
Abstract
Background
Intravenous administration of amino acid (AA) formulation (IVAA) as intradialytic parenteral nutrition is widely used for malnourished patients with end-stage kidney disease (ESKD) treated with hemodialysis (HD) or hemodiafiltration (HDF). Although various therapy recipes such as AA compositions or simultaneous administration of glucose and/or lipids have been attempted, the specific effects of each recipe on AA behaviors and metabolic consequences have not been well investigated. To clarify the effect of simultaneous glucose administration with IVAA, we investigated the behavior of AAs, insulin as a metabolic hormone, and energy-related metabolites during an HDF session in two patients.
Case presentation
We aimed to determine the effect of IVAA with or without simultaneous glucose administration. The plasma levels of AAs, branched-chain AAs (leucine, isoleucine, and valine), major nonessential AAs (alanine and glutamine with glutamate), insulin, glucose, and ketone bodies were measured before HDF and at the second hour (prior to the meal in the HDF session). Lost AAs in the spent dialysate were also measured for the first two hours during the HDF session.
Conclusion
In the absence of glucose administration, plasma AA levels and the loss of AAs in the dialysate increased owing to IVAA, with the increase in plasma levels in ketone bodies occurring because of scarce secretion of plasma insulin. In the presence of glucose administration, plasma levels and the loss of AA decreased even when the same amount of AAs was injected, possibly because of the profound secretion of insulin with a decrease in ketone bodies. The present findings suggest that the metabolic effects of simultaneous glucose administration on IVAAs enhanced AA uptake into the body during HDF sessions, which might increase the effectiveness of IVAAs.
Similar content being viewed by others


Introduction
In recent years, high-efficiency hemodialysis (HD) and hemodiafiltration (HDF) for patients with end-stage kidney disease (ESKD) have become the dominant therapeutic approach. Such high efficacy treatment, however, increases the depletion of small molecule nutrients, especially amino acids (AAs) [1,2,3]. The removal efficacies of AAs were reported to have no substantial differences between HD and HDF [2]. A loss of AAs from the body not only means they flow out from the plasma but also entails protein breakdown in muscle, as HD (HDF) treatment itself also involves a protein-catabolic aspect [4, 5]. In addition, the current progressive aging of patients with ESKD [6] requires an effective strategy to minimize the negative effects of highly efficacious treatments on AA kinetics. Therefore, adequate nutritional therapy for ESKD patients treated with dialysis therapy should be highlighted, especially for maintaining body protein levels through minimizing protein breakdown.
As a nutrient therapy for ESKD patients several studies concerning intradialytic parenteral nutrition (IDPN) with various AA constitutions or coadministration of glucose and/or lipids [7,8,9,10,11,12] have evaluated long-term influences on patients’ clinical parameters regarding mortality. However, no definite consensus has been reached on the effect of IDPN recipes on nutrients in ESKD patients. Moreover, IDPN involves a direct injection of certain amounts of AAs or other constituents into the blood, which may invoke additional metabolic disruption in the treatment. Therefore, the intercorrelations between AAs, insulin as a metabolic hormone, and energy-related metabolites during session should be investigated in detail. However, few studies have elucidated metabolic behaviors during sessions with or without IDPN.
In our previous study regarding the intravenous administration of amino acids (IVAA) with only AA formulation without simultaneous glucose administration to patients with diabetes mellitus during HDF, analysis of AA profiles in plasma and spent dialysate showed in imperfect compensation in individual AAs for the dialysis removal [13]. IVAA is often dispensed along with glucose coadministration in a clinical setting; however, the metabolic effect of additional glucose administration on IDPN has not yet been evaluated.
In a previous study, we found that HD or HDF induced disruption of energy homeostasis through rapid depletion of insulin and elevation of ketone bodies in plasma, which often invoked cell starvation [14, 15]. In addition, plasma levels of branched-chain AAs (BCAA) were found to increase after the first hour of the fasting HD session [15]. BCAAs belong to the essential AA (EAA) group, and EAAs have no in vivo biosynthesis; therefore, the increase in plasma BCAA levels during dialysate was suggested to originate from the free AA pool along with body protein breakdown.
