
Abstract
Background
Chronic kidney disease (CKD) is characterized by structural abnormalities in nephrons, loss of functional nephrons, and impaired renal excretory function. A pro-vegetarian dietary pattern (PDP) is a gradual and progressive approach to vegetarianism. The current study aimed to assess the association between PDP and the odds of protein-energy wasting (PEW) and sarcopenia in patients with CKD.
Methods
The present cross-sectional study was conducted on kidney disease patients (n = 109) referred to two clinics in Shiraz, Iran. The diagnosis of sarcopenia and PEW was made according to the guidelines of the Asian Working Group for Sarcopenia (AWGS) and the International Society of Renal Nutrition and Metabolism (ISRNM) criteria, respectively. The participants’ dietary intake was evaluated using a 168-item semi-quantitative food frequency questionnaire (FFQ). For PDP index calculation, plant and animal food sources were categorized into 12 subgroups. The association between sarcopenia and PEW with PDP was evaluated using logistic regression.
Results
The PDP was significantly associated with a lower risk of PEW in the second tertile compared to the first in the crude model (odds ratio (OR) = 0.225; confidence interval (CI): 0.055–0.915; p-value = 0.037). After adjusting for potential confounders, lower significant odds of PEW were observed in the second and last tertiles of PDP compared to the first (T2: OR = 0.194; CI: 0.039–0.962; p-value = 0.045, and T3: OR = 0.168; CI: 0.030–0.950; p-value = 0.044). In contrast, no significant relationship was observed between PDP and the odds of sarcopenia (p-value ˃ 0.05).
Conclusions
Overall, the findings indicated that greater adherence to PDP was negatively associated with the odds of PEW. Additionally, the results showed no association between PDP and the odds of sarcopenia. Further studies are needed to support these findings.
Similar content being viewed by others


Introduction
Chronic kidney disease (CKD) is defined by structural abnormalities in nephrons, the loss of functional nephrons, and impaired renal excretory function [1]. Hypertension and diabetes are important risk factors for this disease [2], which mainly occurs in people over 65 [3]. CKD causes complications such as anemia, cachexia, fatigue, anorexia, and nausea [4].
Protein-energy wasting (PEW) is a condition characterized by metabolic and nutritional disorders in CKD patients, where body energy reserves and systemic protein are simultaneously lost [5]. The cause of PEW are related to decreased appetite, a hypercatabolic state, autoimmune conditions, and systemic inflammation [6]. PEW is one of the most powerful predictors of mortality in patients with CKD [7]. The prevalence of this disorder increases as kidney function decreases. In stages 1 to 2, its prevalence is less than 2% [8, 9]; in stages 3 to 5, its prevalence increases to 11 to 46% [9,10,11,12].
Sarcopenia is a decrease in muscle mass that reduces the quality of life by impairing physical performance [13]. In CKD, sarcopenia can occur due to increased catabolism and decreased muscle synthesis, resulting in a negative balance of protein homeostasis [14]. The decrease in muscle synthesis in CKD is caused by reduced expression of myogenic regulatory factors, decrease cell activation, and consequently, impaired regeneration [15]. This disorder in CKD patients is associated with increased fracture risk, hospitalization, and mortality [14].
In CKD patients, whose probability of death is high, interventions to improve nutritional status and correct or prevent sarcopenia and PEW can be life-saving [16]. It has been shown that plant-based diets, which are low in animal products and high in plant foods, may benefit kidney health [17]. A pro-vegetarian dietary pattern (PDP) is a gentle and progressive approach to vegetarianism [18] and is rich in whole grains, vegetables, and fruits [19]. This dietary pattern contains sufficient micronutrients and bioactive phytochemicals [20]. The role of this dietary pattern in reducing the risk of cardiometabolic diseases [21], breast cancer [19], and cardiovascular mortality [22] has been studied. However, limited research has been conducted on the relationship between this dietary pattern and the risk of CKD. One study demonstrated that PDP reduces certain metabolites related to the incidence of CKD, suggesting that plant-based diets could reduce CKD incidence by controlling glycemia, reducing inflammation, and preventing adiposity [17]. Another study revealed that a pro-vegetarian diet reduces the risk of CKD [23].
