
Abstract
Background
In Thailand, the epidemiological data on the relationship between obesity and heart failure (HF) among high-risk populations was limited. We assessed the association between body mass index (BMI) and the new-onset HF among people with hypertension (HTN), and also assessed the effect modifier of uncontrolled HTN on this association.
Methods
We analyzed the data obtained from the 2018 Thailand DM/HT study database. Thai people with HTN aged 20 years and older receiving continuous care at outpatient clinics in hospitals nationwide were included. The new-onset HF was defined regarding the ICD-10 as I50 in the medical records within 12 months. Obesity was defined as BMI \(\ge\) 25 kg/m2. Multivariable log-binomial regression analysis was used to determine the association between BMI and new-onset HF and presented as the adjusted risk ratio (aRR) and 95% confidence interval (CI).
Results
A total of 35,756 participants were included in the analysis. In all, 50.0% of the participants had BP control for the last two consecutive visits. The mean BMI was 25.1 \(\pm\) 4.7 kg/m2. New-onset HF occurred in 75 participants (0.21%; 95% CI 0.17–0.26). After adjusting for potential confounders, an elevated BMI was associated with new-onset HF (p value for quadratic trend < 0.001). In comparison with participants with normal BMI (18.5–22.9 kg/m2), the aRR for new-onset HF was 1.57 (95% CI 0.80–3.07) and 3.97 (95% CI 1.95–8.10) in those with BMI 25.0–29.9, and ≥ 30.0 kg/m2. For participants with obesity, aRR for new-onset HF was 2.05 (95% CI 1.24–3.39) compared to non-obese participants. The study found that among patients with control BP, obesity was associated with a higher risk of new-onset HF with an adjusted RR of 2.33 (95% CI 1.12–4.83). For those with uncontrolled BP, the adjusted RR was 1.83 (95% CI 0.93–3.58), but there was no heterogeneity with p value = 0.642.
Conclusion
An increased BMI had a higher risk for new-onset HF among Thai people with HTN. Obesity was independently associated with new-onset HF among people with HTN, regardless of uncontrolled HTN. Our findings highlight that weight reduction is crucial for mitigating the risk of HF development in HTN patients, regardless of their BP control status.
Similar content being viewed by others


Background
Heart Failure (HF) is a complex and life-threatening syndrome that poses a significant public health problem worldwide [1, 2]. In 2017, the number of individuals affected by HF was estimated to be over 64 million globally [2,3,4]. Although the incidence of HF has stabilized at approximately 1–20 cases per 1,000 person-years in developed countries, its mortality rate remains high, with a 1-year mortality rate of approximately 25–30% [3, 4]. Robust evidence indicates that HF is a leading cause of morbidity and mortality, particularly in high-risk populations such as those with hypertension (HTN) [2, 3].
Overweight and obesity are considered global health concerns and are known metabolic risk factors for noncommunicable diseases, particularly cardiovascular disease (CVD) [5, 6]. Previous studies have shown that an increase in body mass index (BMI) is associated with a higher risk of HF [7,8,9]. For instance, a 1 kg/m2 increase in BMI was linked to an 11% increase in the risk of HF, according to a large-scale prospective cohort study of the Physicians' Health Study [9]. Similarly, the Framingham Heart Study reported that individuals with BMI in the range of 25.0–29.9 kg/m2 had an adjusted hazard ratio of 1.5 (95% CI 1.3–1.7) for the risk of HF compared to those with BMI < 25 kg/m2 [8]. However, a reverse epidemiology was observed among Hispanic males in the Multi-Ethnic Study of Atherosclerosis [7]. Another study conducted in the Asian population found higher HF hospitalization rates in individuals with low BMI [10].
In Thailand, the prevalence of metabolic risk factors for CVD, including HTN and obesity, has been on the rise [11,12,13,14,15]. Approximately one-fourth of Thai adults are affected by HTN, and approximately two-thirds (66.6%) of Thai patients with HTN can control their blood pressure (BP) [16]. The prevalence of obesity (BMI ≥ 25 kg/m2) among Thai adults is 37.8% and 46.4% in men and women, respectively [11]. A recent study, the Thailand DM/HT study, reported that almost half of Thai patients with HTN (47.6%) have obesity [16].
