
Abstract
Background
Stunting is associated with socioeconomic status (SES) which is multidimensional. This study aimed to compare different SES indices in predicting stunting.
Methods
This was the secondary data analysis using Tanzania Demographics and Health Surveys (TDHS). The study used 7492, 6668, and 8790 under-five-year children from TDHS 2004/5, 2010, and 2015/16, respectively. The Household Wealth Index (HWI); Water and Sanitation, Assets, Maternal education and Income (WAMI); Wealth Assets, Education, and Occupation (WEO); and the Multidimensional Poverty Index (MPI) indices were compared. The summated scores, principal component analysis (PCA), and random forest (RF) approaches were used to construct indices. The Bayesian and maximum likelihood multilevel generalized linear mixed models (MGLMM) were constructed to determine the association between each SES index and stunting.
Results
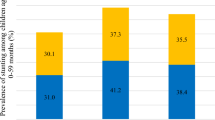
The study revealed that 42.3%, 38.4%, and 32.4% of the studied under-five-year children were stunted in 2004/5, 2010, and 2015/16, respectively. Compared to other indicators of SES, the MPI had a better prediction of stunting for the TDHS 2004/5 and 2015/16, while the WAMI had a better prediction in 2010. For each score increase in WAMI, the odds of stunting were 64% [BPOR = 0.36; 95% CCI 0.3, 0.4] lower in 2010, while for each score increase in MPI there was 1 [BPOR = 1.1; 95% CCI 1.1, 1.2] times higher odds of stunting in 2015/16.
Conclusion
The MPI and WAMI under PCA were the best measures of SES that predict stunting. Because MPI was the best predictor of stunting for two surveys (TDHS 2004/5 and 2015/16), studies dealing with stunting should use MPI as a proxy measure of SES. Use of BE-MGLMM in modelling stunting is encouraged. Strengthened availability of items forming MPI is inevitable for child growth potentials. Further studies should investigate the determinants of stunting using Bayesian spatial models to take into account spatial heterogeneity.
Similar content being viewed by others
Introduction
Over decades, stunting among under-five-year children has been a global health concern. Stunting is defined as poor linear growth among under-five-year children which hinders child growth potentials [1, 2]. Stunting leads to poor participation in production activities and academic performance due to reduced school attendance [3] and accelerates repeated infections [4]. Furthermore, stunting leads to deaths and injuries [5] which in turn increases health spending among the economically disadvantaged population. Compared to other forms of undernutrition, stunting is the general indicator of child’s overall levels of undernutrition and poor life quality [6]. Additionally, compared to other forms of undernutrition, the observed higher prevalence of stunting at both global and national levels over decades [7] requires further investigation.
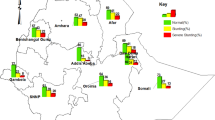
Globally, it was estimated that 149.2 (22%) million under-five-year children were stunted in 2021 [7]. In 2017, approximately 2% of 155 million stunted children lived in high-income countries while about 50% lived in low-income countries [8]. Out of 155 million stunted children in 2017, about 59 million lived in Africa of which 24 million lived in Eastern Africa [8]. These figures imply that despite global efforts to reduce stunting, progress has been uneven and slow, especially in low-income countries and regions. Tanzania, being one such country, experiences a high burden of stunting that varies across regions and districts. In Tanzania, stunting declined too slowly from 34 to 31.8% in 2016 and 2018, respectively [9]. According to the WHO-UNICEF classification [7], the prevalence of stunting in Tanzania was very high (above 30%) in 26 regions and above 40% in 6 regions [9]. In these aspects, we should not be comfortable with the overall trend of stunting at a national level, as it conceals the larger disparity within and between regions. The observed uneven distribution of stunting is underlined by the fact that diseases occur at random and have different causal pathways, triggered by interaction between socioeconomic factors [10,11,12].
Different SES indices for predicting health outcomes have been developed including single indices like maternal education [10, 13,14,15], income [10, 15, 16] and multivariate indices like wealth assets [13, 17, 18], WEO [12, 15], WAMI and MPI [13, 15]. Health outcomes including stunting do not occur at random, as socioeconomic determinants are unevenly distributed. The fact that SES variables interact differently when causing diseases, necessitates the establishment of the best indicator of SES associated with stunting rather than using the known measure of SES (HWI). Knowing the SES index associated with stunting could be useful for developing targeted and focused interventions in developing countries including Tanzania.
