
Abstract
Purpose
This study aimed to assess the biodistribution, detection rate, and uptake of the [18F]FAPI-42 at two distinct time intervals.
Methods
This prospective study enrolled 60 consecutive patients (median age 59; range 35–74) referred to [18F]FAPI-42 PET/CT. [18F]FAPI-42 PET/CT was performed early and late timepoint after tracer injection for staging or restaging. Positive lesions specified for anatomic locations (primary or recurrent tumor, LN metastasis and other metastasis) by visual analysis at both timepoints. Semiquantitative analysis of the tracer activity in lesions as well as normal tissues at both time points were measured and compared. In a subgroup analysis, eleven patients underwent 2-[18F]FDG PET/CT within 1 week, the detection rate and uptake of lesion were compared between early [18F]FAPI-42 and 2-[18F]FDG.
Results
Uptake of [18F]FAPI-42 in the late timepoint was significantly lower than the early timepoint in most organs (all p < 0.05), except for bone (SUVmean 0.88 vs. 0.85; p = 0.218). Tracer retention at biliary system showed less frequent at early timepoint than late timepoint. A total of 194 lesions were detected in 60 patients. One lesion was only seen at early timepoint but not at late timepoint. Lesions on early [18F]FAPI-42 PET/CT had higher visual score than that of late image(23 vs. 6). The uptake of lesion decreased significantly from early to late timepoint (all p < 0.05). In subgroup analysis, early [18F]FAPI-42 illustrated higher detection rate, visual score, and uptake of lesion than that of 2-[18F]FDG PET/CT.
Conclusion
Early [18F]FAPI-42 PET/CT provided consistent detection rates and lesion uptake, but less tracer retention in the biliary system compared to late images. Therefore, acquisition at early timepoint could be a feasible strategy for improving acquisition protocols of [18F]FAPI-42 PET/CT.
Trial registration: ChiCTR2200063441. Registered 28 September 2022—Retrospectively registered, https://www.chictr.org.cn/bin/project/edit?pid=149714.
Similar content being viewed by others


Introduction
Fibroblast activation protein (FAP) is abundantly expressed in cancer-associated fibroblasts (CAFs) within the tumor microenvironment, while its presence in healthy tissues is minimal (Loktev et al. 2018). The introduction of FAP-specific small molecule inhibitors, known as FAPI, for positron emission tomography (PET) imaging marked a significant milestone (Kratochwil et al. 2019; Giesel et al. 2019). Numerous studies have since highlighted their rapid clearance from the body, outstanding diagnostic efficacy, and impressive tumor-to-background ratios (TBR) in detecting a variety of cancers (Wass et al. 2023; Yang et al. 2023; Hirmas et al. 2023). Given the observed attributes of FAPI PET, it shows potential in contributing to the determination of the TNM stage and could have implications for clinical decision-making in cancer treatments (Koerber et al. 2023). In some types of cancer, FAPI PET demonstrated even better tumor detection and staging, contrasting with 2-[18F]FDG on oncologic PET/computed tomography (CT) imaging (Yang et al. 2023).
Currently, molecular imaging probes targeting FAP predominantly utilize Gallium-68 (68 Ga) for PET imaging (Mori et al. 2023). Among these, 68[Ga]Ga-FAPI-04 and 68[Ga]Ga-FAPI-46 stand out as the most employed tracers, with exceptional diagnostic capabilities and notably straightforward workflow, such as no need for a complex fasting process, and short interval time from injection to acquisition (Ferdinandus et al. 2021). However, while these attributes underscore the benefits of 68[Ga]Ga-FAPI, its widespread clinical application is constrained by the short half-life of 68 Ga, elevated costs, and limited availability of radionuclides from the 68Ge/68 Ga generator (Mori et al. 2023).
