
Abstract
Background
The objectives of the study were to describe caffeine intake by 10 years of age or older Brazilian individuals and to investigate possible associations with demographic and socioeconomic determinants as well as the major dietary sources.
Methods
The data used are from the personal food consumption module (n = 34,003) of a country-representative household budget survey. Consumed foods and beverages were identified during the application of food diaries. Caffeine contents in food and beverage sources were obtained primarily in national publications. Multivariate regressions were calculated to assess the correlations between population factors and caffeine intake.
Results
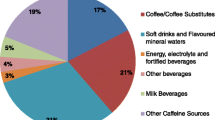
The daily intake per person was estimated as 115.7 mg, ranging from 84.7 mg, for 10–13 years of age children and adolescents, to 139.8 mg, for individuals with no education. The percentage of individuals whom diet reveals daily caffeine intake higher than 400 mg is up to 3.0 %, according to age groups. Males and individuals living in the Northeast or South regions or in the states of Minas Gerais, Rio de Janeiro, and Espírito Santo are likely to ingest higher contents of the substance. The major dietary sources are coffee (63.1 %) and coffee with milk (24.9 %), cola soft drinks (3.6 %) and yerba mate (1.9 %).
Conclusions
Caffeine intake in Brazil is below the recommended limit reference value for adults, and the percentage of individuals whom diet reveals excessive content of caffeine is low. Thus, excessive caffeine intake may not be a health issue in Brazil and depends on the domicile and gender. The major source in the Brazilian diet is coffee.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Caffeine (1,3,7-trimethyl-xanthine) is a substance widely consumed throughout the world. This compound is found in coffee beans (Coffea arabica and Coffea robusta), cocoa beans (Theobroma cacao), cola nuts (Cola acuminata), tea leaves (Camellia sinensis), yerba mate (Ilex paraguariensis), and in prepared or manufactured foods made with these plants [1]. Coffee, for example, is the most often referred beverage by the Brazilian population regarding consumption [2].
Caffeine is a xanthine alkaloid, which can be found in foods such as a naturally derived or synthetic molecule [3]. Being ingested and absorbed into the body, it competes with adenosine for binding to receptors found in the cerebral cortex, peripheral blood circulation, kidney, heart, gastrointestinal tract, and respiratory system [4]. Instead of acting as an inhibitor and depressive agent as adenosine, caffeine has a stimulatory effect that is related to an increase of blood circulation (acute blood pressure increase) and respiratory activity, hydrochloric acid secretion in the stomach, and possibly, an increase of alert ability as well as psychomotor speed [5, 6]. However, the short half-life, which generally ranges from 5 to 8 h, combined with high intakes may produce anxiety, poor quality sleep, headache, and nausea [7–11].
There is evidence that moderate daily coffee consumption, providing 300–400 mg of caffeine, may be associated with preventing chronic diseases such as type II diabetes, Parkinson’s disease, and cirrhosis in healthy adults [12]. The daily intake of up to 400 mg of caffeine provided by coffee is recommended for adults in Canada [13] and in the USA, since it is within other healthful behaviors [14]. There is not enough evidence for association with an increase of risk of cardiovascular diseases in adults [15] or osteoporosis in elderly people [5]. However, adverse effects related to excessive intakes have been reported in specific population groups, such as inducing miscarriage in pregnant women and limitation on fetus development [5, 12]. The estimated fatal dose for adults is 170 mg per kg of body weight, which corresponds to 11.9 g for an individual with 70 kg [16]. Death cases due to overdose are rare [5].
Despite the widespread consumption of foods and beverages containing caffeine, no studies involving a Brazilian nationally representative sample regarding this alkaloid intake or its determinants were identified. The objectives of this study were to estimate caffeine intake by 10 years of age or older individuals in Brazil and to investigate the association with demographic and socioeconomic determinants. Another objective was to identify the major dietary sources.
Methods
Personal food consumption module
Data from the personal food consumption module (PFCM) of a household budget survey (HBS), conducted by the Brazilian Institute of Geography and Statistics (IBGE), were used. Between May 19 2008 and May 18 2009, 13,569 domiciles (24.1 % of the HBS sample) all over the country and representative of all social and demographic strata were visited [17]. The PFCM sample includes only 10 years of age or older individuals, totalizing 34,003 [18], which corresponds to 160,511,094 people, due to the expansion factors of the sample provided by the IBGE.
