
Abstract
To date, many kinds of immune cells have been identified, but their precise roles in intestinal immunity remain unclear. Understanding the in vivo behavior of these immune cells and their function in gastrointestinal inflammation, including colitis, inflammatory bowel disease, ischemia–reperfusion injury, and neutrophil extracellular traps, is critical for gastrointestinal research to proceed to the next step. Additionally, understanding the immune responses involved in gastrointestinal tumors and tissue repair is becoming increasingly important for the elucidation of disease mechanisms that have been unknown. In recent years, the application of intravital microscopy in gastrointestinal research has provided novel insights into the mechanisms of intestine-specific events including innate and adaptive immunities. In this review, we focus on the emerging role of intravital imaging in gastrointestinal research and describe how to observe the intestines and immune cells using intravital microscopy. Additionally, we outline novel findings obtained by this new technique.
Similar content being viewed by others


Background
The gastrointestinal tract is a very complex integrated organ that includes a prominent intestinal immune system and plays an important role in life support, including digestion and absorption, while coexisting with the gut microbiome. There is no question about the importance of research into intestinal inflammation, but most findings to date have been based on static evaluation of histological sections, flow cytometry, or an alternative index such as the myeloperoxidase activity. Because conventional research methods do not provide insights into the nature of cellular interactions in vivo during intestinal inflammation, more physiological in vivo, real-time mechanistic analysis has been desired. Recent progress of intravital microscopy (IVM) has enabled the visualization and quantification of immune cell recruitment in vivo [1]. It provides invaluable information about immune cell motion, proliferation, and death processes, as well as cell–cell interactions at the single-cell resolution in a number of organs and disease models. In recent years, IVM has played an emerging role in intestinal research, yielding many insights that were not possible by previous methods. Furthermore, with the development of various transgenic mice and fluorescent antibodies, the subdivision of immune cells that can be observed and the application of IVM are expanding.
This review describes how IVM is used to image the behavior of the gut and associated immune cells during steady-state or inflammatory conditions. We also provide an overview of the invaluable findings obtained by this novel technique with respect to intestinal inflammation, cancer, and tissue repair.
Intravital imaging of the gastrointestinal tract
The development of microscopy techniques from simple light microscopy to confocal microscopy, including laser scanning and spinning disk, and two-photon laser scanning microscopy (TPLSM) has had a significant effect on studying immune responses in living organs using IVM [2, 3]. In a confocal microscope, light is focused to a point and emitted fluorescence passes through a pinhole before reaching the detector. A spinning disk consists of multiple pinholes on a rotating disk, which has the advantage of shortening the scanning process. However, the penetration depth of confocal microscopy is limited, making it difficult to image all layers of the intestinal wall. In TPLSM, a pulsed laser directs two excitation photons of approximately half the energy onto the sample. When these two, low-energy photons hit the fluorophore simultaneously, they are excited to the same level as one high-energy photon. This principle provides numerous advantages including high resolution, deep site imaging of at least 100 µm below the organ surface, less phototoxicity, and less photobleaching compared with conventional confocal microscopy. These advantages make it suitable for long-term imaging of pathophysiological changes in all layers of the intestinal tract. These properties of microscopies have been discussed elsewhere in detail [2,3,4], and we focus on intestinal imaging and the findings obtained by IVM in this review.
Difficulty in controlling intestinal peristalsis and flattening is a major issue when applying intravital imaging to the intestinal tract. To reduce motion artifacts and perform optimal imaging, it is necessary to fix organs using a suction window or glue, appropriate anesthesia to minimize motion artifact, administration of butylscopolamine, or expanding the intestinal wall [5,6,7]. Imaging preparation has been developed on the basis of certain conditions such as the target intestinal layer and whether the microscope is inverted or upright (Figs. 1 and 2). A confocal microscope has a limited capacity to image deep into the intestine, and therefore, the optimal images can be obtained by observing from the side of the object to be observed, whether it is the mucosa or the serosa. We believe that it is important to understand the aforementioned pros and cons of the confocal microscope and TPLSM and to select the microscope that provides the best image of the subject (i.e., intestinal layer, immune cells, disease model, etc.) to be observed. Notably, Rakhilin et al. reported an intravital colonic window using a ferromagnetic scaffold for chronic imaging [8]. Using this technique, they imaged fluorescently labeled Lgr5-positive stem cells, bacteria, and immune cells in the live murine colon. In oncological studies, a surgical orthotopic organoid transplantation approach has been used to visualize colorectal cancer progression in vivo [9].