The mostly used proxy of SES at the household level is the Household Wealth Index (HWI) [10, 13, 19,20,21,22]; however, this index does not include mother’s education [12, 13, 21] and occupation [12] which are important indicators of SES. Other indices include the availability of safe Water and sanitation, Assets, Maternal education and Income (WAMI) and the Multidimensional Poverty Index (MPI) [13]. The multicountry study conducted in Africa assessing the measurement of socioeconomic status in relation to stunting revealed that the WAMI index had a statistically significant negative relationship with stunting [13]. The HWI and maternal education had a negative association with stunting, as children from poor-wealth households and born from uneducated mothers had higher odds of being stunted as compared to children from highest-wealth quintile households [19, 21, 23,24,25,26,27,28,29,30,31]. In Tanzania, most studies use HWI as an indicator of SES [27, 32,33,34,35,36], ignoring the possible correlation between HWI and other indicators of SES including occupation and maternal education. However, the findings that WAMI predicted stunting better than maternal education, HWI and MPI [13] were limited to children living in Haydom district, Manyara region, hence lacking generalizability to the whole country. Furthermore, the study [13] did not compare the WEO with other SES indices.
Furthermore, despite the available advanced statistical modelling techniques of child stunting like the multilevel generalized linear mixed models (MGLMM) still are not sufficiently utilized in Tanzania. Most studies use classical regression models (logistic and linear) [28, 36,37,38,39,40,41,42,43] and very little on the MGLMM [32] which use the maximum likelihood estimation (MLE) techniques. The multilevel models take into account unmeasurable factors [44, 45] and control the correlation between subjects and geographical areas using random effects [32]. However, compared to MLE multilevel generalized linear mixed models (MLE-MGLMM), the Bayesian Estimation -MGLMM (BE-MGLMM) produces unbiased estimates even in areas with smaller sample sizes [46, 47]. Additionally, the BE-MGLMM produces unbiased estimates even at level two where the MLE- MGLMM may lead to biased estimates [48]. The fact that mother–child pairs living in the same geographic areas may share common characteristics concerning stunting and that some enumeration areas may have fewer observations raises concern of using BE-MGLMM. If this analysis is not used, we should expect underestimated standard errors, hence an increased likelihood of committing type one error [44]. Therefore, this study aimed to compare the SES indices in predicting stunting among under-five-year children in Tanzania accounting for correlation at regional and enumeration areas using the MLE-MGLMM and the BE-MGLMM.
Methods
Data source
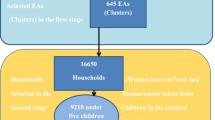
The data used in this study were obtained from TDHS. The study used the 2004/5, 2010 and 2015/16 TDHS datasets being the recent surveys. The study used three surveys to determine the consistency of the constructed indices in predicting stunting. The DHS used a two-stage sampling technique to select households for study after stratifying the study areas into rural or urban in each region. The two-stage sampling started by selecting Primary Sampling Units (PSUs) from the most recent census enumeration areas (EAs). After selecting the PSUs from strata using the probability proportional to size, then a fixed number of households was selected from each PSU using equal probability systematic sampling. The detailed methodology for the DHS data collection and analysis was documented [49, 50].
The DHS collects information at the household level, on men and women of reproductive age who slept in the household a night before the survey. Of women aged 15–49 years, their children eligible for the study, their birth records and anthropometric measurements of both mothers and under-five children are taken. The unit of analysis for this study is a child–mother pair. The survey recruits women aged 15–49 years, and their respective under-five-year children are interviewed. The study merged the household member, household, individual and child recode datasets for each survey year using unique identifiers. The study inclusion criteria were children aged 0–59 months, while the exclusion criteria were children not living with their mothers, children with missing and out of range measurements of Height for Age Z-scores (HAZ) used for computing stunting status.
Measurement of variables
The outcome of interest was stunting, classified as stunted if the child’s HAZ score was below–2.0 standard deviation (SD), otherwise not stunted [51]. The selection of independent variables was based on previous studies classified into three basic groups namely; child, maternal, and household covariates. Child covariates include sex, age (coded: 0–11 months, 12–33 and 34–49 months), size at birth (coded: small, medium and large), birth order [52], and self-reported diarrhoea status (coded as yes or no). A child was considered diarrheic if had loose stool more frequently than usual in two weeks Maternal characteristics included age [36], age at birth, breastfeeding duration, frequency of use of Antenatal Care (ANC) services, maternal BMI (coded: 0 “below 18.5” and 1 “at least 18.5” kg/m2) [52, 53], work status and age at first birth [52]. Household characteristics included the number of under-five children, household size, area of residence (rural or urban), and wealth index [54, 55]. The coding for each study variable is presented in appended Table 6.
The random variables included enumeration areas (EAs) and regions. The EAs are defined based on rural–urban areas perspective. In urban area, an EA may be a block or apartment building, while in rural areas it can either be a village or a group of villages. The DHS randomly selects EAs as adopted from the previous national census surveys. Based on regions, Tanzania had a total number of 26 regions by 2015. However, the composition of these regions in terms of geographical boundaries has been varying over time due to the changes in political regime and need for distribution of socioeconomic services. A detailed description on EAs and regions for each survey year are detailed [49, 50].
Statistical analysis
Descriptive analysis
The weighted and unweighted frequencies were presented in a frequency distribution table. The study used the Chi-square test of independence to determine the association between the selected socioeconomic categorical covariates and stunting status. The Pearson correlation coefficient was used to evaluate the relationship between constructed SES indices.
