
Abstract
Objective
Although some studies have linked smoking to mortality after out-of-hospital cardiac arrests (OHCAs), data regarding smoking and mortality after OHCAs have not yet been discussed in a meta-analysis. Thus, this study conducted this systematic review to clarify the association.
Methods
The study searched Medline-PubMed, Web of Science, Embase and Cochrane libraries between January 1972 and July 2022 for studies that evaluated the association between smoking and mortality after OHCAs. Studies that reportedly showed relative risk estimates with 95% confidence intervals (CIs) were included.
Results
Incorporating a collective of five studies comprising 2477 participants, the analysis revealed a lower mortality risk among smokers in the aftermath of OHCAs compared with non-smokers (odds ratio: 0.77; 95% CI 0.61–0.96; P < 0.05). Egger's test showed no publication bias in the relationship between smoking and mortality after OHCAs.
Conclusions
After experiencing OHCAs, smokers had lower mortality than non-smokers. However, due to the lack of data, this ‘smoker’s paradox’ still needs other covariate effects and further studies to be considered valid.
Similar content being viewed by others


Introduction
Out-of-hospital cardiac arrests (OHCAs) are a major challenge to global health and have high morbidity and mortality rates [1,2,3]. More than 345,000 OHCAs (1.4% incidence) are reported annually in America [4]. In England, about 80,000 people per year have an OHCA [5]. Survival rates following OHCAs in Europe are notably limited, ranging between 0.6 and 25% [1, 6]. In stark contrast, OHCA incidents represent less than 1% of reported cases in China [7]. It is noteworthy to mention that coronavirus disease (COVID-19) reportedly increases mortality rates for OHCAs, as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) interacts closely with angiotensin-converting enzyme-2 (ACE2) receptors on myocardial cells that could mediate SARS-CoV-2 into myocardial cells and cause cardiotoxicity [8, 9].
Smoking is a major public health challenge affecting human health worldwide [10], and approximately 7 million deaths are attributed to smoking each year [11]. The risk of premature mortality is three times higher for smokers than non-smokers [12]. Smoking significantly influences morbidity and mortality of various diseases, including cardiovascular diseases [12]. These also place a significant financial burden not only on the national healthcare systems but also on individuals, which has an upward trend every year [13,14,15].
Several factors are associated with the mortality of patients with OHCA, such as obesity [16], diabetes [17], age [18], smoking, coronary heart disease [19], cardiopulmonary resuscitation time [20] and quality of cardiopulmonary resuscitation [20]. However, the relationship between smoking and mortality following OHCAs remains unclear and needs further investigation. While recent studies have demonstrated conflicting findings, some studies have shown that smoking is strongly associated with an increased risk for cardiovascular disease that increases the incidence and mortality rate following OHCAs [21, 22]. Lahmann et al. [23] demonstrated conflicting findings, as smoking lowered the mortality rate and improved the prognosis of neurological functions, termed the ‘smoker's paradox’.
Due to the conflicting findings, the purpose of this study was to perform a comprehensive assessment of the impact of smoking on patient prognosis after OHCAs using existing literature evidence. A meta-analysis and systematic review will determine the relationship between smoking and mortality-related outcomes in patients with OHCAs. Finally, the study will provide a theoretical basis for resolving the ‘smoker's paradox’.
Methods
Ethical considerations
Previously published studies, which described prospective and retrospective studies and did not need ethical approval, were included.
Search strategy
This review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42022361239). This study was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. Literature searches on the Medline-PubMed, Web of Science, Embase and Cochrane libraries for trial studies between January 1972 and July 2022 were included. To ensure data integrity, the study was also combined with manual research. Keywords and related terms were used, such as ‘cardiac arrest’, ‘heart arrest’, ‘cardiopulmonary arrest’, ‘smoking’, and ‘behaviors, smoking’. There were no language restrictions on the publication of this study.