Preparation for intravital intestinal imaging using an inverted microscope. Representative intestinal fixation method for intravital intestinal imaging from the mucosa (upper row) or serosa (lower row) using an inverted microscope. Details of each method are described in the box below

Preparation for intravital intestinal imaging using an upright microscope. The upper row shows a typical intestinal fixation method for in vivo intestinal imaging using an upright microscope. The intestine is fixed using a suction window. The lower row shows representative intestinal images in CX3CR1GFP/+CCR2RFP/+ mice
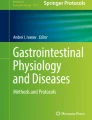
Various fluorescent reporter mice are available for intestinal imaging using IVM. In fact, many new findings have been obtained by capturing the real-time movement of immune cells in the inflamed intestinal tract (Table 1). Specific fluorescent antibodies are similarly useful to identify immune cells and delineate intestinal structures such as blood vessels and lymphatic capillaries [10, 11]. As a novel technique for intravital imaging, mesenteric collecting lymphatic vessel cannulation has enabled in vivo lymph flow assessment [12]. Additionally, Orzekowsky-Schroeder et al. demonstrated the utility of TPLSM excited autofluorescence to differentiate the cell types in living intestines [13]. Intriguingly, metabolic labeling of gut anaerobic bacteria has enabled visualization of the anaerobic microbial niche by various methods, such as IVM and non-invasive whole body imaging, which can be used to observe microbial colonization and host–microbe interactions in real time [14]. Moreover, when an ultrashort pulsed laser beam in the order of femtoseconds is irradiated onto an asymmetric material such as a crystal, light with half the wavelength or twice the frequency of the incident laser beam is emitted. In recent years, with the development of ultrashort pulse lasers such as TPLSM, they have also been used for biological imaging [15]. Second harmonic generation (SHG) is induced in vivo by collagen, myosin, and tubulin. In particular, collagen is abundant and generated with high efficiency. Therefore, it can be visualized specifically in living tissue by SHG imaging and observed without staining (Fig. 3). Maier et al. imaged layers within murine colorectums via SHG and showed that submucosa had the largest collagen fiber diameters, followed by serosa and muscle [16]. They also showed that collagen fibers aligned with muscle fibers in the two muscular layers. These findings would support to identify which of the layers we are observing during intestinal imaging. Moreover, SHG imaging is useful for observing how collagen is produced in response to intestinal inflammation, infection, and tumor development.

Imaging of the second harmonic generation using a two-photon laser scanning microscope. Representative images of second harmonic generation (SHG) in the liver (left) and colon (right) at the steady state obtained under a two-photon laser scanning microscope
Intestinal immune responses in inflammation
Enterocolitis/inflammatory bowel disease (IBD)
In recent years, various new findings have been obtained using the mouse enterocolitis model and IVM technique [27, 28]. Observations targeting various immune cells are also progressing. For example, using LysMeGFP + mice as a neutrophil-targeted study, Lammers et al. revealed slowing of eGFP + neutrophils in vessels and influx into small intestinal mucosal tissue via formyl peptide receptor 1 within 2 h after oral gavage of gliadin, the immunogenic component of gluten and trigger of celiac disease [17]. Using TPLSM, another group reported the activities of extracellular signal-regulated kinase and protein kinase A in neutrophils in inflamed intestines [29]. In an oxazolone-induced colitis model, IVM with fluorescence resonance energy transfer technology showed frequent Ca2+ signaling in B cells of cecal patches during the early phase of colitis, suggesting B cell differentiation into plasma cells [30]. In a monocyte-focused study, interruption of the fractalkine–CX3CR1 axis ameliorated colitis through regulation of intravascular monocyte behaviors on the venous endothelium of inflamed colons in oxazolone-induced colitis models [31]. In a salmonella infection model, IVM revealed that CX3CR1 + macrophages and CD103 + dendritic cells efficiently phagocytosed salmonella using intraepithelial dendrites [19, 20]. Various T cells exist in the intestinal tract, and research using IVM has been widely conducted. A cell dynamics study of Foxp3 + regulatory T cells and intraepithelial CD4 + T cells revealed their distinct, but complementary roles in suppressing intestinal inflammation [23]. Lok et al. used a CD2/IL-13 double reporter mouse to image group 2 innate lymphoid cells [24]. They showed increases in the IL-13 + ILC2 size and movement in Peyer’s patch after helminth infection, but shorter cellular contacts with T cells. Additionally, T cells facilitated the patrolling attributes of group 3 innate lymphoid cells under inflammatory conditions by producing the chemokine CCL25 [25]. Intravital imaging has also shown that GPR55-deficient intraepithelial lymphocytes migrate faster and interact more extensively with epithelial cells [21]. Imaging of the jejunal mucosa in lipopolysaccharide-treated TcrdEGFP mice showed that ɤδ intraepithelial lymphocytes maintain prolonged contact with shedding enterocytes [22]. Another study focused on eosinophils and established EoCre/tdTomato+/− mice [26]. Eosinophils were observed by IVM to rapidly surround murine-specific helminth parasites that invaded the small intestines. To image mast cells in vivo, c-Kit-eGFP mice or Mcpt5-CreROSA26-EYFP double transgenic can be used [32], but they have not been widely used for intravital imaging during intestinal inflammation. Moreover, Koike et al. imaged intestinal microcirculation in a murine necrotizing enterocolitis model using TPLSM and demonstrated that remote ischemic conditioning in the early stages of disease progression counteracted the poor microcirculatory response to formula feeding and preserved the arteriole flow velocity, diameter, and flow volume [33, 34].
