
Abstract
Background
Cinacalcet hydrochloride (cinacalcet), an oral calcimimetics for secondary hyperparathyroidism (SHPT), has been widely used worldwide. In contrast, evocalcet, an improved derivative of cinacalcet, was approved only in Japan in 2018 and has not received approval overseas. Consequently, the available information on the long-term use of evocalcet relies solely on data from a 1-year dosing phase III clinical trial.
Methods
The cohort of 147 chronic hemodialysis patients on cinacalcet to manage SHPT was simultaneously switched to the lowest dose of evocalcet (1 mg/day) and prospectively followed for 5 years in real-world clinical settings.
Results
The median evocalcet dose was 1 mg/day at 0.5 years, and it remained stable at 2 mg/day from 1 to 5 years after the prescription initiation. Additionally, serum parathyroid hormone, corrected calcium, phosphorus, and total alkaline phosphatase levels showed no significant changes compared with their levels at the time of the switch and remained stable over the 5-year period. Furthermore, no adverse events related to vital signs, serum biochemistries, or upper gastrointestinal symptoms were observed in patients during treatment with evocalcet.
Conclusions
These results suggest that only a small number of patients require higher evocalcet doses, and that SHPT can be effectively managed with low-dose evocalcet for 5 years. Additionally, the drug’s long-term safety has been confirmed.
Trial registration: name of the registry: Prescription change from cinacalcet hydrochloride to evocalcet in hemodialysis patients. Trial registration number R000041815. Trial registration UMIN000036702. Registered 10 May 2019—retrospectively registered. https://center6.umin.ac.jp/cgi-open-bin/ctr/ctr_his_list.cgi?recptno=R000041815.
Similar content being viewed by others


Background
Secondary hyperparathyroidism (SHPT) is one of the major complications in chronic hemodialysis patients [1, 2]. Persistent high parathyroid hormone (PTH) secretion increases bone turnover, resulting in bone fractures and vascular calcification, which decrease the patient’s quality of life and prognosis. Therefore, serum PTH levels should be appropriately controlled [3, 4].
Compounds that act on the calcium-sensing receptor (CaSR) on the parathyroid cell surface and inhibit PTH secretion are termed calcimimetics [5, 6]. The first-generation calcimimetic drug, cinacalcet hydrochloride (cinacalcet, Regpara Tablets®), caused a paradigm shift in the treatment of SHPT because, unlike vitamin D receptor activators (VDRAs), it can reduce both calcium (Ca) and phosphorus (P) levels in the blood [6,7,8,9]. However, cinacalcet has limiting side effects, particularly upper gastrointestinal (GI) symptoms such as nausea and vomiting, which lead to low adherence and insufficient dosage [10]. Additionally, it presents certain metabolic drawbacks, such as low bioavailability, primarily being metabolized by CYP3A4, and inhibiting CYP2D6 [11, 12]. In 2018, a new oral calcimimetic product, evocalcet (Orkedia Tablets®), was launched only in Japan to address these limitations and provide improved treatment options [12, 13]. Consequently, the available information on the long-term use of evocalcet relies solely on data from a 1-year dosing phase III clinical trial [14].
We have already reported in Japanese on the progress of 147 chronic hemodialysis patients who were initially treated with cinacalcet for their SHPT and subsequently switched to evocalcet, with follow-up assessments conducted up to 8 months [15] and 1 year later [16]. This study now presents prospective observations for the same cohort, spanning up to 5 years.
Subjects and methods
Subjects
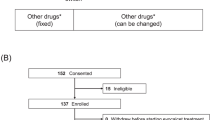
Of the 539 chronic hemodialysis patients at our dialysis center (Heisei Hidaka Clinic, Takasaki, Gunma, Japan), 147 patients who had been on a stable prescription of cinacalcet for the past 3 months were included in this study.
Methods
In September 2018 (baseline, BL), 147 patients who were initially treated with cinacalcet were simultaneously switched to the lowest dose of evocalcet (1 mg/day). The dose was subsequently adjusted at approximately monthly intervals to control serum intact PTH (i-PTH) levels according to the guidelines proposed by the Japanese Society for Dialysis Therapy (JSDT) [3].
For the patients prescribed evocalcet, dose, serum i-PTH, corrected Ca (cCa), P, and total alkaline phosphatase (ALP) levels were prospectively observed for 5 years until September 2023. Since the ALP measurement method was changed from the JSCC (Japan Society of Clinical Chemistry) method to the IFCC (International Federation of Clinical Chemistry and Laboratory Medicine) method during the observation period, the value obtained by the IFCC method was multiplied by 2.84 to convert to the value determined by the JSCC method.