The application of 18F-labeled FAPI compounds presents a compelling alternative, enhancing the performance limit in the clinical routine. Specifically, [18F]FAPI boasts benefits such as high production accommodating more examinations per batch, facilitating multicenter transportation, and delivering high-resolution imaging (Mori et al. 2023). Compared to 68[Ga]Ga-FAPI, [18F]FAPI exhibit similar characteristics, biodistribution and tracer kinetics, such as high affinity to tumor, swift renal clearance and minimal non-specific uptake in normal tissue (Hu et al. 2022). That made that [18F]FAPI has performed promising diagnostic performance for various cancers (Yang et al. 2023; Zhang et al. 2023; Watabe et al. 2023; Yao et al. 2022). However, a distinction between 68 Ga- and 18F-FAPI lies in the chelator (normally DOTA for 68[Ga]Ga-FAPI; NOTA for [18F]FAPI). This leads to increased lipophilicity in [18F]FAPI, resulting in excretion through the biliary system. Consequently, this may impact the visualization of gastrointestinal lesions and reduce its diagnostic efficacy (Wang et al. 2021).
In most of these studies, static PET acquisition was performed at an hour after the injection of [18F]FAPI (Yang et al. 2023; Qiao et al. 2023). While some research has identified 10–30 min as an optimal timepoint for 68[Ga]Ga-FAPI PET acquisition (Naeimi et al. 2023; Glatting et al. 2022), the ideal timepoint for [18F]FAPI PET remains unclear. Dynamic scans of [18F]FAPI-42 PET/CT from a prior study revealed that tumor activity peaked at 18 min and then began to decrease, with gallbladder activity increasing thereafter (Hu et al. 2022). In preclinical assessment, tumor presented highest uptake on early [18F]FAPI-42 PET/CT (Huang et al. 2023). These findings prompted us to investigate the variations between early and late timepoints for [18F]FAPI-42 PET/CT in cancer imaging.
In this study, we assessed the biodistribution, detection rate, and tumor uptake of [18F]FAPI-42 across various cancers between early and late for [18F]FAPI-42 PET/CT. Additionally, in a subset of patients, the detection rate and tumor uptake on early [18F]FAPI-42 PET/CT was compared to that of 2-[18F]FDG PET/CT.
Methods and materials
Study design and patients
This study received approval from the Ethics Committee of our hospital (Approval No. 2022WJWZCLL-01) and was registered in the Chinese Clinical Trial Registry (ChiCTR2200063441). Every participant provided written informed consent.
Between August 2022 and July 2023, 65 patients were consecutively enrolled from The Affiliated Hospital of Guilin Medical University. Patients were referred for one of three primary reasons:1. Determining lesion characteristics and disease severity 2. Restaging due to inconclusive findings on conventional imaging 3. Regular follow-up. Five patients were excluded in analysis due to patients with non-oncology disease. Finally, 60 patients were analyzed.
Radiopharmaceuticals and PET/CT imaging
The Affiliated Hospital of Guilin Medical University's Department of Nuclear Medicine routinely synthesized 2-[18F]FDG using standardized procedures. The synthesis and labeling of [18F]AlF‑NOTA‑FAPI‑42 (abbreviated as [18F]FAPI-42) have been previously documented (Mu et al. 2023). Both 2-[18F]FDG and [18F]FAPI-42 maintained a radiochemical purity of over 95%.
In each patient, whole-body [18F]FAPI-42 PET was acquired twice: early (mean 22 min) and late (mean 73 min) after injection of radiotracer. Eleven patients underwent sequential 2-[18F]FDG and [18F]FAPI-42 PET/CT scans within a week. The 2-[18F]FDG PET/CT protocols adhered to the European Association of Nuclear Medicine's international guidelines (Boellaard et al. 2015). All images were captured using the Ingenuity TF PET/CT scanner (Philips, Amsterdam, Holland). A low-dose CT scan (tube voltage: 120 kV, tube current: 50 mAs, slice thickness: 5.0 mm, pitch: 1.0) was first taken for attenuation correction, followed by PET imaging (2.5 min per bed position, 6–7 PET bed positions).