According to the studies mentioned above, the PDP can have a favorable effect on CKD. To our knowledge, no study has examined the association between PDP and the risk of PEW and sarcopenia in patients with CKD. If this dietary pattern can affect these two indicators, following it could decrease the odds of death in CKD patients.
Methods
Study population
The present cross-sectional study was conducted on kidney disease patients referred to Imam Reza and Motahari clinics between January and October 2022 in Shiraz (Fars province of Iran). Based on the sample size formula for estimating proportions and utilizing statistical software, the necessary sample size has been calculated as 97. This calculation was made with an alpha level (α) of 0.05, a proportion (p) of 0.5, and a margin of error (d) of 0.1. Considering a potential dropout rate of 12%, the final sample size was determined to be 109 patients. This calculation adheres to guidelines that suggest utilizing an expected prevalence of 50% in cases where the actual prevalence is unknown [24,25,26].
Based on inclusion and exclusion criteria, 109 patients with glomerular filtration rate (GFR) less than 60 mL/min/173m2, diagnosed by physicians, aged over 18 years, without cognitive problems, and willing to participate in the study were included in the present cross-sectional research. The GFR is calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation as follow:
(Scr is the serum creatinine (mg/dL), κ is 0.7 for females and 0.9 for males, α is -0.329 for females and − 0.411 for males, min indicates the minimum of Scr/κ or 1, and max indicates the maximum of Scr/κ or 1) [27, 28].
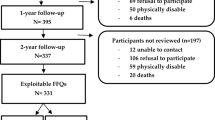
Also, participants on dialysis, with heart failure, active infection, liver cirrhosis and those who had a daily caloric intake of 800 or ≥ 4200 kcal for men and ≤ 500 or ≥ 3500 kcal for women (Numerous other studies have utilized these cut points for defining plausible energy intakes [29,30,31]), as well as those who answered less than 60% of the food frequency questionnaire (FFQ), were excluded (Fig. 1).

Study flow diagram
Physical evaluation, biological sampling, medical, nutritional, and general information were conducted at the beginning of the study by experts. Some details of the present study have been previously published [32, 33]. The Medical Research and Ethics Committee of Shiraz University of Medical Science approved this study (IR.SUMS.SCHEANUT.REC.1400.087).
Data collection
Muscle mass and fat percentage were assessed by bioelectrical impedance analysis (BIA) (IN BODY-S10). Weight was measured using the Omron BF511 scale (without shoes and minimal clothing, accurate to 100 g). Mid-arm circumference (MAC) and height were measured using a non-stretchable tape (accuracy of 0.5 cm). Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Additionally, after a 12–14 h fast according to the study protocol, a 5 mL blood sample was collected from all participants for evaluation of albumin, creatinine, and other biochemical variables. Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ), which has been previously validated [34].
Sarcopenia diagnosis
Low muscle mass, low muscle strength, and/or low muscle function are considered for sarcopenia diagnosis according to the Asian Working Group for Sarcopenia (AWGS) guideline. Muscle strength was assessed using a dynamometer to measure handgrip strength (HGS). Muscle and fat mass were measured using BIA. Muscle function was evaluated through physical performance using the 5-time chair stand test and gait speed (walking speed over 6 m). Also, a skeletal muscle mass index (SMI) of less than 7 kg/m2 for men and 5.7 kg/m2 for women, calculated as appendicular skeletal muscle mass (ASM) divided by the squared height (meters), we used to confirm sarcopenia. Moreover, muscle strength less than 28 kg for men and 18 for women and/or low physical performance (5-time chair stand test ≥ 12 s or gait speed less than 1 m/s) were considered criteria to confirm the diagnosis of sarcopenia [35, 36].
PEW diagnosis
PEW was diagnosed according to the criteria set by the International Society of Renal Nutrition and Metabolism (ISRNM). The diagnosis includes four categories recommended by ISRNM: low protein intake (dietary protein intake (DPI) less than 0.6 g/kg/day), low body mass (body mass index (BMI) less than 23 kg/m2), biochemical parameter (serum albumin less than 3.8 g/dL), and decreased muscle mass (24-hour urine creatinine excretion (UCE): lower quartile based on sex). Patients with less than 500 mL/day of 24 h urine were excluded for concerns regarding urine collection errors. Diagnosis of PEW required three or more of these indicators to be present [9].