According to existing evidence in Thailand, approximately 1% of patients with HTN have a history of HF, and the prevalence of HF increases significantly with age, particularly in individuals older than 65 years [16]. However, epidemiological data on the relationship between obesity and HF among high-risk populations, particularly those with HTN, remain limited in Thailand. Therefore, in the present study, we aimed to assess the association between increased BMI and new-onset HF among patients with HTN receiving continuous care in Thailand, as well as to evaluate the effect modifier of BP control status on this association.
Methods
Study designs and subjects
In the present study, we obtained the data from the Thailand DM/HT study database in 2018, supported by the National Health Security Office (NHSO). As described elsewhere by Sakboonyarat et al.[16], the Thailand DM/HT study, an annual survey, focused on evaluating clinical outcomes, such as BP control and cardiovascular complications, in patients with HTN aged 20 and above who received HTN care for at least 12 months at outpatient clinics in hospitals across the country. However, the study did not include patients who had a history of pregnancy within 12 months from the date of data collection and patients receiving care at university hospitals.[16]
The study database on DM/HT in Thailand during the period of January 2018 to July 2018 comprised an initial sample size of 36,557 hypertensive patients [16]. After excluding 530 subjects without BMI data in their medical records and 271 individuals with a history of HF prior to 12 months from the date of data collection (i.e., before January 2017 for the data collection date on January 2018), a total of 35,756 hypertensive patients without baseline HF and having information on BMI were included in the final analysis. Regarding the retrospectively collected database, with a short follow-up period, we examined the cross-sectional association between obesity and the risk of new-onset HF.
Data collection
In the Thailand DM/HT study, the registered nurse, who was trained, meticulously reviewed and abstracted the data from medical records using a case report form (CRF) that was based on a standardized protocol. Once the data was carefully collected, it was then transmitted to the data management unit located in Nonthaburi province [16, 17]. The information that was collected included a comprehensive analysis of the demographic characteristics of patients with HTN, health insurance scheme, the location of the outpatient clinic, weight and height, smoking status, alcohol use, comorbidities, the history of antihypertensive medication use, BP, and any cardiovascular complications such as ischemic heart disease (IHD) and HF.
Outcome and exposure
In the present study, the new-onset HF was defined as the occurrence of HF as a new onset in hypertensive patients within 12 months until the data collection date. The definition was based on the International Classification of Diseases, Tenth Revision Codes (ICD-10) I50, which appeared in patients' medical records [18]. It is important to note that in Thailand, patients are covered by health insurance schemes, such as Universal Health Coverage (UHC), Civil Servant Medical Benefit (CSMB), or Social Security (SS). As such, when a patient develops new-onset HF, they are typically able to receive appropriate and standardized care based on their specific health insurance coverage. Regarding the exposure of interest, BMI was calculated based on the recorded weight and height of the subjects during their most recent medical visit. The BMI values were segregated into five categories: 18.5–22.9 kg/m2 (normal weight), < 18.5 kg/m2 (underweight), 23.0–24.9 kg/m2 (overweight), 25.0–29.9 kg/m2 (obese I), and ≥ 30 kg/m2 (obese II). Furthermore, obesity was defined as BMI equal to or greater than 25 kg/m2.[19]
Covariates
The covariates considered in this study comprised a range of demographic variables, including age and sex, as well as a variety of health-related information. Geographic regions were also taken into account, with North, Central, Northeast, and South all being included. In terms of health insurance schemes, UHC, CSMB, SS and others were all encompassed. Hospital location of the clinic was categorized into regional hospital, general hospital, community hospital, private hospital, and others, while comorbidities were defined based on the ICD-10, including type 2 diabetes (T2D) (E11), dyslipidemia (DLP) (E78), and renal insufficiency (N18) [18]. History of IHD was defined based on the ICD-10: I20-I25 [18], or a recorded history of coronary revascularization [20]. Tobacco use was determined based on the smoking status recorded in the medical records as either never smoked or ever smoked, and alcohol consumption was similarly determined based on the history of alcohol use recorded in the medical records as either never alcohol use or ever alcohol use. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (ACEI/ARB) use was defined as a history of ACEI/ARB being prescribed in the medical record within 12 months before the data collection date. BP control was defined as systolic BP < 140 mmHg and diastolic BP < 90 mmHg, and BP control for two consecutive times was defined as BP control at both the latest visit and one time before the latest visit [16, 21].