Food consumption data were obtained by the application of food diaries, which considered foods and beverages consumed inside and outside home along 24 h in two nonconsecutive days. The registration instrument was validated within 79 adults (31 males; 20 to 59 years old) from two cities, one in South and another in the Northeast region, by doing a double-marked water method in order to check the total estimated caloric intake of individuals out of the confinement. The average percentage of under reporting was 17 % [18]. A detailed description of the methodology adopted by IBGE, including the preliminary tests and the validation of the dietary records, can be found on the following publications: IBGE [18] and Sichieri et al. [17].
Caffeine database
Food and beverage items recorded during the PFCM implementation, which likely contain caffeine, were previously selected based on the literature [19, 20]. In this step, the following items were excluded: animal origin products, legumes, fruits (except guarana), juices, fruit smoothies (except those containing guarana), leafy vegetables, milk, bakery products (except items containing cocoa products), sugars, sweeteners, fish, soy products, cereals, nuts, sandwiches, pizzas, savory cereal bars, pasta, and meals (except foods containing cocoa products, cappuccino flavor, tea, guarana, or coffee). Thus, the constructed database included 169 food and beverage items.
Caffeine data is not available in national food databases, so a search was conducted at Science Direct (http://www.sciencedirect.com), Scopus (http://www.scopus.com/standard/), Scielo (http://www.scielo.org/php/index.php), and digital libraries of the University of São Paulo (http://dedalus.usp.br/F?RN=498210588), the University of Campinas (http://www.bibliotecadigital.unicamp.br/), and São Paulo State University “Júlio de Mesquita Filho” (http://www2.fc.unesp.br/BibliotecaVirtual/). The keywords used in Portuguese/English were “cafeína/caffeine”, “conteúdo/content”, and “ingestão/intake” along with “Brasil/Brazil”. Only two papers were identified [21, 22] with representative sampling of coffees, teas, chocolate products, and soft drinks. Andrade et al. [21] have used a methodology for high performance liquid chromatography (HPLC) with UV/VIS detector for yerba mate infusions. Camargo [22] have used the same method (HPLC-UV/VIS) in three batches of coffee, teas, chocolate products, and soft drinks available in the market. Caffeine contents in processed foods were obtained in the basis of nutritional data from the United States Department of Agriculture Release 25 [23]. Table 1 shows part of the constructed database.
To the record of mixtures of coffee with milk or flour, the caffeine content in coffee prepared from the ground grains (not instant coffee) was considered, and the amount of coffee was estimated as 50 % [18, 24]. Caffeine contents in food supplements were not considered. The amounts of caffeine were calculated and expressed as milligrams per 100 g or milliliters per 100 ml.
Statistical analysis
Caffeine intake was expressed as average ± standard deviation. Multivariate regressions were calculated to estimate the association between caffeine intake and different independent variables. The variables assessed were age and five binary variables to distinguish six regions (São Paulo was segregated from Minas Gerais, Rio de Janeiro, and Espírito Santo states for being the most populous federal state: 22 % of the country’s population [25]). Also, the following were taken into account: gender: male or female; ethnic group: white, black, brown, or yellow; education as years of study; binaries to nine age groups; and four strata per capita of family income (PCFI). The monetary values were expressed as dollars, converted from the values in Reais of January 15, 2009 [18] (considering conversion values on that day).
Observations with a missing value for any of the variables used in the regression were excluded from the sample, as well as persons with a zero per capita family income. This procedure reduces the sample in 33,453 observations. An α value of 5 % was considered, and all statistical analyses were carried out using the Statistical Analysis System – SAS® program, version 9.3 [26].
Results
The distribution of the population, according to age groups, domicile, ethnic group, education, and PCFI, is shown in Fig. 1.

Distribution of the individuals from the personal food consumption module 2008–2009, according to factors
Women correspond to 53.8 % of the sample. People from the Northeast region are 37.1 %, and adults are 79.6 % of the sample (24.5 % between 19 and 30 years + 32.9 % between 31 and 50 years + 17.4 % between 51 and 70 years, and 4.8 % between 71 years of age and older). About 50 % of the individuals declared themselves as brown and 40.7 % as white. The years of education of 59.5 % are amidst one and nine. More than 50 % of the sample had income between 84.01 and 168.00 dollars (26.6 %) or between 168.01 and 336.00 dollars (27.5 %).
Caffeine intake in Brazil, according to different factors, is shown in Table 2. The analyzed data refer to the first food diary, because it tends to be more reliable [19]. People who only filled in the questionnaire on the second day had this information considered.