Dietary assessment and food grouping
The participants’ dietary intake was assessed using a 168-item semi-quantitative FFQ, which has been validated for the Iranian population [37]. A trained dietician recorded the portion sizes and frequencies of food items based on daily, weekly, monthly or yearly intake. To facilitate estimation of food portions, participants were provided with a set of household measurements (such as plates, bowls, tablespoons, teaspoons, glasses, and cups) and a validated food album [38].
Upon completion of the FFQ, all food items’ portion sizes were converted to gram. These values were then multiplied by the frequency of daily intake to determine the amount of each item was consumed. The energy values of foods were obtained from the nutrient composition databases of Iranian foods [39] and the United States Department of Agriculture (USDA) Food Composition Data. Average energy and nutrient intakes were calculated using Nutritionist IV for Iranians software (version 7.0; N-Squared Computing, Salem, OR, USA).
For the calculation of the PDP index, plant and animal sources of food sources were categorized into 12 subgroups. Plant-based food items were classified into 7 categories (cereals, fruits, vegetables, olive oil, potatoes, nuts, and legumes), while animal-based foods were grouped into 5 categories (meat products, fish, dairy products, eggs, and animal fats).
Next, the intake of all 12 categories was converted into quantiles. Subsequently, the quantiles of animal-based food groups were reversed, assigning 5 points to the first quantile, 4 points to the second, 3 points to the third, 2 points to the fourth, and 1 point to the fifth.
To determine the total PDP score, the reversed quintile values of animal foods were summed with the quintile values of plant foods. This scoring system resulted in PDP scores ranging from 12 to 60, with higher scores indicating great adherence to PDP scores [18, 40].
Finally, the adherence scores were categorized into three classes: less than 32 (low adherence), 32–38 (moderate adherence), and more than 39 (high adherence).
Statistical analysis
In the study, parametric continuous variables were described using mean and standard deviation (SD), while median (interquartile range (IQR)) for non-parametric continuous varia and percentage was used for categorical variables. Baseline characteristics of the study participants based on the PDP tertiles were presented as percentage or median (IQR) and mean ± SD for categorical and continuous variables, respectively.
The association between PDP and the odds ratio (OR) and 95% confidence intervals (CIs) for sarcopenia and PEW was assessed using logistic regression in both crude and adjusted models. The final model included adjustments for age, sex, physical activity, fat and energy intake. SPSS software (version 26) was used for all statistical analyses in this study. Figures were created using R software (version 3.0.2). A significance level of p-value less than 0.05 was used to determine statistical significance.
Results
Based on Table 1, significant differences were observed among PDP tertiles for several variables: PEW (p-value = 0.034), smoking status (p-value = 0.019), alanine transaminase (ALT) level (p-value = 0.019), bicarbonate (HCO3) level (P = 0.016), and the total score of PDP (p-value < 0.001).
Macronutrients and food group’s consumption across the tertile of PDP are presented in Figs. 2 and 3, respectively. According to Fig. 2, the intake of protein, carbohydrates, saturated fatty acids (SFA), monounsaturated fatty acids (MUFA), and polyunsaturated fatty acids (PUFA) did not show significant differences among the tertiles of PDP (p-value ˃ 0.05 for all).

The contribution of macronutrient intake based on the PDP tertile

Participants’ food group intake across the tertiles of PDP
In contrast, Fig. 3 indicates that compared to the first tertile, participants in the last tertile of the PDP index had significantly higher consumption of fruits, vegetables, nuts, and olive oils (p-value < 0.001).
In Table 2, participants macro and micronutrient intake is presented based on PDP tertiles. According to the table, in the highest tertile of the PDP index, the intake of several nutrients was significantly higher compared to the first tertile (fiber (p-value < 0.001), MUFA (p-value = 0.010), PUFA (p-value = 0.003), potassium (p-value < 0.001), iron (p-value = 0.035), magnesium (p-value = 0.006), calcium (p-value = 0.043), vitamin A (p-value < 0.001), vitamin K (p-value < 0.001), vitamin E (p-value < 0.001), vitamin C (p-value < 0.001), vitamin B1 (p-value = 0.003), vitamin B6 (p-value = 0.002) and vitamin B9 (p-value < 0.001)).
