
Abstract
Background
Fatigue is a highly prevalent and disabling symptom in cancer survivors. Although many measures have been developed to assess survivors’ fatigue, their ability to accurately capture change following intervention has rarely been assessed in post-treatment survivors. Ultra-brief fatigue measures are preferable in clinical practice but have limited evidence supporting their use with cancer survivors. We examined the psychometric properties of four Fatigue Symptom Inventory (FSI) measures, including the new FSI-3, in cancer survivors. Examined properties included responsiveness to change and minimally important differences (MIDs).
Methods
We analyzed data from three randomized controlled trials with post-treatment cancer survivors (N = 328). Responsiveness to change was evaluated by comparing standardized response means for survivors who reported their fatigue as being better, the same, or worse at 2–3 months. Responsiveness to intervention was assessed via effect sizes, and MIDs were estimated by using several methods. We also computed area under the curve (AUC) values to assess FSI measures’ discriminative accuracy compared to an established cut-point.
Results
All FSI measures differentiated survivors who reported improvement at 2–3 months from those with stable fatigue, but did not uniformly differentiate worsening fatigue from stable fatigue. Measures showed similar levels of responsiveness to intervention, and MIDs ranged from 0.29 to 2.20 across FSI measures. AUC analyses supported the measures’ ability to detect significant fatigue.
Conclusions
Four FSI scales show similar responsiveness to change, and estimated MIDs can inform assessment of meaningful change in fatigue. The FSI-3 shows promise as an ultra-brief fatigue measure for survivors.
Plain English Summary
Fatigue is a highly prevalent and disabling symptom in cancer survivors. Although many measures have been developed to assess survivors’ fatigue, their ability to accurately capture change following intervention has rarely been assessed in post-treatment survivors. A minimally important difference in fatigue, or clinically meaningful change, also has rarely been documented for fatigue scales in studies of post-treatment survivors. Ultra-brief fatigue measures are preferable in clinical practice, but have limited evidence supporting their use with cancer survivors. This study aimed to address these gaps in the literature through analyses of Fatigue Symptom Inventory (FSI) data from three randomized behavioral intervention trials with post-treatment cancer survivors (N = 328). Four FSI measures (i.e., FSI total score, FSI severity and interference subscales, and the FSI-3) showed comparable ability to detect change in fatigue and responsiveness to intervention with cancer survivors. Estimated minimally important differences ranged from 0.29 to 2.20 across FSI measures and warrant further study to inform assessment of meaningful score change in research and clinical practice. Results support continued use of the FSI with cancer survivors and provide initial evidence for use of the ultra-brief FSI-3 measure.
Similar content being viewed by others
Background
Fatigue is a highly prevalent, persistent, debilitating problem in cancer survivors [1]. Up to 40% of solid-tumor (e.g., breast, colorectal cancer) survivors experience moderate-to-severe fatigue in the first year after treatment [2, 3], and one third report this level of fatigue at 5 years post-diagnosis [3,4,5]. Fatigue often co-occurs with other disabling symptoms, such as pain, mood, and sleep problems [5,6,7,8,9,10,11,12,13], and has a substantial negative impact on activities [14,15,16]. Thus, reducing fatigue severity and interference with functioning is critical for improving survivors’ quality of life [12, 14, 16,17,18].
Many self-report measures have been developed to assess fatigue. The selection of a measure is guided by several considerations [19, 20]. These include the aspects of fatigue that one wishes to measure (e.g., severity, interference, time interval), respondent burden, the measure's clinical or research utility, and psychometric properties in the target population. The Fatigue Symptom Inventory (FSI) [21] is a 13-item self-report measure that assesses fatigue severity, fatigue frequency, and the interference of fatigue with activities, mood, and cognition. This measure has been extensively used with cancer survivors with strong evidence of construct validity and reliability [22]. In a review of fatigue measures for cancer populations, the FSI received the highest psychometric quality rating relative to other fatigue measures [23].
Multidimensional assessments of fatigue are recommended for clinical trials and other types of research [23]. In clinical settings, however, a brief measure may be preferable. Although 1-item fatigue measures have shown promise in cancer populations, they solely focus on fatigue severity and have inadequate evidence of validity or issues with responsiveness [20, 24]. A few measures of fatigue with 3 or 4 items have also been tested in cancer studies [25,26,27,28]. To date, these measures have been limited by their emphasis on one aspect of fatigue (e.g., physical sensations) [25] or lack of evidence of predictive validity and reliability [19, 26, 28]. Despite literature reviews on fatigue measurement [19, 20], there is no consensus regarding an optimal tool for briefly assessing fatigue in cancer populations. However, the International Society of Quality of Life Research has developed minimal standards for patient-centered outcomes, such as evidence of reliability, validity, responsiveness, and score interpretability [29].
An important psychometric property of fatigue measures is their responsiveness to change. Responsiveness includes the measures’ ability to accurately capture change following an intervention of known efficacy as well as change that is not the result of an intervention. In oncology research, clinical change in fatigue has primarily been evaluated in patients with advanced disease or those undergoing cancer treatment [30, 31]. In a review of FSI studies, effect sizes for responsiveness to change ranged from small to large in behavioral and disease treatment trials with cancer patients [22]. Standardized response means (SRMs), statistics that might better characterize the ability of the FSI to change over time, were unable to be computed. Another study found evidence of the FSI’s responsiveness to change by calculating effect sizes and SRMs for a trial targeting pain and depression during cancer treatment [32]. Further research is needed to document responsiveness to change for the FSI and other fatigue measures, especially in post-treatment survivors [19]. On average, fatigue tends to increase during cancer treatment and remit within 1 year following treatment [1, 33]. However, these averages mask substantial individual differences in survivors’ fatigue trajectories that warrant further assessment with responsive measures [1, 4].