Statistical analysis
The present study employed StataCorp. 2021. Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC, for all data analysis. Descriptive statistics was utilized to characterize the study participants, where categorical data was presented in percentages, while continuous data was presented as mean with standard deviation (SD) and median with Q1 and Q3. A chi-square test was used to compare the characteristics of participants between the obesity and non-obesity groups for categorical variables, while a t-test was employed for continuous variables. To evaluate the association between BMI and new-onset HF, a log-binomial regression analysis was conducted and presented as a risk ratio (RR) and 95% confidence interval (CI). The multivariable analysis adjusted for several covariates, including model 1: age, and sex; model 2: variables in model 1 plus health insurance schemes, geographic regions, location of clinic, T2D, DLP, renal insufficiency, history of IHD, smoking status, alcohol use, control BP consecutively two latest visits, and ACEI/ARB use, and presented as adjusted RR, and 95% CI. The average adjusted prediction of new-onset HF by increased BMI was illustrated using the margins command.
Furthermore, a subgroup analysis was performed using multivariable log-binomial regression analysis to evaluate the association between obesity and the risk of new-onset HF among patients with control BP for the last two consecutive visits and among those with uncontrolled BP. The interaction was tested to explore whether BP control status modifies the association between obesity and new-onset HF. A statistical significance was considered by a two-sided p value less than 0.05.
Sensitivity analysis
Despite adjusting for potential confounders in the multivariable model in the primary analysis, we did not have the opportunity to include physical activity and dietary behavior in the final model, which means that residual confounding may exist. Therefore, we conducted a sensitivity analysis for unmeasured confounding using E-values estimated by the evalue package [22].
Ethic considerations
The study was reviewed and approved by the Institutional Review Board, the Royal Thai Army Medical Department, in compliance with international guidelines such as the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines, and ICH-GCP (approval number S055h/65_Exp). A waiver of documentation of informed consent was utilized due to the use of secondary data, and was granted by the Institutional Review Board, the Royal Thai Army Medical Department.
Results
Characteristics of study participants
The present study included a total of 35,756 patients with HTN who received continuous care. The majority of participants (61.4%) were women, and the average age of participants was 64.5 ± 11.8 years. Of all the participants, 74% were under the UHC scheme. Regarding comorbidities, 13.1%, 15.4%, and 62.8% of the study participants had a history of renal insufficiency, T2D, and DLP, respectively. Our analysis revealed that 50.0% of the participants had BP control for the last two consecutive visits. The average BMI of the participants was 25.1 ± 4.7 kg/m2. The prevalence of obesity (BMI ≥ 25 kg/m2) was found to be 47.1%. Table 1 presents the characteristics of the participants in the study and stratified by obesity.