In the multivariate analysis (Table 3), the PDP was found to be significantly associated with a lower risk of PEW in the second tertile compared to the first one in the crude model (OR = 0.225; CI: 0.055–0.915; p-value = 0.037). After adjusting for potential confounders, lower significant odds of PEW were observed in the second and last tertiles of PDP compared to the first (T2: OR = 0.194; CI: 0.039–0.962; p-value = 0.045, and T3: OR = 0.168; CI: 0.030–0.950; p-value = 0.044). In contrast, no significant relationship was observed between PDP and the odds of sarcopenia (p-value ˃ 0.05).
Discussion
The present study’s findings showed that adherence to the PDP in adults with CKD was associated with lower odds of PEW. This association was not found between PDP adherence and the odds of sarcopenia. The results support a reduction in the likelihood of PEW associated with adherence to the PDP, which may not reflect a completely plant-based diet, but rather a diet that focuses on plant consumption, some animal products, and the restriction of sweetened processed foods and beverages.
PDP is a novel dietary pattern that may significantly impact public health in the future, although it has yet to be adequately studied [41]. New evidence suggests that dietary patterns compatible with vegetarianism, such as PDP, can be beneficial for CKD patients by delaying the progression of the disease to the end-stage of kidney disease (ESKD) and preventing its complications [42]. Delaying the progression of CKD benefits both the healthcare system and the patient.
We found an inverse association between adherence to PDP and the likelihood of PEW in CKD patients. To our knowledge, the association between these two indicators has not been investigated in other studies, making comparisons with our results difficult. However, it has been shown that uremic toxins derived from the gut can contribute to PEW by causing insulin resistance, oxidative stress, and inflammation. Bacterial activity produces these toxins from aromatic amino acids [43,44,45]. Studies have shown that these toxins are higher in non-vegetarian patients than in vegetarian patients [46, 47]. A vegetarian diet may reduce the concentration of these toxins due to its fiber contents, possibly by reducing the time of food transit in the intestine and thus decreasing the production and absorption of these toxins, or altering the activity and composition of the intestinal microbiome [48, 49].
Another factor contributing to PEW in CKD patients is acidosis [50]. Plant foods have lower acid load than animal foods [50], and higher protein intake from plant foods is associated with greater bicarbonate intake [51]. Despite the mentioned benefits of plant protein intake, nutrient-based dietary guidelines recommend animal protein foods to prevent PEW in kidney patients [52] as animal proteins have higher quality and bioavailability [50]. However, animal proteins also have a higher acid load than plant proteins and can increase uremic toxins derived from the gut more than plant proteins [50]. Therefore, as mentioned above, in PDP, which is not a completely plant-based diet and includes some animal products, may effectively reduce PEW through these mechanisms.
The results of the present study indicated no association between PDP and sarcopenia. Sarcopenia, a prevalent condition in patients with CKD, is diagnosed based on criteria involving low muscle mass and impaired physical performance [53, 54]. In CKD, sarcopenia can arise from heightened protein breakdown due to the disease process and dialysis treatment [55]. Additionally, factors such as insulin resistance, hormonal imbalance, chronic inflammation, anorexia, and increased protein catabolism due to hyperparathyroidism, or activation of the renin-angiotensin system contribute to its development [14].
As kidney function declines, there is often a gradual reduction in protein intake [56]. Recommendations for protein intake vary depending on CKD stage and risk of ESKD. High-risk CKD patients (stages 4 and 5) are typically advised to limit protein intake to 0.8 g per kilogram per day, whereas those with lower risk (stage 3) may not need to restrict protein intake (< 1.5 g per kilogram per day) unless they have significant proteinuria [57, 58].
Research indicates that vegans and lacto-ovo vegetarians generally consume less protein compared to meat-eaters [59], and some vegetarian diets may compromise protein intake [60]. Furthermore, proteins from plant-based sources often have lower bioavailability compared to animal proteins. Patients with CKD may naturally decreases their protein intake due to dietary restrictions related to their condition.