Image interpretation
All images were interpreted by Q.J. and Z.L. with more than 5 years of experience in PET interpretation. These specialists were unaware of the 2-[18F]FDG PET/CT outcomes when evaluating the [18F]FAPI-42 PET/CT. Image assessments encompassed both visual analysis and quantitative measurement. Consensus was reached after discussions. Elevated 2-[18F]FDG/[18F]FAPI-42 uptake, paired with anomalies in CT density or signals, was deemed positive after ruling out physiological uptake, trauma, infection, and inflammation. The number of lesions was recorded and categorized by region: primary tumor or recurrence, metastatic lymph nodes, as well as distant metastasis. A visual scoring system was developed to assess lesion detection capabilities. This system, detailed in previous studies (Liu et al. 2023; Qin et al. 2022), was based on three criteria: lesion area, count, and tracer uptake. The scoring system was applied to compare lesions detected by early [18F]FAPI-42 PET with those by late [18F]FAPI-42 PET and 2-[18F]FDG PET. The detail of this visual scoring system was depicted in Additional File 1.
Tracer uptake and biodistribution in normal organs were quantified using mean standardized uptake values (SUVmean)at both early and late timepoints. For the evaluation of these organs: Specific region of interest (ROI) measurements was employed. For smaller organs like the thyroid, parotid gland, and salivary glands, a spherical ROI with a 1 cm diameter was used. For larger organs such as the brain, muscle, liver, pancreas, spleen, kidney, aortic lumen content (blood pool), lung, and bone, a 2 cm diameter spherical ROI was adopted. The ROI was placed entirely within the organ parenchyma. The presence of biliary and intestinal tracer retention and was recorded for both late and early time-points. The tracer uptake of each lesion was assessed using multiple SUV metrics, including maximum standardized uptake values (SUVmax), SUVmean, and peak standardized uptake values (SUVpeak), at both early and late timepoints. For SUV calculations: Circular volumes of interest were manually outlined around tumor lesions on trans-axial slices at the late timepoint. These were then automatically transferred to images from the early timepoint using the MedEx software (MedEx Technology Limited Corporation, China), with a 3-dimensional ROI set at a 40% iso-contour. Image contrast was quantified using tumor-to-background ratios (TBR). The formula employed the ratio of SUVmax of the lesion to the SUVmean of background tissue, which included measurements from the blood pool (TBRblood) and liver (TBRliver) tissue at both early and late timepoints, respectively.
Statistics
Statistical evaluations were conducted using IBM SPSS Statistics version 26.0 and GraphPad Prism version 9.0. Continuous variables are depicted as [median (IQR)], while categorical variables are shown as [n, (%)]. Chi-square tests were used to compare presence of biliary and intestinal tracer retention between two timepoints. The Wilcoxon matched-pairs signed-rank test was employed to compare tracer uptake in normal organs and lesions between two timepoints as well as that in 2-[18F]FDG. All tests were two-sided, with p < 0.05 denoting statistical significance.
Results
Between August 2022 and July 2023, 65 patients were consecutively enrolled in this study. Five were excluded due to benign diseases, resulting in 60 patients for the analysis. Of these, 25 patients underwent [18F]FAPI-42 PET/CT for primary staging, while 35 were assessed using [18F]FAPI-42 PET/CT for restaging. Eleven patients underwent 2-[18F]FDG within 1 week. Baseline patient characteristics are provided in Table 1.
Biodistribution in normal organs
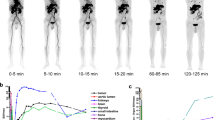
The biodistribution of normal organs at the early and late [18F]FAPI-42 PET/CT is depicted in Fig. 1a. Uptake of [18F]FAPI-42 in the late timepoint was significantly lower than the early timepoint in most organs (14 out of 15 organs, all p < 0.05), except for bone (SUVmean 0.88 vs. 0.85; p = 0.218; Additional file 1: Table S1). In early vs. late imaging, tracer retention in biliary was presented in 34/60 (56.7%) vs. 52/60 (86.7%) patients respectively (p < 0.001), and intestinal 3/60(5%) vs. 18/60(30%) patients, respectively (p < 0.001) (Fig. 1b).