Association between obesity and new-onset heart failure
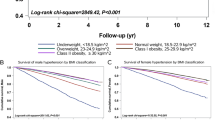
Within a year, 75 new-onset HF events were observed, accounting for 0.21% (95% CI 0.17–0.26) of the study population. Univariable log-binomial regression analysis for factors associated with new-onset HF is presented in Additional file 1: Table S1. The association between BMI and new-onset HF was analyzed through a multivariable log-binomial regression, as presented in Table 2. After adjusting for potential confounders, the analysis revealed that an elevated BMI was associated with new-onset HF (p value for quadratic trend < 0.001). Figure 1 demonstrates the increased BMI (started at 18.5 kg/m2) for the average adjusted prediction of new-onset HF per 1000 patients and 95% CI. Further, the high categories of BMI, i.e., 25.0–29.9 kg/m2 and ≥ 30 kg/m2, were associated with an increased risk of new-onset HF, as compared to the normal BMI category (18.5–22.9 kg/m2), with adjusted RRs of 1.57 (95% CI 0.80–3.07) and 3.97 (95% CI 1.95–8.10), respectively. Among the overall participants, individuals with obesity (BMI ≥ 25 kg/m2) had a higher risk of new-onset HF (adjusted RR 2.05; 95% CI 1.24–3.39), as compared to those with non-obesity (BMI < 25 kg/m2). Similarly, the adjusted RR for new-onset HF in HTN patients with BMI ≥ 30.0 kg/m2 was 3.19 (95% CI 1.85–5.57) compared to those with BMI < 30 kg/m2. Table 3 presents the association between BMI and new-onset HF stratified by BP control for the last two consecutive visits. Among patients with control BP, the adjusted RR for the association between obesity (BMI ≥ 25 kg/m2) and new-onset HF was 2.33 (95% CI 1.12–4.83), while the adjusted RR was insinuated as 1.83 (95% CI 0.93–3.58) among those with uncontrol BP. However, the interaction testing revealed no heterogeneity with p value = 0.642.

Average adjusted prediction of risk of new-onset heart failure per 1000 patients with hypertension and 95% CI. RR: relative risk, CI: confidence interval. Average adjusted prediction of risk of new-onset heart failure per 1000 patients and 95% CI per 1 kg/m2 of BMI (started at 18.5 kg/m2), adjusting for age, sex, health schemes, geographic regions, hospital types, type 2 diabetes, dyslipidemia, renal insufficiency, history of ischemic heart disease, smoking status, alcohol use, control blood pressure consecutively two latest visits, and ACEI/ARB use.
Regarding the sensitivity analysis, the E-value for the RR to identify the association between the unmeasured confounder and the factors associated with new-onset HF is presented in Additional file 1: Table S2. The E-value for the point estimate of the association between obesity and new-onset HF (aRR 2.05; 95% CI 1.24–3.39) was 3.52. therefore, the observed RR of 2.05 could be explained away by an unmeasured confounder that was associated with both obesity and HF by an RR of 3.52-fold each, above and beyond the measured confounders, but weaker confounding could not do so [22].
Discussion
The results of our study demonstrate a noteworthy and positive association between obesity and the risk of new-onset HF among patients with HTN receiving continuous care in Thailand. Moreover, we identified a quadratic association between elevated BMI and increased risk of new-onset HF in this population. Notably, subgroup analysis stratified by the status BP control for the last two consecutive visits revealed that the association between obesity and new-onset HF was mitigated among those with uncontrolled BP; however, no heterogeneity was observed. It is worth mentioning that this study is the most extensive and up-to-date investigation to date that examines the relationship between BMI and HF risk among patients with HTN who receive continuous care in Thailand. Our findings suggest that obesity is an independent risk factor for new-onset HF in patients with HTN, whether controlling BP and weight reduction may be effective strategies to alleviate the risk of HF in this population.
In the present research, our findings revealed a significant association between BMI and the risk of new-onset HF, with each unit increase in BMI (started at 18.5 kg/m2) resulting in a 10% increase in the risk of new-onset HF. Moreover, our investigation disclosed that individuals categorized as overweight, obesity I, and obesity II exhibited an elevated risk of new-onset HF, estimated to be 11%, 57%, and 297%, respectively, compared to those with normal weight. Notably, when assessing the risk of new-onset HF among HTN patients with BMI ≥ 25 kg/m2, which is the cutoff for defining obesity status among the Asian population [19], the results demonstrated a relatively precise estimate, with a calculated risk of 2.1 times higher among individuals with BMI ≥ 25 kg/m2 compared to those with BMI < 25 kg/m2, with a 95% CI of 1.2–3.4. Furthermore, when we use the cutoff at 30 kg/m2, we found that the risk of new-onset HF among HTN patients with BMI ≥ 30 kg/m2 was 3.2 times the risk of that among those with BMI < 30 kg/m2 which indicates the robust of our findings among high-risk population.