Therefore, while the PDP encourages the consumption of plant-based foods and limits animal protein intake, this dietary pattern may not effectively reduce the risk of sarcopenia in CKD patients, particularly if it results in insufficient protein intake.
Among the weaknesses of the study, several points should be noted. First, as the first investigation into the association between PDP and the likelihood of sarcopenia and PEW, comparison with similar studies were not feasible. Secondly, due to limited access to data on inflammatory factors relevant to CVD complications, the study did not explore PDP impact on inflammation. However, the study small sample size might have contributed to the inability to establish a significant association between PDP and the risk of sarcopenia.
On the other hand, the study has notable strengths. It contributes novelty to the field by addressing this association for the first time and includes rigorous adjustment for important confounding factors.
Conclusions
Overall, the findings indicated that greater adherence to PDP was negatively associated with the odds of PEW. Additionally, the results showed no association between PDP and the odds of sarcopenia. Further studies are needed to substantiate these findings.
Data availability
No datasets were generated or analysed during the current study.
References
Romagnani P, Remuzzi G, Glassock R, Levin A, Jager KJ, Tonelli M, Massy Z, Wanner C, Anders H-J. Chronic kidney disease. Nat Reviews Disease Primers. 2017;3(1):1–24.
Levey AS, Astor BC, Stevens LA, Coresh J. Chronic kidney disease, diabetes, and hypertension: what’s in a name? Kidney Int. 2010;78(1):19–22.
Centers for Disease Control Prevention. Chronic kidney disease in the United States, 2019. Atlanta, GA: US Department of Health and Human Services. Centers Disease Control Prev 2019, 3.
Bello AK, Alrukhaimi M, Ashuntantang GE, Basnet S, Rotter RC, Douthat WG, Kazancioglu R, Köttgen A, Nangaku M, Powe NR. Complications of chronic kidney disease: current state, knowledge gaps, and strategy for action. Kidney Int Supplements. 2017;7(2):122–9.
Hanna RM, Ghobry L, Wassef O, Rhee CM, Kalantar-Zadeh K. A practical approach to nutrition, protein-energy wasting, Sarcopenia, and cachexia in patients with chronic kidney disease. Blood Purif. 2020;49(1–2):202–11.
Obi Y, Qader H, Kovesdy CP, Kalantar-Zadeh K. Latest consensus and update on protein energy-wasting in chronic kidney disease. Curr Opin Clin Nutr Metab Care. 2015;18(3):254.
Koppe L, Fouque D, Kalantar-Zadeh K. Kidney cachexia or protein‐energy wasting in chronic kidney disease: facts and numbers. Volume 10. Wiley Online Library; 2019. pp. 479–84.
Dai L, Mukai H, Lindholm B, Heimbürger O, Barany P, Stenvinkel P, Qureshi AR. Clinical global assessment of nutritional status as predictor of mortality in chronic kidney disease patients. PLoS ONE. 2017;12(12):e0186659.
Hyun YY, Lee K-B, Han SH, Kim YH, Kim Y-S, Lee SW, Oh YK, Chae DW, Ahn C. Nutritional status in adults with predialysis chronic kidney disease: KNOW-CKD study. J Korean Med Sci. 2017;32(2):257–63.
Cupisti A, D’Alessandro C, Morelli E, Rizza GM, Galetta F, Franzoni F, Barsotti G. Nutritional status and dietary manipulation in predialysis chronic renal failure patients. J Ren Nutr. 2004;14(3):127–33.
Campbell KL, Ash S, Bauer JD, Davies PS. Evaluation of nutrition assessment tools compared with body cell mass for the assessment of malnutrition in chronic kidney disease. J Ren Nutr. 2007;17(3):189–95.
Pérez-Torres A, Garcia MEG, San José-Valiente B, Rubio MAB, Diez OC, López-Sobaler AM, Selgas R. Protein-energy wasting syndrome in advanced chronic kidney disease: prevalence and specific clinical characteristics. Nefrología (English Edition). 2018;38(2):141–51.
Hara H, Nakamura Y, Hatano M, Iwashita T, Shimizu T, Ogawa T, Kanozawa K, Hasegawa H. Protein energy wasting and sarcopenia in dialysis patients. Recent Adv Dialysis Therapy Japan. 2018;196:243–9.