Caffeine intake (mean values) in Brazil was 115.7 mg per day, and ranged from 96.6 mg, in the Midwest region, to 127.9 mg, in the Southern region. High caffeine intakes were more likely to be observed in adults 51–70 years of age (129.9 mg) and 31–50 years of age (125.2 mg), men (121.6 mg), individuals with PCFI between 21.01 and 168.00 dollars, and with no education (139.8 mg). Individuals that claimed themselves yellow ingested less caffeine. The frequency of individuals who had daily caffeine intake higher than 400 mg during the implementation of the HBS 2008–2009 is shown in Table 3, according to age groups.
Caffeine daily intake higher than 400 mg was observed in up to 3.0 % of the Brazilian population, according to age groups. Table 4 presents multivariate regressions estimated to assess the association between different population factors with caffeine intake for 10 years of age or older individuals interviewed during the PFCM.
The majority of the determinants analyzed in this study had significant regression coefficients (p < 0.005). Considering the PCFI strata of US$ 168 to US$ 336 as basis for this research, it was verified that caffeine intake is higher among individuals that are relatively poor (US$ 21 < PCFI ≤ US$ 168), and it is low among those who are relatively rich (PCFI >US$ 336). The poorer ones (0 < PCFI ≤ US$ 21) show lower intake, but the difference in relation to the basic category is not statistically significant because it consists of a small strata (1.4 % of the sample).
In terms of age, the range between 10 and 13 years old was adopted as basis in this study. The intake is statistically higher in other age groups. It increases until the age of 41 to 50 years, and later, it tends to decrease.
The intake is substantially higher and statistically significant for males. The “white” was adopted as basis for analyzing the effect of color claimed by these individuals. The “yellow” people, with the lowest intake, are the only ones that show a statistical significant difference. It is relevant to mention that the coefficient of a multiple regression demonstrate the effect of an explanatory variable after having the effects from the other explanatory variables controlled, which were included in the regression equation. Thus, the coefficient (−17.5) for “yellow” individuals is an estimation of the effect that belongs to this category, after having family income, schooling, and the other effects discounted from the variables included in the equation.
The increase of the schooling effect is associated with a reduction on caffeine intake. In regard to the region of living, the Northeast was adopted as basis. Caffeine consumption showed to be statistically low in the North, in São Paulo state, and in the Midwest. On the other hand, it is statistically higher in the South. The intake in Minas Gerais + Espírito Santo + Rio de Janeiro is higher, but it is not statistically significant.
Coffee (63.1 %) was the major dietary source, followed by coffee with milk (24.9 %), cola soft drinks (3.6 %) and yerba mate (1.9 %).
Discussion
The database used is country-representative and, such as other household budget surveys conducted at regular time intervals, provides reliable and representative data based on a sample size large enough to generate statistically relevant information about complex dietary patterns [27]. It also allows the linkage to demographic and socioeconomic factors that may be associated with food consumption and or substance intakes, such as of caffeine.
It is recognized by the authors that this research has limitations due to the used data being referred to a domicile-single food diary only. The values observed in this study are lower than the ones estimated by Camargo [22] in a survey conducted in the city of Campinas, São Paulo state, Brazil. The author reported a daily average intake of 2.74 mg/kg body weight (191.8 mg for a 70-kg person) within a representative sample based on individuals of both genders and aging between 9 and 80 years old (n = 600). To the best of our knowledge, there are no other studies regarding the theme conducted in the country.
The results of the present study are comparable with values obtained from studies conducted in other countries with nationally representative individual food consumption data. In the UK, Fitt et al. [28], using intake data obtained from four non-weighed food diaries and a North American food composition data, observed similar daily values, ranging from 122 mg (women, 19 to 64 years of age) to 143 mg (men, at least 65 years of age). It is worth noting that only individuals who reported consuming foods and beverages that contain caffeine were considered for the analysis. Mitchell et al. [29], exploring data obtained by applying seven consecutive non-weighed food diaries and caffeine content from a national food composition database, estimated the daily intake (mean value) of 165 mg in the USA. Yamada et al. [30], using 16 weighed food records and national food composition data, obtained higher values in Japan for individuals 30–69 years of age: 256.2 mg for men and 268.3 mg for women. High daily intakes of 357 mg were also reported in a research conducted in Austria using a semi-quantitative food frequency questionnaire in individuals of 14 to 39 years of age and national caffeine content data [31]. The mentioned studies, however, adopted different dietary survey techniques and methods, sources of food composition data (national or foreign), and demographic aspects of the sample, which may limit result comparison.
Caffeine intake higher than 400 mg was observed in a little part of the Brazilian population. The value is lower than the one reported for adults in Japan (11 % for women and 15 % for men), where the caffeine intake reported for this age group was also higher [30]. It is important to point out that caffeine daily intake recommendations may be lower for healthy children aging 12 years old or younger [13].
