
Abstract
In this article, I investigate the association between maternal socioeconomic status (SES) and children’s birth outcomes (birth weight) across three different birth cohorts. I also perform mediation analysis to assess the degree to which maternal smoking habits during pregnancy account for this relationship. I draw from three UK cohort studies: the 1958 National Child Developmental Study (NCDS); the 1970 British Cohort (B70); and the 2001 Millennium Cohort study (MCS). There are two main results. First, low-SES mothers are more likely to have children with poor birth outcomes and this association has remained persistent throughout the last 50 years. Second, smoking explains a large part of this association, but only in the two most recent cohorts.
Similar content being viewed by others

Introduction
There is a vast literature focusing on trends in demographic phenomena. Much attention has being given to long term fluctuations in fertility, age at first child, as well as mortality and infant mortality (Christensen et al., 2009; Frejka & Sardon, 2006; Goldstein et al., 2009) and the variation of these trends by different socio-economic groups (Arntzen et al., 2004; Jalovaara et al., 2019; Masters et al., 2015). However, trends in other important population outcomes such as birth outcomes have received surprisingly less attention. Birth outcomes as birth weight (BW) and low birth weight (LBW) have been shown to be important predictor of future socio-economic success (Almond & Mazumder, 2013; Härkönen et al., 2012; Heckman, 2007; Torche & Conley, 2016). They have been also shown to be socially stratified (Currie, 2011; Kramer et al., 2000), making them a first pathway of transmitting socio-economic status from one generation to the next.
A few studies have showed a persistent longitudinal association between maternal socio-economic status and birth outcomes (Aizer & Currie, 2014; Fairley & Leyland, 2006; Moser et al., 2003; Ward, 2015). However, studies addressing socioeconomic inequality in birth outcomes usually examine a short time span (Aizer & Currie, 2014; Fairley & Leyland, 2006; Moser et al., 2003). Furthermore, little is known on the underlying determinants of the observed trends in SES inequality in birth outcomes. A particularly important factor accounting for inequalities in birth outcomes may be maternal smoking behaviors. Smoking is the most important cause of poor birth outcomes in developed countries (Kramer et al., 2000; Rogers, 2009), and it has a strong social gradient, which changed notably over time (Fertig, 2010; Pampel, 2005; Thun et al., 2012).
In this article, I provide novel evidence on the association between SES and BW across three British cohorts over a time span of almost 50 years and examine what may account for the association over time. More specifically, I posit four research questions. First, is there an association between SES and BW? Second, how has this association changed over time? Third, does maternal smoking in pregnancy account for the SES gradient in BW? Fourth, how has its relevance changed over time? To answer these research questions, I draw on three large-scale representative cohort studies from the United Kingdom: the 1958 National Child Development Study (NCDS), the 1970 British Cohort (B70), and the 2001 Millennium Cohort Study (MCS).
Background
Birth weight and its stratification
The social environment a mother lives in plays a crucial role in triggering the biological processes shaping birth weight. Research has shown how, consistently across countries with different levels of development, maternal socio-economic conditions are linked to their children’s fetal development and ultimately to their birth outcomes, with children born from low socio-economic mothers showing lower birth weight, shorter gestational length, higher incidence of low birth weight and pre-term births (Currie, 2011; Kramer et al., 2000). There may be many causes linking maternal socioeconomic conditions to birth outcomes (de Graaf et al., 2013). Material conditions specific to disadvantaged mothers such as low financial resources, poor housing conditions, restricted access to healthcare, and unstable working conditions may have a detrimental effect on maternal health and consequently on birth weight (Aizer et al., 2016; Persson & Rossin-Slater, 2018; Tattarini et al., 2018). Environmental and community factors may also play a role, as poor mothers are more often exposed to residential segregation in poor neighborhoods and to high level of toxic pollutants, chemicals, violence, and stress, and worse climatic conditions (Conte Keivabu & Cozzani, 2022; Cozzani et al., 2021a, 2021b; Currie, 2011; Slama et al., 2008). Psychosocial conditions such as resilience to stress and access to social support may also play in harming or sheltering birth outcomes (Turner & Avison, 2003). Non-material resources such as health literacy, and education, may also shape maternal health and thus affect fetal development (de Graaf et al., 2013).
Among the social determinants of birth weight, stratified health behaviors may play a pivotal role in shaping SES inequalities in birth outcomes, especially in developed countries, where access to nutrition is not a major concern (Kramer et al., 2000). Research has shown that there is a strong SES gradient in a large set of unhealthy behaviors such has having a poor diet, scarce physical activity, tobacco, and alcohol consumption (Pampel et al., 2010).Footnote 1 The SES gradient in health behaviors holds also for pregnant women, as low-SES mothers are more likely to smoke during pregnancy than their higher SES counterparts (Härkönen et al., 2018). Moreover, maternal smoking is likely to be one of the strongest determinant of SES inequalities in birth outcomes across developed countries, as it is both highly prevalent in the population and strongly socially stratified (Kramer et al., 2000).
