
Abstract
Background and objective
Healthy diets and diets rich in phytochemicals can have health-promoting benefits in prostate cancer. Therefore, this study aimed to explore the possible association between Healthy Diet Indicator (HDI) and Phytochemical Index (PI) with prostate cancer odds ratio.
Methods
This is a case-control study conducted in Shiraz, Iran, involving 62 newly diagnosed prostate cancer cases and 63 hospital-based controls. The study collected demographic and anthropometric data, as well as dietary intake information via a semi-quantitative food frequency questionnaire. Logistic regression models were employed to evaluate the association between HDI and PI with prostate cancer.
Results
The study included 120 participants and found that individuals with higher HDI and PI scores had a lower odds ratio of prostate cancer (HDI: odds ratio (OR): 0.322 – confidence interval (CI) 95%: 0.14–0.700 - PI: OR: 0.426 - CI 95%: 0.204–0.888). After adjusting for potential confounders, a lower odds ratio of prostate cancer was observed specifically among those with higher HDI scores (OR: 0.376 - CI 95%: 0.163–0.868).
Conclusion
The findings of the present study suggest that adopting healthier dietary habits rich in dietary phytochemicals could be effective in preventing and halting the progression of prostate cancer.
Similar content being viewed by others


Introduction
The prevalence of chronic diseases has significantly increased due to the rising trend of sedentary lifestyles, reduced physical activity, and dietary modifications in recent decades [1]. Chronic diseases contribute to increased mortality rates [2]. Prostate cancer, as a chronic disease, is the second most frequent malignancy in men worldwide, with 1,276,106 new cases and 358,989 deaths (3.8% of all deaths caused by cancer in men) in 2018, following lung cancer [3]. The age-standardized rate of prostate cancer in Iran is 9.11 per 100,000 [4]. Previous studies have shown that herbal and complementary medicine, due to their natural compounds and antioxidant content, have beneficial effects in the prevention and treatment of chronic diseases [2, 5].
Recent findings underscore the importance of focusing on the combined effects of foods as dietary patterns [6]. These patterns can significantly influence the odds ratio of chronic diseases such as cardiovascular diseases, diabetes, and cancer [7]. For instance, the Western dietary pattern, high in saturated fatty acids, processed meat, refined grains, salt, and sugar, and low in fruits and vegetables, is associated with an increased odds ratio of chronic disorders. Therefore, recognizing the importance role of diet in preventing and managing chronic disorders, the World Health Organization (WHO) recommends dietary modifications such as balanced energy intake, limiting saturated and trans fatty acids, increasing fruit and vegetable consumption, and reducing salt and sugar [7,8,9].
Phytochemicals such as organosulfur, isoprenoid, and phenolic compounds are non-nutritive bioactive compounds [6]. Diets rich in phytochemicals have protective effects against chronic disorders due to their antioxidant and anti-inflammatory effects [6]. Therefore, McCarty proposed the Dietary Phytochemical Index (PI) as the percentage of calories derived from phytochemical-rich foods because of the health-promoting effects of phytochemicals [6, 10]. Recent findings have emphasized the relationship between the dietary PI and health indicators such as oxidative stress, inflammation, and cancer [6, 11, 12]. It has been demonstrated that phytochemicals exert anti-cancer effects by inducing apoptosis, reducing cell proliferation, and inhibiting angiogenesis [13, 14].
The Healthy Diet Index (HDI) is an index proposed by Huijbregts et al. [15]. This index is based on the WHO dietary guidelines for the prevention of chronic diseases and encompasses 9 nutrients and food groups: saturated fatty acids (SFA), unsaturated fatty acids, protein, carbohydrates, fiber, fruits and vegetables, pulses, nuts, seeds, and cholesterol [15].
To our knowledge, there has been no study in this field, especially in Iranian men. The purpose of this study was to investigate the association between the Healthy Diet Indicator (HDI) and the PI and the odds ratio of prostate cancer in Iranian men.
Methods and materials
Study design and participants
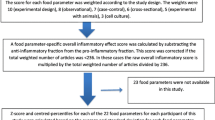
This case-control study was conducted from April until September 2015 at two main hospitals in Shiraz, Iran, which were referral centers for urological disorders. The study sample size calculated based on the study by Askari et al. based on α error = 0.05, β error = 0.3, and anticipated odds ratio (OR) of 0.4 [16]. A total of 125 individuals participated, comprising 62 cases and 63 controls. Medical records of the patients were obtained from the cancer registry database of hospitals, which are the primary referral centers in southern Iran for cancer and other diseases (Fig. 1) [17, 18].