These evocalcet dosage and serum parameters were analyzed every 6 months over time for 5 years and statistically compared with the values at BL. Additionally, the prescription status of other intravenous VDRAs and calcimimetics (etelcalcetide hydrochloride; etelcalcetide) in patients who had withdrawn from evocalcet in this cohort was analyzed. Furthermore, regarding serum i-PTH levels, we calculated the percentage of patients within the management target range (60–240 pg/mL) recommended by the JSDT [3].
Statistical analyses
After normality was determined by the Shapiro–Wilk test, normally distributed data were expressed as mean ± standard deviation, while non-normally distributed data were expressed as median (first quartile –third quartile). Repeated tests of paired samples were performed using one-way analysis of variance (with Bonferroni adjustment) or Friedman test, as appropriate. Statistical analysis was conducted using SPSS software (version 21, IBM, NY). P-values less than 0.05, based on two-sided calculations, were considered statistically significant.
Research ethics
This study was conducted under the approval of the Hidaka Hospital Medical Ethics Committee (approved no. 244; UMIN000036702) and in the spirit of the “Declaration of Helsinki.” The analysis and reporting were conducted in compliance with the “Guidelines for Protecting Patient Privacy in the Society Meeting Presentations and Medical Papers, including Case Reports” by the JSDT.
Results
Patient characteristics
Table 1 presents the main characteristics, dialysis conditions, and prescription statuses of drugs related to chronic kidney disease–mineral and bone disorder (CKD–MBD) in the cohort of 147 patients at BL. The median dose of cinacalcet immediately before the switch was 25 (12.5‒37.5) mg/day. Some of this data have been previously reported [15].
Evocalcet dosage
All patients were switched from cinacalcet to 1 mg/day of evocalcet at the BL. Subsequently, evocalcet doses were slightly increased, with the median reaching 2 mg/day after 1 year and remaining at a median of 2 mg/day until 5 years (Fig. 1). The highest dose observed during the observation period was 10 mg/day in 1 patient at 1.5 years, followed by 9 mg/day in 1 patient, 8 mg/day in 8 patients, and 7 mg/day in 12 patients.

Evocalcet dosage after switching from cinacalcet. The median evocalcet dose was 1 mg/day at 0.5 years and was maintained at 2 mg/day from 1 to 5 years after the switch. The number of patients receiving evocalcet at 1, 3, and 5 years is presented in Table 2. × mean values
Serum chemistries
Serum i-PTH levels during treatment with cinacalcet and at 6-month intervals for up to 5 years after switching to evocalcet are shown in Fig. 2, serum cCa and P levels in Fig. 3, and total ALP levels in Fig. 4. Comparing these four serum values with their respective BL levels, no statistically significant differences were observed at any time point. Additionally, the percentages of patients within the PTH control target range (60–240 pg/mL), below the lower target (< 60 pg/mL), and above the upper target (> 240 pg/mL) were also not substantially different over the 5-year period compared with when cinacalcet was prescribed (Fig. 5).

Serum i-PTH levels before and after switching from cinacalcet to evocalcet. Purple columns represent values under cinacalcet treatment, while blue ones represent values under evocalcet treatment. No statistically significant differences were observed at any time point compared with the BL values. i-PTH intact parathyroid hormone, BL baseline, × mean values

Serum corrected Ca (○) and P (△) levels before and after switching from cinacalcet to evocalcet. Purple circles and triangles represent values under cinacalcet treatment, while blue ones represent values under evocalcet treatment. No statistically significant differences were found at any time point compared with the respective BL values. Ca calcium, P phosphorus, BL baseline, × mean values

Serum total ALP levels before and after switching from cinacalcet to evocalcet. Purple columns represent values under cinacalcet treatment, while blue ones represent values under evocalcet treatment. No statistically significant differences were observed at any time point compared with the BL values. ALP alkaline phosphatase, BL baseline, × mean values

Percentage of patients within PTH control targets before and after switching from cinacalcet to evocalcet. Purple columns represent patients with i-PTH within target values under cinacalcet treatment, while blue ones represent those with i-PTH within target values under evocalcet treatment. Yellow columns represent patients with i-PTH < 60 pg/mL, while orange ones represent those with i-PTH > 240 pg/mL. i-PTH intact parathyroid hormone, BL baseline
Prescription persistence rate of evocalcet
In this cohort of 147 patients who switched from cinacalcet to evocalcet, the number of patients undergoing hemodialysis at our hospital gradually decreased due to hospital transfers or death: 133 (90.5%) at 1 year, 100 (68.0%) at 3 years, and 76 (51.7%) at 5 years (Table 2). Simultaneously, the number of patients prescribed evocalcet gradually decreased: 115 at 1 year, 68 at 3 years, and 42 at 5 years. Consequently, the prescription persistence rate of evocalcet was calculated as follows: 86.5% at 1 year, 68.0% at 3 years, and 55.3% at 5 years. However, no vital signs, serum biochemistries, or upper GI-related adverse events were observed in patients during evocalcet treatment that would necessitate discontinuation of the evocalcet prescription or a switch to other drugs for SHPT.