The results of our study are consistent with previous research. Notably, a large-scale prospective cohort study of 21,094 men conducted as part of the Physicians' Health Study found that every 1 kg/m2 increase in BMI was associated with an 11% increase in the risk of HF [9]. Furthermore, this study showed that individuals with BMI in the range of 25.0–29.9 kg/m2 had an adjusted hazard ratio of 1.5 (95% CI 1.3–1.7) for the risk of HF, compared to those with BMI < 25 kg/m2 [9]. Similarly, the Framingham Heart Study (FHS) also reported that every 1 kg/m2 increase in BMI was linked to a 6% increase in the risk of HF [8]. The FHS further demonstrated that the risk of HF was notably higher among individuals with BMI in the range of 25.0–29.9 kg/m2 and ≥ 30 kg/m2, compared to those with BMI in the range of 18.5–24.9 kg/m2, with adjusted hazard ratios of 1.3 (95% CI 1.1–1.7) and 2.0 (95% CI 1.6–2.6), respectively [8].
On the other hand, in the Multi-Ethnic Study of Atherosclerosis, BMI was found to be positively associated with HF incidence among Caucasians and African Americans. In contrast, a paradoxical or reverse epidemiology between BMI and HF incidence was observed among Hispanic males [7]. In addition, the study in the Asian population also found that the HF hospitalization rate in individuals with high BMI was higher than in those with low BMI [10]. However, the obesity paradox may be an artifact of residual confounding at the statistical level, according to existing literature [23, 24].
In the present study, we observed that the new-onset HF was 2.3 times higher among HTN patients with obesity as compared to those without obesity who had controlled BP. However, among HTN patients with uncontrolled BP, this association between obesity and new-onset HF was alleviated to 1.8. However, no heterogeneity was observed in our study. Based on the solid evidence available, it can be inferred that uncontrolled HTN leads to an increased likelihood of cardiac remodeling, while HF is associated with structural and hemodynamic changes in the heart [25,26,27]. Thus, it is probable that cardiac remodeling exists in individuals with uncontrolled BP, making them more susceptible to developing HF. This could potentially weaken the association between elevated BMI and new-onset HF, particularly among individuals with uncontrolled BP compared to those with controlled BP. Our findings suggest that weight reduction should be encouraged in HTN patients, whether to control BP or not, to alleviate the risk of HF in the future.
Multiple mechanisms have been proposed to explain the observed independent association between obesity and the development of new-HF. One possible mechanism is the increased metabolic demand resulting from excessive adipose tissue and fat-free mass in obesity, which leads to hyperdynamic circulation, including increased blood volume and stroke volume [28, 29]. These changes can result in hemodynamic overload and increased cardiac stroke work, eventually causing left ventricular failure [28,29,30,31,32]. Another mechanism is the alteration in cardiac structure, which is due to the excessive epicardial fat commonly found in obesity [31, 33]. The epicardial fat, which is strongly associated with visceral adiposity, extends into the myocardium, resulting in fatty infiltration and fibrosis, which can facilitate left ventricular hypertrophy and cardiac dysfunction [29, 32,33,34,35]. A third possible mechanism is cardiac lipotoxicity, whereby adiposity promotes ectopic deposition of triglyceride in the heart, leading to cardiac steatosis [36,37,38]. Cardiomyocytes have limited storage capacity, and excess free fatty acids are shunted into the nonoxidative pathway, leading to lipotoxicity and facilitating apoptosis of lipid-filled cardiomyocytes [29, 37,38,39]. Additionally, Obesity is often accompanied by comorbidities such as obstructive sleep apnea and obesity hypoventilation syndrome [33]. These conditions increase the demand for ventilation and breathing workload, making respiratory muscles less efficient. Consequently, alveolar hypoventilation and ventilation-perfusion mismatch occur, resulting in pulmonary HTN due to hypoxia-induced vasoconstriction. This can lead to right ventricular failure [30, 40].