Selection criteria
Articles were included if the study evaluated mortality in smokers with cardiac arrest through odds ratios (OR), hazard ratios (HR), or relative risk (RR) ratios with 95% confidence intervals (CIs). All patients were older than 18 years of age. This analysis included case–control or cohort studies comparing exposure factors between both groups. Non-smokers with OHCA were used as a control group.
Patients who suffered from a drug overdose, trauma, asphyxiation or electrocution due to cardiac arrest were excluded, along with their respective reviews. Additionally, there was an assessment of the literature's quality, and any studies characterised by low-quality, incomplete datasets or those in which the data could not be ascertained from the literature due to insufficient descriptions were systematically excluded.
Data extraction
Two reviewers independently collected titles, first author names, research methods, smoking events, smokers, mortalities, abstracts and full texts of the obtained reviews. Studies were screened according to their admission and exclusion criteria, and all relevant data based on the pre-designed form were extracted. After screening, the data were cross-checked. When the opinions of the authors were inconsistent, they were resolved through discussion or consultation with a third person and were finally included in the study.
Quality assessment
The Newcastle–Ottawa scale (NOS) scoring system [24] was used to evaluate the methodological quality of included studies, and the principle of the star system was adopted. The NOS scoring system comprises three main parts, with a maximum of nine stars.
Statistical analysis
STATA 16.1 was used to test the heterogeneity of collected information and synthesise the summary RR, OR and HR values with their corresponding 95% CIs depending on the type of study. The χ2 and I-square (I2) tests were used to test the heterogeneity of the included studies. When P was > 0.05 and I2 was < 50%, there was no statistical heterogeneity among the studies, and the fixed effect model was used to analyse the study. When P was < 0.05 and I2 was > 50%, heterogeneity was considered significant among the studies, and the source of heterogeneity was further searched. If heterogeneity could not be eliminated and clinical consistency was found, the random effects model and subgroup analysis were used for statistical literature analysis; otherwise, descriptive analysis was used. Potential publication bias was analysed by Egger's analysis and funnel plots. Two reviewers autonomously evaluated the risk of bias within individual studies employing the Cochrane Risk of Bias Tool for Randomised Trials, version 2. In cases of dissenting assessments, consensus was achieved through dialogue. The evaluation of bias risk was conducted for each outcome encompassed within the trial. Yet, it was reported at the trial level, encapsulating the highest risk of bias score across all outcomes. The stability of meta-analysis results was tested by sensitivity analysis: Documents were excluded one by one. Each included study was eliminated one by one before merging effect sizes. The inclusion and exclusion criteria were changed, or certain types of literature were excluded before merging effect sizes.
Results
Search results
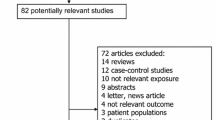
The study’s search identified 30,710 relevant citations, and after removing duplicates, 26,804 studies were screened. A total of 1,526 studies were excluded, as they were animal experiments, reviews and case reports. After reading the abstract, 25,056 studies were excluded. Thus, 222 studies were evaluated with the full text in detail, and 217 were excluded. Among them, 42 were letters, editorials or commentaries, and 70 showed no relationship between smoking and mortality caused by cardiac arrest. The remaining 105 studies did not have a relevant date. Finally, only five studies [25,26,27,28,29] were included in this meta-analysis (Fig. 1). Three studies had an NOS score of 6, and the others had NOS scores of 7 and 8. All studies had NOS scores over 6 (Table 1).

Flowchart of the study
Characteristics of selected studies
Five studies were included in this meta-analysis, and a total of 2903 participants were involved. Four studies were retrospective, and one was a prospective study. All included studies were published between 2006 and 2021 (Table 2).
Meta-analysis for mortality
A heterogeneity test was performed in this study and showed mild heterogeneity. (I2 = 42.3%; P = 0.140 > 0.1) (Fig. 2). The forest plot found that smokers have lower mortality compared to non-smokers (HR: 0.77; 95% CI: 0.61–0.96), and the overall effect was 2.37 (P = 0.018 < 0.05), showing a statistically significant difference between the groups.