Information on a minimally important difference (MID) in fatigue scores is another important psychometric property. An MID is the smallest difference in fatigue scores that the patient perceives as having positive or negative impact [34]. Perceived negative impact may lead the patient or clinician to consider a change in the patient’s fatigue management. Whereas an MID refers to change in fatigue that is meaningful to the patient irrespective of the context, a minimal clinically important difference (MCID) refers to change in patient-reported fatigue that leads to a change in clinical care [34]. MIDs for fatigue measures have substantially varied in studies of patients with advanced disease or those undergoing cancer treatment [35,36,37,38] and have yet to be evaluated among post-treatment survivors. As survivors recover from treatments, their MIDs may differ from those experiencing acute treatment side effects. MIDs for the FSI and its subscales have yet to be established.
Because different methods may produce somewhat different MID estimates, some experts recommend triangulating several approaches when estimating MIDs for a patient-reported outcome (PRO) [39, 40]. Distribution-based metrics include 0.2 to 0.5 standard deviations (SDs) or 1 to 2 standard errors of measurement (SEMs) [40,41,42,43,44,45]. However, these metrics are inferior to anchor-based methods and are instead best used as “supportive information for MID estimates from different anchor-based approaches and systematic reviews of the clinical trial literature” (p. 106) [39]. Common anchors include patient-rated global impression of change and comparison with absolute change on a legacy measure of the same domain. Whereas anchor-based methods have certain advantages [46], some PRO domains such as fatigue, pain, and some psychological symptoms may lack a criterion standard anchor. Moreover, the magnitude of an MID may vary depending upon whether one is measuring a difference or change at the level of an individual person vs. using aggregated individual-level data to compare differences between groups in research or clinical populations [47, 48]. To be considered meaningful, change within an individual may need to be larger than differences that are detected between groups [49].
This study aimed to determine the psychometric properties of four FSI measures in post-treatment cancer survivors enrolled in behavioral intervention trials. The measures were the FSI total score, FSI severity and interference subscales, and a new 3-item FSI (FSI-3). Examined psychometric properties included responsiveness to change (calculated via SRMs), responsiveness to intervention, and MID estimates. Additionally, area under the receiver operating curve (ROC) values were computed to estimate each FSI measure’s discriminative accuracy relative to an established cut-point, and a preliminary cut-point for the FSI-3 was determined based on these values. Cut-points are used in research and clinical practice to indicate need for further assessment or intervention.
Methods
Study samples
We analyzed data from three randomized controlled trials (RCTs) with post-primary treatment cancer survivors (N = 328) conducted between 2011 and 2015. Detailed methodology and results of these studies are published elsewhere [50,51,52,53]. These RCTs were approved by their respective institutional review boards (IRB approval numbers: Indiana University 1003-02B, 01206008951, Southern Illinois University School of Medicine 08–022, University of Alabama at Birmingham F121114008, University of Illinois Urbana-Champaign 09707), and all participants provided informed consent.
Briefly, sample 1 consisted of 35 cancer survivors participating in a pilot RCT comparing a 7-week Mindfulness-based Stress Reduction (MBSR) course for fatigue to a waitlist control condition (NCT01247532) [50]. Sample 2 consisted of 71 cancer survivors participating in a pilot RCT comparing the effects of an 8-week MBSR course vs. a psychoeducation/support group on fatigue (NCT01919853) [51]. For both trials, survivors were considered eligible if they were ≥ 18 years old with a non-metastatic cancer diagnosis; had not received cancer treatment in the past 3 months (other than endocrine therapy); reported persistent fatigue (≥ 2 months); and had clinically significant fatigue scores (FSI severity ≥ 4) at eligibility screening [50, 51]. Participants in both trials completed self-report questionnaires at baseline and approximately 2 months post-baseline. Given the similarities between samples 1 and 2, these data were combined for most analyses. Sample 3 consisted of 222 breast cancer survivors participating in an RCT comparing a 3-month physical activity behavior change intervention to usual care, with fatigue as a secondary outcome (NCT00929617) [52, 53]. For this trial, survivors were eligible if they were women between 18 and 70 years of age with a history of non-metastatic breast cancer; not currently receiving chemotherapy or radiation therapy; ≥ 2 months post-surgery; and participating in ≤ 30 min of vigorous or ≤ 60 min of moderate activity each week in the past 6 months [52, 53]. Our analyses focused on baseline and 3 months post-baseline assessments.
Measures
The measures described below were administered in all three trials.
Fatigue Symptom Inventory (FSI)
The FSI is a 13-item fatigue self-report measure with evidence of reliability and validity in cancer populations [21, 54]. The FSI includes three subscales: severity, interference, and frequency of fatigue during the past week. FSI Severity is measured with four items using an 11-point scale (0 = Not at all fatigued to 10 = As fatigued as I could be). FSI Interference is measured with seven items using an 11-point scale (0 = No interference to 10 = Extreme interference). FSI frequency is measured with two items assessing the number of days (range = 0 to 7) and the extent of the day on average the respondents felt fatigued over the past week (0 = None of the day to 10 = The entire day). For each scale, the total score is the average of all items, with a higher score indicating worse fatigue.
We derived a 3-item fatigue measure (the FSI-3) that includes 1 severity item (average severity) and 2 interference items (interference with general activity and enjoyment of life) from the FSI. The FSI-3 uses the same scales and scoring (mean of the items) as the FSI. The FSI-3 was adapted from the 3-item PEG which is an ultra-brief version of the Brief Pain Inventory (BPI) [55]. The FSI and BPI items are identical except that fatigue is substituted for pain. The same severity and interference items have also recently been validated in the 3-item DEG scale for assessing dyspnea [56].
Short form-36 health survey vitality subscale (SF-36 vitality)
The SF-36 Vitality subscale (version 2) is a 4-item self-report measure assessing energy level during the past 4 weeks [57]. It is commonly used as a brief measure to assess fatigue in a variety of populations [58]. Scores are transformed into a scale ranging from 0 to 100, with higher scores indicating greater vitality. In prior research, survivors with scores less than 50 on the SF-36 Vitality measure showed biological and psychological/behavioral indicators of elevated fatigue compared to survivors with scores ≥ 50, supporting this cut-point’s validity [4, 33, 59,60,61,62]. Consistent with prior research [63], a more stringent cutoff (score ≤ 45) was used to indicate clinically meaningful fatigue. Given the measure’s established responsiveness to change [32, 64], it was used as an anchor when calculating responsiveness to change for fatigue measures in the current study.