a SUVmean of normal organs at early and late timepoint in patients with cancer on [18F]FAPI-42 PET/CT. b The tracer retention of biliary and intestinal between early and late timepoint on [18F]FAPI-42 PET/CT. Vertical bar with error bar shows the mean with standard error
Visual and quantitative evaluation
In total, 194 lesions were detected in 60 patients. Lesions were rated as primary or recurrent lesions (29/194, 19.8%), lymph node metastasis (100/194, 21.5%), or other metastasis (65/194, 5.8%). Representative images were shown in Fig. 2. One of 194 (0.05%) of lesions were seen in early timepoint imaging but not in late timepoint imaging. That is a patient with differentiated thyroid cancer, referred for a metastatic bone assessment following a total thyroidectomy and 131-iodine ablation therapy (Fig. 3). For this case the disease stage did not change, as other lesions of the same region were visible. No additional lesions were observed on late imaging. For visual scoring system, there was a higher visual score was observed on early imaging (23 vs. 6, Fig. 4a).

Maximum-intensity-projection images of [18F]FAPI-42 PET/CT at early and late timepoint in different types of cancer. NSCLC = Non-small cell lung cancer; HNSCC = Head and neck squamous cell carcinoma

A 49-year-old woman with multiple bone metastasis of differentiated thyroid cancer. a Comparison of maximum-intensity projection images between early and late [18F]FAPI-42 PET (lesions indicated by arrows). b PET/CT images on early and late [18F]FAPI-42 PET (arrows indicate metastatic lesions). Early [18F]FAPI-42 PET detected more metastatic bone lesions than late [18F]FAPI-42 (SUVmax of humerus lesion is 4.9 and 2.4, respectively; SUVmax of vertebrae is 7.6 and 6.4, respectively; SUVmax of femur is 4.8 and 4.1)

Comparison of visual score between early and late [18F]FAPI-42 PET in primary lesions, LN metastasis, and other metastasis (a) and visual score of lesions on early [18F]FAPI-42 PET compared with 2-[18F]FDG PET (b). LNM = Lymph node metastasis; M = Metastasis
Overall, the uptake of all lesions statistically decreased over time (median SUVmax: 4.6 vs. 4.6; SUVmean: 2.9 vs. 2.8; SUVpeak: 3.7 vs. 3.2, all p < 0.05; Fig. 4a). However, for individual anatomical regions, including primary or recurring lesions (median SUVmax: 6.3 vs. 5.9, p = 0.08), lymph nodes (median SUVmax: 4.3 vs. 4.2, p = 0.12), and distant metastases (median SUVmax: 4.6 vs. 4.6, p = 0.38), no statistically significant differences in SUVmax between the early and late scan were observed (Fig. 5a). Furthermore, the SUVmean and SUVpeak of all lesions were evaluated based on their anatomical locations (Fig. 5b, Additional file 1: Fig. S1). While the [18F]FAPI-42 activity in lesions showed higher uptake in the early scan compared to the late scan, the TBR increased over time due to a significant decrease in background activity from the early to late timepoint. Consequently, statistical analysis revealed a significant decrease in the median TBR blood and TBR liver across all lesions (median 3.2 vs. 4.8, 4.6 vs. 7.7; all p < 0.001, respectively, Fig. 5), irrespective of their specific anatomical locations (Additional file 1: Fig. S1).