Study flowchart
The inclusion criteria for the case group included patients diagnosed with prostate cancer within the past month and eligible for prostatectomy. The control group consisted of healthy participants or patients with non-cancerous and acute illnesses. Controls were selected from individuals with specific conditions: 8 with kidney issues, 9 with gastrointestinal problems, 5 with neurological disorders, 21 with eye-related ailments, and 20 with ear, nose, and throat (ENT) disorders. Controls were chosen at the same time and from the same hospitals as the cases. Exclusion criteria for both groups included daily total energy intake exceeding 4200 kcal/d or less than 800 kcal/d, and incomplete responses (less than 70 items) on the food frequency questionnaire (FFQ) [19]. The study protocol was approved by the Ethics Committee of Shiraz University of Medical Sciences in Iran (IR.SUMS.REC.1394.S438), following the guidelines of the Declaration of Helsinki. Written informed consent was obtained from all participants. Some details of the present study have been published previously [20, 21].
Demographic and anthropometric assessments
Lifestyle and demographic information such as age, education, ethnicity, physical activity, and smoking status were assessed through face-to-face interviews and with questionnaire. Anthropometric indicators were measured by standard protocol. Weight, measured without shoes in minimal clothing, determined with the precision of 0.1 kg using a digital scale (Glamor BS-801, Hitachi, China). Height was measured with an accuracy of 0.1 cm using a rigid tape measure, with participants standing against a wall without shoes, ensuring heels and head were firmly against the wall.
Dietary intake assessments
The dietary intake was assessed using a reliable and valid semi-quantitative FFQ [22]. Participants reported their food frequency based on portion size categorized as follow: “never or less than one time in a month”, “1–3 times in a month”, “one time in a week”, “2–4 times in a week”, “5–6 times in a week”, “one time in a day”, “2 or 3 times in a day”, “4 or 5 times in a day”, and “6 times or more in a day”. Portion sizes were classified as small (half the mean of consumption or less), medium (equal to the mean of consumption), and large (one and a half times the mean of consumption of more). Borland Delphi Professional, Visual Basic 2008, version 7.0 software was utilized for analyzing the FFQs. Additionally, Nutritionist 4 software was employed to convert foods into nutrients data.
The HDI was first described by Huijbregts et al. [15]. It consists of nine components scored according to WHO healthy diet recommendations. Each component, including energy intake SFA, monounsaturated fatty acids (MUFA), polyunsaturated fatty acids (PUFA), protein, and carbohydrates, cholesterol intake, fiber, fruits and vegetables intake, and pulses, nuts and seeds intake, was dichotomized into adhering to or not adhering to the recommendations. A score of 1 was assigned if a participant’s diet met the recommended criteria for a component, otherwise, a score of 0 was given (see Table 1). Therefore, the maximum score is 9 [23].
The PI was calculated using the method developed by McCarty [10]: [PI= (daily energy obtained from foods phytochemicals- rich foods (kcal) / total daily energy intake (kcal)) × 100]. Initially, the energy intake from each phytochemical-rich foods item was calculated based on their total gram intake. Subsequently, the total energy intake from phytochemical-rich foods was computed. These foods included whole grains, legumes, nuts, olives and olive oil, soy products, seeds tea, coffee, and spices. Natural vegetable and fruit juices, as well as tomato sauces, were categorized within the vegetable and fruit groups due to their phytochemical richness. However, potatoes and pickled vegetables were excluded from the vegetable groups due to their low phytochemicals content. The total PI intake was then categorized as lower and higher than of mean intake.
Statistical analysis
Data analysis was performed using SPSS version 22 software (SPSS Inc. Chicago, IL, USA). The normality of data distribution was assessed using the Kolmogorov-Smirnov test. Independent samples T-test was employed for parametric distributed continuous variables, while the Mann-Whitney test was used for non-parametric distributed variables. Chi-square test was utilized for categorical variables.
The association between HDI and PI with prostate cancer was examined using regression models, adjusting for age, BMI, education and physical activity in the final regression model (adjusted variables were selected based on variables with a P-value < 0.25 as reported in Table 3). A P-value < 0.05 was considered statistically significant.