Data analysis
For most analyses, data from MBSR trials were combined and analyzed together, and data from the BEAT Cancer trial were analyzed separately. Analyses were performed using SPSS, version 25.0, R v.4.0.3 [65], and MedCalc statistical software [66]. Baseline and first follow-up data were used in the analyses (i.e., 2 months post-baseline in the MBSR trials and 3 months post-baseline in the BEAT Cancer trial). We calculated descriptive psychometrics (means, SDs, Cronbach’s αs), interscale correlations at baseline, and interscale correlations for change scores. Standard errors of measurement (SEMs) were computed by multiplying SDs by the square root of (1-Cronbach’s α). The coefficient of repeatability was calculated as 1.96 times SEM times the square root of 2 [47].
Responsiveness to change was examined by calculating SRMs for each fatigue measure (i.e., FSI severity, FSI interference, FSI-3, and FSI Total). SRMs are effect sizes calculated as the difference between mean scores within groups from baseline to post-intervention divided by the SD of the change score. SRMs of 0.2, 0.5, and 0.8 represent small, moderate, and large change, respectively [67]. We stratified SRMs by the following changes in SF-36 Vitality from baseline to follow-up: (1) Worse (i.e., fatigue increased by ≥ 1 SEM), (2) Same (i.e., fatigue remained about the same, change was < 1 SEM), and (3) Better (i.e., fatigue decreased by ≥ 1 SEM). We stratified the samples into worse-same-better groups using a legacy measure anchor, consistent with prior research [68, 69]. For each fatigue measure, pairwise t-tests were conducted comparing change scores in the Worse and Better categories with the change score in the Same category. The 95% CIs for each SRM were calculated via bias-corrected bootstrapping with 10,000 samples. Empirical cumulative distribution function plots were created to visually examine the distribution of change in fatigue scores by group (i.e., Worse, Same, Better).
Each measure’s responsiveness to intervention effects was examined by computing between-group treatment effect differences evaluated in two ways: (1) effect sizes, calculated as the difference between change score means of two independent groups divided by the pooled SD of baseline scores [70]; and (2) SRM, calculated as the difference between change score means of two independent groups divided by the SD of the pooled change score [71]. Given that MBSR trials included different control groups [50, 51], these between-group effect sizes were calculated for each trial separately. Effect sizes of 0.2, 0.5, and 0.8 represent small, moderate, and large change, respectively [72].
Four additional metrics were calculated for each FSI measure [43, 45]. First, we calculated 0.2 SD, 0.35 SD, and 0.5 SD for baseline FSI scores [73]. Second, we computed 1 SEM and 2 SEM for baseline FSI scores as lower and upper bounds of an MID. Third, we computed the difference in FSI score change from baseline to follow-up between the Better and Same SF-36 Vitality categories as a potential MID estimate. Fourth, we computed the coefficient of repeatability by multiplying 1.96 with the square root of 2 times SEM [47]. This metric is an estimate of the significance of individual change and is the minimal amount of change needed to be significant at p < 0.05 based on the reliable change index.
Area under the ROC curve (AUC) values were computed to estimate each FSI measure’s discriminative accuracy relative to the established cut-point for the SF-Vitality scale (≤ 45) at baseline. AUC values represent the probability of a measure correctly discriminating between survivors who had clinically significant fatigue and those who did not. An AUC value of 0.5 represents no ability to discriminate and 1.0 represents perfect discrimination.
To establish a preliminary cut-point for the FSI-3, AUC values and operating characteristics such as sensitivity (true positive rate), specificity (true negative rate), and Youden’s index (sensitivity + specificity − 1) were examined. The ROC curve graphically represents the trade-off between sensitivity and specificity for the range of possible scores on the FSI-3 scale compared to the SF-Vitality criterion (≤ 45) at baseline. Given that the MBSR trials required elevated fatigue for eligibility, we only used the BEAT Cancer trial data to explore potential cut-points for the FSI-3.
Results
Patient characteristics
Additional file 2: Table 1 shows participants’ baseline characteristics. In the MBSR trials [50, 51], participants’ mean age was 57 years, and most were female (86%), non-Hispanic White (71%), and diagnosed with breast cancer (82%). In the BEAT Cancer trial [53], all participants were female breast cancer survivors, with an average age of 54 years. The majority were non-Hispanic White (82%).
Descriptive psychometrics and interscale correlations
At baseline, all scale scores demonstrated good internal consistency reliability (αs = 0.74 to 0.95; Table 1). Within MBSR and BEAT Cancer trials, all FSI scales were strongly correlated at baseline. As expected, the SF-36 Vitality scale (for which a lower score represents worse fatigue) was negatively correlated with all FSI scales. A correlation ≥ 0.3 is one criterion that can used to support the use of an anchor [39, 40], a threshold clearly met by the SF-36 Vitality scale for which baseline correlations with the FSI scales ranged from − 0.44 to − 0.79 (correlations are negative because worse fatigue is represented by higher scores on the FSI scales vs. lower scores on the SF-36 Vitality scale). Additionally, change in FSI scores from baseline to follow-up showed moderate correlations with change in SF-36 Vitality scores (Additional file 3: Table 2).
Responsiveness to change: standardized response means (SRMs)
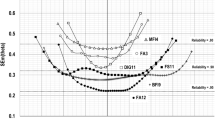
Table 2 shows the change in FSI scores between baseline and follow-up (i.e., 2 months post-baseline in the MBSR trials and 3 months post-baseline in the BEAT Cancer trial) for each group (i.e., Worse, Same, or Better SF-36 Vitality scores). The p values denote the statistical significance of the change between the reference (i.e., Same) and other (i.e., Worse, Better) groups. Within trials, SRMs for fatigue measures yielded generally comparable results for each group. For the BEAT Cancer trial, all FSI measures significantly differentiated the Worse and Better groups from the Same group (SRMs: 0.69 to 0.95 and − 0.78 to − 0.96, respectively). For the MBSR trials, all FSI measures significantly differentiated the Better group from the Same group (SRMs: − 0.88 to − 1.13). However, the measures did not significantly discriminate the Worse group from the Same group. Whereas all point estimates were negative (SRMs: − 0.24 to − 0.47), the confidence intervals included zero. Empirical cumulative distribution function plots showed that differentiation between groups (i.e., Better, Same, Worse) was better in the BEAT Cancer trial compared to the MBSR trials (Additional file 1: Figs. 1 and 2). Differentiation of the four versions of the FSI scales was similar within each trial.