Comparison of uptake on [18F]FAPI-42 PET between early and late [18F]FAPI-42 PET: SUVmax in all lesions, primary lesions, LN metastases, and other metastases (a); SUVmean, SUVpeak, TBRblood and TBRliver on [18F]FAPI-42 PET between early and late timepoint in all lesions (b). LN = Lymph nodes; SUVmax = Maximum standardized uptake value; SUVmean = Mean standardized uptake value; SUVpeak = Peak standardized uptake value; TBR = Tumor-to-background ratio. Vertical bar shows the mean
Comparative analysis of early [18F]FAPI-42 and 2-[18F]FDG PET/CT
Table 2 presents the lesions between early [18F]FAPI-42 and 2-[18F]FDG in eleven patients. On the early [18F]FAPI-42 PET/CT, 57 malignant lesions were identified, in contrast to the 51 lesions spotted on 2-[18F]FDG PET/CT. Collectively, the visual scores for these patients were elevated in the early [18F]FAPI-42 PET/CT compared to 2-[18F]FDG PET/CT (22 vs. 7; Fig. 4b). In a quantitative assessment, the SUVmax for lesions was higher in the early [18F]FAPI-42 PET/CT than in 2-[18F]FDG PET/CT, though the difference wasn't statistically significant (median SUVmax, 5.3 vs. 4.8, p = 0.818; Fig. 5). Similarly, there was no significant difference in the TBRblood ratio for lesions between the two scans (median TBRblood 2.9 vs. 3.1, p = 0.282; Fig. 6). Yet, when using liver radioactivity as a reference, the TBRliver exhibited greater uptake in the early [18F]FAPI-42 PET/CT than in 2-[18F]FDG PET/CT (median TBRliver 3.6 vs. 2.4, p = 0.057; Fig. 5). Representative PET images are presented in Fig. 7.

Quantitative comparisons (left, SUVmax; middle, TBRblood; right, TBRliver) between early [18F]FAPI-42 and 2-[18F]FDG in all lesions; SUVmax = Maximum standardized uptake value; TBR = Tumor-to-background ratio

Maximum-intensity-projection images of early [18F]FAPI-42 and 2-[18F]FDG PET/CT in patients with different types of cancer. HCC = Hepatocellular carcinoma; DTC = Differentiated thyroid carcinoma; NSCLC = Non-small cell lung cancer
Discussion
In this study, we compared the biodistribution, tracer retention, lesion detection, and uptake of early and late [18F]FAPI-42 PET. Both time points showed equal lesion detection; however, there was less tracer retention in the biliary system for the early time point. The uptake of normal organs and lesions was significantly higher for early PET acquisition, but it did not have a relevant impact on lesion detection or tumor staging due to the higher TBR for late acquisition. Furthermore, in some patients, early [18F]FAPI-42 PET demonstrated higher lesion detection and TBR compared to 2-[18F]FDG.
Hu et al. previously reported a rapid decrease in radioactivity in normal organs and satisfactory retention in tumors using [18F]FAPI-42 PET/CT with dynamic acquisition (Hu et al. 2022). Consistent with their findings, our study observed a similar decline in radioactivity from early to late imaging in normal organs, with no significant difference observed in bone tissue (median SUVmean 0.88 vs. 0.85; p = 0.218). In contrast to 68[Ga]Ga-FAPI, the lipophilicity of [18F]FAPI leads to substantial accumulation in the biliary tract system, potentially limiting the detection of gastrointestinal lesions. Fortunately, our research suggests that early [18F]FAPI-42 imaging may reduce tracer accumulation in the biliary system, mitigating this drawback. Although some published studies have suggested that modifying [18F]FAPI ([18F]FAPT) can reduce hepatobiliary physiological excretion of 18F-labeled FAPI tracers, high tracer accumulation in other organs were observed up to 120 min after injection (Huang et al. 2023). Presently, no available data demonstrate whether this substantial accumulation in these organs will impact the diagnostic performance of [18F]FAPT. In this context, early acquisition appears to be a feasible strategy for [18F]FAPI-42, which is the most frequently utilized 18F-labeled FAPI tracer, as it helps mitigate the impact of excretion.