Results
At first, 125 participants were enrolled in the study (62 in the case and 63 in the control group). During the final analysis, 5 participants were excluded due to incomplete responses on the FFQ (2 from the case and 3 from the control group). Baseline characteristics of the study participants are presented in Table 2. Significant difference were observed between the case and control groups in terms of age (P-value = 0.003), physical activity (P-value = 0.024), total fat intake (P-value = 0.049), SFA (P-value = 0.016), cholesterol intake (P-value = 0.008), total HDI score (P-value<0.001), PI (P-value = 0.005), fruits intake (P-value = 0.006) and vegetable intake (P-value = 0.029).
The association between baseline characteristics of the study population and the odds ratio of prostate cancer is presented in Table 3. According to the table, there was a statistically significant increase in the odds of prostate cancer with each unit increase in age (OR): 1.052– confidence interval (CI) 95%: 1.011–1.095). Additionally, compared to those with lower levels of physical activity, individuals with high level of physical activity showed lower odds of prostate cancer (OR: 0.261 – (CI) 95%: 0.098–0.698).
The association between HDI and PI with the odds ratio of prostate cancer is shown in Table 4. In the crude model, a statistically significant and lower odds ratio of prostate cancer was observed with higher HDI and PI scores compared to lower scores (HDI: OR: 0.322 – CI 95%: 0.148-0.700 - PI: OR: 0.426 - CI 95%: 0.204–0.888). However, after adjusting for potential confounders (age, BMI, education, and physical activity), a statistically significant lower odds ratio of prostate cancer was seen only in those with higher HDI scores (OR: 0.376 - CI 95%: 0.163–0.868).
Discussion
In the current study, the dietary PI showed an inverse association with the odds of prostate cancer. The significant association was only observed in crude analysis but did not in remain significant in the multivariate analysis. Additionally, we found an inverse association between the HDI and the odds ratio of prostate cancer.
It’s crucial to adhere to a high-quality diet to reduce the risk of cancer. For instance, the Healthy Eating Index (HEI) has been associated with a 15% reduction in the odds ratio of cancer [24]. Investigating the beneficial effects of healthy dietary habits, such as the Mediterranean diet, on the odds ratio of prostate cancer involves considering various types of foods within these dietary patterns. High consumption of fruits, vegetables, whole grains and fish, coupled with low intake of red and processed meat, enriched the diet with bioactive molecules known for their antioxidant, anti-inflammatory, and alkalizing properties [25].
Fruits and vegetables, being primary components of healthy dietary patterns, are rich in fiber, micronutrients, and phytochemicals with known as anti-cancer properties [25]. Kolonel et al. demonstrated an inverse relationship between the intake of yellow-green vegetables, cruciferous vegetables, and carrots, and the odds ratio of advanced prostate cancer [26]. A meta-analysis study by Liu et al. further supports this, showing that the consumption of cruciferous vegetables is linked to a reduction in the odds ratio of prostate cancer [27]. Additionally, Allium vegetables, containing sulfur phytochemicals, are known to enhance the immune system, inhibit cell proliferation, induce apoptosis, and changing the activation of androgen-responsive genes [28, 29].
Despite the reported protective effects of vegetables against prostate cancer, the findings of various studies are conflicting [29].
Fruits, vegetables, legumes, and whole grains serve as rich sources of fiber, which has been demonstrated protective effects against various types of cancer [30,31,32,33,34]. The role of gut microbiota is crucial in this regard, as they metabolized dietary fiber into short-chain fatty acids (SCFA), particularly butyrate, which induces cell apoptosis [30]. Furthermore, the consumption of fruits and vegetables provides abundant phytochemicals known for their anti-cancer effects [30]. Recent finding from a meta-analysis of prospective observational studies have also highlighted an inverse relationship between intake of antioxidant phytochemicals or their serum levels and the odds ratio of cancer [35]. Similarly, emerging evidence suggests that phytochemicals and other natural bioactive compounds possess potential protective effects against the occurrence and progression of various cancer [36]. Therefore, phytochemicals are recommended as a complementary strategy for cancer treatment. Plant-based foods rich in phytochemicals exert anti-cancer effects through bioactive compounds such as soluble and insoluble fiber, lignans, sterols, flavonoids, phenolic compounds, and other bioactive metabolites [36].