Trends in birth outcomes: previous research
There is plenty of research investigating how and why demographic phenomena such as fertility and mortality vary across decades and even centuries (Christensen et al., 2009; Goldstein et al., 2009). Other phenomena such birth outcomes, on the other hand, have received surprisingly less attention, but they also evolve over time. Birth outcomes follow secular trends in epidemiological conditions, population compositional changes, maternal behaviors, and technological innovations. A recent longitudinal analysis examined birth weight distributions across the nineteenth and twentieth century and found a substantial stagnation in average birth weight in the US (Schneider, 2017). Other studies have investigated recent trends in birth weight in the UK, and they generally found that newborns were getting bigger (Bonellie & Raab, 1997; Ghosh et al., 2018; Power, 1994). Yet, investigations from other countries (i.e., France, Germany, and the US) showed a small decrease in average birth weight within the last two decades (Diouf et al., 2011; Donahue et al., 2010; Schiessl et al., 2009). These discordant findings may be due to various reasons. First, compositional changes in the population of live births may alter the population averages. The increasing amount of multiple births due the sharp increase in medical assisted reproduction (MAR) in the last decades (Pison et al., 2015), for example, may have reduced average birth weight at the population level, as twins are usually smaller than singleton newborns. Second, improvement in maternal nutrition, the introduction of supplements, and overall more attention towards maternal health during pregnancy may have boosted birth outcomes over time. Third, medical technological advancements aimed at improving perinatal health may have reduced stillbirths, which, in turn, may increase the share of low-birth-weight deliveries, slowing improvement in average birth weight. Fourth, and likely with a large importance in advanced societies, changes in health behaviors, such as smoking, which peaked and then started to reduce in the twentieth centuries, following the stages of the tobacco epidemic (Lopez et al., 1994), may have improved birth outcomes over time. Moreover, these mechanisms may work simultaneously and may be true for some population groups but not for others.
Regarding socio-economic differences in birth weight, Aizer and Currie (2014) found substantial differences in birth weight between advantaged and disadvantaged mothers in the US, which has slightly decreased across the 1990s and the early 2000s. In the UK, Moser et al. (2003) found that class differences in birth weight remained constant across the 1990s. Similarly, also Maher and Macfarlane (2004) found stable class differences in birth weight between the 1980s and the 1990s. To sum up, despite some improvements in birth weight at the population level, research investigating socioeconomic differences in birth weight has reported stable or only small reductions in socioeconomic inequality in birth outcomes over time. There may be many forces at work in different groups in generating trends in inequalities in birth outcomes. On one hand, it may be possible that the selective growth of MAR births among high SES groups (Cozzani et al., 2021a; Goisis et al., 2020, 2023) may have slowed the advancement in birth outcomes among them. On the other hand, the capability of having higher returns of medical advancements may instead have boosted high SES children’s birth outcomes (Link & Phelan, 1995). In addition, the capability of rescuing frail fetuses may be more relevant among low SES groups, which may have higher stillbirths and miscarriages rates, slowing more their birth outcomes advancements. Finally, and again more importantly, tobacco consumption changes happened heterogeneously in the twentieth century, with high SES being the firstcomer in abandoning this behavior and low SES the last ones (Thun et al., 2012). Overall, many forces may together influence birth outcomes for different socio-economic groups. Tobacco consumption is the one studied here as it is the most important determinants of poor birth outcomes in Western Societies (Kramer et al., 2000).
Data and variables
Data
To investigate the association between social background and BW, I draw on three large-scale longitudinal UK cohort studies: the 1958 National Child Development Study (NCDS), the 1970 British Cohort (B70), and the 2001 Millennium Cohort Study (MCS), which all have the newborn as unit of analysis. From each of these cohort studies, I use the first wave. In the analyses, there are three sample restriction criteria. First, I restrict the sample to those who have a UK or in European ethnic origin to maintain homogeneity of the sample, as the ethnic composition across the three cohorts varies considerablyFootnote 2 making comparison across time difficult. Furthermore, ethnic origin overlaps with social background and maternal behaviors (Fertig, 2010),Footnote 3 and another study has already investigated class differences in birth weight between ethnically European and various non-European groups with the MCS data (Kelly et al., 2008). Second, I also examine only singleton births, as fetal development varies significantly between singleton and multiple deliveries. Furthermore, the share of multiple births has changed over time, increasing the share of small deliveries (Moser et al., 2003). Third, I exclude births without complete information.Footnote 4 The final analytical sample consists of 45,671 births.
The NCDS is a large-scale longitudinal study that consists of a representative sample of children born in the United Kingdom in the week commencing March 3, 1958. The first wave was completed by midwives who attended the delivery. The final analytical sample consists of 15,500 births. The B70 design resembles the one of the NCDS, and it includes children born in the week commencing April 5th, 1970. The final analytical sample includes 15,552 births. Differently from the previous two cohorts, the MCS is a sample of children born in the 12 months following September 2000. The respondent of the MCS was mainly the biological mother. Since MCS has a complex sampling design, analyses adopt sampling weights. The final analytical sample consists of 14,619 births.
Dependent variable
The main outcome variable in this article is birth weight. I operationalize it both as a metric variable in grams, and as a binary variable for low birth weight (birth smaller than < 2500 g; LBW). Birth weight and LBW are good predictors of fetal environment, fetal health impairments, and developmental potential (Hernández-Alava & Popli, 2017; Torche & Conley, 2016).
As outlined in the data section, birth information, including birth weight, is reported by midwives attending the delivery in the NCDS and B70 cohorts, whereas the respondent was the mother in the last cohort. Despite this difference, data on birth weight in the MCS is mostly consistent with the hospital records (Goisis et al., 2018; Tate et al., 2005).