In a study by Ferdinandus et al., a comparison was conducted between early imaging (approximately 10 min post-injection) and late imaging (approximately 60 min post-injection) using [68 Ga]Ga-FAPI-46. They reported an equivalent detection rate between these two time points. Interestingly, they observed two lesions that were only visible in the early time point, although this did not alter the staging for the patients (Ferdinandus et al. 2021). They investigated three different time points for imaging with [68 Ga]Ga-FAPI-46 in various types of cancers (10 min, 60 min, and 180 min post-injection). Surprisingly, they found a similar detection rate among the three time points (Naeimi et al. 2023). Consistent with these earlier findings, our study also revealed an equal detection rate between the early and late timepoints for [18F]FAPI-42. This emphasizes the advantages of early time point acquisition for [18F]FAPI-42, as it maintains an equal detection rate while streamlining workflow and reducing patient waiting times.
Regarding lesion uptake, Ferdinandus et al. demonstrated that the mean SUVmax of lesions reached its peak at 10 min (8.2) and exhibited a slight decline at 1 h (8.15) and 3 h (7.6) after tracer administration (Naeimi et al. 2023). This observation is consistent with earlier reports, which indicated that lesion uptake reaches its peak around 20–30 min, followed by a gradual decrease until the 120-min mark. Our own data substantiate these findings, confirming the decline in lesion uptake over time. Moreover, in conjunction with the elevated lesion uptake, we noted a higher visual score for lesions in the early [18F]FAPI-42 images (23 vs. 6). Crucially, this outcome remained consistent and was not affected by a substantial increase in TBR for lesions over time. This observation can be valuable for aiding physicians in the interpretation of lesions on early [18F]FAPI-42 images. Notably, there was a significant discrepancy where one lesion was missed in late time-point imaging but detected in early timepoint imaging. We speculate that this inconsistency is linked to the decline in lesion uptake over time. Based on these findings, we can infer that a short waiting period after [18F]FAPI-42 administration suffices for effective lesion detection. Theoretically, a longer delay image of [18F]FAPI-42 (up to 120 min or more) may not be recommended, because prolonged delayed time does not yield higher tumor uptake. Therefore, even in cases where certain patients may require dual-time imaging with [18F]FAPI-42 to differentiate the nature of lesions, utilizing the early and late timepoints may be sufficient.
Despite the relatively complex preparation requirements, which include fasting, maintaining appropriate blood sugar levels, and extended waiting times, 2-[18F]FDG continues to serve as a well-established late for diagnostic imaging in various cancer types and as a guide for treatment planning. Consistent with existing literature, our research has demonstrated that early [18F]FAPI-42 detected more postive lesions than that of 2-[18F]FDG PET/CT (Yang et al. 2023; Wu et al. 2022; Lyu et al. 2023). Although there were no significant differences in SUVmax values for lesions between early [18F]FAPI-42 and 2-[18F]FDG, early [18F]FAPI-42 yielded higher visual scores for lesions, potentially attributed to the elevated TBR of lesions in early [18F]FAPI-42 (Lyu et al. 2023). However, despite the promising detection capabilities of [18F]FAPI-42, solely relying on imaging the tumor microenvironment with [18F]FAPI-42 may not be universally recommended or consistently adequate for the diagnostic assessment of malignant diseases, owing to inherent tumor heterogeneity. Given the distinct mechanisms of action and tracer retention, 2-[18F]FDG and [18F]FAPI-42 PET/CT may serve as complementary tools, capturing different aspects of tumor biology. Our results suggest that early [18F]FAPI-42 can serve as a valuable complementary tool alongside 2-[18F]FDG. This approach capitalizes on high lesion uptake and clinical feasibility, potentially leading to increased scan volumes, streamlined workflows, and reduced spatial requirements in the nuclear medicine department.