The present study has some limitations. One significant limitation is the relatively brief duration of the observation period for the outcome within 12 months. While the findings suggest a positive association between higher BMI and new-onset HF among patients with HTN, the causal inference cannot be drawn from these results. To ensure that the outcome of interest, namely new-onset HF, occurred within 12 months, we excluded HTN patients with a history of HF before 12 months of the data collection date. We abstracted information on the BMI of participants from the latest visit within the 12-month period, which is the same period during which new-onset HF occurs. However, it is important to note that longitudinal studies have documented only slight changes in BMI over a decade in midlife and older adults [41]. In the present study, HF was defined using ICD-10, which appears on the medical records which may have caused misclassification and also did not provide a specific type of HF, such as HF with preserved ejection fraction (HFpEF) or HF with non-preserved ejection fraction (HFnpEF). Therefore, the association between obesity and a specific type of HF was not explored.
Additionally, as the data used in this study was collected from the Thailand DM/HT study, we did not have the opportunity to include physical activity and dietary behavior in the final model, which means that residual confounding may exist. We perform a sensitivity analysis and the evidence for causality from the E-values (Additional file 1: Table S2) looks relatively strong because substantial unmeasured confounding would be needed to reduce the observed association between obesity and new-onset HF. Despite these limitations, the study boasts several notable strengths. The large sample size analyzed in the study provides a robust dataset for our analyses. In addition, the study population is highly representative of Thai patients with HTN receiving continuous care nationwide, thereby enhancing the generalizability of our findings.
Conclusion
In conclusion, our study indicates a positive association between elevated BMI and the incidence of new-onset HF in Thai patients with HTN. In particular, individuals with obesity exhibited a higher risk for new-onset HF as compared to those without obesity. The association between obesity and new-onset HF was attenuated among patients with uncontrolled BP; nevertheless, no heterogeneity was observed. Our findings highlight the importance of weight reduction in patients with HTN, irrespective of their BP control status, as a key strategy for mitigating the risk of HF development in the future.
Availability of data and materials
Data cannot be shared publicly because the data set contains identifying information; additionally, the data belong to the Thailand DM/HT study of the Medical Research Network of the Consortium of Thai Medical Schools (MedResNet). Thus, ethical restrictions exist on the data set. Data are available from the Thai National Health Security Office (NHSO), Bangkok, Thailand (contact via https://dmht.thaimedresnet.org/) for researchers who meet the criteria for access to confidential data.
Abbreviations
- HF:
-
Heart failure
- BMI:
-
Body mass index
- HTN:
-
Hypertension
- BP:
-
Blood pressure
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- CVD:
-
Cardiovascular disease
- IHD:
-
Ischemic heart disease
- T2D:
-
Type 2 diabetes
- DLP:
-
Dyslipidemia
References
Bahrami H, Kronmal R, Bluemke DA, Olson J, Shea S, Liu K, et al. Differences in the incidence of congestive heart failure by ethnicity: the multi-ethnic study of atherosclerosis. Arch Intern Med. 2008;168:2138–45.
Collaborators GBD. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017; 2018.
Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology. Cardiovasc Res. 2023;391:572–80.
Conrad N, Judge A, Tran J, Mohseni H, Hedgecott D, Crespillo AP, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. 2018;391:572–80.
World Health Organization. Noncommunicable diseases [Internet]. 2022 [cited 2023 May 3]. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
Ritchie SA, Connell JMC. The link between abdominal obesity, metabolic syndrome and cardiovascular disease. Nutr Metab Cardiovasc Dis. 2007;17:319–26.
Ebong IA, Goff DC Jr, Rodriguez CJ, Chen H, Bluemke DA, Szklo M, et al. The relationship between measures of obesity and incident heart failure: the multi-ethnic study of atherosclerosis. Obesity. 2013;21:1915–22.