Responsiveness to intervention: between-group effect sizes
Table 3 shows the change in each measure by study condition for all trials and corresponding between-group effect sizes and SRMs. Of note, there were only modest differences between effect sizes and SRMs. Within each trial, all FSI scales showed similar levels of responsiveness to intervention. Across FSI and SF-36 Vitality measures, between-group effect sizes and SRMs were large for MBSR trial 1 and small to moderate for MBSR trial 2 and the BEAT Cancer trial.
Additional psychometric values
Table 4 provides four psychometric values for the FSI scales in the MBSR and BEAT Cancer trials. The MID estimate using the global change anchor ranged from 0.90 to 1.69 on the 0 to 10 point FSI scales. The coefficient of repeatability ranged from 1.10 to 2.20. The two distribution-based metrics were somewhat lower, with 0.5 SD ranging from 0.73 to 1.10 and 2 SEM ranging from 0.79 to 1.59.
Area under the ROC (AUC)
Within trials, all FSI measures yielded similar AUC values for differentiating significant fatigue at baseline using an SF-36 Vitality score ≤ 45 as the criterion (Table 5). Most AUC values had acceptable to excellent discriminatory ability (range: 0.64–0.88, with 7 of 8 values being 0.74 or higher).
For the FSI-3, visual inspection of the ROC curves and examination of operating characteristics across a range of scores suggested that a mean score ≥ 5 could be considered a preliminary cut-point. This cut-point optimizes the Youden index and takes into account the elbow of the ROC curve. It yielded a sensitivity of 0.77 and a specificity of 0.87 relative to the SF-36 Vitality score criterion (≤ 45). When examining the likelihood ratios (LRs) for FSI-3 score intervals, the 5–6 interval was the first interval with a LR > 1, suggesting that survivors with scores < 5 would be less likely to have clinically significant fatigue.
Discussion
Across several trials with cancer survivors, four FSI measures, including the new FSI-3, showed evidence of internal consistency reliability (αs = 0.81 to 0.93) and convergent validity based on correlations with the SF-36 Vitality measure and among FSI measures. Furthermore, across trials, all FSI measures performed well in distinguishing improvement in fatigue from lack of change. However, the measures showed mixed ability across trials to distinguish worsening fatigue from lack of change. Additionally, responsiveness to behavioral interventions was similar across FSI measures, as were preliminary MID estimates. Finally, AUC analyses based on an established anchor supported the FSI measures’ ability to detect clinically significant fatigue.
SRMs were of large magnitude in survivors who improved over 2 or 3 months and differed significantly from SRMs in survivors with stable fatigue. SRMs were variable in survivors with worsening fatigue, and only differed significantly from SRMs in BEAT Cancer trial participants with stable fatigue. The small number of survivors with worsening fatigue in the MBSR trials (n = 11) may have contributed to the null findings. Another potential explanation is that the MBSR trials only enrolled survivors with significant fatigue at screening [50, 51]. Regression to the mean is more likely when initial fatigue scores are high. Finally, scales for other symptoms have also proven better at detecting improvement than worsening [42, 74, 75].
The FSI scales and SF-36 Vitality measure showed small to moderate change in response to a physical activity intervention with a usual care control and an MBSR intervention with an attention control. Conversely, these measures showed large change in the trial of MBSR versus a waitlist control. These effect sizes are typical for the literature on behavioral interventions for fatigue in cancer survivors [76, 77].
Our preliminary MID estimate using the global change anchor ranged from 0.90 to 1.69 on the 0 to 10 point FSI scales. Several limitations of this estimate should be noted. Rather than a comparison to a patient-reported global impression of change anchor (PGIC), our anchor defined change as ≥ 1 SEM change on the SF-36 vitality scale. This approach is used less commonly than the PGIC and, more importantly, did not allow for more granular assessments of change (e.g., small, moderate, large) captured by many PGIC scales. However, these are approximations and require further research in other samples and using additional MID approaches such as PGIC and other anchors [47, 48]. In the chronic illness literature, the magnitude of MIDs for fatigue measures has varied considerably based on the estimation method, patient population, and context [37].
Across FSI measures, AUC values ranged from 0.64 to 0.88, which represent moderate to strong differentiation between survivors with and without significant fatigue. Regarding the FSI-3, a preliminary cut-point ≥ 5 yielded optimal sensitivity and specificity relative to the widely used SF-36 Vitality subscale. Prior research has also supported a cut-point of 5 on a 0–10 scale for fatigue [78]. The FSI-3 addresses the need for a validated fatigue measure that briefly assesses both fatigue severity and interference in cancer populations. Across studies, the FSI-3 showed comparable psychometrics relative to lengthier FSI measures.
Limitations of the present analyses warrant mention. The samples primarily consisted of non-Hispanic White women who had completed primary treatment for early-stage breast cancer. Additionally, the FSI was originally developed in a sample that did not represent the racial and ethnic diversity of cancer survivors [21]. Generalizability of the findings to diverse cancer populations requires further research. Furthermore, the sample sizes for the MBSR trials were relatively small, which limited statistical power for detecting effects and analyzing specific racial or ethnic groups. The SF-36 Vitality subscale was the only anchor used in analyses of responsiveness to change and AUC values and has a slightly different time frame than the FSI (past 4 weeks vs. 1 week). There is no criterion standard for testing the responsiveness of fatigue measures. Although the SF-36 Vitality subscale is one of the most established measures with evidence of responsiveness to change [32], it also relies on patient self-report. Other indices of improvement (e.g., activity engagement) would strengthen our findings. In addition, although a 3-category approach (i.e., Worse, Same, or Better SF-36 Vitality scores) has commonly been used to determine MIDs and converges with distribution-based methods [68, 69], it may result in overestimation of MIDs. Finally, the psychometric properties of the FSI-3, including a cut-point and its sensitivity to change, warrant replication. Test–retest reliability should also be assessed.