Regarding domicile, the higher intake of caffeine in the South, Northeast, and Southeast regions is coherent with the coffee consumption observed in these Brazilian regions during the same period of time [18], except for São Paulo state. Furthermore, tea consumption is more than five times higher in the South than in the other regions of Brazil, which contributed to caffeine intake [18].
The higher caffeine intake among males may be related to cultural or behavioral factors, such as the tendency of individuals of this gender also smoke more [32]. In fact, individuals with low education and higher caffeine intake, regardless of the gender, are also more likely to smoke [12, 32, 33]. Lower education and low income (PCFI), which are well-known related factors, were also correlated with higher caffeine intake in Brazil.
It is relevant to notice that the coefficient of determination of a multiple regression equation for caffeine intake is 4.5 %, despite including the family income per capita, color, ethnical group, age, gender, schooling, and region of living as explanatory variables. Hence, it means that caffeine consumption varies a lot among people, probably because of the influence of cultural or behavioral variables, showing no relevant association with the described characteristics. However, although the power of explanation is considered low, statistical significance effects are detected due to the large number of sample observation (n = 33,453).
This study reports few caffeine dietary sources. Caffee was also the major dietary source of caffeine in the USA [28], UK [29], and Austria [31]. In Japan, not only coffee but also tea had important contributions [30]. Soft drinks seem to be a greater caffeine contributor to the diet among predominantly younger groups [29] and represent a small portion of caffeine in the PFCM sample.
Conclusions
Daily caffeine intake (mean values) in Brazil (115.7 mg) is below the recommended limit reference value for adults. The percentage of individuals whom diet reveals excessive content of caffeine (>400 mg) is low (up to 3.0 %). Thus, excessive caffeine intake may not be a health issue in Brazil.
Despite the coefficient of determination of the multiple regression equation for caffeine intake of only 4.5 %, most of the determinants analyzed showed significant regression coefficients (p < 0.005). Adjusting the other coefficients, an association was observed between caffeine intake and gender and domicile. Males and individuals living in the Northeast or South regions or in the states of Minas Gerais, Rio de Janeiro, and Espírito Santo are likely to ingest higher contents of the substance. The major dietary sources are coffee, regular or with milk.
Abbreviations
HBS, household budget survey; HPLC, high performance liquid chromatography; IBGE, Brazilian Institute of Geography and Statistics; PCFI, per capita family income; PFCM, personal food consumption module; UV/VIS, ultraviolet/visible detector
References
Finnegan D. The health effects of stimulant drinks. Nutr Bull. 2003;28:147–55.
Souza AM, Pereira RA, Yokoo EM, Levy RB, Sichieri R. Alimentos mais consumidos no Brasil: inquérito nacional de alimentação 2008-2009. Rev Saude Publica. 2013;47(1):190S–9S.
Heckman MA, Weil J, Gonzalez de Mejia E. Caffeine (1,3,7-trimethylxanthine) in foods: a comprehensive review on consumption, functionality, safety, and regulatory matters. J Food Sci. 2010;75(3):77–87.
Mandel HG. Update on caffeine consumption, disposition and action. Food Chem Toxicol. 2002;40:1231–4.
Nawrot P, Jordan S, Eastwood J, Rotstein J, Hugenholtz A, Feeley M. Effects of caffeine on human health. Food Addit Contam. 2003;20(1):1–30.
Dawkins L, Shahzad FZ, Ahmed SS, Edmonds CJ. Expectation of having consumed caffeine can improve performance and mood. Appetite. 2011;57(3):597–600.
Shirlow MJ, Mathers CD. A study of caffeine consumption and symptoms: indigestion, palpitations, tremor, headache and insomnia. Int J Epidemiol. 1985;14(2):239–48.
Shirlow MJ, Berry G, Stokes G. Caffeine consumption and blood pressure: an epidemiological study. Int J Epidemiol. 1988;17(1):90–7.
Hering-Hanit R, Gadoth N. Caffeine-induced headache in children and adolescents. Cephalalgia. 2003;23:332–5.
Charles BG, Townsend SR, Steer PA, Flenady VJ, Gray PH, Shearman A. Caffeine citrate treatment for extremely premature infants with apnea: population pharmacokinetics, absolute bioavailability, and implications for therapeutic drug monitoring. Ther Drug Monit. 2008;30(6):709–16.
Calamaro CJ, Mason TB, Ratcliffe SJ. Adolescents living the 24/7 lifestyle: effects of caffeine and technology on sleep duration and daytime functioning. J Pediatr. 2009;123:1005–10.