An inverse association between phytochemical-rich foods with inflammation was reported [37,38,39]. The positive effects of a high intake of in phytochemicals-rich plant foods on the levels of inflammatory markers can be attributed to the inhibitory action of polyphenols on pro-inflammatory enzymes, as well as their role in protecting cells against inflammation and oxidative stress [40]. Polyphenols prevent prostate cancer through the following mechanisms: increasing the activity of antioxidant enzymes (glutathione peroxidase and superoxide dismutase); reducing inflammatory factors such as interleukin-1β, interleukin-6, tumor necrosis factor-alpha, 5-lipogenase, and cyclooxygenase-2 (COX-2); inhibiting of 5α-reductase, and increasing apoptotic factors such as pro-apoptotic caspase-3 protein, and G protein-coupled estrogen receptor 1 (GPER) [41].
Moreover, a high intake of legumes and cereals increases vegetable fiber intake, which has anti-cancer effects by reducing glycemic load, lowering insulin-like growth factor-1 (IGF1) levels, and improving insulin sensitivity [25]. It has been reported that high consumption of leguminous fiber is associated with a reduced odds ratio of prostate cancer [25]. Bosire et al. reported an inverse relationship between the fish component of the alternate Mediterranean diet score and the omega-3 component of the alternate healthy eating index and fatal prostate cancer [42]. A meta-analysis has also shown that fish intake has significantly reduces prostate cancer-specific mortality [43]. These findings are attributed to the high omega-3 content of fish [25]. These findings are attributed to the high omega-3 content in fish, which decreases the expression of COX-2 and inflammatory cytokines [25].
It has also been reported that frequent consumption of whole grains effectively reduces the odds ratio of cancer due to the protective effects of their compounds, such as phytosterols, benzoxanizoids, and alkylresorcinols [30]. On the other hand, adherence to healthy diets, such as the Mediterranean diet, reduces the intake of red and processed meat, thereby decreasing exposure to potential carcinogens such as heterocyclic amines, N-nitroso compounds, and polycyclic aromatic hydrocarbons, which increases odds ratio of cancer [30]. Therefore, designing a balanced diet that includes a variety of plant foods provides high amounts of phytochemicals, vitamins, minerals, and other non-nutrients that have synergistic effects [40].
In the present study, several strengths and weaknesses should be mentioned. This research is the first to investigate the HDI and PI in relation to the odds ratio of prostate cancer in Iranian men. Additionally, a valid and reliable questionnaire was used to assess the dietary intake of the participants.
However, there was a risk of over-reporting and under-reporting in the use of this questionnaire, which is considered a weakness of the study. Moreover, the case-control study design introduced a risk of selection bias, and causality of the association could not be determined. Another limitation of our study was the unavailability of data on family history of prostate cancer and geographical location. These factors could potentially influence the results and should be considered in future research.
Conclusion
In conclusion, the findings of this study indicate that adopting dietary habits favoring healthy diets rich in dietary phytochemicals could be effective in preventing the occurrence and progression of prostate cancer.
Data availability
No datasets were generated or analysed during the current study.
References
Nattagh-Eshtivani E, Gheflati A, Barghchi H, Rahbarinejad P, Hachem K, Shalaby MN, et al. The role of pycnogenol in the control of inflammation and oxidative stress in chronic diseases: molecular aspects. Phytother Res. 2022;36(6):2352–74.
Barghchi H, Dehnavi Z, Nattagh-Eshtivani E, Alwaily ER, Almulla AF, Kareem AK, et al. The effects of Chlorella vulgaris on cardiovascular risk factors: a comprehensive review on putative molecular mechanisms. Biomed Pharmacother. 2023;162:114624.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2018;68(6):394–424.
Hassanipour S, Fathalipour M, Salehiniya H. The incidence of prostate cancer in Iran: a systematic review and meta-analysis. Prostate Int. 2018;6(2):41–5.
Nattagh-Eshtivani E, Pahlavani N, Ranjbar G, Gholizadeh Navashenaq J, Salehi‐Sahlabadi A, Mahmudiono T, et al. Does propolis have any effect on rheumatoid arthritis? A review study. Food Sci Nutr. 2022;10(4):1003–20.
Vasmehjani AA, Darabi Z, Nadjarzadeh A, Mirzaei M, Hosseinzadeh M. The relation between dietary phytochemical index and metabolic syndrome and its components in a large sample of Iranian adults: a population-based study. BMC Public Health. 2021;21(1):1–10.
Cena H, Calder PC. Defining a healthy diet: evidence for the role of contemporary dietary patterns in health and disease. Nutrients. 2020;12(2):334.
Organization WH. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. World Health Organization; 2013.
Bach-Faig A, Berry EM, Lairon D, Reguant J, Trichopoulou A, Dernini S, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011;14(12A):2274–84.
McCarty MF. Proposal for a dietary phytochemical index. Med Hypotheses. 2004;63(5):813–7.