Conclusions
In summary, examined FSI measures had comparable responsiveness to change and preliminary estimates of MID in cancer survivors. Our results strongly support continued use of the FSI with survivors and provide initial evidence for use of the FSI-3. As fatigue is a top concern of survivors [79], its rigorous assessment is an important first step in optimizing quality of life. Examining the generalizability of our findings to non-cancer populations is also important given the substantial prevalence of fatigue across many medical and psychological conditions as well as the potential benefits of measurement-based care for optimal fatigue management.
Availability of data and materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Abbreviations
- AUC:
-
Area under the curve
- BPI:
-
Brief pain inventory
- FSI:
-
Fatigue Symptom Inventory
- LR:
-
Likelihood ratio
- MBSR:
-
Mindfulness-based stress reduction
- MID:
-
Minimally important difference
- RCT:
-
Randomized controlled trial
- ROC:
-
Receiver operating curve
- SEM:
-
Standard error of measurement
- SF-36:
-
Short-form 36
- SRM:
-
Standardized response mean
References
Bower JE (2014) Cancer-related fatigue—mechanisms, risk factors, and treatments. Nat Rev Clin Oncol 11(10):597–609. https://doi.org/10.1038/nrclinonc.2014.127
Abrahams HJG, Gielissen MFM, Schmits IC, Verhagen CAHHVM, Rovers MM, Knoop H (2016) Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: a meta-analysis involving 12 327 breast cancer survivors. Ann Oncol 27(6):965–974. https://doi.org/10.1093/annonc/mdw099
Jones JM, Howell D, Olson KL, Jiang H, Catton CN, Catton P et al (2012) Prevalence of cancer-related fatigue in a population-based sample of colorectal, breast, and prostate cancer survivors. J Clin Oncol 30(Suppl. 15):9131. https://doi.org/10.1200/jco.2012.30.15_suppl.9131
Bower JE, Ganz PA, Desmond KA, Bernaards C, Rowland JH, Meyerowitz BE et al (2006) Fatigue in long-term breast carcinoma survivors. Cancer 106(4):751–758. https://doi.org/10.1002/cncr.21671
Thong MS, Mols F, Wang XS, Lemmens VE, Smilde TJ, van de Poll-Franse LV (2013) Quantifying fatigue in (long-term) colorectal cancer survivors: a study from the population-based patient reported outcomes following initial treatment and long term evaluation of survivorship registry. Eur J Cancer 49(8):1957–1966
Hung R, Krebs P, Coups EJ, Feinstein MB, Park BJ, Burkhalter J et al (2011) Fatigue and functional impairment in early-stage non-small cell lung cancer survivors. J Pain Symptom Manage 41(2):426–435. https://doi.org/10.1016/j.jpainsymman.2010.05.017
Hwang IC, Yun YH, Kim Y-W, Ryu KW, Kim YA, Kim S et al (2014) Factors related to clinically relevant fatigue in disease-free stomach cancer survivors and expectation–outcome consistency. Support Care Cancer 22(6):1453–1460. https://doi.org/10.1007/s00520-013-2110-2
Kim SH, Son BH, Hwang SY, Han W, Yang J-H, Lee S et al (2008) Fatigue and depression in disease-free breast cancer survivors: Prevalence, correlates, and association with quality of life. J Pain Symptom Manage 35(6):644–655. https://doi.org/10.1016/j.jpainsymman.2007.08.012
Kuhnt S, Ernst J, Singer S, Rüffer JU, Kortmann RD, Stolzenburg J et al (2009) Fatigue in cancer survivors – prevalence and correlates. Oncol Res Treat 32(6):312–317. https://doi.org/10.1159/000215943
Storey DJ, McLaren DB, Atkinson MA, Butcher I, Liggatt S, O’Dea R et al (2011) Clinically relevant fatigue in recurrence-free prostate cancer survivors. Ann Oncol 23(1):65–72. https://doi.org/10.1093/annonc/mdr034
Wang XS, Zhao F, Fisch MJ, O’Mara AM, Cella D, Mendoza TR et al (2014) Prevalence and characteristics of moderate to severe fatigue: a multicenter study in cancer patients and survivors. Cancer 120(3):425–432. https://doi.org/10.1002/cncr.28434
Meeske K, Smith AW, Alfano CM, McGregor BA, McTiernan A, Baumgartner KB et al (2007) Fatigue in breast cancer survivors two to five years post diagnosis: a HEAL Study report. Qual Life Res 16(6):947–960. https://doi.org/10.1007/s11136-007-9215-3
Levkovich I, Cohen M, Alon S, Kuchuk I, Nissenbaum B, Evron E et al (2018) Symptom cluster of emotional distress, fatigue and cognitive difficulties among young and older breast cancer survivors: The mediating role of subjective stress. J Geriatr Oncol 9(5):469–475. https://doi.org/10.1016/j.jgo.2018.05.002
Ekenga CC, Pérez M, Margenthaler JA, Jeffe DB (2018) Early-stage breast cancer and employment participation after 2 years of follow-up: A comparison with age-matched controls. Cancer 124(9):2026–2035. https://doi.org/10.1002/cncr.31270
Lee MK, Kang HS, Lee KS, Lee ES (2017) Three-year prospective cohort study of factors associated with return to work after breast cancer diagnosis. J Occup Rehabil 27(4):547–558. https://doi.org/10.1007/s10926-016-9685-7