Moorthi RN, Avin KG. Clinical relevance of Sarcopenia in chronic kidney disease. Curr Opin Nephrol Hypertens 2017, 26(3):219.
Avin KG, Chen NX, Organ JM, Zarse C, O’Neill K, Conway RG, Konrad RJ, Bacallao RL, Allen MR, Moe SM. Skeletal muscle regeneration and oxidative stress are altered in chronic kidney disease. PLoS ONE. 2016;11(8):e0159411.
Jadeja YP, Kher V. Protein energy wasting in chronic kidney disease: an update with focus on nutritional interventions to improve outcomes. Indian J Endocrinol Metabol. 2012;16(2):246.
Kim H, Yu B, Li X, Wong KE, Boerwinkle E, Seidelmann SB, Levey AS, Rhee EP, Coresh J, Rebholz CM. Serum metabolomic signatures of plant-based diets and incident chronic kidney disease. Am J Clin Nutr. 2022;116(1):151–64.
Martínez-González MA, Sánchez-Tainta A, Corella D, Salas-Salvado J, Ros E, Arós F, Gómez-Gracia E, Fiol M, Lamuela-Raventós RM, Schröder H. A provegetarian food pattern and reduction in total mortality in the Prevención Con Dieta Mediterránea (PREDIMED) study. Am J Clin Nutr. 2014;100(suppl1):S320–8.
Romanos-Nanclares A, Toledo E, Sánchez-Bayona R, Sánchez-Quesada C, Martínez-González MÁ, Gea A. Healthful and unhealthful provegetarian food patterns and the incidence of breast cancer: results from a Mediterranean cohort. Nutrition. 2020;79:110884.
Liu RH. Health benefits of fruit and vegetables are from additive and synergistic combinations of phytochemicals. Am J Clin Nutr. 2003;78(3):S517–20.
Oncina-Canovas A, Vioque J, Gonzalez-Palacios S, Martínez-González MÁ, Salas-Salvado J, Corella D, Zomeño D, Martínez JA, Alonso-Gomez AM, Wärnberg J. Pro-vegetarian food patterns and cardiometabolic risk in the PREDIMED-Plus study: a cross-sectional baseline analysis. Eur J Nutr 2022:1–16.
Lassale C, Beulens J, Van der Schouw Y, Roswall N, Weiderpass E, Romaguera D, Riboli E, Tzoulaki I. A pro-vegetarian food pattern and cardiovascular mortality in the epic study. Circulation. 2015;131(suppl1):A16–16.
Kim H. Plant-based diet indices and the risk of chronic kidney disease, cardiovascular morbidity and mortality in American adults. Johns Hopkins University; 2019.
Daniel WW, Cross CL. Biostatistics: a foundation for analysis in the health sciences. Wiley; 2018.
Draugalis JR, Plaza CM. Best practices for survey research reports revisited: implications of target population, probability sampling, and response rate. Am J Pharm Educ. 2009;73(8):142.
Lwanga SK, Lemeshow S, Organization WH. Sample size determination in health studies: a practical manual. World Health Organization; 1991.
Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–12.
Park S, Jeong TD. Estimated glomerular filtration Rates Show Minor but significant differences between the single and Subgroup Creatinine-based chronic kidney disease epidemiology collaboration equations. Ann Lab Med. 2019;39(2):205–8.
Turner-McGrievy GM, Davidson CR, Wilcox S. Does the type of weight loss diet affect who participates in a behavioral weight loss intervention? A comparison of participants for a plant-based diet versus a standard diet trial. Appetite. 2014;73:156–62.
Bowen ME, Cavanaugh KL, Wolff K, Davis D, Gregory B, Rothman RL. Numeracy and dietary intake in patients with type 2 diabetes. Diabetes Educ. 2013;39(2):240–7.
Du H, van der Bakel AD, van der Kallen MM, Blaak CJ, van Greevenbroek EE, Jansen MM, Nijpels EH, Stehouwer G, Dekker CD. Glycemic index and glycemic load in relation to food and nutrient intake and metabolic risk factors in a Dutch population. Am J Clin Nutr. 2008;87(3):655–61.