Socio-economic background
I use a binary measure of low and high maternal education as a proxy for social background. In the NCDS and B70, maternal education is considered low if the mother has attained less than compulsory education. In the MCS, low maternal education is considered if she has less than a university degree. These categorizations allow to consistently identify as high educated about the top 30% of the education distribution across the three cohorts and to compare it to the rest of the distribution, which is identified as low. Since between 1958 and 2001, the UK has experienced a large educational expansion that has led to changes in the educational distribution over time (Breen, 2010; Goldthorpe, 2016), operationalizing maternal education by identifying about the top 30% of the educational distributions allows to address structural changes in the educational distribution across the cohorts, and thus should ensure comparability across the three cohorts. Moreover, in this way I am able to always identify a similar share of individuals at the top of the educational distribution, comparing across the cohorts those at the top against those at the bottom. This approach is similar to that of considering educational as a positional good (Triventi et al., 2016). Moreover, beyond the advantage in comparability, among the possible measures of social background (i.e., social class, income, prestige scores), I use maternal education because it is considered as one of the most important predictors of maternal smoking (Härkönen et al., 2018). Finally, in Fig. 2 in the appendix I also report a sensitivity analysis using the highest parental social class among the parents (managers vs. manual workers) and results are consistent. Similarly, by controlling for maternal occupational status results do not change (results available upon request).
Prenatal maternal smoking in pregnancy
Smoking during pregnancy is a binary variable having value one when a mother did not stop smoking during pregnancy. In the NCSD and MCS cohorts, mothers are considered to have smoked during pregnancy if they continued smoking after the fourth month of pregnancy. For the B70, it is possible to distinguish only whether a mother continued smoking after the fifth month of pregnancy. The distribution of smoking during pregnancy across the three cohorts is consistent with previous studies (Fertig, 2010; Goisis et al., 2018).
Control variables
In the analyses, in order to account for possible confounders and changes in population characteristics across cohorts, I include a set of control variables. (1) Maternal age is included as it is associated with birth outcomes across the three cohorts (Goisis et al., 2018), and the average age at birth varies considerably over time (Maher & Macfarlane, 2004); it is discrete and operationalized in five age categories: < 19; 20–29; 30–39; 40 + . (2) I include maternal height in cm (standardized within each cohort in the analyses), as a proxy for maternal health.Footnote 5 (3) The sex of the newborn. (4) Maternal marital status at birth. (5) Birth order as a categorical variable: first born, second born, third + born. (6) Timing of the first visit to antenatal care: before the 12th week of gestation; 12th–23rd; 23rd + ; no visit.
Analytical strategy
Cohort comparison
To investigate how the association between SES and birth outcomes changed over time, I use a combination of linear and logistic regression models, depending on whether the outcome is binary or metric. I define and describe here the basic structure of the logistic and linear regression models, which are computed separately for each one of the three cohorts:
where \({Y}_{i}\) indicates the outcome variables: birth weight measured in grams or the probability of delivering a LBW child i. \(\beta 1\left({\mathrm{SES}}_{i}\right)\) is the binary variable for high- versus low-educated mothers; and \(\left({\mathrm{Controls}}_{I}\right){\varvec{\delta}}\) is the array of control variables specified in the section above.
SES differences in birth outcomes: the mediating effect of maternal smoking
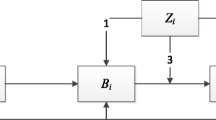
To estimate the mediation effects, I adopt the strategy outlined by causal mediation analyses literature (VanderWeele, 2015), and its applied empirical strategy (see Hicks & Tingley, 2011 for a description of the estimation strategy and the estimation algorithm). Using this framework has several advantages. First it allows to estimate mediation effects for any kind of outcomes and functional forms. Second, it provides a clear estimate of the mediation effect as the average effect of the mediator at fixed level of the independent variable of interest, in this case maternal education. In other words, how much of the effect of maternal education on birth outcomes is due to smoking. Third, it provides tools for sensitivity analyses of the mediation effect. Fourth, it provides uncertainty estimates of the mediation effect. In the results below, I will thus report the mediation effect both as the quantity of the effect of maternal education mediated by smoking and as the share of the effect in maternal education which is mediated by maternal smoking.
Results
Descriptive results
Table 1 describes the variables used in the analyses for each of the three cohorts. Birth outcomes generally improved across the three cohorts. The average birth weight in grams remained similar in the first two cohorts, being of about 3300 g, whereas it increased to about 3400 g in the MCS. The share of LBW children decreased from 7.23% of all births in the 1958 cohort to 5.46% in the youngest cohort in the 2001. The independent variable SES refers to the level of education of the mother, as described in the variable section above. The share of high-educated mothers slightly increases across the three cohorts, from about a quarter of cases in the 1958 cohort, to about 33% in the 1970 and in the 2001 cohort. The share of mothers that smoked during pregnancy, on the other hand, changed notably across the three cohorts. One out of three mothers smoked after their fourth month of pregnancy in the 1958; more than 40% of mothers smoked after the fifth month in the 1970; but in the 2001, the share of smoking mothers decreased and only 1 out of 5 smoked after the fourth month of pregnancy.
For the other variables, it can be noticed an increase in the average age of the mothers: the share of women giving birth between 20 to 29 years decreased 20 percentage points from 1958 to 2001, whereas the share of mothers giving birth between 30 and 39 years increased from about 31% in the NCDS to 51% in the 2001 cohort; a 20 percentage points increase. An even more pronounced change happened for marital status. In the 1958 cohort almost every woman was married at the time of birth, whereas only half were married in the 2001 cohort. The share of cohort members being first child (compared to other birth orders) slightly increased across the three cohorts: the share was about 37% in the 1958 and 1970, increasing to 40% in the 2001. A greater change happened among those who were the third or subsequent child of a mother: they decreased from 31% in the 1958 cohort to only about 20% in the 2001 cohort. Finally, mothers have become more attentive to prenatal care, and accessed this service at earlier stages of the gestation across the three cohorts: if only 20% of women were doing their first visit before the 12th week in the 1968 cohort, more than 40% accessed the care early in the 2001 cohort.