Forest plot regarding the risk of death between smokers vs. non-smokers with out-of-hospital cardiac arrest
Sensitivity analysis and funnel plot analysis
Sensitivity analysis regarding mortality risk indicated that results did not significantly change due to the impact on each study (Fig. 3). Funnel plots indicated symmetrical distribution in this study, which suggested no significant evidence of bias in all included publications (Fig. 4). Egger’s regression asymmetry tests showed no significant bias among the five studies (P = 0.65 > 0.05).

Sensitive analysis regarding the risk of death between smokers and non-smokers with out-of-hospital cardiac arrest

Funnel plot of the included publications
Discussion
This meta-analysis systematically evaluated the latest evidence regarding the comparison of mortality between smokers and non-smokers after they experienced OHCAs. Upon the inclusion of 2477 patients from a compilation of five studies, this study revealed a notably diminished mortality risk among smokers compared to non-smokers following OHCAs. These findings allude to the presence of a phenomenon commonly referred to as the ‘smoker’s paradox’. However, this phenomenon still awaits validation in subsequent large, high-quality studies.
Patients with OHCAs have high mortality rates and experience considerable healthcare costs. Many studies explored the factors that influenced the prognosis of OHCAs. For instance, previous meta-analyses demonstrated that women experienced slight differences among those who survived OHCAs and were discharged [30]. Patients who underwent cardiopulmonary resuscitation before arriving at the hospital had an increased 30-day survival after OHCAs [20]. Previous studies may have suggested a potential association between smoking and unfavourable outcomes regarding OHCA-related mortality. No single epidemiological meta-analysis contradicts the increased risk of smoking regarding mortality from OHCA. Smoking is well known to be bad for public health, whereas this study’s results showed smokers had lower mortality rates than non-smokers, thus named the ‘smoker's paradox’.
The smoker's paradox was recognized a few decades ago in patients with acute myocardial infarction [31], and its existence has been continuously reported in subsequent studies. In 2017, data derived from the 2013–2016 China Acute Myocardial Infarction Registration study, encompassing 40,640 patients diagnosed with acute myocardial infarction and conducted by Fuwai Hospital, unveiled a noteworthy observation. The findings indicated that smoking persisted as a mitigating factor in in-hospital mortality [32]. A recent study found that a patient’s current smoking status is related to lower susceptibility to COVID-19 infection [33]. A pooled analysis of 10 randomised studies published in the Journal of the American College of Cardiology in 2020 of patients with ST-elevation myocardial infarction undergoing coronary intervention found that smokers had lower mortality rates within 1 year than non-smokers. Smokers had higher mortality risk after adjustments for age and other risk factors, and the results suggested short-term prognosis was better in smoking patients who suffered heart attacks simply because smokers were younger and had fewer cardiovascular risk factors [34].
However, the independent association between smoking and favourable outcomes after cardiac arrest remains unknown. It is understood that smoking may protect against ischemic injury, as the lack of oxygen caused by smoking may produce an ischemic precondition that could reduce the mortality of ischaemia–reperfusion injury. Ischemic conditioning was originally described by Murry et al. [35]. Hausenoly et al. [36] discovered that when transient nonfatal ischaemia and reperfusion were applied to the organ or tissue bed, it could prevent future reperfusion injury. Recent clinical studies showed that ischemic conditioning was beneficial in alleviating ischemic reperfusion [37,38,39]. Reperfusion is essential in maintaining vital signs and survival. In addition, studies suggested that acute myocardial infarction was the leading cause of cardiac arrest in patients. Smoking can reduce the infarction size by decreasing ischaemia reperfusions [40]. A new HUNT study from Norway discovered that both current and former smokers had lower levels of high-sensitivity cardiac troponin I (hs-cTnI) than non-smokers, and there existed a dose–response relationship between hs-cTnI and smoking in past smokers. It could be possible that the composition of tobacco could induce ischaemia preconditioning, which would make the heart muscle more resistant to ischemic damage and have a protective effect on the heart. This was found in smokers, which could partly explain the ‘smoker’s paradox’ [41].