Shateri Z, Eskandarzadeh S, Nouri M, Jahromi SE, Mansouri F, Babajafari S. The role of ultra-processed food consumption in protein-energy wasting and Sarcopenia development in patients with chronic kidney diseases. BMC Nephrol. 2024;25(1):4.
Mansouri F, Jafari F, Ranjbar S et al. Dietary inflammatory index could increase the risk of sarcopenia in patients with chronic kidney disease. Sci Rep. 2024;14:15284. https://doi.org/10.1038/s41598-024-65340-6.
Moghaddam MB, Aghdam FB, Jafarabadi MA, Allahverdipour H, Nikookheslat SD, Safarpour S. The Iranian version of International Physical Activity Questionnaire (IPAQ) in Iran: content and construct validity, factor structure, internal consistency and stability. World Appl Sci J. 2012;18(8):1073–80.
Chen L-K, Liu L-K, Woo J, Assantachai P, Auyeung T-W, Bahyah KS, Chou M-Y, Chen L-Y, Hsu P-S, Krairit O. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101.
Mahmoodi M, Hejazi N, Bagheri Z, Nasimi N, Clark CC, Moosavi M, Dabbaghmanesh MH, Mazloom Z. Validation of the Persian version of the Sarcopenia-specific quality of life questionnaire (SarQoL®-IR). Aging Clin Exp Res. 2023;35(1):137–45.
Mirmiran P, Esfahani FH, Mehrabi Y, Hedayati M, Azizi F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62.
Ghaffarpour M, Houshiar-Rad A, Kianfar H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran: Nashre Olume Keshavarzy. 1999;7(213):42–58.
Azar M, Sarkisian E. Food composition table of Iran. Tehran: Natl Nutr Food Res Inst Shaheed Beheshti Univ 1980, 65.
Hosseini Y, Hadi Sichani P, Moslemi E, Nouri M, Rajabzadeh-dehkordi M, Jalali S, Heidari Z, Shateri Z, Rashidkhani B. Pro-vegetarian dietary pattern and risk of breast cancer: a case–control study. Breast Cancer Res Treat. 2024;205(2):395–402.
Oncina-Cánovas A, González-Palacios S, Notario-Barandiaran L, Torres-Collado L, Signes-Pastor A, de-Madaria E, Santibañez M, García-de la Hera M, Vioque J. Adherence to pro-vegetarian food patterns and risk of Oesophagus, stomach, and pancreas cancers: a Multi case–control study (the PANESOES Study). Nutrients. 2022;14(24):5288.
Banerjee T, Carrero JJ, McCulloch C, Burrows NR, Siegel KR, Morgenstern H, Saran R, Powe NR. Dietary factors and prevention: risk of end-stage kidney disease by fruit and vegetable consumption. Am J Nephrol. 2021;52(5):356–67.
Koppe L, Pillon NJ, Vella RE, Croze ML, Pelletier CC, Chambert S, Massy Z, Glorieux G, Vanholder R, Dugenet Y. p-Cresyl sulfate promotes insulin resistance associated with CKD. J Am Soc Nephrol. 2013;24(1):88–99.
Vanholder R, Schepers E, Pletinck A, Nagler EV, Glorieux G. The uremic toxicity of indoxyl sulfate and p-cresyl sulfate: a systematic review. J Am Soc Nephrol. 2014;25(9):1897–907.
Fernandez-Prado R, Esteras R, Perez-Gomez MV, Gracia-Iguacel C, Gonzalez-Parra E, Sanz AB, Ortiz A. Sanchez-Niño MD: nutrients turned into toxins: microbiota modulation of nutrient properties in chronic kidney disease. Nutrients. 2017;9(5):489.
Patel KP, Luo FJ-G, Plummer NS, Hostetter TH, Meyer TW. The production of p-cresol sulfate and indoxyl sulfate in vegetarians versus omnivores. Clin J Am Soc Nephrol. 2012;7(6):982–8.
Kandouz S, Mohamed AS, Zheng Y, Sandeman S, Davenport A. Reduced protein bound uraemic toxins in vegetarian kidney failure patients treated by haemodiafiltration. Hemodial Int. 2016;20(4):610–7.