Constructing SES indices
The household’s SES was constructed in four different indices namely the HWI, WAMI, WEO and MPI. These SES indices were constructed using the summated scores and principal component analysis (PCA) aided by the random forest (RF) technique for variable selection. The HWI was computed using PCA, while the WAMI, WEO and MPI were computed using both PCA and summated score. The RF was used to select the best eight wealth assets associated with stunting. Further description on computing SES indices using both summated score and PCA is presented.
Constructing SES indices using summated scores
The computation of WAMI, WEO and MPI includes independent variables like mother’s education, occupation, wealth assets and water and sanitation services. The mothers education was coded according to the UNESCO 2011 international standard classification of the level of education [56] while the occupation was classified according to the international standard classification of occupation [57] and upgraded relative to the importance of Tanzania. Occupation was grouped into four categories, namely; unskilled, semi-skilled, skilled and professional. The four categories were assigned weights ranging from 1 to 4, respectively [12]. Mother’s level of education was classified as uneducated, did not complete primary, completed primary, did not complete secondary, and completed secondary as well as completed higher education [12, 58]. These levels of education were assigned weights from 0 to 5, respectively [12]. Each wealth asset was coded as a binary variable, the RF was used to select the best 8 assets associated with stunting [13]. While other wealth assets were assigned a unit weight [59], car and land ownership were assigned weights 0.1 and 0.5, respectively [12]. Then, the summated score for the WEO index as adopted from [12, 59] was expressed as:
The second proxy indicator of SES was the WAM index, constructed using wealth assets, availability of improved water and toilets as well as maternal education. The availability of improved water and toilets formed the WASH index, which was then combined with maternal education and wealth assets. A household was termed having improved water and toilets according to WHO standards [60, 61]. The improved water and toilets were dummies thus each assigned a weight of four which then totaled 8 when forming the Water, Sanitation and Hygiene (WASH) score [13]. The maternal education was formed using years of education, the maximum being 16 years and then was divided by 2 to get the maximum score of 8. The best 8 assets associated with stunting were selected using the RF [13], then combined with WASH and maternal years of schooling to form the WAMI. Ever since DHS does not collect household income, this index did not consider income. Household income can be collected using actual income or proxy indicators like consumption and expenditure; however, its collection is difficult [59, 62] specifically in developing countries. Thus, the WAMI index adopted from [13] was expressed as: \(\mathrm{WAMI}=\mathrm{WASH}+\mathrm{Assets}+\mathrm{Education}\).
Based on the MPI, each of the wealth assets ownership was coded as a dummy. A household was considered educated if either a mother is educated or a child attends school and was otherwise uneducated. Furthermore, whether a household had under-five death, as well as mother being undernourished were used. Child nutrition status being an indicator of MPI was not included because it was the dependent variable for this study. To reflect the poverty nature of MPI, the lack of ownership of a particular item was coded as 1 while owning a particular item was coded as 0. Therefore, the study expects the MPI to have opposite sign as compared to WAMI, WEO and HWI when predicting stunting.
Constructing SES indices using principal component analysis
The PCA is a variable reduction method used to identify correlated items, grouping them in similar constructs, thereby forming fewer dimensions or components [62]. Different studies used PCA in computing SES indices [62,63,64] for evaluating health problems. Normally, the first component has the largest eigenvalue representing the largest amount of variation in the original data [62]. Thus, the first component is a proxy of the particular index under consideration [62, 64]. For each SES index identified in the previous section, its corresponding items were expressed as dummy variables and then PCA was applied. Each SES index was modelled independently, and the first component was predicted and hence used for further analysis [62,63,64]. The obtained indices were used in their original forms, and no quintiles were developed.
Statistical modelling
The statistical modelling of this study was centralized on the GLMMs. The GLMM typically use numerical optimization techniques to estimate model parameters and maximum likelihood estimation (MLE) is the most common method. Recently, the modelling of human health is featured in with the Bayesian estimation frameworks. This section provides a summarized explanation on the GLLMs and its corresponding estimation approaches, namely the MLE and Bayesian methods.
Generalized linear mixed models
The analysis of this study was centred on the generalized linear mixed models (GLMM) which extends the idea of generalized linear models (GLM). The GLM uses the linear predictor for the random and fixed effects under the assumption that the data are normal [65]. However, in some instances, the dependent variable is non-normal and the data have random effects, and then the GLMM are preferred [66]. Stunting status is a binary outcome following the Bernoulli distribution, and still child health characteristics are influenced the nested structure of EAs and regions hence requiring the use of binary logit mixed models which are under the umbrella of GLMM.
The study assumed that children born to the same mother, or children living with the same enumeration area (EA) or region may share common characteristics attributable to their stunting status. Thus, children may be nested within EA and EA may be nested within in regions. The nesting structure of children being nested to mothers formed level 1, the nesting structure of children being nested on EA formed level 2 while the nesting structure of regions formed level 3. A detailed expression on the named three models is presented under the specification of the mathematical models section.