Jones JM, Olson K, Catton P, Catton CN, Fleshner NE, Krzyzanowska MK et al (2016) Cancer-related fatigue and associated disability in post-treatment cancer survivors. J Cancer Surviv 10(1):51–61. https://doi.org/10.1007/s11764-015-0450-2
Jung JY, Lee JM, Kim MS, Shim YM, Zo JI, Yun YH (2018) Comparison of fatigue, depression, and anxiety as factors affecting posttreatment health-related quality of life in lung cancer survivors. Psychooncology 27(2):465–470. https://doi.org/10.1002/pon.4513
Schmidt ME, Chang-Claude J, Vrieling A, Heinz J, Flesch-Janys D, Steindorf K (2012) Fatigue and quality of life in breast cancer survivors: temporal courses and long-term pattern. J Cancer Surviv 6(1):11–19. https://doi.org/10.1007/s11764-011-0197-3
Al Maqbali M, Hughes C, Gracey J, Rankin J, Dunwoody L, Hacker E (2019) Quality assessment criteria: psychometric properties of measurement tools for cancer related fatigue. Acta Oncol 58(9):1286–1297. https://doi.org/10.1080/0284186X.2019.1622773
Fisher MI, Davies C, Lacy H, Doherty D (2018) Oncology section EDGE task force on cancer: measures of cancer-related fatigue—a systematic review. Rehabil Oncol 36(2):93–105. https://doi.org/10.1097/01.Reo.0000000000000124
Hann DM, Jacobsen PB, Azzarello LM, Martin SC, Curran SL, Fields KK et al (1998) Measurement of fatigue in cancer patients: development and validation of the Fatigue Symptom Inventory. Qual Life Res 7(4):301–310. https://doi.org/10.1023/a:1024929829627
Donovan KA, Jacobsen PB (2011) The Fatigue Symptom Inventory: a systematic review of its psychometric properties. Support Care Cancer 19(2):169–185. https://doi.org/10.1007/s00520-010-0989-4
Agasi-Idenburg C, Velthuis M, Wittink H (2010) Quality criteria and user-friendliness in self-reported questionnaires on cancer-related fatigue: a review. J Clin Epidemiol 63(7):705–711. https://doi.org/10.1016/j.jclinepi.2009.08.027
Barsevick AM, Cleeland CS, Manning DC, O’Mara AM, Reeve BB, Scott JA et al (2010) ASCPRO recommendations for the assessment of fatigue as an outcome in clinical trials. J Pain Symptom Manage 39(6):1086–1099. https://doi.org/10.1016/j.jpainsymman.2010.02.006
Fuhrmann K, Mehnert A, Geue K, Hinz A (2015) Fatigue in breast cancer patients: psychometric evaluation of the fatigue questionnaire EORTC QLQ-FA13. Breast Cancer 22(6):608–614. https://doi.org/10.1007/s12282-014-0527-1
Davis MP, Khoshknabi D, Walsh D, Lagman R, Karafa MT, Aktas A et al (2013) Four-item fatigue screen: replacing the brief fatigue index. Am J Hosp Palliat Med 30(7):652–656. https://doi.org/10.1177/1049909112460567
Lewson AB, Johns SA, Krueger E, Chinh K, Kidwell KM, Mosher CE (2021) Symptom experiences in post-treatment cancer survivors: associations with acceptance and commitment therapy constructs. Support Care Cancer 29(7):3487–3495
Davis M, Sevidova Khoshknabi D, Walsh D, Lagman R, Karafa M, Hauser K (2012) Validation of a four item fatigue screen (FIFS) in cancer-related fatigue (CRF). J Pain Symptom Manage 43(2):P423–P424
Reeve BB, Wyrwich KW, Wu AW, Velikova G, Terwee CB, Snyder CF et al (2013) ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual Life Res 22(8):1889–1905. https://doi.org/10.1007/s11136-012-0344-y
Cella D, Lai J-S, Jensen SE, Christodoulou C, Junghaenel DU, Reeve BB et al (2016) PROMIS fatigue item bank had clinical validity across diverse chronic conditions. J Clin Epidemiol 73:128–134. https://doi.org/10.1016/j.jclinepi.2015.08.037
Chan A, Lew C, Wang XJ, Ng T, Chae J-W, Yeo HL et al (2018) Psychometric properties and measurement equivalence of the Multidimensional Fatigue Syndrome Inventory-Short Form (MFSI-SF) amongst breast cancer and lymphoma patients in Singapore. Health Qual Life Outcomes 16(1):20. https://doi.org/10.1186/s12955-018-0846-6
Brown LF, Kroenke K, Theobald DE, Wu J (2011) Comparison of SF-36 Vitality scale and Fatigue Symptom Inventory in assessing cancer-related fatigue. Support Care Cancer 19(8):1255–1259. https://doi.org/10.1007/s00520-011-1148-2
Bower JE, Ganz PA, Desmond KA, Rowland JH, Meyerowitz BE, Belin TR (2000) Fatigue in breast cancer survivors: occurrence, correlates, and impact on quality of life. J Clin Oncol 18(4):743. https://doi.org/10.1200/jco.2000.18.4.743
Schünemann HJ, Guyatt GH (2005) Commentary–goodbye M(C)ID! Hello MID, where do you come from? Health Serv Res 40(2):593–597. https://doi.org/10.1111/j.1475-6773.2005.00374.x
Chan A, Yo TE, Wang XJ, Ng T, Chae J-W, Yeo HL et al (2018) Minimal clinically important difference of the Multidimensional Fatigue Symptom Inventory-Short Form (MFSI-SF) for fatigue worsening in Asian breast cancer patients. J Pain Symptom Manage 55(3):992–7.e2. https://doi.org/10.1016/j.jpainsymman.2017.10.014
Yost KJ, Eton DT, Garcia SF, Cella D (2011) Minimally important differences were estimated for six Patient-Reported Outcomes Measurement Information System-Cancer scales in advanced-stage cancer patients. J Clin Epidemiol 64(5):507–516