This study aimed to evaluate AA behaviors and effects on energy metabolism of simultaneous glucose administration with IVAA during HDF in two patients without diabetes mellitus through measuring the plasma levels of BCAA (leucine [Leu], isoleucine [Ile], and valine [Val]), the major nonessential AAs (NEAA, alanine, and glutamine including glutamate), insulin, ketone bodies, and blood glucose together with dialysate loss in BCAA and NEAA.
Case presentation and methods
In this report, we evaluated two malnutritional ESKD patients without diabetes mellitus (P1 and P2) needing IDPN therapy, who underwent maintenance 5 h predilution HDF. They were Patient characteristics are presented in Table 1. In these two patients, the dialysate glucose concentration was 150 mg/dL. Table 1 shows patient’s profile including nutritional parameters.
Three HDF conditions were specified for this study, as follows: (i) HDF without IVAA (C1), (ii) HDF with IVAA (C2), and (iii) HDF with IVAA and simultaneous glucose administration (C3).
For IVAAs in C2 and C3, an AA-containing solution (Kidmin®, Otsuka Pharmaceutical. Co Ltd., Tokyo, Japan) for the two patients with ESKD was injected consistently throughout each HDF session at a constant rate for two hours into venous blood (40 mL/h) during each HDF session (Fig. 1). Kidmin® includes a total of 5.76 g AAs, comprising 17 kinds of AAs, including 9 EAAs. Of these, 3 BCAAs (isoleucine, valine and leucine) are the major components (Fig. 2). For glucose administration in C3, a 50% glucose solution was injected for two hours during HDF at a constant rate of 40 mL/h, similar to the Kidmin® infusion (Fig. 1). The patients ate their lunch at the second hour from the start of HDF; thus, our study was conducted in the earlier half of the session, from the start to the second hour before meals, to avoid the metabolic influence of meal intake. In each condition, plasma samples were collected before the HDF (initial) session and at the second hour before the lunchtime meal (final) using a method reported in a previous study [16, 17]. Dialysate was collected at four time points, namely, at 15 min, 30 min, 1 h, and 2 h (before lunch) from the start of the session (Fig. 1).

The time courses of AA and glucose administration and the timing of the sample collection. Time course of 5 h HDF session. (C1): without IVAA or glucose, (C2): with IVAA only, (C3): with IVAA and glucose coadministration. Blood was sampled at two time points (0 h and 2 h), and spent dialysate was sampled at four time points (15 min, 30 min, 1 h and 2 h) before meals. Blood samples were taken from the inflow of the dialysis apparatus

Major components of IVAA solution Kidmin® (mmol)
The plasma levels of the following molecules were quantified in these samples: major components of NEAAs (alanine [Ala], glutamine, and glutamate), three BCAAs (Ile, Leu, Val), glucose, and immunoreactive insulin (IRI). As glutamine is easily converted to glutamate in normal laboratory settings [13, 15], the sum of the glutamine and glutamate levels was evaluated as glutamine-glutamate (Glx) levels. In the dialysate samples, three BCAAs, Ala, and Glx were measured using the same method as for blood, and ketone bodies (KB; including 3-hydroxy butyrate and acetoacetate) were measured using quantitative 1HNMR spectroscopy of dialysate and converted to plasma levels [14,15,16].
IRI, AA, and plasma glucose (PG) levels were determined using CLIA, HPLC, and enzymatic methods, respectively (LSI Medience Corp., Tokyo, Japan).
Quantification of AA lost in the dialysate was conducted using an area under the curve of time course change in dialysate AA levels using a rectangular approximation method [18]. The balance of each AA was subtracted from the loss starting from the entry of respective Kidmin® components flowing into the blood.
This study was approved by the Ethical Committee of Teikyo University (TU-20-194), and written informed consent was obtained from both patients.