Maximum likelihood approach
The MLE is one of the parameter estimation methods which utilizes the observed data to determine the parameter which maximizes the likelihood [67,68,69]. The parameters values are computed in a manner of being most likely to represent the observed data [67,68,69]. The MLE provides a simultaneous estimation approach of the fixed and random parameter [69]. However, the MLE works best in presence of larger sample sizes. In case of small sample sizes, the estimates are negatively biased [70] and sometimes the model may fail to converge.
In evaluating the parameter that maximizes the likelihood given the observed data, the MLE operates under two conditions; namely the first partial derivative known as the differential equation should be equal to zero and the second partial derivative should be less than zero. Mathematically, if we let \(L\left[\theta /x\right]\) be the likelihood function,\(\theta\); be the parameter value to be estimated from the observed data \(x\), then the two conditions as adopted from [67] may be summarized as follows;
The first condition aims at satisfying the existence of the parameter under MLE (\({y}_{MLE}\) \({\uptheta }_{\mathrm{MLE}}\) \({\uptheta }_{\mathrm{MLE}}\)) while the second condition aims at making sure that the \({y}_{MLE}\) \({\theta }_{\mathrm{MLE}}\) \({\theta }_{\mathrm{MLE}}\) is the maximum parameter value [67]. The MLE algorithm seeks to maximize the likelihood function, which measures how well the model explains the observed data.
Bayesian inference approach
The Bayesian model uses the prior distribution to update the posterior distribution when estimating the parameters. The prior information as obtained from the prior distribution represents the prior assumption about the parameter being estimated. The prior distribution influences the posterior distribution which represents the updated degree of uncertainty after analysing the particular data. If \(X\) represents a random variable (stunting status) with the density function \(f(x|\theta )\), the prior distribution with the density function \(f(\theta )\); the density function \(f\left(\theta |x\right)\) of the posterior distribution using Bayes theorem as adopted [71] may be computed.
\(f\left(\theta |x\right)=\frac{f(x|\theta )f(\theta )}{\sum f\left(x|\theta \right)f\left(\theta \right)d\theta }\). Where \(f(x|\theta )\) is defined as the likelihood function.
Normally, the posterior distribution is the product of the likelihood and the density of the prior distribution, expressed as \(f\left(\theta |x\right)=L\left(\theta \right)f(\theta )\). Because stunting status follows the binomial distribution, the log link function was used when estimating the odds of stunting.
Based on the prior distribution, either the non-informative or the informative priors may be used [72, 73]. However, the informative priors may lead to biased estimates if not carefully chosen, or even obtained in sources where they are weakly defined [74] [75]. Additionally, compared to informative priors, non-informative priors provide a larger number of parameters to be estimated [76], and have minimum influence on the posterior distribution [71]. In such instances, the diffuse/non-informative prior are preferred [72]. The study used the flat diffuse normal priors with the distribution (0, 10,000) for fixed effect estimates and the inverse gamma priors for the higher hierarchical orders (hyperparameters) with the distribution (0.01, 0.01). In updating the posterior distribution, 10,000 simulations were conducted for each model at a burn-in of 2500.
The specification of mathematical models
The study estimated both the BE-MGLMM and MLE-MGLMM to assess the association between SES indices and stunting. The hierarchical nature of data was considered as children living in the same enumeration area or region may have the same characteristics towards acquiring stunting. Thus, children were nested in enumeration areas and enumeration areas were nested in regions. The standard logistic regression model without hierarchy, the two and three-level hierarchical model was constructed and compared. The hierarchy was based on the fact that enumeration areas were nested in regions. The three models namely the [1] standard logistic regression, [2] random effect model and [3] nested random effect model.
Model 1: \(\mathrm{log }\left({p}_{ij}/{1-p}_{ij}\right)={\beta }_{0}+ \beta X\)
Model 2: \(\mathrm{log }\left({p}_{ij}/{1-p}_{ij}\right)={\beta }_{0}+ \beta X+ {\mu }_{j}\)
Model 3: \(\mathrm{log }\left({p}_{ijk}/{1-p}_{ij}k\right)={\beta }_{i}{X}_{k|j}+ {\beta }_{j}X+ {\mu }_{k|j}+ {\mu }_{j}\)where \(\mathrm{log }\left({p}_{ij}/{1-p}_{ij}\right)\) is the log odds of stunting for child \(i\) living in region \(j\). \(\mathrm{log }\left({p}_{ijk}/{1-p}_{ijk}\right)\) is the log odds of stunting for child \(i\) in region \(j\) and enumeration area \(k\). \(X{\prime}s\) are the covariates. \(\beta {\prime}s\) are the regression coefficient. \({\beta }_{j}X\) shows the extent to which region affects the slope of \(X\). \({\beta }_{i}{X}_{k|j}\) shows the extent to which enumeration area affects the slope of \(X\) in a given similar region. \({\mu }_{i}\) is the is a vector of variances for each random effect (regions) associated with stunting. \({\mu }_{k|j}\) is the random effect capturing showing the variation due to different enumeration area \(k\) within a common region \(j\). \(X\) is the SES index under consideration.