Kenchaiah S, Evans JC, Levy D, Wilson PWF, Benjamin EJ, Larson MG, et al. Obesity and the risk of heart failure. N Engl J Med. 2002;347:305–13.
Kenchaiah S, Sesso HD, Gaziano JM. Body mass index and vigorous physical activity and the risk of heart failure among men. Circulation. 2009;119:44–52.
Chandramouli C, Tay WT, Bamadhaj NS, Tromp J, Teng T-HK, Yap JJL, et al. Association of obesity with heart failure outcomes in 11 Asian regions: a cohort study. PLoS Med. 2019;16:916.
Aekplakorn W. Thai National Health Examination Survey VI (2019–2020) [Internet]. 2019. Available from: https://online.fliphtml5.com/bcbgj/znee/#p=187
Sakboonyarat B, Poovieng J, Jongcherdchootrakul K, Srisawat P, Hatthachote P, Mungthin M, et al. Rising trends in obesity prevalence among Royal Thai Army personnel from 2017 to 2021. Sci Rep. 2022;12:7726.
Hatthachote P, Rangsin R, Mungthin M, Sakboonyarat B. Trends in the prevalence of obesity among young Thai men and associated factors: from 2009 to 2016. Mil Med Res. 2019;6:1–8.
Sakboonyarat B, Pornpongsawad C, Sangkool T, Phanmanas C, Kesonphaet N, Tangthongtawi N, et al. Trends, prevalence and associated factors of obesity among adults in a rural community in Thailand: serial cross-sectional surveys, 2012 and 2018. BMC Public Health. 2020;20:850.
Sakboonyarat B, Poovieng J, Srisawat P, Hatthachote P, Mungthin M, Rangsin R, et al. Prevalence, awareness, and control of hypertension and associated factors among Royal Thai Army personnel in Thailand from 2017 to 2021. Sci Rep. 2023;13:6946.
Sakboonyarat B, Rangsin R. Characteristics and clinical outcomes of people with hypertension receiving continuous care in Thailand: a cross-sectional study. Lancet Reg Health Southeast Asia. 2024;21:100319.
The National Health Security Office T. DAMUS: Data Archival for Maximum Utilization System [Internet]. 2022 [cited 2022 Oct 7]. Available from: https://www.damus.in.th/
World Health Organization. International statistical classification of diseases and related health problems, 10th revision [Internet]. 5th ed. 2016 [cited 2022 Nov 18]. Available from: https://apps.who.int/iris/handle/10665/246208
Inoue S, Zimmet P, Caterson I, Chunming C, Ikeda Y, Khalid AK, et al. The Asia–Pacific perspective: redefining obesity and its treatment. Sydney: Health Communications Australia Pty Ltd.; 2000.
Sakboonyarat B, Rangsin R. Prevalence and associated factors of ischemic heart disease (IHD) among patients with diabetes mellitus: a nation-wide, cross-sectional survey. BMC Cardiovasc Disord. 2018;18:151.
Kunanon S, Chattranukulchai P, Chotruangnapa C, Kositanurit W, Methavigul K, Boonyasirinant T, et al. 2019 Thai guidelines on the treatment of hypertension: executive summary. J Med Assoc Thai. 2021;104:1729–38.
Linden A, Mathur MB, VanderWeele TJ. Conducting sensitivity analysis for unmeasured confounding in observational studies using E-values: the evalue package. Stata J. 2020;20:162–75.
Sohn M, Budiman-Mak E, Oh EH, Park MS, Stuck RM, Stone NJ, et al. Obesity paradox in amputation risk among nonelderly diabetic men. Obesity. 2012;20:460–2.
Turer AT, Hill JA, Elmquist JK, Scherer PE. Adipose tissue biology and cardiomyopathy: translational implications. Circ Res. 2012;111:1565–77.
Schwinger RHG. Pathophysiology of heart failure. Cardiovasc Diagn Ther. 2021;21:365–71.