Results
Figure 3 shows the plasma levels of Leu, Ile, Val, Ala, and Glx before HDF (initial) and at the second hour before lunch (final) under the three conditions (C1–C3). Under C1 (without IVAA), all plasma levels of AA decreased toward the final level owing to HDF removal. Comparing the final to the initial plasma levels of C1 and C2 in each AA, the levels in C2 were much higher than those in C1, except Ala and Glx for P2. These increases were due to IVAAs, and the composition of the five AAs is presented in Fig. 2. In C3 (with IVAA and simultaneous glucose administration), the final plasma levels were much lower than those in C2, even with the same injected amounts of AA via IVAA as in C2. These final and initial plasma levels (labeled in Fig. 3) were used to calculate the increased ratio defined as; (final level–initial level)/initial level. The ratios for P1 in C2 and C3 were 2.23 and 0.87 (Ile), 1.96 and 0.71(Leu), 0.98 and 0.21(Val), respectively. Those for P2 were 0.36 and 0.05 (Ile), 0.24 and 0.04 (Leu), -0.07 and-0.12 (Val), respectively. These decreased ratios in C3 compared to C2 presented the effects of glucose coadministration on plasma levels in BCAAs.

Plasma levels of Leu, Ile, Val Ala and Glx (μmol/L) at two time points; 0 h and 2 h. In each graph, the dotted line depicts C1 (without IVAA), the broken line C2 (with IVAA), and the real line C3 (with IVAA and simultaneous glucose administration). All the data were labeled to each point in graphs
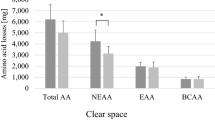
Figure 4 shows the AA loss (into dialysate) and amount balance in each AA in the three conditions (C1–C3) for P1 and P2. Concerning AA loss as shown in the left panels of Fig. 4, there were larger decreases in C2 than in C1 owing to IVAA; however, they became smaller in C3 than in C2, with the exception of Ala in P2. The right panels show balance graphs for each AA (administered amount (Kidmin®) subtracted by loss) outlined in the three conditions (C1–C3) for P1 and P2. The bars with positive signs indicate the amount preserved in the body, and the bars with negative signs indicate the amount of flow out of the body. In C1, the blank bars of all the AAs have negative signs showing flow out of the body due to HDF removal, which are equal to the blank bars in the left panels of Fig. 4. In C2 and C3 (with IVAA), the values of the three BCAAs (P1 and P2) had positive signs, and the values of Ala and Glx had negative signs.

The loss and the balance of amino acids (0–2 h) (mmol). Each AA loss and balance was lined in the three conditions. In each graph, the blank bar depicts C1 (without IVAA), the blue bar C2 (with IVAA), and the red bar C3 (with IVAA and simultaneous glucose administration)
Figure 5 illustrates the time change of plasma levels for IRI, PG, and KB in the three conditions for P1 and P2. As to the changes of IRI and KB, their time course profiles were quite different: the increase of IRI was observed only in C3, and the increase of KB (which indicates cell-starvation state) was lacking only in C3.

Plasma levels of insulin (mU/L), glucose (mg/mL) ketone bodies (μM) at two time points; 0 h and 2 h. The green fields indicate the normal range for IRI and KB, respectively
Discussion
Behavior in amino acids
In HDF with no IVAA or glucose addition (C1), the plasma levels in five types of AAs decreased, which showed flow out from the blood (Fig. 3) and negative signs that indicated flow out from the body (Fig. 4).
With IVAA but without glucose administration (C2), the plasma levels of BCAA in the final stage increased to become higher than the initial levels (Fig. 3), and these increases for P1 were much higher than those for P2. Possible reasons to explain the difference between P1 and P2 could be that the initial levels were lower for P1 and that there might be differences in insulin sensitivities between the two patients, as will be mentioned below. Other AAs such as Ala and Glx, which are minor components in IVAA (Fig. 2), did not increase but rather decreased in a similar manner as in C1. Due to IVAA, a certain amount of injected BCAA was replete not only in the blood (Fig. 3) but also in the body (the right panels of Fig. 4), and some flowed out in the dialysate (the left panels of Fig. 4).