Figure 1 displays the percentage of mothers that smoked during pregnancy across the three cohorts by their educational level. The bars report the share of smokers across the educational categories and the three cohorts. Across the three cohorts, it is possible to notice that there is a relationship between smoking during pregnancy and maternal education, as low-educated mothers were consistently more likely to smoke in respect to their high educated counterpart. However, this relationship changed over time. In the 1958 and 1970 cohort, a sizeable proportion of both high- and low-educated mothers smoked, although a difference of 13 percentage points in 1958 and 19 percentage points in 1970 existed between high- and low-educated mothers. The largest change in smoking habits happened among the 2001 cohort. Both educational groups reduced smoking during pregnancy, but the decrease was more pronounced among highly educated mothers: only less than 1 in every 10 women smoked during pregnancy. To sum up, educational differences persisted across the three cohorts, but in the most recent cohort highly educated mothers almost completely quit smoking during pregnancy.

(Source: NCDS; B70; MCS. First waves. Own elaboration)
Smoking during pregnancy by maternal education across the three cohorts
Maternal education & birth outcomes across three cohorts
Table 2 shows the results of six regression models estimating the effect of maternal SES on birth weight (measured in grams) and LBW across the three cohorts. In Panel A, coefficients in the table report the average difference between high- and low-educated in birth weight. Coefficients in Panel B show the difference in odds ratios between high- and low-educated mothers in the chance of delivering a LBW child. Standard errors are in brackets.
Overall, Table 2 shows an association between maternal education and birth outcomes across the three cohorts analyzed (P < 0.05), with low SES children having worst birth outcomes than children born from high SES mothers. Model 1 in Panel A shows a difference of about 54 g between high- and low-educated mothers in the 1958s cohort. Model 2 in Panel A reports the same coefficient for the 1970 cohort, predicting a difference of about 46 g between high- and low-educated mothers. In addition, in Model 3, the result for the most recent cohort displays a difference in birth weight between high- and low-educated mothers of about 59 g. In Panel B, where the outcome is whether a child is born with LBW, we find a similar pattern. Model 1, for the 1958 cohort, shows an increase of about 47% in the chances of low-educated mothers in delivering an LBW child with respect to their high-educated counterparts (2.4 percentage points). In the 1970 this difference is about 26% (1.4 percentage points). In the youngest 2001 cohort, the relative difference is about a 45% increase (1.77 percentage points).
I also compare these effects with results found in previous research on birth outcomes (Bernardi et al., 2016). Difference of about 50 g in birth weight are generally similar to the effect found in programs aimed to enhance birth weight (Bitler & Currie, 2005; Torche, 2011) or in relation to the exposure to heavy pollutants (Currie & Schwandt, 2015). An increase of about 2 percentage points in LBW is generally higher than the effects found in the case of an exposure to a violent earthquake (about 1.5 percentage points) (Torche, 2011), an upset victory in the Super Bowl (0.4 percentage points), or pollutants (0.76 percentage points) (Currie & Schwandt, 2015; Duncan et al., 2017).
Mediation analyses: the role of maternal smoking
Table 3 reports the mediating effect of maternal smoking during pregnancy across the three birth cohorts. The estimates reflect the quantity and the share of the effect of maternal education accounted by smoking in pregnancy. Panel A shows the mediating effects on birth weight measured in grams. Panel B reports the mediating effects on LBW. Confidence intervals of the estimates are reported in brackets. All the mediation effects reported in the table are statistically significant.
In both Panel A and Panel B, it is possible to notice that the relevance of the effect of maternal smoking behaviors changed across the three cohorts for both outcomes. Maternal smoking accounted for about 35% of birth weight reduction and 16% LBW increase among the 1958 cohort. Among the following cohorts, the influence of maternal smoking became substantially larger. It accounted for 65% and 60% of the effect on birth weight in the 1970 and 2001 cohort, respectively. Similarly, the share of the effect mediated by smoking increased also for LBW, from 16% in the 1958 cohort, to about 46% in the 1970 and 2001 cohorts. These results highlight the fact that maternal behaviors such as smoking have become important in explaining educational differences in birth outcomes only among the more recent cohorts, whereas other factors may have been at play in before.
Sensitivity and secondary analyses
In this section, I provide a sensitivity analysis for the mediation effects I estimated and two secondary analyses. The mediation effects estimated in these analyses are valid under the assumption that no other confounders affect the mediator outcome relationship. However, even when controlling for a large set of covariates, the sequential ignorability assumption is seldomly respected. This risks to be especially true when comparing three different cohorts with only a limited set of comparable control and maternal behaviors variables.
