low- to middle-income countries, the database can be done by using available resources to create a limited database (Kipsaina et al. 2015). Although if multiple stakeholders can be involved to formulate and fund a nationally representative information system, this can be wholly beneficial, not only to the community and government but may also impact on private companies with regard to product development and reformation due to its comprehensive coverage of preventable deaths (Dunstan 2019; Hargrove et al. 2018; Saar et al. 2017; Blair et al. 2016; Lyndal et al. 2016).
Conclusions
This scoping review summarized the evidence on data management and practice systems and their benefits and challenges in forensic medicine. The very appropriate use of words in an article’s title “Saving Lives Through the Power of Data” reiterates the appropriate use of information from preventable deaths. The imperative to use autopsy data for statistically relevant but also representative data can be time-consuming and an arduous task. The electronic systems, ranging from the most sophisticated (NCIS, NVDRS, Virtopsy Switzerland, Tokyo CDISC/ODM) to those created considering resource limitations (Nigerian trial), are cited as beneficial to the pathologist, researchers and for public health. The limitations to implementing electronic systems may include the reluctance of various stakeholders (such as government agencies) to participate and the need for additional funding to sustain more sophisticated database systems. However, the use of simple and available tools such as in the Nigerian trial still managed to contribute to statistically relevant data for impactful research.
Availability of data and materials
All data generated or analyzed during this study will be included in the published scoping review article.
Abbreviations
- CADS:
-
Central Anonymous Database System and IDS Institutional Database System (Part of CDISC/ODM Clinical Data Interchange Standards Consortium Operational Data Model)
- CDC:
-
Centres for Disease Control and Prevention
- ICRC AM/PM Database:
-
International Committee of the Red Cross Antemortem/Postmortem Database
- LMIC:
-
Low- to middle-income countries
- IID:
-
Infant Injury Database
- MeSH:
-
Medical Subject Headings
- NCIS:
-
National Coronial Information System
- NIMSS:
-
The National Injury Mortality Surveillance System
- NVDRS:
-
National Violent death Reporting System
- WHO:
-
World Health Organization
References
Aase S (2013) Autopsy-still the gold standard? Tidsskr nor Legeforen 133(7):730–731
Aghayev E, Staub L, Dirnhofer R, Ambrose T, Jackowski C, Yen K et al (2008) Virtopsy - the concept of a centralized database in forensic medicine for analysis and comparison of radiological and autopsy data. J Forensic Leg Med 15(3):135–140
Arksey H, O’Malley L (2005) Scoping studies: towards a methodological framework. Int J Soc Res Methodol 8:19–32
Bagher A, Wingren CJ, Ottosson A, Andersson L, Wangefjord S, Acosta S (2015) Necessity of including medico-legal autopsy data in epidemiological surveys of individuals with major trauma. Injury 46(8):1515–1519
Barbería E, Gispert R, Gallo B, Ribas G, Puigdefàbregas A, Freitas A et al (2018) Improving suicide mortality statistics in Tarragona (Catalonia, Spain) between 2004–2012. Revista Psiquiatr Salud Mental 11(4):227–233
Blair JM, Fowler KA, Jack SP, Crosby AE (2016) The National Violent Death Reporting System: overview and future directions. Inj Prev 22 Suppl 1(Suppl 1):i6-11
CDC (2012) National Violent Death Reporting System. Available from: https://www.cdc.gov/violenceprevention/datasources/nvdrs/index.html.
Choo T, Choi Y-S (2012) Historical development of forensic pathology in the United States. Korean J Legal Med 36:15
Colville-Ebeling B, Frisch M, Lynnerup N, Theilade P (2014) HOMED-homicides eastern Denmark: an introduction to a forensic medical homicide database. Scand J Public Health 42(7):683–686
Dennis M, Elder A, Semsarian C, Orchard J, Brouwer I, Puranik R (2018) A 10-year review of sudden death during sporting activities. Heart Rhythm 15(10):1477–1483
du Toit-Prinsloo L, Saayman G (2012) Performance of autopsies in South Africa: selected legal and ethical perspectives
Dunstan L (2019) The national coronial information system: saving lives through the power of data. Aust Econ Rev 52(2):247–254
Fowler K, Jack S, Lyons B, Betz C, Petrosky E (2018) Surveillance for violent deaths - national violent death reporting system, 18 States, 2014. MMWR Surveill Summ 67:1–36
Grills NJ, Ozanne-Smith J, Bartolomeos K (2011) The mortuary as a source of injury data: Progress towards a mortuary data guideline for fatal injury surveillance. Int J Inj Contr Saf Promot 18(2):127–134
Hargrove SL, Bunn TL, Slavova S, Quesinberry D, Corey T, Ralston W et al (2018) Establishment of a comprehensive drug overdose fatality surveillance system in Kentucky to inform drug overdose prevention policies, interventions and best practices. Inj Prev 24(1):60–67
Hofmeister U, Martin SS, Villalobos C, Padilla J, Finegan O (2017) The ICRC AM/PM database: challenges in forensic data management in the humanitarian sphere. Forensic Sci Int 279:1–7
Kipsaina C, Eze UO, Ozanne-Smith J (2015) A standardised mortuary-based injury surveillance system: lessons learned from the Ibadan Nigerian trial. Int J Inj Contr Saf Promot 22(3):193–202
Kiuchi T, Yoshida K-i, Kotani H, Tamaki K, Nagai H, Harada K et al (2013) Legal medicine information system using CDISC ODM. Legal Med 15(6):332–4
Koehler SA (2016) Chapter 7 - death investigation. In: Freeman MD, Zeegers MP (eds) Forensic Epidemiology. Academic Press, Amsterdam, pp 179–199
Levy B (2015) The need for informatics to support forensic pathology and death investigation. J Pathol Inform 6:32
Lyndal B, Joseph EI, Noha F, Briony M, Melissa W, David R (2016) The utility of medico-legal databases for public health research: a systematic review of peer-reviewed publications using the National Coronial Information System. Health Res Policy Syst. 14(1):28. Available from: https://doi.org/10.1186/s12961-016-0096-1.
McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C (2016) PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol 75:40–46
Ottaviani G, Perlasca P, Mesiti M, Ferrari L, Lavezzi AM (2017) Authorised access web portal for Italian data bank on sudden unexpected perinatal and infant death. Acta Paediatr 106(7):1196–1197
Pan M, Wang X, Zhao Y, Liu W, Xiang P (2019) A retrospective analysis of data from forensic toxicology at the Academy of Forensic Science in 2017. Forensic Sci Int 298:39–47
Pearse J (2012) The National Coronial Information System: a decade of challenges and achievements. Inj Prev 18(Suppl 1):A22. Available from: https://injuryprevention.bmj.com/content/injuryprev/18/Suppl_1/A22.1.full.pdf.
Prahladh S, van Wyk J (2020) Protocol for a scoping review of the current data practices in forensic medicine. Syst Rev 9(1):76
Prinsloo M (2019) Estimating injury mortality in South Africa and identifying urban-rural differences
Rao C, Lopez AD, Yang G, Begg S, Ma J (2005) Evaluating national cause-of-death statistics: principles and application to the case of China. Bull World Health Organ 83(8):618–625
Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N et al (2018) Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392(10159):1736–1788
Saar E, Bugeja L, Ranson DL (2017) National coronial information system: epidemiology and the coroner in Australia. Acad Forensic Pathol 7(4):582–590
Salona Prahladh TN (2018) Missed injuries in motor vehicle accidents: autopsy vs clinical findings. Surg Chron 23(2):105–111
Soto Martinez ME, Love JC, Pinto DC, Wiersema JM, Derrick SM, Bachim A et al (2019) The infant injury database: a tool for the study of injury patterns in medicolegal investigations of child abuse. J Forensic Sci 64(6):1622–1632
Statistics Canada (2012) Canadian Coroner and Medical Examiner Database: Annual Report. Available from https://www150.statcan.gc.ca/n1/en/catalogue/82-214-X2012001
Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tunçalp Ö, Straus SE (2018) PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 169(7):467–473. https://doi.org/10.7326/M18-0850. Epub 2018 Sep 4
Tseng ZH, Olgin JE, Vittinghoff E, Ursell PC, Kim AS, Sporer K et al (2018) Prospective countywide surveillance and autopsy characterization of sudden cardiac death: POST SCD study. Circulation 137(25):2689–2700
Willcox ML, Price J, Scott S, Nicholson BD, Stuart B, Roberts NW et al (2020) Death audits and reviews for reducing maternal, perinatal and child mortality. Cochrane Database Syst Rev 3(3):CD012982
Acknowledgements
Special thanks to Dr. Desmond Kuupiel who assisted in designing the database search strategy and text screening of the articles. We also thank the staff from the UKZN Medical School library for assisting in obtaining full-text articles for the review.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
The first author conceptualized the study and prepared the scoping review under the supervision of the second author. Both first and second authors contributed to the development of the background, design of the study, and planned output of the research. The first author prepared the manuscript and the second author reviewed it. The abstract and full-text screening was conducted by the first author and an external reviewer to ensure transparency and reduce bias. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Although research ethics approval was not required for this scoping review because the study did not include human or animal participants, the study was approved by an ethics committee. Data was sourced only from published literature and gray literature.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Prahladh, S., van Wyk, J. Introductory evidence on data management and practice systems of forensic autopsies in sudden and unnatural deaths: a scoping review. Egypt J Forensic Sci 12, 38 (2022). https://doi.org/10.1186/s41935-022-00293-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41935-022-00293-3