Under the condition of IVAA and simultaneous glucose administration (C3), it should be noted that the final plasma BCAA levels became much lower as calculated above (Fig. 3) and that the amount of every BCAA retention became greater (the right panels of Fig. 4) than in C2, despite the same amount of IVAA having been injected for both patients. This phenomenon suggests that simultaneous glucose administration enhances AA uptake from the IVAA into the body, perhaps mainly in the liver and muscles.
Behaviors in energy-related metabolites: plasma glucose and insulin
Under conditions with no IVAA or glucose administration (C1), in P1, PG levels increased with an increase in IRI levels [20], whereas KB levels increased to an extremely high level. In contrast, in P2, PG levels were maintained with a decrease in IRI levels and an increase in KB levels up to a high level, but not higher than in P1. These results suggest that P1 might have had an insulin-secretion potential, which surpassed adsorption by the dialysis membrane [21], while insulin sensitivity might have been somewhat impaired. As a result, PG levels were not suppressed but increased up to the level of dialysate glucose (perhaps re-stimulating the secretion of IRI in P1). However, P2 might not have had enough insulin secretion potential to surpass the adsorption by the membrane, while insulin sensitivity might have been relatively preserved; thus, the PG level was suppressed, with possibly no further IRI secretion. Further study is necessary for identifying these different metabolic responses of the two.
Under the condition with IVAA but without glucose administration (C2), there were not much differences in the changes to PG, IRI, and KB levels compared with those in C1, except for slightly lower KB levels. This finding in both patients possibly indicates that there was no effect of IVAAs (containing BCAA and other AAs) on insulin secretion, which is characterized by the abnormal increase in KB levels.
On the other hand, under the conditions of IVAA and simultaneous glucose administration (C3), changes in the PG, IRI, and KB levels differed profoundly from those in conditions without glucose administration (C1 and C2). For P1, PG levels increased to approximately 250 mg/dL, with an evident increase in IRI levels. For P2, PG and IRI levels also increased, but their levels were not as high as those in P1. However, in both patients, KB levels decreased and then recovered to within the normal range.
Behaviors in ketone bodies
In the patients without diabetes in this report, toward the second hour of sessions without glucose administration (C1 and C2), KB levels increased to high levels. This significantly high level of KB might correspond to pathophysiological starvation [22, 23]. As mentioned in introduction, the increase of plasma levels of KB during treatments in patients with diabetes mellitus have been reported [14, 15], and underlined mechanism of them were suggested to be cell starvation. Circulating KB appears during starvation when the depletion of insulin induces free fatty acid release from adipose tissue, and β-oxidation is accelerated in the liver. During starvation, metabolism generally tends to be catabolic (entailing lipolysis and proteolysis); thus, even the preserved BCAA in C2 (Fig. 4) might not predispose to protein synthesis, but may be oxidized as a substrate for gluconeogenesis to produce energy. In such a catabolic condition, if dose of IVAA was augmented in the nutrient recipes, it might result in only the increase of loss of AA into dialysate or a part of absorbed AA might be refrained from protein synthesis.
In contrast, in the presence of simultaneous glucose administration with IVAA (C3), KB levels decreased and finally recovered to within the normal range. The disappearance of KB in plasma indicated suppressed lipolysis might be due to insulin secretion (Fig. 5), which could enhance the availability for possible protein synthesis in this anabolic state. Further investigation is required to verify the protein synthesis of these absorbed BCAAs.
Following the recent report that elevated blood KB levels correlated with water removal ratios among sessions [24], these correlations were evaluated in the present cases and resulted in negligible changes among the conditions (C1–C3), and the averages of water removal ratios were presented in Table 1.