Intravenous drugs for SHPT
Patients prescribed intravenous drugs for SHPT (VDRAs and etelcalcetide), from BL to 5 years later, in this cohort are presented in Table 2. The number of patients prescribed evocalcet gradually decreased, while the number of patients prescribed maxacalcitol or etelcalcetide gradually increased. Additionally, there were several patients who were not prescribed either evocalcet or intravenous drugs for SHPT.
Discussion
This is the first report on the long-term use of evocalcet in real-world clinical settings. With a median dose of 2 mg/day of evocalcet, serum i-PTH, cCa, P, and total ALP levels remained stable for 4 years without dose escalation or clinically problematic side effects.
The noninferiority of evocalcet to cinacalcet in suppressing serum i-PTH levels, along with fewer GI-related adverse events, has been robustly demonstrated in a phase 3, randomized, double-blind, double-dummy clinical trial [17]. In our present cohort study, we also reported using a questionnaire that switching from cinacalcet to evocalcet significantly reduced the number of patients complaining of GI-related symptoms [15]. Additionally, we successfully discontinued the prescription of GI-promoting medications in some patients after switching [15]. However, it is important to note a significant limitation in our study; specifically, the absence of a control group continuing to receive the cinacalcet prescription. Therefore, it is not possible to make a rigorous comparison of the efficacy and safety of cinacalcet and evocalcet.
Several factors may explain why evocalcet was able to control PTH levels for a long time without requiring dose escalation. First, some patients whose PTH was not adequately suppressed with low-dose evocalcet had been switched to etelcalcetide prescriptions rather than increasing their doses to medium or high levels. The maximum dose of evocalcet is 12 mg/day. However, due to the availability of only two formulations (1 mg and 2 mg tablets), a pill burden occurs when prescribing higher doses. In fact, during the 5-year study period, only a few patients were prescribed more than 8 mg (i.e., 4 pills of 2 mg tablet), and at the end of the 5-year period, 22 patients had switched to intravenous etelcalcetide to avoid this pill burden. We have previously reported, based on medical information data, that the prescription persistence rate for cinacalcet treatment at 3 years was approximately 75% in Japan [18]. This result was obtained before the introduction of etelcalcetide to the market in Japan. Therefore, the current 3-year prescription persistence rate (68.0%) is considered to be somewhat lower than this. As supplementary information, Orkedia Tablets® 4 mg were launched in November 2023, with an expected improvement in prescription persistence due to reduced pill burden.
Second, the bioavailability of evocalcet is significantly higher than that of cinacalcet [12, 13], which means there were no patients with difficulty achieving adequate blood concentrations [19]. As a result, all patients were able to maintain effective blood concentrations even at low doses.
Third, because evocalcet has a potent inhibitory effect on parathyroid cell proliferation [20], it may have prevented the development of parathyroid hyperplasia during the treatment period. It is worth noting that the administration of cinacalcet to hemodialysis patients has been reported to lead to a reduction in parathyroid gland volumes [21, 22]. Due to the positive correlation between blood PTH levels and total parathyroid gland volumes [23], it is likely that evocalcet not only suppressed PTH secretion acutely but also maintained low PTH levels by inhibiting parathyroid cell proliferation and preserving a small gland size. Additionally, in our present cohort, seven patients were not prescribed evocalcet, intravenous VDRAs, or etelcalcetide even after 3 years. It is interesting to consider the possibility that these patients may have experienced complete regression of hyperplastic parathyroid glands.
Finally, cinacalcet can increase the number of CaSRs on the surface of parathyroid cell membranes through a pharmacological chaperone action [24,25,26]. Since evocalcet and cinacalcet bind to the same site on the CaSRs [27], it is assumed that the CaSRs on the surface of parathyroid cell membranes would be either maintained or increased under evocalcet treatment, which may explain why the low dose remains effective.