IBD is a general term for diseases that cause uncontrolled chronic inflammation in the intestinal mucosa and generally refers to ulcerative colitis and Crohn’s disease. The dextran sulfate sodium (DSS) colitis model has been widely used as an animal model of IBD. Intravital imaging of DSS-induced colitis using TPLSM and an organ-stabilizing system revealed an irregularity and disappearance of crypts, infiltration of immune cells, and increased rolling of white blood cells along the vascular wall [35]. Administration of 5A peptide decreased leukocyte–endothelium interactions [36]. Furthermore, real-time imaging of a bacterial translocation model showed that RFP-Escherichia coli translocated from the luminal side of the intestines into blood vessels. Administration of steroids ameliorated intravital three-dimensional dynamic pathological changes caused by DSS-induced colitis [37]. Our observations showed that the gut microbiota affects the tissue repair process in DSS-induced colitis by facilitating blood-derived monocyte conversion from classical CCR2hiCX3CR1lo monocytes to alternative CCR2loCX3CR1hi monocytes [18]. Peritoneal GATA6 + macrophages were microbiome-independently recruited to the colon in a DSS colitis model and contributed to ameliorating intestinal inflammation [38].
Intestinal ischemia–reperfusion injury (IRI)
Intestinal IRI is related to various clinical conditions, such as ischemic enteritis, abdominal surgeries, and organ transplantation, and reduces patient survival because of bacterial translocation, systemic inflammation, intestinal necrosis, and multiple organ failure. We observed real-time neutrophil recruitment during IRI in small intestines using LysMegfp mice and TPLSM [5]. This method enabled real-time assessment of neutrophil recruitment and pathophysiological changes in the intestinal wall in vivo. Voisin et al. showed that blocking neutrophil elastase-dependent neutrophil extravasation may be an effective strategy to reduce the number and activation of neutrophils in IRI, but it may also inhibit the recruitment of tissue-healing immune cells including monocytes and M2 macrophages [39]. Systemic treatment of mice with sulforaphane, an isothiocyanate with anti-inflammatory characteristics, reduced platelet activation and blocked leukocyte adhesion, significantly reducing leukocyte rolling at 2 and 8 h after intestinal IRI [40]. Moreover, the transfer of sulforaphane-treated platelets significantly reduced rolling leukocytes during reperfusion.
NETs
Neutrophil extracellular traps (NETs) are the formation and release of sticky web-like structures composed of decondensed chromatin filaments that are decorated with histones and neutrophil granule proteins [41]. NETs play a pivotal role in intestinal infection by helping neutrophils catch and kill pathogens. Moreover, excessive NET formation has proinflammatory characteristics and induces innate immune responses [42]. Although many IVM studies on NETs have focused on the liver, Tanaka et al. successfully visualized NETs in vivo in the postcapillary venules of the murine cecum using the lipopolysaccharide-induced sepsis model [43]. They also observed leukocytes with cytoplasmic vacuoles that adhered to the vascular endothelium in LPS-treated mice at the subcellular level, and some of them released NETs. As discussed below, it has also been shown that colon cancer induces NETs in the liver, thereby promoting circulating cancer cell adhesion and liver metastasis [44]. Thus, the relationship between intestinal inflammation and NETs is a very interesting research field, but research using IVM has not progressed thus far and future development is desired.