Nordin Å, Taft C, Lundgren-Nilsson Å, Dencker A (2016) Minimal important differences for fatigue patient reported outcome measures—a systematic review. BMC Med Res Methodol 16(1):62. https://doi.org/10.1186/s12874-016-0167-6
Ousmen A, Touraine C, Deliu N, Cottone F, Bonnetain F, Efficace F et al (2018) Distribution- and anchor-based methods to determine the minimally important difference on patient-reported outcome questionnaires in oncology: a structured review. Health Qual Life Outcomes 16(1):228. https://doi.org/10.1186/s12955-018-1055-z
Revicki D, Hays RD, Cella D, Sloan J (2008) Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol 61(2):102–109. https://doi.org/10.1016/j.jclinepi.2007.03.012
Mouelhi Y, Jouve E, Castelli C, Gentile S (2020) How is the minimal clinically important difference established in health-related quality of life instruments? Review of anchors and methods. Health Qual Life Outcomes 18(1):136. https://doi.org/10.1186/s12955-020-01344-w
Norman GR, Sloan JA, Wyrwich KW (2003) Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care 41(5):582–592. https://doi.org/10.1097/01.mlr.0000062554.74615.4c
Kroenke K, Baye F, Lourens SG (2019) Comparative responsiveness and minimally important difference of common anxiety measures. Med Care 57(11):890–897
Kroenke K, Stump TE, Chen CX, Kean J, Bair MJ, Damush TM et al (2020) Minimally important differences and severity thresholds are estimated for the PROMIS depression scales from three randomized clinical trials. J Affect Disord 266:100–108. https://doi.org/10.1016/j.jad.2020.01.101
Wyrwich KW, Tierney WM, Wolinsky FD (1999) Further evidence supporting an SEM-based criterion for identifying meaningful intra-individual changes in health-related quality of life. J Clin Epidemiol 52(9):861–873. https://doi.org/10.1016/S0895-4356(99)00071-2
Chen CX, Kroenke K, Stump TE, Kean J, Carpenter JS, Krebs EE et al (2018) Estimating minimally important differences for the PROMIS pain interference scales: results from 3 randomized clinical trials. Pain 159(4):775–782. https://doi.org/10.1097/j.pain.0000000000001121
Wyrwich KW, Norquist JM, Lenderking WR, Acaster S, The Industry Advisory Committee of International Society for Quality of Life Research (2013) Methods for interpreting change over time in patient-reported outcome measures. Qual Life Res 22(3):475-83. https://doi.org/10.1007/s11136-012-0175-x
Hays RD, Peipert JD (2021) Between-group minimally important change versus individual treatment responders. Qual Life Res 30(10):2765–2772. https://doi.org/10.1007/s11136-021-02897-z
King MT, Dueck AC, Revicki DA (2019) Can methods developed for interpreting group-level patient-reported outcome data be applied to individual patient management? Med Care 57(Suppl 5 1):S38–S45. https://doi.org/10.1097/MLR.0000000000001111
Donaldson G (2008) Patient-reported outcomes and the mandate of measurement. Qual Life Res 17(10):1303–1313. https://doi.org/10.1007/s11136-008-9408-4
Johns SA, Brown LF, Beck-Coon K, Monahan PO, Tong Y, Kroenke K (2015) Randomized controlled pilot study of mindfulness-based stress reduction for persistently fatigued cancer survivors. Psychooncology 24(8):885–893. https://doi.org/10.1002/pon.3648
Johns SA, Brown LF, Beck-Coon K, Talib TL, Monahan PO, Giesler RB et al (2016) Randomized controlled pilot trial of mindfulness-based stress reduction compared to psychoeducational support for persistently fatigued breast and colorectal cancer survivors. Support Care Cancer 24(10):4085–4096. https://doi.org/10.1007/s00520-016-3220-4
Rogers LQ, McAuley E, Anton PM, Courneya KS, Vicari S, Hopkins-Price P et al (2012) Better exercise adherence after treatment for cancer (BEAT Cancer) study: Rationale, design, and methods. Contemp Clin Trials 33(1):124–137. https://doi.org/10.1016/j.cct.2011.09.004
Rogers LQ, Courneya KS, Anton PM, Hopkins-Price P, Verhulst S, Vicari SK et al (2015) Effects of the BEAT Cancer physical activity behavior change intervention on physical activity, aerobic fitness, and quality of life in breast cancer survivors: a multicenter randomized controlled trial. Breast Cancer Res Treat 149(1):109–119. https://doi.org/10.1007/s10549-014-3216-z
Hann DM, Denniston MM, Baker F (2000) Measurement of fatigue in cancer patients: further validation of the Fatigue Symptom Inventory. Qual Life Res 9(7):847–854
Krebs EE, Lorenz KA, Bair MJ, Damush TM, Wu J, Sutherland JM et al (2009) Development and initial validation of the PEG, a three-item scale assessing pain intensity and interference. J Gen Intern Med 24:733–738. https://doi.org/10.1007/s11606-009-0981-1
Ha DM, Deng LR, Lange AV, Swigris JJ, Bekelman DB (2022) Reliability, validity, and responsiveness of the DEG, a three-item dyspnea measure. J Gen Intern Med. https://doi.org/10.1007/s11606-021-07307-1
Ware JE, Koskinski M. The SF-36 Health Survey (Version 2.0) Technical Note. Boston, MA: Health Assessment Lab; 1996.