The three models, namely level 1 (children nested in mother), level 2 (children nested in EAs), and level 3 (EAs nested in regions), were compared using Akaike information criterion (AIC) and the deviance information criterion (DIC) for MLE-MGLMM and BE-MGLMM, respectively. The model with three levels was revealed parsimonious due to lower AIC and DIC for MLE-MGLMM and BE-MGLMM, respectively. The Bayes prefix was used when conducting the B-MGLM. The obtained estimates for the B-MGLM were reported as Bayesian posterior odds ratio (BPOR) [77, 78] instead of the known posterior mean. The obtained results for the MLE-MGLMM were reported as odds ratio. Furthermore, the flexibility of Bayesian models to update the prior distribution ignores the need for sampling weights even for complex surveys [79, 80]. In this aspect, the study used unweighted samples. For the case of MLE-MGLMM, the Akaike information criterion (AIC) was used to decide on the best index predicting stunting. The rule of thumb is that the lower the AIC, the better the model. All analyses were conducted using STATA version 15.
Results
Participant’s demographic characteristics
The study revealed that out of 7492, 6806 and 8929 children, approximately 42.3%, 40.2% and 33% were stunted in 2004/5, 2010 and 2015/16, respectively. Of those who were stunted in 2010, 5219 (79.11%) lived in rural areas, 1699 (24.27%) lived in richer wealth quintile households, and 4290 (68.2%) were born to mothers with primary education. For the case of TDHS 2015/16, the study revealed that out of 2991 stunted children, 6911 (74.13%) were among those living in rural areas, 2069 (24.7) lived in the poorest wealth quintile households and 5368 (64.5) were among children born to mothers with primary education (Table 1).
Based on the distribution of stunting across the selected socioeconomic variables, the study revealed that the majority were 2129 [41.8], 1954 [38.2%] and 2363 [34.8] among children living in rural areas for survey years 2004/5, 2010 and 2015/16, respectively. The majority of stunted children were 956 [44.9%], 434 [40.3%] and 691 [37.8] among children living in the richest, poorer and poorer wealth quintile households for survey years 2004/5, 2010 and 2015/16, respectively. Furthermore, the study revealed that in all survey years, the majority of stunted children were 2667 [43.1%], 2212 [39.9%], and 2306 [33.6%] among children born to currently working mothers. A statistically significance difference between groups was observed for the mother’s education and the mother’s work status in all survey years. The rural–urban differences were statistically significant for survey years 2004/5 and 2015/16, while the wealth index was statistically significant for the 2015/16 survey (Table 2).
The association between SES indices and stunting
The association between SES indices and stunting was determined using the MLE-MGLM and B-MGLM as presented in Tables 3 and 4. Based on the AIC for selecting the best SES index in predicting stunting, the study revealed that MPI, HWI(overall) and MPI had lower AIC as compared to other indices for TDHS 2004/5, 2010 and 2015/16, respectively. For instance, the MPI had the lowest AIC of 11,567.5 as in 2004/5. In the 2010 survey, the HWI (overall) had a minimum AIC of 9757.9 in 2015/16, while the MPI had a minimum AIC of 11,919.1 as compared to other indices. The study observed a non-statistical significance association between SES indices and stunting hence the MPI having lower AIC was the best for the TDHS 2004/5. For the case of TDHS 2010, the lower AIC was for HWI (overall); however, the association was not statistically significant. For the case of 2015/16, all indices were statistically significant at p < 0.001, and the MPI having the lowest AIC was used (Table 4).
Based on Table 3, the study revealed that each unit increase in MPI, the odds of stunting was 1% [OR = 0.99; 95% CI 0.96, 1.02] lower in 2004/5, however not statistically significant at even 5% level. For the case of 2010 TDHS, the study revealed that for each unit increase in HWI (overall), the odds of stunting declined by 1% [OR = 0.99; 95% CI 0.97, 1]; however, the association was not statistically significant even at a 5% level. In 2015/16, for each unit increase in MPI, the odds of stunting were statistically significantly increased by 1 [OR = 1.13; 95% CI 1.09, 1.16] at p < 0.001.
Based on the B-MGLM, we revealed that the MPI was the best predictor of stunting for the survey years 2004/5 and 2015/16, respectively. For the survey year 2010, the WAMI was the best index in predicting stunting due to its lower AIC as compared to other indices. As expected, the HWI, WAMI and WEO had a reducing effect on stunting for each unit score increase. Similarly, the MPI revealed an expected positive relationship with stunting, as each unit increase in MPI the odds of stunting increased (Table 4).
Compared to the MLE-MGLM, the B-MGLM had the capacity of producing variances for both the region and enumeration area random effects. The MLE-MGLM produced only variances for region-level random effects. However, results for variances pertaining to random effects were not reported in this paper. These estimates are available upon request.