Here, I provide sensitivity analyses for the mediating effect of maternal smoking in pregnancy on birth weight in grams (Keele et al., 2015). This sensitivity analysis simulates a confounder factor correlated with error terms in both the mediator and outcome equations and re-estimates the mediation effect for various level of correlation (ρ) among the error terms. Here, to consider reliable the estimated mediation effect we would expect that small variations in ρ would not be associated with large changes in the mediation effect.Footnote 6 Figure 2 in the appendix reports the results of a sensitivity analysis. The x-axis reports the simulated correlation (ρ) between the error terms in mediator and outcome equations, and the y-axis displays the value the mediation effect would take at different levels of (ρ). Across the three cohorts, the results of the sensitivity analyses point towards the conclusion that the estimated mediation effect is less sensitive to unobserved confounders in the 2001 cohort with respect to previous cohorts (ρ = − 0.3 in 2001; ρ = − 0.2 in 1958 and 1970), as it requires the highest correlations between the error terms to both reduce the effect to zero or double it in size. Across the three cohorts, maternal smoking in pregnancy seems to be a more robust mediator in the relationship between maternal socio-economic status and birth outcomes in the 2001 cohort.
I further performed two secondary analyses to better understand the role of improvement in antenatal care and of MAR for inequalities in birth outcomes. First, perinatal medical technologies have improved drastically in the last 50 years, boosting birth outcomes and increasing fetal survival (Goisis et al., 2017a, 2017b). This increase in survival may have led to an increase share of rescued “frail” births (Fertig, 2010). In other words, medical technological advancements “rescue” frail fetuses that would have ended up in miscarriages. I investigated this scenario using the share of very low birth weight children (VLBW—born smaller than 1500 g) as a proxy for weak fetuses surviving gestation. I find that VLBW deliveries remained almost constant among the high-SES: about 0.5% across the three cohorts; and VLBW deliveries decreased for low-SES from about 1.1% in the 1958 to about 0.7% in 2001. If medical advancements impacted birth outcomes inequalities, they may have contributed in reducing them, as the number of very frail births slightly decreased for the low SES.
Second, another possible explanation to the persistence of inequalities across cohorts may be that the composition of live-births among highly educated has changed due to the increased number of MAR-conceived children. Since MAR children are both more likely to be born from high SES parents and are more likely to have poor birth outcomes, their conceptions may have stagnated birth outcomes among the high SES: I re-estimated Eq. (1) for the MCS (the cohort where MAR may play a role), including a control for whether the child is MAR born. Results are identical and reported in Table A3. This suggests that MAR did not contribute in mantaining inequalities constant.
Conclusions and discussion
In this article, I investigated the association between socioeconomic status measured as maternal education and birth outcomes across three British cohorts. I further investigated how maternal smoking behaviors during pregnancy accounted for this association. There are two main findings in this article. First, the difference in birth weight and in the probability of LBW between high- and low-educated mothers is non-trivial, and it persists across the three cohorts with values similar to those found by causal literature on the effect of exogenous shocks on birth outcomes. This result holds also when SES is measured as the highest social class among the parents. I further investigated the role of MAR and medical advancement in accounting for these trends and they did not seem to play a large role in explaining the persistence of these differentials.
The second main finding of this article is that the amount maternal smoking accounts for the SES gradient in LBW varies notably across the three cohorts, highlighting the fact that underlying causes of these disparities may have changed across time. An explanation for the change in the relevance of maternal smoking across the three cohorts may be that also among mothers smoking followed the stages of tobacco epidemic. Prenatal maternal smoking was more evenly distributed among socioeconomic strata in 1958, and it became a behavior mainly concentrated among low-SES among the 1970 and 2001 cohorts, following the stage of the tobacco epidemic (Khlat et al., 2016; Lopez et al., 1994), as also Fig. 1 seems to suggest. What may have contributed to SES disparities in the 1958 cohort remains an open question. In this regard, I investigated (analyses not shown) whether quality and quantity to access prenatal care played a role in explaining educational differences in 1958, but I did not find any evidence. It may be thus possible that material conditions such as maternal nutrition and working conditions may have played a predominant role in shaping SES differences in birth outcomes.
Taken together, the two main results of this study suggest that the constant levels in inequalities in birth outcomes may reflect many processes that evolved across these four decades, many of which may be at play together and in opposite directions, as I argued in the background section. In fact, despite smoking in pregnancy become more stratified and consequently a more important determinant of inequalities, it did not imply a change in levels of the trends of inequalities overall. Further research should examine how the evolution of different—often contradictory—phenomena contributed to shape levels of inequalities in birth outcomes.
This work is not free of caveats. I have only a limited number of comparable covariates to use across the three cohorts, reducing the number of possible confounders I can control for. Second, following from the previous limitation, I can only account for one maternal behavior during pregnancy, and consequently the estimates of the mediation effect are likely to be biased upwards. However, maternal smoking during pregnancy is likely to be positively correlated with other health behaviors (Pampel et al., 2010), and consequently it could be considered as a proxy for unhealthy behaviors. Third, I decided to approach the comparability of the SES measure using a relative measure of education. This is only one of the possible approaches to make this measure comparable across cohort, also accounting for large changes in the composition of highly educated women over time.
This study corroborates the idea that together with better-known inequality in health, morbidity and mortality in the adult population (Mackenbach, 2012; Mackenbach et al., 2008), also disparities in birth outcomes exist. These inequalities, and their persistence across these three cohorts, also imply that children from lower SES consistently started with a disadvantage at the very beginning of life for over 40 years, and this may have contributed to the reproduction of observed disparities in health and socioeconomic success across childhood and adulthood (Skopek & Passaretta, 2020). Moreover, in the 1970 and 2001 cohorts, disparities in birth outcomes are most likely determined by preventable factors, such as maternal smoking and behaviors.
Availability of data and materials
Data are available under reasonable request to the corresponding author.