Kehat I, Molkentin JD. Molecular pathways underlying cardiac remodeling during pathophysiological stimulation. Circulation. 2010;122:2727–35.
Mayet J, Hughes A. Cardiac and vascular pathophysiology in hypertension. Heart. 2003;89:1104–9.
Vasan RS. Cardiac function and obesity. Heart. 2003;89:1127–9.
Ebong IA, Goff DC, Rodriguez CJ, Chen H, Bertoni AG. Mechanisms of heart failure in obesity. Obes Res Clin Pract. 2014;8:e540–8.
Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on obesity and heart disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2006;113:898–918.
Alpert MA. Obesity cardiomyopathy: pathophysiology and evolution of the clinical syndrome. Am J Med Sci. 2001;321:225–36.
Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer FX, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss. Arterioscler Thromb Vasc Biol. 2006;11:898–918.
Ashrafian H, Le Roux CW, Darzi A, Athanasiou T. Effects of bariatric surgery on cardiovascular function. Circulation. 2008;118:2091–102.
Gradman AH, Alfayoumi F. From left ventricular hypertrophy to congestive heart failure: management of hypertensive heart disease. Prog Cardiovasc Dis. 2006;48:326–41.
Bauml MA, Underwood DA. Left ventricular hypertrophy: an overlooked cardiovascular risk factor. Cleve Clin J Med. 2010;77:381–91.
Szczepaniak LS, Dobbins RL, Metzger GJ, Sartoni-D’Ambrosia G, Arbique D, Vongpatanasin W, et al. Myocardial triglycerides and systolic function in humans: in vivo evaluation by localized proton spectroscopy and cardiac imaging. Magn Reson Med. 2003;49:417–23.
Ebong IA, Goff DC, Rodriguez CJ, Chen H, Sibley CT, Bertoni AG. Association of lipids with incident heart failure among adults with and without diabetes mellitus multiethnic study of atherosclerosis. Circ Heart Fail. 2013;6:371–8.
McGavock JM, Victor RG, Unger RH, Szczepaniak LS. Adiposity of the heart, revisited. Ann Intern Med. 2006;144:517–24.
Schaffer JE. Lipotoxicity: when tissues overeat. Curr Opin Lipidol. 2003;14:281–7.
Dela Cruz CS, Matthay RA. Role of obesity in cardiomyopathy and pulmonary hypertension. Clin Chest Med. 2009;30:509–23.
Arigo D, Ainsworth MC, Pasko K, Brown MM, Travers L. Predictors of change in BMI over 10 years among midlife and older adults: associations with gender, CVD risk status, depressive symptoms, and social support. Soc Sci Med. 2021;279:113995.
Acknowledgements
The authors thank the National Health Security Office in Thailand for supporting the Thailand DM/HT study dataset.
Funding
This study was funded by the Phramongkutklao College of Medicine, Bangkok, Thailand. The National Health Security Office in Thailand supported the Thailand DM/HT study.
Author information
Authors and Affiliations
Contributions
B.S. conducted the study concept, analyzed and interpreted the data, and was a major contributor to writing the manuscript. J.P. conducted the study concept, analysis, and interpretation of the data. R.R. performed the study concept/design, data collection, and interpretation of the data. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
This study was reviewed and approved by the Institutional Review Board, Royal Thai Army Medical Department, following international guidelines including the Declaration of Helsinki, the Belmont Report, CIOMS Guidelines, and the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use–Good Clinical Practice (ICH–GCP) (approval number S055h/65_Exp). Due to the use of secondary data, a waiver of documentation of informed consent was utilized. The Institutional Review Board, Royal Thai Army Medical Department, approved an informed consent waiver.
Consent for publication
Consent for publication is not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Supplementary tables.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sakboonyarat, B., Poovieng, J. & Rangsin, R. Association between obesity and new-onset heart failure among patients with hypertension in Thailand. J Health Popul Nutr 43, 33 (2024). https://doi.org/10.1186/s41043-024-00530-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-024-00530-6