Summary
In the present patients without diabetes, glucose concentration (150 mg/dL) in dialysate was consistently higher than the normal serum level (100 mg/dL) and even IVAA therapy only (C2) could not deter a state of (abnormal) starvation [25]. Glucose coadministration with IVAA has altered the AA kinetic behavior to an unexpected effect beside glucose itself as an energy generation. To compare C3 to C2, the plasma levels of every BCAA decreased (Fig. 3) and net-balance amounts of every BCAA have increased (Fig. 4) together with the synchronous changes in the values of PG, IRI and KB (Fig. 5).
In conclusion, the present cases study suggests that coadministration of glucose with IVAA exhibited potential usefulness in preserving AA in the body, which might enhance IVAA availability. This effect was probably due to the action of insulin, which is secreted through the administrated glucose.
Present our finding is preliminary but novel and the larger study is warranted in near future.
Availability of data and materials
The data and materials were all included in the manuscript.
Abbreviations
- AA:
-
Amino acid
- ESKD:
-
End-stage kidney disease
- HD:
-
Hemodialysis
- HDF:
-
Hemodiafiltration
- IVAA:
-
Intravenous administration of amino acid
- IDPN:
-
Intradialytic parenteral nutrition
- BCAA:
-
Branched-chain amino acid
- NEAA:
-
Nonessential amino acid
- EAA:
-
Essential amino acid
- IRI:
-
Immunoreactive insulin
- KB:
-
Ketone bodies
- PG:
-
Plasma glucose
- Ala:
-
Alanine
- Glx:
-
Glutamine, and glutamate
- Leu:
-
Leucine
- Ile:
-
Isoleucine
- Val:
-
Valine
References
Navarro JF, Mora C, León C, et al. Amino acid losses during hemodialysis with polyacrylonitrile membranes: effect of intradialytic amino acid supplementation on plasma amino acid concentrations and nutritional variables in nondiabetic patients. Am J Clin Nutr. 2000;71:765–73.
Murtas S, Aquilani R, Iadarola P, et al. Differences and effects of metabolic fate of individual amino acid loss in high-efficiency hemodialysis and hemodiafiltration. J Ren Nutr. 2020;30:440–51.
Hendriks FK, Smeets JSJ, Broers NJH, et al. End-stage renal disease patients lose a substantial amount of amino acids during hemodialysis. J Nutr. 2020;150:1160–6.
Lim VS, Ikizler TA, Raj DSC, Flanigan MJ. Does hemodialysis increase protein breakdown? Dissociation between whole-body amino acid turnover and regional muscle kinetics. J Am Soc Nephrol. 2005;16:862–8.
Ikizler TA, Pupim LB, Brouillette JR, et al. Hemodialysis stimulates muscle and whole body protein loss and alters substrate oxidation. Am J Physiol Endocrinol Metab. 2002;282:E107–16.
Watanabe Y, Kawanishi H, Suzuki K, et al. Japanese society for dialysis therapy clinical guideline for “maintenance hemodialysis: hemodialysis prescriptions.” Ther Apher Dial. 2015. https://doi.org/10.1111/1744-9987.12294.
Kopple JD, Foulks CJ, Piraino B, Beto JA, Goldstein J. National kidney foundation position paper on proposed health care financing administration guidelines for reimbursement of enteral and parenteral nutrition. J Ren Nutr. 1996;6:45–7.
Pupim LB, Flakoll PJ, Brouillette JR, Levenhagen DK, Hakim RM, Ikizker TA. Intradialytic parenteral nutrition improves protein and energy homeostasis in chronic hemodialysis patients. J Clin Invest. 2002;110:483–92.
Czekalski S, Hożejowski R. Malnutrition working group intradialytic amino acids supplementation in hemodialysis patients with malnutrition: results of a multicenter cohort study. J Ren Nutr. 2004. https://doi.org/10.1053/j.jrn.2004.01.007.
Corbello J, Rosner M (2009) Intradialytic total parenteral nutrition (IDPN): evidence-based recommendations. Pract Gastroenterol. 13–28.