Immunity in colorectal cancer
IVM techniques have been applied to gastrointestinal cancer research. Mainly by analyzing colorectal cancer (CRC) metastasis models using tumor-specific transgenic mice and fluorescence-labeled cancer cell lines, the dynamics of tumor cells, tumor angiogenesis, chemotherapy responses in the liver microenvironment, and interactions with various immune cells have been clarified [45,46,47,48]. IVM through an abdominal imaging window allowed imaging a single step of CRC metastasis formation in the liver over 2 weeks [49]. Single extravasated CRC tumor cells proliferated to form pre-micrometastases, where tumor cells were active and motile within a confined region of the growing clone. Conversely, tumor cells within micrometastases were immotile. Fumagalli et al. reported real-time migration patterns of Lgr5 + and Lgr5 − CRC cells using a CRC mouse model generated by orthotopic transplantation of CRC organoids (RFP-Confetti and CRC Lgr5eGFR) [50]. They found that the majority of CRC cells in circulation were Lgr5 − and caused distant metastases in which Lgr5 + CRCs appeared. Another study focused on the cell cycle and performed intravital imaging of fluorescence ubiquitination-based cell cycle indicator (Fucci)-bearing human CRC cells [51]. Unexpectedly, S/G2/M Fucci green cells were more motile and invasive compared with Fucci red G1 cells. Intravital imaging of subcutaneously implanted CRC organoids using an imaging window enabled live genetic lineage tracing at the single-cell level over 30 days [52]. Dormant LGR5 + CRC stem cells are characterized by p27 expression, and IVM revealed that LGR5 + p27 + cells survive chemotherapy and then undergo clonal expansion. Intrasplenic injection of the CRC cell line MC38-RFP showed a significant increase in hepatic sinusoidal adhesion of MC38-RFP cells in tumor-bearing mice (TBM) compared to non-TBM, DAase1- or NET inhibitor-treated TBM, and PAD4 − / − TBM [44]. These data suggest that colon cancer induces NETs in the liver to facilitate the adhesion of circulating cancer cells and hepatic metastases. Similarly, the same group also reported high expression of NOD1 in human and murine CRC cell lines, and NOD1 activation augmented CRC cell adhesion in hepatic sinusoids [53]. As another model, Shimura et al. established a xenograft model of metastatic gastric cancer in the peritoneum using RFP-expressing gastric cancer cell line NUGC4 [54]. Overall, these results suggest that combining IVM data, which focuses on the real-time movement of cancer cells, and in vitro experimental results would enable the development of new treatment strategies for gastrointestinal cancer.
Interestingly, a recent study showed that peritoneal GATA6 + macrophages invade CRC liver metastases directly from the peritoneal cavity by sensing tumor-induced mesothelial injury [55]. Moreover, intravital imaging has revealed that peritoneal GATA6 + macrophages upregulate PD-L1 upon taking up apoptotic bodies from tumor cells and promote the growth of CRC liver metastases. These findings might lead to novel therapeutic strategies for CRC liver metastasis and its recurrence by manipulating peritoneal GATA6 + macrophages and considering the intraperitoneal cavity as a more effective route of drug administration.
Mechanisms of tissue repair in intestinal injury
The study of the immune system during tissue damage is important for elucidating tissue repair mechanisms, and research using intravital imaging has provided many insights. Studies using a liver sterile injury model have shown that the first immune cells mobilized during tissue remodeling are platelets and neutrophils and recently revealed GATA6-positive peritoneal cavity macrophages [56, 57]. Subsequently, accumulation of CCR2-positive classical monocytes occurs, which are converted to CX3CR1-positive monocytes and macrophages that act in tissue repair [58]. iNKT cells orchestrate monocyte conversion from inflammation to resolution by producing interleukin-4 [59]. In a model of acute intestinal injury, IVM showed that neutrophils followed by CCR2-positive monocytes are accumulating into the injured area (Fig. 4). CCR2, Nr4a1, and the microbiome were necessary for appropriate monocyte recruitment, conversion, and development to mature CX3CR1-positive macrophages, allowing debris removal and rapid repair of the vasculature [18]. The same mechanisms are needed to repair colonic ulcers caused by DSS-induced colitis. Recently, we have shown that large F4/80hiGATA6-positive peritoneal cavity macrophages promptly accumulate at damaged intestinal sites via a direct route from the peritoneal cavity [38]. Compared with bloodstream-derived monocytes/macrophages, recruitment of cavity macrophages depended on ATP released by dead cells and exposed hyaluronan at the injury site. They contributed to the removal of necrotic cells, revascularization, and collagen deposition and thus resolution of intestinal tissue damage. The roles of platelets, neutrophils, and iNKT cells in intestinal tissue repair have not been investigated in detail and are a topic for further research.

LysMhi neutrophils and CCR2+ monocytes accumulate in injured intestines. Representative images of the colonic lamina propria over 10 min at 4 h after focal intestinal injury in LysMGFP/+CCR2RFP/+ mice. White and yellow arrows indicate migration paths of neutrophils and CCR2+ monocytes for 10 min, respectively
The epithelial barrier function contributes to maintaining intestinal tissue homeostasis. Focusing on continuous renewal and turnover of the intestinal epithelium, imaging of intestinal crypts by IVM with an abdominal window and Lgr5EGFP−Ires−CreERT2 mice enabled tracing the fate of individual Lgr5 + intestinal stem cells and their progeny over time [60]. Bruens et al. used this approach and revealed that crypt fission and fusion in the intestinal epithelium regulate crypt numbers as a counterbalancing mechanism [61]. Another study showed that, when crypt cells were ablated, they were expelled from the crypt base by the rapid motion of crypt cells [62]. Subsequently, Lgr5 + stem cells and Paneth cells restored the alteration in the pattern. Interestingly, these mechanisms were impaired by inhibition of the ROCK pathway and aging. Using RAC1 knockout mice, it has also been shown that impairment of epithelial RAC1 functions causes cell overcrowding and epithelial leakage [63]. Future studies may reveal the mechanisms of the motion dynamics of crypt cells in more detail, leading to new insights into the intestinal epithelium repair process.