Notes
The reasons why low-SES individuals engage more in unhealthy behaviors remain somehow debated (Pampel et al., 2010), but there is some evidence that exposure to harsh life conditions, stress, peer-influence, and lack of medical knowledge may play a role in generating SES disparities in health behaviors (Cutler & Lleras-Muney, 2010).
Among observation with valid information for all the variable used in the analyses, non-European-origin individuals are: 1.2% in the NCDS (N = 188); 4.72% in the B70 (N = 771); 12.47% in the MCS (2,883).
I also computed the analysis for non-EU individuals in the MCS cohort (given the larger sample size), and the results are different. Maternal smoking during pregnancy does not play any role in explaining these differences. Results are available in the Appendix, Table 4.
Table 5 in the appendix report the distributions of the variables used for the cases having missing information in BW. The share of missing cases for birth weight is higher in the NCDS, where they are about 9,75% of the sample (N = 1776). In the B70 and MCS the cases are a few, being the 0.18% (N = 31) and the 0.36% (N = 65) respectively. Moreover, when Table 5 in the appendix and Table 1 are compared, no major systematic differences are found.
This is unfortunately not the best proxy for maternal health status, but a better proxy as body mass index was not computable in all the three cohorts, as the B70 did not report maternal weight.
References
Aizer, A., & Currie, J. (2014). The intergenerational transmission of inequality: maternal disadvantage and health at birth. Science, 344(6186), 856–861.
Aizer, A., Stroud, L., & Buka, S. (2016). Maternal stress and child outcomes evidence from siblings. Journal of Human Resources, 51(3), 523–555. https://doi.org/10.3368/jhr.51.3.0914-6664R
Almond, D., & Mazumder, B. (2013). Fetal origins and parental responses. In K. J. Arrow & T. F. Bresnahan (Eds.), Annual review of economics (Vol. 5, pp. 37–56). Annual Reviews.
Arntzen, A., Samuelsen, S. O., Bakketeig, L. S., & Stoltenberg, C. (2004). Socioeconomic status and risk of infant death. A population-based study of trends in Norway, 1967–1998. International Journal of Epidemiology, 33(2), 279–288.
Bernardi, F., Chakhaia, L., & Leopold, L. (2016). ‘Sing Me a Song with Social Significance’: The (Mis) use of statistical significance testing in european sociological research. European Sociological Review. https://doi.org/10.1093/esr/jcw047
Bitler, M. P., & Currie, J. (2005). Does WIC work? The effects of WIC on pregnancy and birth outcomes. Journal of Policy Analysis and Management: THe Journal of the Association for Public Policy Analysis and Management, 24(1), 73–91.
Bonellie, S. R., & Raab, G. M. (1997). Why are babies getting heavier? Comparison of Scottish births from 1980 to 1992. BMJ, 315(7117), 1205.
Breen, R. (2010). Educational expansion and social mobility in the 20th century. Social Forces, 89(2), 365–388.
Christensen, K., Doblhammer, G., Rau, R., & Vaupel, J. W. (2009). Ageing populations: The challenges ahead. The Lancet, 374(9696), 1196–1208.
Conte Keivabu, R., & Cozzani, M. (2022). Extreme heat, birth outcomes, and socioeconomic heterogeneity. Demography, 59(5), 1631–1654.
Cozzani, M., Aradhya, S., & Goisis, A. (2021a). The cognitive development from childhood to adolescence of low birthweight children born after medically assisted reproduction—a UK longitudinal cohort study. International Journal of Epidemiology, 50(5), 1514–1523.
Cozzani, M., Triventi, M., & Bernardi, F. (2021b). Maternal stress and pregnancy outcomes evidence from a natural experiment: The 2004 Madrid train bombings. European Sociological Review. https://doi.org/10.1093/esr/jcab045
Currie, J. (2011). Inequality at birth: some causes and consequences. American Economic Review, 101(3), 1–22. https://doi.org/10.1257/aer.101.3.1
Currie, J., & Schwandt, H. (2015). The 9/11 dust cloud and pregnancy outcomes: A reconsideration. Journal of Human Resources., 51(4), 805–831.
Cutler, D. M., & Lleras-Muney, A. (2010). Understanding differences in health behaviors by education. Journal of Health Economics, 29(1), 1–28.
de Graaf, J. P., Steegers, E. A., & Bonsel, G. J. (2013). Inequalities in perinatal and maternal health. Current Opinion in Obstetrics and Gynecology, 25(2), 98–108.
Diouf, I., Charles, M. A., Blondel, B., Heude, B., & Kaminski, M. (2011). Discordant time trends in maternal body size and offspring birthweight of term deliveries in France between 1972 and 2003: Data from the French National Perinatal Surveys. Paediatric and Perinatal Epidemiology, 25(3), 210–217.
Donahue, S. M., Kleinman, K. P., Gillman, M. W., & Oken, E. (2010). Trends in birth weight and gestational length among singleton term births in the United States: 1990–2005. Obstetrics and Gynecology, 115(2 Pt 1), 357.
Duncan, B., Mansour, H., & Rees, D. I. (2017). It’s just a game the super bowl and low birth weight. Journal of Human Resources, 52(4), 946–978.
Fairley, L., & Leyland, A. (2006). Social class inequalities in perinatal outcomes: Scotland 1980–2000. Journal of Epidemiology & Community Health, 60(1), 31–36.
Fertig, A. R. (2010). Selection and the effect of prenatal smoking. Health Economics, 19(2), 209–226.