Our study has several limitations that should be considered. Firstly, one limitation stems from the absence of histological confirmation of the lesions. We did not include accuracy assessment as an endpoint, and formal lesion validation was not part of this analysis. This limitation could potentially result in the misclassification of lesions. Secondly, due to the limited number of patients underwent paired 2-[18F]FDG PET/CT in the study, reliable comparisons among different tumor types were not possible. Therefore, any conclusions drawn from our data comparing early [18F]FAPI-42 and 2-[18F]FDG should be made with caution.
Conclusion
In conclusion, when compared to the late approach, early [18F]FAPI-42 PET acquisition yielded comparable lesion detection rates but exhibited higher lesion uptake and visual scores at an early timepoint. In a subgroup analysis, early [18F]FAPI-42 depicted more positive lesions with higher TBR than that of 2-[18F]FDG PET/CT. Thus, for increasing scan volumes and streamline workflows, acquisition at early timepoint could be a feasible protocol of [18F]FAPI-42 PET/CT.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Boellaard R, Delgado-Bolton R, Oyen WJ et al (2015) FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2.0. Eur J Nucl Med Mol Imaging 42:328–354
Ferdinandus J, Kessler L, Hirmas N et al (2021) Equivalent tumor detection for early and late FAPI-46 PET acquisition. Eur J Nucl Med Mol Imaging 48:3221–3227
Giesel FL, Kratochwil C, Lindner T et al (2019) 68Ga-FAPI PET/CT: biodistribution and preliminary dosimetry estimate of 2 DOTA-containing FAP-targeting agents in patients with various cancers. J Nucl Med 60:386–392
Glatting FM, Hoppner J, Liew DP et al (2022) Repetitive early 68Ga-FAPI PET acquisition comparing 68Ga-FAPI-02, 68Ga-FAPI-46, and 68Ga-FAPI-74: methodologic and diagnostic implications for malignant, inflammatory/reactive, and degenerative lesions. J Nucl Med 63:1844–1851
Hirmas N, Hamacher R, Sraieb M et al (2023) Fibroblast-activation protein PET and histopathology in a single-center database of 324 patients and 21 tumor entities. J Nucl Med 64:711–716
Hu K, Wang L, Wu H et al (2022) [18F]FAPI-42 PET imaging in cancer patients: optimal acquisition time, biodistribution, and comparison with [68Ga]Ga-FAPI-04. Eur J Nucl Med Mol Imaging 49:2833–2843
Huang J, Fu L, Zhang X et al (2023) Noninvasive imaging of FAP expression using positron emission tomography: a comparative evaluation of a [18F]-labeled glycopeptide-containing FAPI with [18F]FAPI-42. Eur J Nucl Med Mol Imaging. https://doi.org/10.1007/s00259-023-06282-5
Koerber SA, Röhrich M, Walkenbach L et al (2023) Impact of 68Ga-FAPI PET/CT on staging and oncologic management in a cohort of 226 patients with various cancers. J Nucl Med 64(11):1712–1720
Kratochwil C, Flechsig P, Lindner T et al (2019) 68Ga-FAPI PET/CT: tracer uptake in 28 different kinds of cancer. J Nucl Med 60:801–805
Liu G, Mao W, Yu H, Hu Y, Gu J, Shi H (2023) One-stop [18F]FDG and [68Ga]Ga-DOTA-FAPI-04 total-body PET/CT examination with dual-low activity: a feasibility study. Eur J Nucl Med Mol Imaging 50(8):2271–2281
Loktev A, Lindner T, Mier W et al (2018) A tumor-imaging method targeting cancer-associated fibroblasts. J Nucl Med 59:1423–1429
Lyu Z, Han W, Zhang Q et al (2023) Clinical application of Al18F-NOTA-FAPI PET/CT in diagnosis and TNM staging of pancreatic adenocarcinoma, compared to 2-[18F]FDG. Cancer Imaging 23:86
Mori Y, Haberkorn U, Giesel FL (2023) 68Ga- or 18F-FAPI PET/CT—what it can and cannot. Eur Radiol. https://doi.org/10.1007/s00330-023-09715-9