Conclusions and future perspectives
The development of intravital imaging has provided new insights into in vivo, real-time immunological processes in many organs and disease models. We recently revealed that dysbiosis alters the localization of intestinal lamina propria macrophages [18], and imaging of the immuno-biome will be challenging, but very intriguing in the future. In vivo fluorescence imaging of the gastrointestinal system is a new research field and has a great advantage of being able to directly capture physiological phenomena in the living state. Because it is possible to elucidate the pathophysiology of intestinal inflammation, which was previously only evaluated statically, and to evaluate the mechanism-of-action of drugs over time, it is expected to be a new experimental model suitable for clinical research.
Availability of data and materials
Not applicable.
Abbreviations
- IVM:
-
Intravital microscopy
- TPLSM:
-
Two-photon laser scanning microscopy
- SHG:
-
Second harmonic generation
- IBD:
-
Inflammatory bowel disease
- DSS:
-
Dextran sulfate sodium
- IRI:
-
Ischemia–reperfusion injury
- NETs:
-
Neutrophil extracellular traps
- CRC:
-
Colorectal cancer
References
Pittet MJ, Weissleder R. Intravital imaging. Cell. 2011;147(5):983–91.
Jorch SK, Deppermann C. Intravital imaging allows organ-specific insights into immune functions. Front Cell Dev Biol. 2021;9:623906.
Kitching AR, Hickey MJ. Immune cell behaviour and dynamics in the kidney - insights from in vivo imaging. Nat Rev Nephrol. 2022;18(1):22–37.
Giampetraglia M, Weigelin B. Recent advances in intravital microscopy for preclinical research. Curr Opin Chem Biol. 2021;63:200–8.
Hashimoto S, Honda M, Takeichi T, Sakisaka M, Narita Y, Yoshii D, Uto K, Sakamoto S, Inomata Y. Intravital imaging of neutrophil recruitment in intestinal ischemia-reperfusion injury. Biochem Biophys Res Commun. 2018;495(3):2296–302.
Kolesnikov M, Farache J, Shakhar G. Intravital two-photon imaging of the gastrointestinal tract. J Immunol Methods. 2015;421:73–80.
Erreni M, Doni A, Weigert R. Method for acute intravital imaging of the large intestine in live mice. Methods Mol Biol. 2021;2304:285–99.
Rakhilin N, Garrett A, Eom CY, Chavez KR, Small DM, Daniel AR, Kaelberer MM, Mejooli MA, Huang Q, Ding S, et al. An intravital window to image the colon in real time. Nat Commun. 2019;10(1):5647.
Fumagalli A, Suijkerbuijk SJE, Begthel H, Beerling E, Oost KC, Snippert HJ, van Rheenen J, Drost J. A surgical orthotopic organoid transplantation approach in mice to visualize and study colorectal cancer progression. Nat Protoc. 2018;13(2):235–47.
Cifarelli V, Eichmann A. The intestinal lymphatic system: functions and metabolic implications. Cell Mol Gastroenterol Hepatol. 2019;7(3):503–13.
Choe K, Jang JY, Park I, Kim Y, Ahn S, Park DY, Hong YK, Alitalo K, Koh GY, Kim P. Intravital imaging of intestinal lacteals unveils lipid drainage through contractility. J Clin Invest. 2015;125(11):4042–52.
Czepielewski RS, Erlich EC, Onufer EJ, Young S, Saunders BT, Han YH, Wohltmann M, Wang PL, Kim KW, Kumar S, et al. Ileitis-associated tertiary lymphoid organs arise at lymphatic valves and impede mesenteric lymph flow in response to tumor necrosis factor. Immunity. 2021;54(12):2795-811 e9.
Orzekowsky-Schroeder R, Klinger A, Martensen B, Blessenohl M, Gebert A, Vogel A, Huttmann G. In vivo spectral imaging of different cell types in the small intestine by two-photon excited autofluorescence. J Biomed Opt. 2011;16(11):116025.
Geva-Zatorsky N, Alvarez D, Hudak JE, Reading NC, Erturk-Hasdemir D, Dasgupta S, von Andrian UH, Kasper DL. In vivo imaging and tracking of host-microbiota interactions via metabolic labeling of gut anaerobic bacteria. Nat Med. 2015;21(9):1091–100.
You S, Tu H, Chaney EJ, Sun Y, Zhao Y, Bower AJ, Liu YZ, Marjanovic M, Sinha S, Pu Y, et al. Intravital imaging by simultaneous label-free autofluorescence-multiharmonic microscopy. Nat Commun. 2018;9(1):2125.
Maier F, Siri S, Santos S, Chen L, Feng B, Pierce DM. The heterogeneous morphology of networked collagen in distal colon and rectum of mice quantified via nonlinear microscopy. J Mech Behav Biomed Mater. 2021;113:104116.