Su Y, Cochrane BB, Yu S-Y, Reding K, Herting JR, Zaslavsky O (2022) Fatigue in community-dwelling older adults: A review of definitions, measures, and related factors. Geriatr Nur (Lond) 43:266–279. https://doi.org/10.1016/j.gerinurse.2021.12.010
Bower JE, Ganz PA, Aziz N (2005) Altered cortisol response to psychologic stress in breast cancer survivors with persistent fatigue. Psychosom Med 67(2):277–280. https://doi.org/10.1097/01.psy.0000155666.55034.c6
Bower JE, Ganz PA, Aziz N, Fahey JL (2002) Fatigue and proinflammatory cytokine activity in breast cancer survivors. Psychosom Med 64(4):604–611
Bower JE, Ganz PA, Aziz N, Fahey JL, Cole SW (2003) T-cell homeostasis in breast cancer survivors with persistent fatigue. J Natl Cancer Inst 95(15):1165–1168. https://doi.org/10.1093/jnci/djg0019
Bower JE, Ganz PA, Dickerson SS, Petersen L, Aziz N, Fahey JL (2005) Diurnal cortisol rhythm and fatigue in breast cancer survivors. Psychoneuroendocrinology 30(1):92–100. https://doi.org/10.1016/j.psyneuen.2004.06.003
Donovan KA, Jacobsen PB, Small BJ, Munster PN, Andrykowski MA (2008) Identifying clinically meaningful fatigue with the Fatigue Symptom Inventory. J Pain Symptom Manage 36(5):480–487. https://doi.org/10.1016/j.jpainsymman.2007.11.013
Kenne Sarenmalm E, Mårtensson LB, Andersson BA, Karlsson P, Bergh I (2017) Mindfulness and its efficacy for psychological and biological responses in women with breast cancer. Cancer Med 6(5):1108–1122. https://doi.org/10.1002/cam4.1052
R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2013.
MedCalc Statistical Software [computer program]. 19.2.6 ed. Ostend, Belgium: MedCalc Software Ltd; 2020.
Kazis LE, Anderson JJ, Meenan RF (1989) Effect sizes for interpreting changes in health status. Med Care 27(3):S178–S189
Monahan PO, Boustani MA, Alder C, Galvin JE, Perkins AJ, Healey P et al (2012) Practical clinical tool to monitor dementia symptoms: the HABC-Monitor. Clin Interv Aging 7:143–157. https://doi.org/10.2147/cia.S30663
Kroenke K, Wu J, Yu Z, Bair MJ, Kean J, Stump T et al (2016) Patient Health Questionnaire Anxiety and Depression Scale: Initial validation in three clinical trials. Psychosom Med 78(6):716–727. https://doi.org/10.1097/psy.0000000000000322
Norman GR, Wyrwich KW, Patrick DL (2007) The mathematical relationship among different forms of responsiveness coefficients. Qual Life Res 16(5):815–822. https://doi.org/10.1007/s11136-007-9180-x
Krebs EE, Bair MJ, Damush TM, Tu W, Wu J, Kroenke K (2010) Comparative responsiveness of pain outcome measures among primary care patients with musculoskeletal pain. Med Care 48(11):1007–1014. https://doi.org/10.1097/MLR.0b013e3181eaf835
Cohen J (1992) A power primer. Psychol Bull 112(1):155–159. https://doi.org/10.1037//0033-2909.112.1.155
Eton DT, Cella D, Yost KJ, Yount SE, Peterman AH, Neuberg DS et al (2004) A combination of distribution- and anchor-based approaches determined minimally important differences (MIDs) for four endpoints in a breast cancer scale. J Clin Epidemiol 57(9):898–910. https://doi.org/10.1016/j.jclinepi.2004.01.012
Chen CX, Kroenke K, Stump T, Kean J, Krebs EE, Bair MJ et al (2019) Comparative responsiveness of the PROMIS Pain Interference short forms with legacy pain measures: Results from three randomized clinical trials. J Pain 20(6):664–675
Kroenke K, Stump TE, Chen CX, Kean J, Damush TM, Bair MJ et al (2021) Responsiveness of PROMIS and Patient Health Questionnaire (PHQ) Depression Scales in three clinical trials. Health Qual Life Outcomes 19(1):41
Johns SA, Tarver WL, Secinti E, Mosher CE, Stutz PV, Carnahan JL et al (2021) Effects of mindfulness-based interventions on fatigue in cancer survivors: A systematic review and meta-analysis of randomized controlled trials. Crit Rev Oncol Hematol 160:103290
Mustian KM, Alfano CM, Heckler C, Kleckner AS, Kleckner IR, Leach CR et al (2017) Comparison of pharmaceutical, psychological, and exercise treatments for cancer-related fatigue: a meta-analysis. JAMA Oncol 3(7):961–968. https://doi.org/10.1001/jamaoncol.2016.6914
Kroenke K, Stump TE, Kean J, Talib TL, Haggstrom DA, Monahan PO (2019) PROMIS 4-item measures and numeric rating scales efficiently assess SPADE symptoms compared with legacy measures. J Clin Epidemiol 115:116–124. https://doi.org/10.1016/j.jclinepi.2019.06.018
Ness S, Kokal J, Fee-Schroeder K, Novotny P, Satele D, Barton D (2013) Concerns across the survivorship trajectory: Results from a survey of cancer survivors. Oncol Nurs Forum 40(1):35–42. https://doi.org/10.1188/13.ONF.35-42
Acknowledgements
We thank Isabella Stuart for her assistance. We also thank the original BEAT Cancer and mindfulness-based stress reduction trials’ investigative teams, staff, and participants.
Funding
This work was supported, in part, by the Walther Cancer Foundation (0106–01), the National Cancer Institute (R25CA117865 and R01CA136859), and the Indiana Clinical and Translational Sciences Institute (TR000163 and TR000006) from the National Institutes of Health, National Center for Advancing Translational Sciences. The funding agencies were not involved in the study design, the collection, analysis, and interpretation of data, the writing of the report, or the decision to submit the article for publication.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Data analyses were performed by ES. SJ, KK, and LR assisted with data acquisition and interpretation. The first draft of the manuscript was written by CM and ES, and all authors reviewed, edited, and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The studies were approved by the institutional review boards of all recruitment sites (Indiana University, Southern Illinois University School of Medicine, University of Illinois at Urbana-Champaign). Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Supplemental figures 1 and 2. Empirical cumulative distribution function plots.
Additional file 2.
Supplemental table 1. Patient characteristics.
Additional file 3.
Supplemental table 2. Correlations of change scores among the fatigue scales.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mosher, C.E., Secinti, E., Johns, S.A. et al. Comparative responsiveness and minimally important difference of Fatigue Symptom Inventory (FSI) scales and the FSI-3 in trials with cancer survivors. J Patient Rep Outcomes 6, 82 (2022). https://doi.org/10.1186/s41687-022-00488-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41687-022-00488-1