Mu X, Huang X, Jiang Z et al (2023) [18F]FAPI-42 PET/CT in differentiated thyroid cancer: diagnostic performance, uptake values, and comparison with 2-[18F]FDG PET/CT. Eur J Nucl Med Mol Imaging 50:1205–1215
Naeimi M, Choyke PL, Dendl K et al (2023) Three-time-point PET analysis of 68Ga-FAPI-46 in a variety of cancers. J Nucl Med 64:618–622
Qiao KL, Qin XT, Fu S et al (2023) Value of [18F]AlF-NOTA-FAPI-04 PET/CT for differential diagnosis of malignant and various inflammatory lung lesions: comparison with [18F]FDG PET/CT. Eur Radiol. https://doi.org/10.1007/s00330-023-10208-y
Qin C, Shao F, Gai Y et al (2022) 68Ga-DOTA-FAPI-04 PET/MR in the evaluation of gastric carcinomas: comparison with 2-[18F]FDG PET/CT. J Nucl Med 63:81–88
Wang S, Zhou X, Xu X et al (2021) Clinical translational evaluation of Al(18)F-NOTA-FAPI for fibroblast activation protein-targeted tumour imaging. Eur J Nucl Med Mol Imaging 48:4259–4271
Wass G, Clifford K, Subramaniam RM (2023) Evaluation of the diagnostic accuracy of FAPI PET/CT in oncologic studies: systematic review and metaanalysis. J Nucl Med 64:1218–1224
Watabe T, Naka S, Tatsumi M et al (2023) Initial evaluation of [18F]FAPI-74 PET for various histopathologically confirmed cancers and Benign Lesions. J Nucl Med 64:1225–1231
Wu C, Zhang X, Zeng Y et al (2022) [18F]FAPI-42 PET/CT versus [18F]FDG PET/CT for imaging of recurrent or metastatic gastrointestinal stromal tumors. Eur J Nucl Med Mol Imaging 50:194–204
Yang L, Xu S, Cheng L et al (2023) [18F]AlF-NOTA-FAPI-04 PET/CT as a promising tool for imaging fibroblast activation protein in gastrointestinal system cancers: a prospective investigation of comparative analysis with 2-[18F]FDG. Eur J Nucl Med Mol Imaging 50(13):4051–4063
Yao Y, Tan X, Yin W et al (2022) Performance of 18F-FAPI PET/CT in assessing glioblastoma before radiotherapy: a pilot study. BMC Med Imaging 22:226
Zhang J, He Q, Jiang S et al (2023) [18F]FAPI PET/CT in the evaluation of focal liver lesions with [18F]FDG non-avidity. Eur J Nucl Med Mol Imaging 50:937–950
Acknowledgements
We gratefully acknowledge the contributions of the cancer patients who participated in this study.
Funding
This work was financially supported by Guangxi Health and Family Commission (Grant No. Z-C20220815).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Xingyu Mu, Biyun Mo, Jie Qin and Zuguo Li. The first draft of the manuscript was written by Xingyu Mu and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical lates of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical lates. This study was approved by the Ethics Committee of our hospital (Approval No. 2022WJWZCLL-01).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publication
The authors affirm that human research participants provided informed consent for publication of the images in Figure(s) 2, 3 and 7.
Competing interests
No potential conflict of interest relevant to this article exist.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1. Table S1.
The biodistribution of 18F-FAPI-42 between early and standard scanTABLE 1. The biodistribution of 18F-FAPI-42 between early and standard scan. Fig. S1. Comparison of uptake on 18F-FAPI-42 PET between early and standard 18F-FAPI-42 PET.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mu, X., Mo, B., Qin, J. et al. Comparative analysis of two timepoints on [18F]FAPI-42 PET/CT in various cancers. European J Hybrid Imaging 7, 27 (2023). https://doi.org/10.1186/s41824-023-00186-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41824-023-00186-1