From Tables 3 and 4, the study revealed that stunting was best predicted by the MPI for survey years 2004/5 and 2015/16, while the WAMI was the best for the TDHS 2010. Then, the multivariable analysis was conducted to oversee the behaviour of these indices adjusted for other covariates. Both the MLE-MGLMM and BE-MGLMM were used to model the association between the MPI and WAMI controlling for other variables. These variables included the child, maternal and household characteristics as described in Table 5.
The study revealed that even after adjusting for other covariates, the effect of WAMI and MPI remained statistically significant for survey years 2010 and 2015/16, respectively. Still, stunting had a positive and negative association with the WAMI and the MPI, respectively. For instance, based on the results of the BE-MGLMM, the study revealed that for each unit increase in the WAMI, there was 64% [BPOR = 0.36; 95% CCI 0.3, 0.4] lower odds of a child to be stunted in 2010. Furthermore, for each unit increase in MPI, there was 1 [BPOR = 1.1; 95% CCI 1, 1.] times higher odds of a child to be stunted in 2015/16 (Table 5).
Discussion
The study aimed to compare the SES indices in predicting stunting using Bayesian multilevel generalized mixed methods for TDHS 2004/5, 2010 and 2015/16. We formulated SES indices using PCA methods. These indices include the wealth assets index, the WAMI, WEO and MPI of which the latter is more complex as compared to others.
The study revealed that MPI had a better predictive capacity of stunting as compared to HWI, WEO and WAMI for the TDHS 2004/5 and 2015/16. For the case of TDHS 2010, the study revealed that WAMI had the best predictive capacity as compared to HWI, WEO and MPI. These findings that WAMI had the best predictive power are similar to a multicounty study conducted in Africa [13]. The fact that each score increases in WAMI results to lower odds of stunting is supported with ability of educated mothers to have better health-seeking behaviour, feeding practices and decision-making power [54, 81, 82]. The role of safe water and sanitation facilities in reducing contamination and eruption of diseases through repeated episodes of diarrhoea which further hinders child food intake and absorption [83] should be acknowledged. Furthermore, living in households with safe water and sanitation and educated mothers may imply higher purchasing power and hence access to nutritious foods which are the backbone for child growth.
It should be considered that WAMI and MPI are the same although works in a different direction and that MPI is more compact as it has additional variables like the mother’s nutrition status and having under-five death in a household. The findings that each score increase in MPI increases the odds of stunting are underlined with other studies which revealed that poor water and toilet facilities increase stunting [81, 84], poor maternal nutrition as measured by BMI [53, 85] and children born to uneducated mothers [30, 53, 81, 86,87,88,89] are prone to stunting. Furthermore, higher values of MPI imply the presence of poor water and toilet facilities which in turn are associated with communicable diseases like diarrhoea [83] as explained above.
Our findings are underlined by the fact that the observed statistical significance in variances of stunting might be attributed to the cultural aspect of educational achievement among mothers [13]. Working mothers were observed to have higher odds of stunting as compared to non-working mothers in previous studies [90] but contrary to [58, 91]. This might be attributed to the fact that the majority of working mothers do not spend much time with their children, as child rearing depends much on house girls and other relatives. It happens that a mother leaves the house at 05:00 AM and comes back home at 06:00 PM for those living in cities like Dar es Salaam and Mwanza. Unfortunately, house girls are normally young to the extent that they do not understand child feeding and caring practices. The assurance that a child is fed what the mother instructed remains doubtful. The observed differences in results compared to that of Ethiopia [91] might be due to cultural differences and food availability. For instance, compared to Tanzania, Ethiopia is largely a desert country with longer seasons of drought thus the majority of unemployed mothers are more likely to be undernourished together with their children due to lack of purchasing power and natural availability of food.
The departure of the constructed SES indices in predicting stunting underlies our hypothesis that these indices do not explain the same on health outcomes [13, 92, 93]. We have observed that the indicators forming a particular indices vary over time. The WEO has a combination of wealth assets, education and occupation. For instance, WAMI has a combination of wealth assets, water and sanitation services as well as maternal education while MPI is the more complex index. The complexity of MPI is defined by its nature of measuring the acute poverty [94].
This study did not bother about using maternal education as an indicator of SES alone as previous studies justified that multivariate indices are better than simple indices [12, 13, 15, 92]. The use of RF provided a more simplified index by selecting assets which are strongly associated with stunting was in agreement with other studies [13, 93, 95, 96]. The study by Krieger et al. [93] reported that rather than using education and occupation, income indicators were strongly associated with mortality, while the study by Psaki et al. [13] gave an assurance of using a multivariate WAMI index in predicting stunting after using RF methods for variable selection.
The study adopted the construction of the WAMI index from previous studies [13]. However, the index does not include household income as DHS does not collect this information. In case the income variable is not available, the use of maternal education, wealth assets as well as water and sanitation provided significant improvement in predicting stunting rather than using wealth assets or education independently [13].