Lammers KM, Chieppa M, Liu L, Liu S, Omatsu T, Janka-Junttila M, Casolaro V, Reinecker HC, Parent CA, Fasano A. Gliadin induces neutrophil migration via engagement of the formyl peptide receptor, FPR1. PLoS ONE. 2015;10(9):e0138338.
Honda M, Surewaard BGJ, Watanabe M, Hedrick CC, Lee WY, Brown K, McCoy KD, Kubes P. Perivascular localization of macrophages in the intestinal mucosa is regulated by Nr4a1 and the microbiome. Nat Commun. 2020;11(1):1329.
Niess JH, Brand S, Gu X, Landsman L, Jung S, McCormick BA, Vyas JM, Boes M, Ploegh HL, Fox JG, et al. CX3CR1-mediated dendritic cell access to the intestinal lumen and bacterial clearance. Science. 2005;307(5707):254–8.
Farache J, Koren I, Milo I, Gurevich I, Kim KW, Zigmond E, Furtado GC, Lira SA, Shakhar G. Luminal bacteria recruit CD103+ dendritic cells into the intestinal epithelium to sample bacterial antigens for presentation. Immunity. 2013;38(3):581–95.
Sumida H, Lu E, Chen H, Yang Q, Mackie K, Cyster JG. GPR55 regulates intraepithelial lymphocyte migration dynamics and susceptibility to intestinal damage. Sci Immunol. 2017;2(18):eaao1135.
Hu MD, Golovchenko NB, Burns GL, Nair PM, Kelly TJT, Agos J, Irani MZ, Soh WS, Zeglinski MR, Lemenze A, et al. Gammadelta intraepithelial lymphocytes facilitate pathological epithelial cell shedding via CD103-mediated granzyme release. Gastroenterology. 2022;162(3):877-89 e7.
Sujino T, London M, Hoytema van Konijnenburg DP, Rendon T, Buch T, Silva HM, Lafaille JJ, Reis BS, Mucida D. Tissue adaptation of regulatory and intraepithelial CD4(+) T cells controls gut inflammation. Science. 2016;352(6293):1581–6.
Lok LSC, Walker JA, Jolin HE, Scanlon ST, Ishii M, Fallon PG, McKenzie ANJ, Clatworthy MR. Group 2 innate lymphoid cells exhibit tissue-specific dynamic behaviour during type 2 immune responses. Front Immunol. 2021;12:711907.
Jarade A, Garcia Z, Marie S, Demera A, Prinz I, Bousso P, Di Santo JP, Serafini N. Inflammation triggers ILC3 patrolling of the intestinal barrier. Nat Immunol. 2022;23(9):1317–23.
Nguyen WNT, Jacobsen EA, Finney CAM, Colarusso P, Patel KD. Intravital imaging of eosinophils: unwrapping the enigma. J Leukoc Biol. 2020;108(1):83–91.
Sullivan DP, Bui T, Muller WA, Butin-Israeli V, Sumagin R. In vivo imaging reveals unique neutrophil transendothelial migration patterns in inflamed intestines. Mucosal Immunol. 2018;11(6):1571–81.
Dickson K, Malitan H, Lehmann C. Imaging of the intestinal microcirculation during acute and chronic inflammation. Biology (Basel). 2020;9(12):418.
Mizuno R, Kamioka Y, Kabashima K, Imajo M, Sumiyama K, Nakasho E, Ito T, Hamazaki Y, Okuchi Y, Sakai Y, et al. In vivo imaging reveals PKA regulation of ERK activity during neutrophil recruitment to inflamed intestines. J Exp Med. 2014;211(6):1123–36.
Watabe T, Nagaishi T, Tsugawa N, Kojima Y, Jose N, Hosoya A, Onizawa M, Nemoto Y, Oshima S, Nakamura T, et al. B cell activation in the cecal patches during the development of an experimental colitis model. Biochem Biophys Res Commun. 2018;496(2):367–73.
Kuboi Y, Nishimura M, Ikeda W, Nakatani T, Seki Y, Yamaura Y, Ogawa K, Hamaguchi A, Muramoto K, Mizuno K, et al. Blockade of the fractalkine-CX3CR1 axis ameliorates experimental colitis by dislodging venous crawling monocytes. Int Immunol. 2019;31(5):287–302.
Tikoo S, Barki N, Jain R, Zulkhernain NS, Buhner S, Schemann M, Weninger W. Imaging of mast cells. Immunol Rev. 2018;282(1):58–72.
Chen Y, Koike Y, Chi L, Ahmed A, Miyake H, Li B, Lee C, Delgado-Olguin P, Pierro A. Formula feeding and immature gut microcirculation promote intestinal hypoxia, leading to necrotizing enterocolitis. Dis Model Mech. 2019;12(12):dmm040998.