Sirich TL, Plummer NS, Gardner CD, Hostetter TH, Meyer TW. Effect of increasing dietary fiber on plasma levels of colon-derived solutes in hemodialysis patients. Clin J Am Soc Nephrol. 2014;9(9):1603–10.
Cummings J, Hill M, Bone E, Branch W, Jenkins D. The effect of meat protein and dietary fiber on colonic function and metabolism II. Bacterial metabolites in feces and urine. Am J Clin Nutr. 1979;32(10):2094–101.
St-Jules DE, Goldfarb DS, Popp CJ, Pompeii ML, Liebman SE. Managing protein‐energy wasting in hemodialysis patients: a comparison of animal‐and plant‐based protein foods. Seminars in Dialysis: 2019. Wiley Online Library; 2019. pp. 41–6.
Scialla JJ, Appel LJ, Wolf M, Yang W, Zhang X, Sozio SM, Miller ER III, Bazzano LA, Cuevas M, Glenn MJ. Plant protein intake is associated with fibroblast growth factor 23 and serum bicarbonate levels in patients with chronic kidney disease: the chronic renal insufficiency cohort study. J Ren Nutr. 2012;22(4):379–88. e371.
Dietary guidelines for adults starting on hemodialysis. National Kidney Foundation Web site. www.kidney.org/atoz/content/dietary hemodialysis. Published 2015. Accessed December 21, 2017.
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel J-P, Rolland Y, Schneider SM. Sarcopenia: European consensus on definition and diagnosisReport of the European Working Group on Sarcopenia in older PeopleA. J. Cruz-Gentoft et al. Age Ageing. 2010;39(4):412–23.
Muscaritoli M, Anker S, Argilés J, Aversa Z, Bauer J, Biolo G, Boirie Y, Bosaeus I, Cederholm T, Costelli P. Consensus definition of Sarcopenia, cachexia and pre-cachexia: joint document elaborated by Special Interest groups (SIG)cachexia-anorexia in chronic wasting diseases and nutrition in geriatrics. Clin Nutr. 2010;29(2):154–9.
Sabatino A, Cuppari L, Stenvinkel P, Lindholm B, Avesani CM. Sarcopenia in chronic kidney disease: what have we learned so far? J Nephrol. 2021;34(4):1347–72.
Ikizler TA, Greene JH, Wingard RL, Parker RA, Hakim RM. Spontaneous dietary protein intake during progression of chronic renal failure. J Am Soc Nephrol. 1995;6(5):1386–91.
Houston DK, Nicklas BJ, Ding J, Harris TB, Tylavsky FA, Newman AB, Lee JS, Sahyoun NR, Visser M, Kritchevsky SB. Dietary protein intake is associated with lean mass change in older, community-dwelling adults: the Health, Aging, and body composition (Health ABC) Study. Am J Clin Nutr. 2008;87(1):150–5.
Isaka Y. Optimal protein intake in pre-dialysis chronic kidney disease patients with Sarcopenia: an overview. Nutrients. 2021;13(4):1205.
Davey GK, Spencer EA, Appleby PN, Allen NE, Knox KH, Key TJ. EPIC–Oxford: lifestyle characteristics and nutrient intakes in a cohort of 33 883 meat-eaters and 31 546 non meat-eaters in the UK. Public Health Nutr. 2003;6(3):259–68.
Tucker KL. Vegetarian diets and bone status. Am J Clin Nutr. 2014;100(suppl1):S329–35.
Acknowledgements
not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
F.M, Z.S, M.M and M.N; Contributed to writing the first draft. M.N; Contributed to all data, statistical analysis, and interpretation of data. S.E.J and S.B; Contributed to the research concept, supervised the work, and revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
this study was approved by the medical research and ethics committee of Shiraz University of Medical Science and the informed consents were completed by all participants. Also, we confirmed all the methods included in this study are in accordance with the Declaration of Helsinki.
Consent for publication
not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mansouri, F., Shateri, Z., Jahromi, S.E. et al. Association between pro-vegetarian dietary pattern and the risk of protein-energy wasting and sarcopenia in patients with chronic kidney disease. J Health Popul Nutr 43, 110 (2024). https://doi.org/10.1186/s41043-024-00606-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-024-00606-3