Mofrad MD, Siassi F, Guilani B, Bellissimo N, Azadbakht L. Association of dietary phytochemical index and mental health in women: a cross-sectional study. Br J Nutr. 2019;121(9):1049–56.
Vincent HK, Bourguignon CM, Taylor AG. Relationship of the dietary phytochemical index to weight gain, oxidative stress and inflammation in overweight young adults. J Hum Nutr Dietetics. 2010;23(1):20–9.
Hosseini A, Ghorbani A. Cancer therapy with phytochemicals: evidence from clinical studies. Avicenna J Phytomedicine. 2015;5(2):84.
Hao Q, Wu Y, Vadgama JV, Wang P. Phytochemicals in inhibition of prostate Cancer: evidence from Molecular mechanisms studies. Biomolecules. 2022;12(9):1306.
Huijbregts P, Feskens E, Räsänen L, Fidanza F, Nissinen A, Menotti A, et al. Dietary pattern and 20 year mortality in elderly men in Finland, Italy, and the Netherlands: longitudinal cohort study. BMJ. 1997;315(7099):13–7.
Askari F, Parizi MK, Jessri M, Rashidkhani B. Dietary patterns in relation to prostate cancer in Iranian men: a case-control study. Asian Pac J cancer Prevention: APJCP. 2014;15(5):2159–63.
Dianatinasab M, Fararouei M, Mohammadianpanah M, Zare-Bandamiri M. Impact of social and clinical factors on diagnostic delay of breast cancer: a cross-sectional study. Medicine. 2016;95(38).
Dianatinasab M, Fararouei M, Mohammadianpanah M, Zare-Bandamiri M, Rezaianzadeh A. Hair coloring, stress, and smoking increase the risk of breast cancer: a case-control study. Clin Breast Cancer. 2017;17(8):650–9.
Esmaillzadeh A, Azadbakht L. Major dietary patterns in relation to general obesity and central adiposity among Iranian women. J Nutr. 2008;138(2):358–63.
Mirjalili F, Rezazadegan M, Jalilpiran Y, Mousavi SM, Jafari A, Mohajeri SAR, et al. The Association between Dietary Diversity score and risk of prostate Cancer: (a case-control study). Nutr Cancer. 2022;74(4):1270–8.
Jalilpiran Y, Mehranfar S, Jafari A, Mohajeri SAR, Faghih S. Dietary energy density and risk of prostate cancer: (a case–control study). Clin Nutr ESPEN. 2021;43:342–7.
Nematy M, Nouri M, Ghazizahedi S, Norouzy A, Mohajeri S, Shalaei N, et al. Validity and reproducibility of Iranian food frequency questionnaire. Switz Res Park J. 2013;102:2137–46.
Maynard M, Ness AR, Abraham L, Blane D, Bates C, Gunnell D. Selecting a healthy diet score: lessons from a study of diet and health in early old age (the Boyd Orr cohort). Public Health Nutr. 2005;8(3):321–6.
Schwingshackl L, Bogensberger B, Hoffmann G. Diet quality as assessed by the healthy eating index, alternate healthy eating index, dietary approaches to stop hypertension score, and health outcomes: an updated systematic review and meta-analysis of cohort studies. J Acad Nutr Dietetics. 2018;118(1):74–100. e11.
López-Guarnido O, Álvarez-Cubero MJ, Saiz M, Lozano D, Rodrigo L, Pascual M, et al. Mediterranean diet adherence and prostate cancer risk. Nutr Hosp. 2014;31(3):1012–9.
Kolonel LN, Hankin JH, Whittemore AS, Wu AH, Gallagher RP, Wilkens LR, et al. Vegetables, fruits, legumes and prostate cancer: a multiethnic case-control study. Cancer Epidemiol Biomarkers Prev. 2000;9(8):795–804.
Liu B, Mao Q, Cao M, Xie L. Cruciferous vegetables intake and risk of prostate cancer: a meta-analysis. Int J Urol. 2012;19(2):134–41.
Lin P-H, Aronson W, Freedland SJ. Nutrition, dietary interventions and prostate cancer: the latest evidence. BMC Med. 2015;13(1):1–15.
Vaioulis A, Yiannis K, Perivoliotis K, Stavros G, Vasilios T, Anastasios K. Association between the Mediterranean diet and prostate cancer risk in a Greek population. medRxiv. 2020:2020.08. 13.20172999.