Higdon JV, Frei B. Coffee and health: a review of recent human research. Crit Rev Food Sci Nutr. 2006;46(2):101–23.
Health Canada. It’s your health: caffeine. 2012. http://www.hc-sc.gc.ca/fn-an/securit/addit/caf/index-eng.php. Accessed 3 Jul 2014.
United States Department of Agriculture. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Washington: USDA; 2015.
Liu J, Sui X, Lavie CJ, Hebert JR, Earnest CP, Zhang J, Blair SN. Association of coffee consumption with all-cause and cardiovascular disease mortality. Mayo Clin Proc. 2013;88(10):1066–74.
Graham DM. Caffeine—its identity, dietary sources, intake and biological effects. Nutr Rev. 1978;36(4):97–102.
Sichieri R, Pereira RA, Martins A, Vasconcellos ABPA, Trichopoulou A. Rationale, design, and analysis of combined Brazilian household budget survey and food intake individual data. BMC Public Health. 2008;8:89–93.
Instituto Brasileiro de Geografia e Estatística. Pesquisa de Orçamentos Familiares 2008-2009: Análise do Consumo Alimentar Pessoal no Brasil. Rio de Janeiro: IBGE; 2011.
Couper Smartt J, Couper SI. Caffeine consumption: a review of its use, intake, clinical effects and hazards. Food Tech Aust. 1984;36(3):131–4.
Barone JJ, Roberts HR. Caffeine consumption. Food Chem Toxicol. 1996;34(1):119–29.
Andrade JB, Pinheiro HLC, Lopes WA, Martins AMMA, Brandão AM. Determinação de cafeína em bebidas através de cromatografia líquida de alta eficiência (CLAE). Quim Nova. 1995;18(4):379–81.
Camargo MCR. Caffeine daily intake from dietary sources in Brazil. Food Addit Contam. 1999;16(2):79–87.
United States Department of Agriculture. Composition of foods raw, processed, prepared: USDA National Nutrient Database for Standard Reference, Release 25. Beltsville: USDA; 2012.
University of Minnesota. Nutrition Coordinating Center. Nutrition Data System for Research. Version 2008. Minneapolis: University of Minnesota. 2008. http://www.ncc.umn.edu/products/ndsr.html. Accessed 15 Feb 2014.
Instituto Brasileiro de Geografia e Estatística. Contagem da população 2007. Rio de Janeiro: IBGE; 2008.
SAS. SAS, version 9.3. 2011.
Lagiou P, Trichopoulou A. The DAPHNE initiative: the methodology for assessing dietary patterns across Europe using household budget survey data. Public Health Nutr. 2001;4(5B):1135–41.
Fitt E, Pell D, Cole D. Assessing caffeine intake in the United Kingdom diet. Food Chem. 2013;140:413–26.
Mitchell DC, Knight CA, Hockenberry J, Teplansky R, Hartman TJ. Beverage caffeine intakes in the U.S. Food Chem Toxicol. 2014;63:136–42.
Yamada M, Sasaki S, Murakami K, Takahashi Y, Okubo H, Hirota N, et al. Estimation of caffeine intake in Japanese adults using 16 d weighed diet records based on a food composition database newly developed for Japanese populations. Public Health Nutr. 2011;13(5):663–72.
Rudolph E, Faerbinger A, Koenig J. Caffeine intake from all sources in adolescents and young adults in Austria. Eur J Clin Nutr. 2014;68:793–8.
Brasil Ministério da Saúde. Vigitel Brasil 2014 - Vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: MS; 2015.
Larsson SC, Männistö S, Virtanen MJ, Kontto J, Albanes D, Virtamo J. Coffee and tea consumption and risk of stroke subtypes in male smokers. Stroke. 2008;39(6):1681–7.
Acknowledgements
Not applicable.
Funding
The corresponding author was granted with a scholarship from the Coordination for the Improvement of Higher Education Personnel (CAPES).
Authors’ contributions
AGdOS contributed to the conception and design of the study and analysis and interpretation of data. MVdS performed the statistical analysis; analysis and interpretation of data; and critical review of the intellectual content. Both authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
The present study used secondary data from a national household budget survey.
Ethics approval and consent to participate
The present study used secondary data from a national household budget survey.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Giovanini de Oliveira Sartori, A., Vieira da Silva, M. Caffeine in Brazil: intake, socioeconomic and demographic determinants, and major dietary sources. Nutrire 41, 11 (2016). https://doi.org/10.1186/s41110-016-0014-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41110-016-0014-x