Strengths and limitations
This meta-analysis has some limitations that must be acknowledged. First, most of the results were based on unadjusted estimates; therefore, future studies should evaluate the impact of other known confounding variables, such as gender, age, body mass index and lifestyle, on the risk of mortality from OHCA among smokers. Second, despite the low heterogeneity found across publications, the study cannot rule out the possibility that other inadequately measured factors may bias the associations. Third, former smokers, current smokers, packs of cigarettes per day and total years of smoking were not reported in this study, so it was impossible to perform a detailed differentiation between patients. Therefore, future studies that research mortality from smoking and OHCA are needed.
However, there are many advantages to this study. Two researchers independently assessed the quality of the included studies using the NOS, and publication bias was evaluated by a funnel plot analysis together with Egger’s test, which provided criteria to evaluate the methodological quality of the studies. To accurately identify the relationship between the mortality from OHCA and smoking, the heterogeneity and sensitivity of the results were analysed in this study.
Conclusion
This is the first systematic review and meta-analysis on the association between cigarette smoking and mortality in patients with OHCA. The results would suggest that smokers had lower mortality than non-smokers. However, due to a lack of data, the ‘smoker’s paradox’ is not a definitive concept, and other covariate effects require further consideration and analysis. Efforts are needed to initiate large multi-centre, randomised, prospective clinical trials to evaluate the association between smoking and mortality after OHCAs. In addition, attention should be given to the research on ischemic preconditioning to promote the diagnosis and treatment of OHCAs.
References
Myat A, Song KJ, Rea T. Out-of-hospital cardiac arrest: current concepts. Lancet. 2018;391(10124):970–9. https://doi.org/10.1016/S0140-6736(18)30472-0.
Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics-2023 Update: A Report from the American Heart Association. Circulation. 2023;147(8):e93–621. https://doi.org/10.1161/CIR.0000000000001123.
Choi Y, Park JH, Jeong J, Kim YJ, Song KJ, Shin SD. Extracorporeal cardiopulmonary resuscitation for adult out-of-hospital cardiac arrest patients: time-dependent propensity score-sequential matching analysis from a nationwide population-based registry. Crit Care. 2023;27(1):87. https://doi.org/10.1186/s13054-023-04384-y.
Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, et al. Heart Disease and Stroke Statistics-2022 Update: A Report From the American Heart Association. Circulation. 2022;145(8):e153–639.
Pareek N, Rees P, Quinn T, et al. British cardiovascular interventional society consensus position statement on out-of-hospital cardiac arrest 1: pathway of care. Interv Cardiol. 2022;17:e18. https://doi.org/10.15420/icr.2022.09.
Gräsner JT, Wnent J, Herlitz J, et al. Survival after out-of-hospital cardiac arrest in Europe—results of the EuReCa TWO study. Resuscitation. 2020;148:218–26. https://doi.org/10.1016/j.resuscitation.2019.12.042.
Shao F, Li CS, Liang LR, Li D, Ma SK. Outcome of out-of-hospital cardiac arrests in Beijing, China. Resuscitation. 2014;85(11):1411–7. https://doi.org/10.1016/j.resuscitation.2014.08.008.
Kang Y, Chen T, Mui D, Ferrari V, Jagasia D, Scherrer-Crosbie M, et al. Cardiovascular manifestations and treatment considerations in COVID-19. Heart. 2020;106(15):1132–41.
Zou X, Chen K, Zou J, Han P, Hao J, Han Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med. 2020;14(2):185–92.
GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885–1906 https://doi.org/10.1016/S0140-6736(17)30819-X
Organization WH. WHO report on the global tobacco epidemic 2017: Monitoring tobacco use and prevention policies - eScholarship. 2017.
Mackenbach JP, Damhuis RA, Been JV. The effects of smoking on health: growth of knowledge reveals even grimmer picture. Ned Tijdschr Geneeskd. 2017;160:D869.
Koronaiou K, Al-Lawati JA, Sayed M, Alwadey AM, Alalawi EF, Almutawaa K, et al. Economic cost of smoking and secondhand smoke exposure in the Gulf Cooperation Council countries. Tob Control. 2021;30(6):680–6.
Boachie MK, Rossouw L, Ross H. The economic cost of smoking in South Africa, 2016. Nicot Tob Res. 2021;23(2):286–93.
John RM. Economic costs of diseases and deaths attributable to bidi smoking in India, 2017. Tob Control. 2019;28(5):513–8.
Lee H, Oh J, Kang H, Lim TH, Ko BS, Choi HJ, et al. Association between the body mass index and outcomes of patients resuscitated from out-of-hospital cardiac arrest: a prospective multicentre registry study. Scand J Trauma Resuscit Emerg Med. 2021;29(1):24.
Mohr GH, Søndergaard KB, Pallisgaard JL, Møller SG, Wissenberg M, Karlsson L, et al. Survival of patients with and without diabetes following out-of-hospital cardiac arrest: a nationwide Danish study. Eur Heart J Acute Cardiovasc Care. 2020;9(6):599–607.
Arunachalam K, Zhang Z, Chu A, Maan A. Impact of racial and gender variations in patients with out-of-hospital cardiac arrest: a nation-wide study. Crit Pathw Cardiol. 2021;20(1):25–30.
Bell SM, Kovach C, Kataruka A, Brown J, Hira RS. Management of out-of-hospital cardiac arrest complicating acute coronary syndromes. Curr Cardiol Rep. 2019;21(11):146.
Hirlekar G, Jonsson M, Karlsson T, Bäck M, Rawshani A, Hollenberg J, et al. Comorbidity and bystander cardiopulmonary resuscitation in out-of-hospital cardiac arrest. Heart (British Cardiac Society). 2020;106(14):1087–93.
Mourão Carvalho N, Martins C, Cartaxo V, et al. Out-of-hospital cardiac arrest in the Algarve region of Portugal: a retrospective registry trial with outcome data. Eur J Emerg Med. 2022;29(2):134–9. https://doi.org/10.1097/MEJ.0000000000000885.
Bray J, Howell S, Ball S, et al. The epidemiology of out-of-hospital cardiac arrest in Australia and New Zealand: a binational report from the Australasian Resuscitation Outcomes Consortium (Aus-ROC). Resuscitation. 2022;172:74–83. https://doi.org/10.1016/j.resuscitation.2022.01.011.
Lahmann AL, Bongiovanni D, Berkefeld A, Kettern M, Martinez L, Okrojek R, et al. Predicting factors for long-term survival in patients with out-of-hospital cardiac arrest—a propensity score-matched analysis. PLoS ONE. 2020;15(1):e0218634.
Stang A. Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5.
Albizreh B, Arabi A, Al Suwaidi J, Patel A, Singh R, Albinali H. Out-of-hospital cardiac arrest in the young: a 23-year middle eastern experience. Heart views. 2021;22(1):3–7.
Pollock JS, Hollenbeck RD, Wang L, Janz DR, Rice TW, McPherson JA. A history of smoking is associated with improved survival in patients treated with mild therapeutic hypothermia following cardiac arrest. Resuscitation. 2014;85(1):99–103.
Arrich J, Sterz F, Fleischhackl R, Uray T, Losert H, Kliegel A, et al. Gender modifies the influence of age on outcome after successfully resuscitated cardiac arrest: a retrospective cohort study. Medicine. 2006;85(5):288–94.