Marsen TA, Beer J, Mann H. German IDPN-Trial group. Intradialytic parenteral nutrition in maintenance hemodialysis patients suffering from protein-energy wasting. Results of a multicenter open prospective randomized trial. Clin Nutr. 2017;36:107–17.
Anderson J, Peterson K, Bourne D, Boundy E. Effectiveness of intradialytic parenteral nutrition in treating protein-energy wasting in hemodialysis: a rapid systematic review. J Ren Nutr. 2019;29:361–9.
Fujiwara M, Ando I, Nemoto T, et al. Amino acid kinetics in diabetic patients during hemodiafiltration performed under intradialytic parenteral amino acid nutrition: a preliminary study. J Jpn Soc Dial Ther. 2019;52:457–62.
Fujiwara M, Ando I, Satoh K, et al. Biochemical evidence of cell starvation in diabetic hemodialysis patients. PLoS ONE. 2018. https://doi.org/10.1371/journal.pone.0204406.
Fujiwara M, Ando I, Shishido Y, Imai Y, Terawaki H. An increase in circulating levels of branched-chain amino acids during hemodialysis with regard to protein breakdown: three case reports. Ren Rep Ther. 2022;8:1–9.
Ando I, Takeuchi K, Oguma S, et al. 1H NMR spectroscopic quantification of plasma metabolites in dialysate during hemodialysis. Magn Reson Med Sci. 2013;12:129–35.
Yamamoto H, Kondo K, Tanaka T, et al. Reference intervals for plasma-free amino acid in a Japanese population. Ann Clin Biochem. 2016;53:357–64.
Lindgren O, Pacini G, Tura A, Holst JJ, Deacon CF, Ahrén B. Incretin effect after oral amino acid ingestion in humans. J Clin Endocrinol Metab. 2015;100:1172–6.
Iwase H, Kobayashi M, Nakajima M, Takatori T. The ratio of insulin to C-peptide can be used to make a forensic diagnosis of exogeneous insulin overdosage. Forensic Sci Int. 2001;115:123–7.
Raimann JG, Kruse A, Thijssen S, et al. Metabolic effect of dialyzate glucose in chronic hemodialysis: results from a prospective, randomized crossover trial. Nephrol Dial Transplant. 2012;27:1559–68.
Abe M, Kalantar-Zadeh K. Haemodialysis-induced hypoglycaemia and glycaemic disarrays. Nat Rev Nephrol. 2015;11:302–14.
Owen OE, Felig P, Morgan AP, Wahren J, Cahill GF. Liver and kidney metabolism during prolonged starvation. J Clin Invest. 1969;48:574–83.
Watford M. Starvation. Metabolic changes. In: eLS. John Wiley & Sons, Ltd: Chichester. 2015; pp1–7.
Suzuki T, Sasaki Y, Komatsu F, Maeda T, Suzuki K, Urita Y. Change of plasma ketone bodies and skin gass acetone in hemodialysis patients. Toho J Med. 2021;7(1):57–65.
Floyd JC, Fajans SS, Pek S, et al. Synergistic effect of essential amino acids and glucose upon insulin secretion in man. Diabetes. 1970;19:109–15.
Acknowledgements
The authors would like to thank the staff of Midorinosato Clinic who collected samples from patients and gave information from the patients.
Financial disclosure
The authors declare that they have no relevant financial disclosure.
Funding
This study received no specific funding.
Author information
Authors and Affiliations
Contributions
MF and IA conceived and analyzed the data. MF wrote the draft of the manuscript. YI, YS, and HT revised the manuscript critically for important intellectual content. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to patients
This study was approved by the Ethical Committee of Teikyo University (TU-20-194), and written informed consent for participation was obtained from the two patients.
Consent for publication
Written informed consent for publication was obtained from the two patients.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fujiwara, M., Ando, I., Shishido, Y. et al. Amino acid availability enhanced through glucose coadministration of amino acid supplementation during hemodiafiltration: two case reports. Ren Replace Ther 8, 28 (2022). https://doi.org/10.1186/s41100-022-00417-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-022-00417-4