Switching from cinacalcet to evocalcet did not further decrease i-PTH, nor did it markedly increase the percentage of patients within PTH control targets. Consequently, there was no marked change in serum cCa, P, or total ALP levels, which fluctuate with blood PTH levels, compared with the BL. The reason for the lack of further improvement in PTH may be that this cohort was already on cinacalcet for PTH control. Future studies should be conducted in patients who have not previously been prescribed any calcimimetics.
Conclusion
The present results indicate that SHPT can be managed for a long period of time under low-dose evocalcet use.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ALP:
-
Alkaline phosphatase
- BL:
-
Baseline
- Ca:
-
Calcium
- CaSR:
-
Calcium-sensing receptor
- cCa:
-
Corrected calcium
- CKD–MBD:
-
Chronic kidney disease–mineral and bone disorder
- GI:
-
Gastrointestinal
- i-PTH:
-
Intact parathyroid hormone
- JSDT:
-
Japanese Society for Dialysis Therapy
- P:
-
Phosphorus
- PTH:
-
Parathyroid hormone
- SHPT:
-
Secondary hyperparathyroidism
- VDRAs:
-
Vitamin D receptor activators
References
Cunningham J, Locatelli F, Rodriguez M. Secondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic options. Clin J Am Soc Nephrol. 2011;6:913–21.
Komaba H, Kakuta T, Fukagawa M. Diseases of the parathyroid gland in chronic kidney disease. Clin Exp Nephrol. 2011;15:797–809.
Fukagawa M, Yokoyama K, Koiwa F, et al. Clinical practice guideline for the management of chronic kidney disease-mineral and bone disorder. Ther Apher Dial. 2013;17:247–88.
Ketteler M, Block GA, Evenepoel P, et al. Executive summary of the 2017 KDIGO chronic kidney disease-mineral and bone disorder (CKD-MBD) guideline update: what’s changed and why it matters. Kidney Int. 2017;92:26–36.
Nagano N, Nemeth EF. Functional proteins involved in regulation of intracellular Ca(2+) for drug development: the extracellular calcium receptor and an innovative medical approach to control secondary hyperparathyroidism by calcimimetics. J Pharmacol Sci. 2005;97:355–60.
Nagano N. Pharmacological and clinical properties of calcimimetics: calcium receptor activators that afford an innovative approach to controlling hyperparathyroidism. Pharmacol Ther. 2006;109:339–65.
Fukagawa M, Yumita S, Akizawa T, et al. Cinacalcet (KRN1493) effectively decreases the serum intact PTH level with favorable control of the serum phosphorus and calcium levels in Japanese dialysis patients. Nephrol Dial Transplant. 2008;23:328–35.
Sprague SM, Evenepoel P, Curzi MP, et al. Simultaneous control of PTH and Ca×P Is sustained over three years of treatment with cinacalcet HCl. Clin J Am Soc Nephrol. 2009;4:1465–76.
Akizawa T, Kido R, Fukagawa M, et al. Decreases in PTH in Japanese hemodialysis patients with secondary hyperparathyroidism: associations with changing practice patterns. Clin J Am Soc Nephrol. 2011;6:2280–8.
Gincherman Y, Moloney K, McKee C, Coyne DW. Assessment of adherence to cinacalcet by prescription refill rates in hemodialysis patients. Hemodial Int. 2010;14:68–72.
Padhi D, Harris R. Clinical pharmacokinetic and pharmacodynamic profile of cinacalcet hydrochloride. Clin Pharmacokinet. 2009;48:303–11.
Akizawa T, Ikejiri K, Kondo Y, Endo Y, Fukagawa M. Evocalcet: a new oral calcimimetic for dialysis patients with secondary hyperparathyroidism. Ther Apher Dial. 2020;24:248–57.
Wada M, Kawata T, Nagano N. Calcimimetics for treating hyperparathyroidism. In: Zaidi M, editor. Encyclopedia of bone biology. 1st ed. New York: Academic Press; 2020. p. 697–710.
Yokoyama K, Shimazaki R, Fukagawa M, Akizawa T. Long-term efficacy and safety of evocalcet in Japanese patients with secondary hyperparathyroidism receiving hemodialysis. Sci Rep. 2019;9:6410.