Morze J, Danielewicz A, Przybyłowicz K, Zeng H, Hoffmann G, Schwingshackl L. An updated systematic review and meta-analysis on adherence to mediterranean diet and risk of cancer. Eur J Nutr. 2021;60:1561–86.
Yang JJ, Yu D, Xiang Y-B, Blot W, White E, Robien K, et al. Association of dietary fiber and yogurt consumption with lung cancer risk: a pooled analysis. JAMA Oncol. 2020;6(2):e194107–e.
Chen S, Chen Y, Ma S, Zheng R, Zhao P, Zhang L, et al. Dietary fibre intake and risk of breast cancer: a systematic review and meta-analysis of epidemiological studies. Oncotarget. 2016;7(49):80980.
Zhang Z, Xu G, Ma M, Yang J, Liu X. Dietary fiber intake reduces risk for gastric cancer: a meta-analysis. Gastroenterology. 2013;145(1):113–20. e3.
Clinton SK, Giovannucci EL, Hursting SD. The world cancer research fund/American institute for cancer research third expert report on diet, nutrition, physical activity, and cancer: impact and future directions. J Nutr. 2020;150(4):663–71.
Aune D, Keum N, Giovannucci E, Fadnes LT, Boffetta P, Greenwood DC, et al. Dietary intake and blood concentrations of antioxidants and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Am J Clin Nutr. 2018;108(5):1069–91.
Bahadoran Z, Karimi Z, Houshiar-Rad A, Mirzayi H-R, Rashidkhani B. Dietary phytochemical index and the risk of breast cancer: a case control study in a population of Iranian women. Asian Pac J Cancer Prev. 2013;14(5):2747–51.
Yu Z, Malik VS, Keum N, Hu FB, Giovannucci EL, Stampfer MJ, et al. Associations between nut consumption and inflammatory biomarkers. Am J Clin Nutr. 2016;104(3):722–8.
Roager HM, Vogt JK, Kristensen M, Hansen LBS, Ibrügger S, Mærkedahl RB, et al. Whole grain-rich diet reduces body weight and systemic low-grade inflammation without inducing major changes of the gut microbiome: a randomised cross-over trial. Gut. 2019;68(1):83–93.
Mazidi M, Katsiki N, George ES, Banach M. Tomato and lycopene consumption is inversely associated with total and cause-specific mortality: a population-based cohort study, on behalf of the International Lipid Expert Panel (ILEP). Br J Nutr. 2020;124(12):1303–10.
Kim C, Park K. Association between phytochemical index and inflammation in Korean adults. Antioxidants. 2022;11(2):348.
Cicero AF, Allkanjari O, Busetto GM, Cai T, Larganà G, Magri V et al. Nutraceutical treatment and prevention of benign prostatic hyperplasia and prostate cancer. Archivio Italiano Di Urol E Andrologia. 2019;91(3).
Bosire C, Stampfer MJ, Subar AF, Park Y, Kirkpatrick SI, Chiuve SE, et al. Index-based dietary patterns and the risk of prostate cancer in the NIH-AARP diet and health study. Am J Epidemiol. 2013;177(6):504–13.
Szymanski KM, Wheeler DC, Mucci LA. Fish consumption and prostate cancer risk: a review and meta-analysis. Am J Clin Nutr. 2010;92(5):1223–33.
Acknowledgements
The authors express their gratitude to the participants for their kind cooperation. The authors also appreciate the Vice-chancellor of research of the Shiraz University of Medical Sciences for supporting this study.
Funding
The Vice-chancellor of research of Shiraz University of Medical Sciences supported this study. Sciences, Shiraz Iran.
Author information
Authors and Affiliations
Contributions
Conceptualization: SF, MN and YJ; Methodology: SF, MN, YJ, FM, MM and MR; Formal analysis and investigation: MN, YJ, FM, MM and MR; Writing – original draft preparation: FM, MM, MR and MM; Writing – review and editing: SF, MN, YJ, FM, MM, MR and MM; Supervision: SF and MN.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The protocol for this study was approved by the Ethics Committee of Shiraz University of Medical Sciences in Iran, following the guidelines of the Declaration of Helsinki. A consent form was obtained from all participants in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it.The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mahmoodi, M., Mohammadi, F., Rajabzadeh-dehkordi, M. et al. The association between healthy diet indicator and phytochemical index with prostate cancer odds ratio: a case-control study. J Health Popul Nutr 43, 116 (2024). https://doi.org/10.1186/s41043-024-00603-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-024-00603-6