Based on the methodological approach, the BE-MGLMM was revealed to be efficient when predicting the association between SES and stunting. This is due to the fact that compared to the MLE-MGLMM, the BE-MGLMM was capable of producing results for random effects. Furthermore, the compactness of 95% CCI was revealed to provide stronger estimates as compared to the MLE-MGLMM. These findings are underlined with the fact that the BE-MGLMM may provide unbiased estimates [48] evenly where the sample size is very small at hierarchical levels [46, 47].
Conclusion
Stunting is still a major problem in Tanzania, varying significantly across regions and enumeration areas. The fact that individual child, maternal and household characteristics influencing child stunting are known still alarms us on the possibility of designing interventions which may reach each individual. This study revealed that contextual factors affects stunting among under-five-year children. The presence of contextual factors, attributable to social and cultural norms with respect to stunting, puts an emphasis on the need of designing well-targeted interventions being more specific to a particular region and enumeration areas as well. Compared to the WAMI index, which was the best predictor of stunting in the TDHS 2010, the MPI would be preferable when modelling stunting as it was the best predictor in 2004/5 and 2015/16. Initiatives should be embarked to make sure that safe water, sanitation facilities, maternal education and housing facilities are available to the socioeconomic disadvantaged population.
Furthermore, proper household wealth assets including dwellings should be of critical value to enhance a better living environment for under-fives. The pinpointed interventions need proper implementation which are bearable by the policy makers. Policies on budget re-allocation from the economic advantaged to the disadvantages population at lower levels like EAs are inevitable. The results of this study are in agreement with the parent–offspring conflict theory, the life history theory and the ecological model. This study emphasizes on other researchers to use these theories. Last but not least, the study emphasize the use of BE-MGLMM in modelling stunting controlling for contextual factors as compared to MLE-MGLMM. This is based on the fact that BE-MGLMM was able to produce random effects even at enumeration areas, believed to be unbiased estimates needed for programme and policy decisions.
The current study has several strengths, first having the capability of providing trustable estimates on the relationship between SES indices and stunting. This is because of having enough sample size and larger datasets obtained from TDHS which is generalizable to the whole country of Tanzania as compared to the results presented by Psaki et al. [13] which was the district level based study. Secondly, the study informs the reader that SES is truly a multidimensional aspect, and its effect on stunting varies over time. Instead of using HWI as the common measure of SES over time, corresponding SES index associated with the stunting should be established as SES indicators vary over time. However, based on these findings the MPI is recommended when assessing the determinants of stunting. Lastly, but not least, the study took into account the correlation between observations and quantified the presence of contextual factors associated with stunting through the use of both the MLE-MGLMM and BE-MGLMM. However, the BE-MGLMM was found more powerful to MLE-GLMM.
The findings of this study should be interpreted with caution as it is limited to some issues. Firstly, the findings should not be directly compared across surveys as some surveys did not have important variables needed for constructing the indices. For instance, the TDHS 2004/5 did not have information on land ownership, owning agricultural land and having a watch as well as a land telephone. In these aspects, the analysis was conducted on yearly bases. Secondly, these findings do not infer the causal relationship between SES indices and stunting. The DHS is normally cross-sectional in nature, thus we could not establish the causal relationship [97] between stunting and a set of independent variables under consideration. Lastly, but not least most of research questions like size of the child at birth, having fever and diarrhoea status are self-reported which increases the chance of obtaining biased estimates [98]. Furthermore, self-reported answers are prone to misclassification bias [99] however, have been trusted for different researches. Further studies should enlighten on three basic issues and these are (i) multilevel modelling of child wasting and underweight, as despite the observed lower prevalence at national levels, might be concealed within EAs and regional variability (ii) explore the spatial determinants of wasting and underweight, preferably using the Bayesian Spatial models which have been reported to identify the prevalent hotspots of a particular health outcome under consideration, and (iii) explore the spatial determinants of stunting and CIAF preferably using the Bayesian spatial modelling techniques, which are useful for identifying prevalent hotspots.
Availability of data and materials
The dataset is freely available from the DHS website at http://www.dhsprogram.com/data/dataset_admin/login_main.cfm.
Abbreviations
- AIC:
-
Akaike information criterion
- ANC:
-
Antenatal care
- BPOR:
-
Bayesian posterior odds ratio
- BE-MGLMM:
-
Bayesian estimation multilevel generalized linear mixed models
- DHS:
-
Demographics and health surveys
- DIC:
-
Deviance information criterion
- HAZ:
-
Height for age Z-scores
- HWI:
-
Household wealth index
- MPI:
-
Multidimensional poverty index
- PCA:
-
Principal component analysis
- MGLMM:
-
Multilevel generalized linear mixed models
- MLE:
-
Maximum likelihood estimation
- MLE-MGLMM:
-
Maximum likelihood multilevel generalized linear mixed models
- OR:
-
Odds ratio
- PSUs:
-
Primary sampling units
- RF:
-
Random forest
- SES:
-
Socio-economic status
- TDHS:
-
Tanzania demographics and health surveys
- WASH:
-
Water, sanitation, and hygiene
- WAMI:
-
Water and sanitation, assets, maternal education and income
- WEO:
-
Wealth assets, education, and occupation
References
Hoddinott J, Alderman H, Behrman JR, Haddad L, Horton S. The economic rationale for investing in stunting reduction. Matern Child Nutr. 2013;9(S2):69–82.