Koike Y, Li B, Ganji N, Zhu H, Miyake H, Chen Y, Lee C, Janssen Lok M, Zozaya C, Lau E, et al. Remote ischemic conditioning counteracts the intestinal damage of necrotizing enterocolitis by improving intestinal microcirculation. Nat Commun. 2020;11(1):4950.
Toiyama Y, Mizoguchi A, Okugawa Y, Koike Y, Morimoto Y, Araki T, Uchida K, Tanaka K, Nakashima H, Hibi M, et al. Intravital imaging of DSS-induced cecal mucosal damage in GFP-transgenic mice using two-photon microscopy. J Gastroenterol. 2010;45(5):544–53.
Nowacki TM, Remaley AT, Bettenworth D, Eisenblatter M, Vowinkel T, Becker F, Vogl T, Roth J, Tietge UJ, Lugering A, et al. The 5A apolipoprotein A-I (apoA-I) mimetic peptide ameliorates experimental colitis by regulating monocyte infiltration. Br J Pharmacol. 2016;173(18):2780–92.
Morimoto Y, Tanaka K, Toiyama Y, Inoue Y, Araki T, Uchida K, Kimura K, Mizoguchi A, Kusunoki M. Intravital three-dimensional dynamic pathology of experimental colitis in living mice using two-photon laser scanning microscopy. J Gastrointest Surg. 2011;15(10):1842–50.
Honda M, Kadohisa M, Yoshii D, Komohara Y, Hibi T. Directly recruited GATA6 + peritoneal cavity macrophages contribute to the repair of intestinal serosal injury. Nat Commun. 2021;12(1):7294.
Voisin MB, Leoni G, Woodfin A, Loumagne L, Patel NS, Di Paola R, Cuzzocrea S, Thiemermann C, Perretti M, Nourshargh S. Neutrophil elastase plays a non-redundant role in remodeling the venular basement membrane and neutrophil diapedesis post-ischemia/reperfusion injury. J Pathol. 2019;248(1):88–102.
Chen Z, Mohr A, Heitplatz B, Hansen U, Pascher A, Brockmann JG, Becker F. Sulforaphane elicits protective effects in intestinal ischemia reperfusion injury. Int J Mol Sci. 2020;21(15):5189.
Honda M, Kubes P. Neutrophils and neutrophil extracellular traps in the liver and gastrointestinal system. Nat Rev Gastroenterol Hepatol. 2018;15(4):206–21.
Chen F, Liu Y, Shi Y, Zhang J, Liu X, Liu Z, Lv J, Leng Y. The emerging role of neutrophilic extracellular traps in intestinal disease. Gut Pathog. 2022;14(1):27.
Tanaka K, Koike Y, Shimura T, Okigami M, Ide S, Toiyama Y, Okugawa Y, Inoue Y, Araki T, Uchida K, et al. In vivo characterization of neutrophil extracellular traps in various organs of a murine sepsis model. PLoS ONE. 2014;9(11):e111888.
Rayes RF, Mouhanna JG, Nicolau I, Bourdeau F, Giannias B, Rousseau S, Quail D, Walsh L, Sangwan V, Bertos N, et al. Primary tumors induce neutrophil extracellular traps with targetable metastasis promoting effects. JCI Insight. 2019;5(16):e128008.
Tanaka K, Morimoto Y, Toiyama Y, Okugawa Y, Inoue Y, Uchida K, Kimura K, Mizoguchi A, Kusunoki M. Intravital dual-colored visualization of colorectal liver metastasis in living mice using two photon laser scanning microscopy. Microsc Res Tech. 2012;75(3):307–15.
Tanaka K, Morimoto Y, Toiyama Y, Matsushita K, Kawamura M, Koike Y, Okugawa Y, Inoue Y, Uchida K, Araki T, et al. In vivo time-course imaging of tumor angiogenesis in colorectal liver metastases in the same living mice using two-photon laser scanning microscopy. J Oncol. 2012;2012:265487.
Tanaka K, Okigami M, Toiyama Y, Morimoto Y, Matsushita K, Kawamura M, Hashimoto K, Saigusa S, Okugawa Y, Inoue Y, et al. In vivo real-time imaging of chemotherapy response on the liver metastatic tumor microenvironment using multiphoton microscopy. Oncol Rep. 2012;28(5):1822–30.
Okigami M, Tanaka K, Inoue Y, Saigusa S, Okugawa Y, Toiyama Y, Mohri Y, Kusunoki M. Intravital imaging of the effects of 5-fluorouracil on the murine liver microenvironment using 2-photon laser scanning microscopy. Oncol Lett. 2016;11(4):2433–9.
Ritsma L, Steller EJ, Beerling E, Loomans CJ, Zomer A, Gerlach C, Vrisekoop N, Seinstra D, van Gurp L, Schafer R, et al. Intravital microscopy through an abdominal imaging window reveals a pre-micrometastasis stage during liver metastasis. Sci Transl Med. 2012;4(158):158ra45.