Leick J, Liebetrau C, Szardien S, Fischer-Rasokat U, Willmer M, van Linden A, et al. Door-to-implantation time of extracorporeal life support systems predicts mortality in patients with out-of-hospital cardiac arrest. Clin Res Cardiol. 2013;102(9):661–9.
Whittaker A, Lehal M, Calver AL, Corbett S, Deakin CD, Gray H, et al. Predictors of inhospital mortality following out-of-hospital cardiac arrest: Insights from a single-centre consecutive case series. Postgrad Med J. 2016;92(1087):250–4.
Malik A, Gewarges M, Pezzutti O, Allan KS, Samman A, Akioyamen LE, et al. Association between sex and survival after non-traumatic out of hospital cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2022;179:172–82.
Kelly TL, Gilpin E, Ahnve S, Henning H, Ross J Jr. Smoking status at the time of acute myocardial infarction and subsequent prognosis. Am Heart J. 1985;110(3):535–41.
Xu H, Li W, Yang J, Wiviott SD, Sabatine MS, Peterson ED, et al. The China Acute Myocardial Infarction (CAMI) Registry: a national long-term registry-research-education integrated platform for exploring acute myocardial infarction in China. Am Heart J. 2016;175:193-201.e3.
Paleiron N, Mayet A, Marbac V, Perisse A, Barazzutti H, Brocq FX, et al. Impact of tobacco smoking on the risk of COVID-19: a large scale retrospective cohort study. Nicot Tobacco Res. 2021;23(8):1398–404.
Redfors B, Furer A, Selker HP, Thiele H, Patel MR, Chen S, et al. Effect of smoking on outcomes of primary PCI in patients With STEMI. J Am Coll Cardiol. 2020;75(15):1743–54.
Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74(5):1124–36.
Hausenloy DJ, Yellon DM. Ischaemic conditioning and reperfusion injury. Nat Rev Cardiol. 2016;13(4):193–209.
Verouhis D, Sörensson P, Gourine A, Henareh L, Persson J, Saleh N, et al. Long-term effect of remote ischemic conditioning on infarct size and clinical outcomes in patients with anterior ST-elevation myocardial infarction. Catheter Cardiovasc Interv. 2021;97(3):386–92.
Akkoca M, Usanmaz SE, Tokgöz S, Köksoy C, Demirel-Yilmaz E. The effects of different remote ischemic conditioning on ischemia-induced failure of microvascular circulation in humans. Clin Hemorheol Microcirc. 2018;70(1):83–93.
Kloner RA, Shi J, Dai W, Carreno J, Zhao L. Remote ischemic conditioning in acute myocardial infarction and shock states. J Cardiovasc Pharmacol Ther. 2020;25(2):103–9.
Symons R, Masci PG, Francone M, Claus P, Barison A, Carbone I, et al. Impact of active smoking on myocardial infarction severity in reperfused ST-segment elevation myocardial infarction patients: the smoker’s paradox revisited. Eur Heart J. 2016;37(36):2756–64.
Skranes JB, Lyngbakken MN, Hveem K, Rosjo H, Omland T. Tobacco consumption and high-sensitivity cardiac troponin i in the general population: the HUNT study. J Am Heart Assoc. 2022;11(2):e021776.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
CY and NZ designed the meta-analysis. PZ, YL and GY searched for the articles, screened titles and abstracts, and extracted the relevant data. CY and PZ performed the statistical analysis and interpretation of data. YL and GY contributed to the conception of the study. CY and NZ drafted the manuscript. NZ critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
As all analyses were based on previously published studies, no ethical approval or patient consent was required.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Zhang, N., Liu, YJ., Yang, C. et al. Comparison of smokers’ mortality with non-smokers following out-of-hospital cardiac arrests: a systematic review and meta-analysis. J Health Popul Nutr 43, 57 (2024). https://doi.org/10.1186/s41043-024-00510-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-024-00510-w