Frejka, T., & Sardon, J.-P. (2006). First birth trends in developed countries: Persisting parenthood postponement. Demographic Research, 15, 147–180.
Ghosh, R. E., Berild, J. D., Sterrantino, A. F., Toledano, M. B., & Hansell, A. L. (2018). Birth weight trends in England and Wales (1986–2012): Babies are getting heavier. Archives of Disease in Childhood Fetal and Neonatal Edition, 103(3), F264–F270. https://doi.org/10.1136/archdischild-2016-311790
Goisis, A., Fallesen, P., Seiz, M., Salazar, L., Eremenko, T., & Cozzani, M. (2023). Educational gradients in the prevalence of Medically Assisted Reproduction (MAR) births in a comparative perspective, European Commission, JRC132792.
Goisis, A., Håberg, S. E., Hanevik, H. I., Magnus, M. C., & Kravdal, Ø. (2020). The demographics of assisted reproductive technology births in a Nordic country. Human Reproduction, 35(6), 1441–1450. https://doi.org/10.1093/humrep/deaa055
Goisis, A., Özcan, B., & Myrskylä, M. (2017a). Decline in the negative association between low birth weight and cognitive ability. Proceedings of the National Academy of Sciences, 114(1), 84–88.
Goisis, A., Remes, H., Barclay, K., Martikainen, P., & Myrskylä, M. (2017b). Advanced maternal age and the risk of low birth weight and preterm delivery: A within-family analysis using Finnish population registers. American Journal of Epidemiology, 186(11), 1219–1226.
Goisis, A., Schneider, D. C., & Myrskylä, M. (2018). Secular changes in the association between advanced maternal age and the risk of low birth weight: a cross-cohort comparison in the UK. Population Studies, 72(3), 381–397. https://doi.org/10.1080/00324728.2018.1442584
Goldstein, J. R., Sobotka, T., & Jasilioniene, A. (2009). The end of “lowest-low” fertility? Population and Development Review, 35(4), 663–699.
Goldthorpe, J. H. (2016). Social class mobility in modern Britain: changing structure, constant process. Journal of the British Academy. https://doi.org/10.5871/jba/004.089
Härkönen, J., Kaymakçalan, H., Mäki, P., & Taanila, A. (2012). Prenatal health, educational attainment, and intergenerational inequality: The Northern Finland Birth Cohort 1966 Study. Demography, 49(2), 525–552.
Härkönen, J., Lindberg, M., Karlsson, L., Karlsson, H., & Scheinin, N. M. (2018). Education is the strongest socioeconomic predictor of smoking in pregnancy. Addiction. https://doi.org/10.1111/add.14158
Heckman, J. J. (2007). The economics, technology, and neuroscience of human capability formation. Proceedings of the National Academy of Sciences of the United States of America, 104(33), 13250–13255. https://doi.org/10.1073/pnas.0701362104
Hernández-Alava, M., & Popli, G. (2017). Children’s development and parental input: Evidence from the UK Millennium cohort study. Demography, 54(2), 485–511. https://doi.org/10.1007/s13524-017-0554-6
Hicks, R., & Tingley, D. (2011). Causal mediation analysis. The Stata Journal, 11(4), 605–619.
Jalovaara, M., Neyer, G., Andersson, G., Dahlberg, J., Dommermuth, L., Fallesen, P., & Lappegård, T. (2019). Education, gender, and cohort fertility in the Nordic countries. European Journal of Population, 35(3), 563–586.
Keele, L., Tingley, D., & Yamamoto, T. (2015). Identifying mechanisms behind policy interventions via causal mediation analysis. Journal of Policy Analysis and Management, 34(4), 937–963.
Kelly, Y., Panico, L., Bartley, M., Marmot, M., Nazroo, J., & Sacker, A. (2008). Why does birthweight vary among ethnic groups in the UK? Findings from the Millennium Cohort Study. Journal of Public Health, 31(1), 131–137.
Khlat, M., Pampel, F., Bricard, D., & Legleye, S. (2016). Disadvantaged social groups and the cigarette epidemic: Limits of the diffusion of innovations vision. International Journal of Environmental Research and Public Health, 13(12), 1230.
Kramer, M. S., Séguin, L., Lydon, J., & Goulet, L. (2000). Socio-economic disparities in pregnancy outcome: Why do the poor fare so poorly? Paediatric and Perinatal Epidemiology, 14(3), 194–210.
Link, B. G., & Phelan, J. (1995). Social conditions as fundamental causes of disease. Journal of Health and Social Behavior, 35, 80–94. https://doi.org/10.2307/2626958
Lopez, A. D., Collishaw, N. E., & Piha, T. (1994). A descriptive model of the cigarette epidemic in developed countries. Tobacco Control, 3(3), 242.
Mackenbach, J. P. (2012). The persistence of health inequalities in modern welfare states: The explanation of a paradox. Social Science & Medicine, 75(4), 761–769. https://doi.org/10.1016/j.socscimed.2012.02.031
Mackenbach, J. P., Stirbu, I., Roskam, A. J. R., Schaap, M. M., Menvielle, G., Leinsalu, M., European Union Working Group on Socioeconomic Inequalities in Health. (2008). Socioeconomic inequalities in health in 22 European countries. New England Journal of Medicine, 358(23), 2468–2481. https://doi.org/10.1056/NEJMsa0707519
Maher, J., & Macfarlane, A. (2004). Trends in live births and birthweight by social class, marital status and mother’s age, 1976–2000. Health Statistics Quarterly, 23, 34–43.