Ito K, Takahashi A, Saito T, et al. Prescription change from cinacalcet hydrochloride to evocalcet: simultaneous switching of 147 chronic hemodialysis patients. J Jpn Soc Dial Ther. 2019;52:585–92 ((In Japanese)).
Tsuchiya Y, Ito K, Ando T, Tsutsui T, Ogawa T, Nagano N. The characteristics of hemodialysis patients continued to be prescribed 1mg of evocalcet for 1 year, after switching from cinacalcet hydrochloride to evocalcet. Kidney and Dialysis. 2020;89:141–8 ((In Japanese)).
Fukagawa M, Shimazaki R, Akizawa T; Evocalcet study group. Head-to-head comparison of the new calcimimetic agent evocalcet with cinacalcet in Japanese hemodialysis patients with secondary hyperparathyroidism. Kidney Int. 2018;94:818–25.
Yokoyama K, Asada S, Kawata T, Nagano N. Compliance and persistence of oral calcimimetics in maintenance hemodialysis patients: a pharmacoepidemiological study utilizing electronic health record. J Jpn Soc Dial Ther. 2018;51:525–33 ((In Japanese)).
Hellriegel ET, Bjornsson TD, Hauck WW. Interpatient variability in bioavailability is related to the extent of absorption: implications for bioavailability and bioequivalence studies. Clin Pharmacol Ther. 1996;60:601–7.
Sakai M, Tokunaga S, Kawai M, et al. Evocalcet prevents ectopic calcification and parathyroid hyperplasia in rats with secondary hyperparathyroidism. PLoS ONE. 2020;15:e0232428.
Komaba H, Nakanishi S, Fujimori A, et al. Cinacalcet effectively reduces parathyroid hormone secretion and gland volume regardless of pretreatment gland size in patients with secondary hyperparathyroidism. Clin J Am Soc Nephrol. 2010;5:2305–14.
Okuno S, Inaba M, Ishimura E, et al. Effects of long-term cinacalcet administration on parathyroid gland in hemodialysis patients with secondary hyperparathyroidism. Nephron. 2019;142:106–13.
Fang L, Tang B, Hou D, Meng M, Xiong M, Yang J. Relationship between parathyroid mass and parathyroid hormone level in hemodialysis patients with secondary hyperparathyroidism. BMC Nephrol. 2015;16:82.
Cavanaugh A, Huang Y, Breitwieser GE. Behind the curtain: cellular mechanisms for allosteric modulation of calcium-sensing receptors. Br J Pharmacol. 2012;165:1670–7.
Leidenheimer NJ, Ryder KG. Pharmacological chaperoning: a primer on mechanism and pharmacology. Pharmacol Res. 2014;83:10–9.
Breitwieser GE. Pharmacoperones and the calcium sensing receptor: exogenous and endogenous regulators. Pharmacol Res. 2014;83:30–7.
Miyazaki H, Ikeda Y, Sakurai O, et al. Discovery of evocalcet, a next-generation calcium-sensing receptor agonist for the treatment of hyperparathyroidism. Bioorg Med Chem Lett. 2018;28:2055–60.
Acknowledgements
We express our gratitude to Mr. Yasuhiro Otsuka (Heisei Hidaka Clinic, Dialysis Center) for compiling a database of regular monthly blood sampling results and drug prescription records.
Funding
None declared.
Author information
Authors and Affiliations
Contributions
N.N. designed and performed the study, analyzed the data, and wrote the manuscript. T.T. and K.I. reviewed and revised the manuscript, and T.O. is responsible for the final version of the manuscript. T.I., M.Y., Y.K., M.M., N.T., S.M., T.O., and K.I. were responsible for drug prescription for patients. K.I. and T.O. supervised the study. All the authors read and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and was approved by the Hidaka Hospital Medical Ethics Committee (approval number: 244). This study took place in a real clinical setting, and patient consent was obtained verbally when changing the prescription from cinacalcet to evocalcet.
Consent for publication
Consent for publication was obtained from all co-authors. Patient consent was not obtained due to the unfortunate circumstances where many patients had either passed away or been transferred to other hospitals.
Competing interests
N.N. has received consulting fees and lecture fees from Kyowa Kirin Co., Ltd. The other authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nagano, N., Ishikawa, T., Yamaguchi, M. et al. Long-term treatment of evocalcet in hemodialysis patients with secondary hyperparathyroidism: a five-year prospective cohort study in 147 Japanese patients. Ren Replace Ther 10, 13 (2024). https://doi.org/10.1186/s41100-024-00529-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-024-00529-z