Fumagalli A, Oost KC, Kester L, Morgner J, Bornes L, Bruens L, Spaargaren L, Azkanaz M, Schelfhorst T, Beerling E, et al. Plasticity of Lgr5-negative cancer cells drives metastasis in colorectal cancer. Cell Stem Cell. 2020;26(4):569-78 e7.
Kagawa Y, Matsumoto S, Kamioka Y, Mimori K, Naito Y, Ishii T, Okuzaki D, Nishida N, Maeda S, Naito A, et al. Cell cycle-dependent Rho GTPase activity dynamically regulates cancer cell motility and invasion in vivo. PLoS ONE. 2013;8(12):e83629.
Ohta Y, Fujii M, Takahashi S, Takano A, Nanki K, Matano M, Hanyu H, Saito M, Shimokawa M, Nishikori S, et al. Cell-matrix interface regulates dormancy in human colon cancer stem cells. Nature. 2022;608(7924):784–94.
Jiang HY, Najmeh S, Martel G, MacFadden-Murphy E, Farias R, Savage P, Leone A, Roussel L, Cools-Lartigue J, Gowing S, et al. Activation of the pattern recognition receptor NOD1 augments colon cancer metastasis. Protein Cell. 2020;11(3):187–201.
Shimura T, Tanaka K, Toiyama Y, Okigami M, Ide S, Kitajima T, Kondo S, Saigusa S, Ohi M, Araki T, et al. In vivo optical pathology of paclitaxel efficacy on the peritoneal metastatic xenograft model of gastric cancer using two-photon laser scanning microscopy. Gastric Cancer. 2015;18(1):109–18.
Hossain M, Shim R, Lee WY, Sharpe AH, Kubes P. Gata6(+) resident peritoneal macrophages promote the growth of liver metastasis. Nat Commun. 2022;13(1):4406.
Slaba I, Wang J, Kolaczkowska E, McDonald B, Lee WY, Kubes P. Imaging the dynamic platelet-neutrophil response in sterile liver injury and repair in mice. Hepatology. 2015;62(5):1593–605.
Wang J, Kubes P. A reservoir of mature cavity macrophages that can rapidly invade visceral organs to affect tissue repair. Cell. 2016;165(3):668–78.
Dal-Secco D, Wang J, Zeng Z, Kolaczkowska E, Wong CH, Petri B, Ransohoff RM, Charo IF, Jenne CN, Kubes P. A dynamic spectrum of monocytes arising from the in situ reprogramming of CCR2+ monocytes at a site of sterile injury. J Exp Med. 2015;212(4):447–56.
Liew PX, Lee WY, Kubes P. iNKT cells orchestrate a switch from inflammation to resolution of sterile liver injury. Immunity. 2017;47(4):752-65 e5.
Ritsma L, Ellenbroek SIJ, Zomer A, Snippert HJ, de Sauvage FJ, Simons BD, Clevers H, van Rheenen J. Intestinal crypt homeostasis revealed at single-stem-cell level by in vivo live imaging. Nature. 2014;507(7492):362–5.
Bruens L, Ellenbroek SIJ, van Rheenen J, Snippert HJ. In vivo imaging reveals existence of crypt fission and fusion in adult mouse intestine. Gastroenterology. 2017;153(3):674-7 e3.
Choi J, Rakhilin N, Gadamsetty P, Joe DJ, Tabrizian T, Lipkin SM, Huffman DM, Shen X, Nishimura N. Intestinal crypts recover rapidly from focal damage with coordinated motion of stem cells that is impaired by aging. Sci Rep. 2018;8(1):10989.
Martinez-Sanchez LDC, Ngo PA, Pradhan R, Becker LS, Boehringer D, Soteriou D, Kubankova M, Schweitzer C, Koch T, Thonn V, et al. Epithelial RAC1-dependent cytoskeleton dynamics controls cell mechanics, cell shedding and barrier integrity in intestinal inflammation. Gut 2022.
Acknowledgements
We thank Mitchell Arico from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Funding
This work was supported by grants from the Ministry of Education, Culture, Sports, Sciences and Technology of Japan (KAKENHI 19H03716) and Mebae Research Promotion Project NEO (Kumamoto University).
Author information
Authors and Affiliations
Contributions
MH provided the study concept and design. MH and MK participated in the data collection. MH had full access to all the study data, wrote the initial draft of the manuscript, and had the final responsibility for the decision to submit for publication. All authors participated in drafting reviewing and approval of the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Honda, M., Kadohisa, M., Yoshii, D. et al. Intravital imaging of immune responses in intestinal inflammation. Inflamm Regener 43, 9 (2023). https://doi.org/10.1186/s41232-023-00262-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41232-023-00262-w