Masters, R. K., Link, B. G., & Phelan, J. C. (2015). Trends in education gradients of ‘preventable’mortality: A test of fundamental cause theory. Social Science & Medicine, 127, 19–28.
Moser, K., Li, L., & Power, C. (2003). Social inequalities in low birth weight in England and Wales: Trends and implications for future population health. Journal of Epidemiology & Community Health, 57(9), 687–691.
Pampel, F. C. (2005). Diffusion, cohort change, and social patterns of smoking. Social Science Research, 34(1), 117–139.
Pampel, F. C., Krueger, P. M., & Denney, J. T. (2010). Socioeconomic disparities in health behaviors. Annual Review of Sociology, 36, 349.
Persson, P., & Rossin-Slater, M. (2018). Family ruptures, stress, and the mental health of the next generation. American Economic Review, 108(4–5), 1214–1252.
Pison, G., Monden, C., & Smits, J. (2015). Twinning rates in developed countries: Trends and explanations. Population and Development Review, 41(4), 629–649.
Power, C. (1994). National trends in birth weight: Implications for future adult disease. BMJ, 308(6939), 1270–1271.
Rogers, J. M. (2009). Tobacco and pregnancy. Reproductive Toxicology, 28(2), 152–160.
Schiessl, B., Beyerlein, A., Lack, N., & von Kries, R. (2009). Temporal trends in pregnancy weight gain and birth weight in Bavaria 2000–2007: Slightly decreasing birth weight with increasing weight gain in pregnancy. Journal of Perinatal Medicine, 37(4), 374–379.
Schneider, E. B. (2017). Fetal health stagnation: Have health conditions in utero improved in the United States and Western and Northern Europe over the past 150 years? Social Science & Medicine, 179, 18–26.
Skopek, J., & Passaretta, G. (2020). Socioeconomic inequality in children’s achievement from infancy to adolescence: The case of Germany. Social Forces. https://doi.org/10.1093/sf/soaa093
Slama, R., Darrow, L., Parker, J., Woodruff, T., Strickland, M., Nieuwenhuijsen, M., & Hurley, F. (2008). Atmospheric pollution and human reproduction: report of the Munich International Workshop. Environmental Health Perspectives, 116(6), 791–798.
Tate, A. R., Dezateux, C., Cole, T. J., & Davidson, L. (2005). Factors affecting a mother’s recall of her baby’s birth weight. International Journal of Epidemiology, 34(3), 688–695.
Tattarini, G., Grotti, R., & Scherer, S. (2018). The buffering role of the family in the relationship between job loss and self-perceived health: Longitudinal results from Europe, 2004–2011. Health & Place, 52, 55–61.
Thun, M., Peto, R., Boreham, J., & Lopez, A. D. (2012). Stages of the cigarette epidemic on entering its second century. Tobacco Control, 21(2), 96–101.
Torche, F. (2011). The effect of maternal stress on birth outcomes: Exploiting a natural experiment. Demography, 48(4), 1473–1491.
Torche, F., & Conley, D. (2016). A pound of flesh: The use of birthweight as a measure of human capital endowment in economics research. In J. Komlos & I. Kelly (Eds.), The Oxford handbook of economics and human biology. Oxford University Press.
Triventi, M., Panichella, N., Ballarino, G., Barone, C., & Bernardi, F. (2016). Education as a positional good: Implications for social inequalities in educational attainment in Italy. Research in Social Stratification and Mobility, 43, 39–52.
Turner, R. J., & Avison, W. R. (2003). Status variations in stress exposure: Implications for the interpretation of research on race, socioeconomic status, and gender. Journal of Health and Social Behavior, 44, 488–505.
VanderWeele, T. (2015). Explanation in causal inference: methods for mediation and interaction. Oxford University Press.
Ward, W. P. (2015). Birth weight as an indicator of human welfare. In J. Komlos & I. Kelly (Eds.), The Oxford handbook of economics and human biology. New York, NY: Oxford University Press. https://doi.org/10.1093/oxfordhb/9780199389292.013.33.
Acknowledgements
I am grateful to the editor and the anonymous reviewers for their constructive feedback on this manuscript. I am also thankful to Fabrizio Bernardi, Alice Goisis, Juho Härkönen, and the participants of IWG and FLOPS at EUI for providing feedback on a previous version of the manuscript.
Funding
This work was supported by the Italian Ministry of University and Research under the 2017 MiUR-PRIN Grant Prot. N. 2017W5B55Y (“The Great Demographic Recession”, PI: Daniele Vignoli, CUP: B14I19000910001).
Author information
Authors and Affiliations
Contributions
The author read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The author declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
See Tables 4, 5, 6 and Figs. 2, 3

Class differences in birth outcomes. This graph is computed by estimating Eq. 1 using a measure of parental class (the highest social class among the father and the mother). The point estimates report the difference in birth outcomes for manual occupations compared to manager (the reference line). BO birth outcomes

Sensitivity analyses for the mediation effect of maternal smoking in pregnancy for each cohort. The graph reports the correlation between the error terms in the mediator (Eq. 4) and outcome models (Eq. 5) and the NIE. Dashed line is the estimated NIE. Estimates obtained with 500 simulations
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cozzani, M. Inequalities at birth: stable socioeconomic differences in birth outcomes in three British cohorts. Genus 79, 18 (2023). https://doi.org/10.1186/s41118-023-00191-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41118-023-00191-z