Lutter CK, Daelmans BMEG, de Onis M, Kothari MT, Ruel MT, Arimond M, et al. Undernutrition, poor feeding practices, and low coverage of key nutrition interventions. Pediatrics. 2011;128(6):e1418–27. https://doi.org/10.1542/peds.2011-1392.
Deborah A, Kavita S, Elisabeth S, Lesley O, Tara K, Joyceline K, et al. Reducing malnutrition in Tanzania: estimates to support nutrition advocacy: Tanzania PROFILES 2014. Reducing malnutrition in Tanzania: estimates to support nutrition advocacy Tanzania PROFILES 2014. 2014. Available from: https://www.fantaproject.org/sites/default/files/resources/Tanzania-PROFILES-Report-2014-June2017.pdf.
De Onis M, Blössner M. WHO Global Database on Child Growth and Malnutrition. Programme of Nutrition World Health Organization Geneva. 1997.
Olofin I, McDonald CM, Ezzati M, Flaxman S, Black RE, Fawzi WW, et al. Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: a pooled analysis of ten prospective studies. PLoS One. 2013;8(5).
Huicho L, Segura ER, Huayanay-Espinoza CA, de Guzman JN, Restrepo-Méndez MC, Tam Y, et al. Child health and nutrition in Peru within an antipoverty political agenda: a Countdown to 2015 country case study. Lancet Glob Heal. 2016;4(6):e414-26.
UNICEF, WHO, WBG. Levels and trends in child malnutrition UNICEF / WHO / World Bank Group Joint Child Malnutrition Estimates Key findings of the 2021 edition. World Heal Organ [Internet]. 2021;1–32. Available from: https://www.who.int/publications/i/item/9789240025257.
Crochemore I, Silva M, França G V, Barros AJD, Amouzou A, Krasevec J, et al. Declining Stunting Prevalence in Low- and Middle-Income Countries. Community Int Nutr. 2018.
MoHCDGEC. Tanzania National Nutrition Survey 2018. Dodoma; 2019. Available from: https://www.unicef.org/tanzania/media/2141/file/TanzaniaNationalNutritionSurvey2018.pdf.
Howe LD, Galobardes B, Matijasevich A, Gordon D, Johnston D, Onwujekwe O, et al. Measuring socio-economic position for epidemiological studies in low-and middle-income countries: a methods of measurement in epidemiology paper. Int J Epidemiol. 2012;41(3):871–86.
Darin-Mattsson A, Fors S, Kåreholt I. Different indicators of socioeconomic status and their relative importance as determinants of health in old age. Int J Equity Health. 2017;16(1):1–11.
Omer W, Al-Hadithi T. Developing a socioeconomic index for health research in Iraq. East Mediterr Heal J. 2017;23(10):670–7.
Psaki SR, Seidman JC, Miller M, Gottlieb M, Bhutta ZA, Ahmed T, et al. Measuring socioeconomic status in multicountry studies: results from the eight-country MAL-ED study. Popul Health Metr. 2014;12(1):1–11.
Frost MB, Forste R, Haas DW. Maternal education and child nutritional status in Bolivia: finding the links. Soc Sci Med. 2005;60(2):395–407.
D’Errico A, Ricceri F, Stringhini S, Carmeli C, Kivimaki M, Bartley M, et al. Socioeconomic indicators in epidemiologic research: A practical example from the LIFEPATH study. Vol. 12, PLoS ONE. 2017. 1–32 p.
Wagstaff A, Watanabe N. Socioeconomic Inequalities in Child Malnutrition in the Developing World. The Development Dilemma. 2000.
Baye K, Laillou A, Chitweke S. Socio-economic inequalities in child stunting reduction in sub-Saharan Africa. Nutrients. 2020;12(1):1–11.
Rabbani A, Khan A, Yusuf S, Adams A. Trends and determinants of inequities in childhood stunting in Bangladesh from 1996/7 to 2014. Int J Equity Health. 2016. https://doi.org/10.1186/s12939-016-0477-7.
Fenta HM, Zewotir T, Muluneh EK. Spatial data analysis of malnutrition among children under-five years in Ethiopia. BMC Med Res Methodol. 2021;21(1):1–13.
Nandy S, Irving M, Gordon D, Subramanian SV, Davey SG. Poverty, child undernutrition and morbidity: new evidence from india. Bull World Health Organ. 2017;011650(04):309–15.
Kazembe LN. An additive regression model for investigating the relationship between childhood health and socio-economic status. Spat Spatiotemporal Epidemiol. 2013;6:71–84. https://doi.org/10.1016/j.sste.2013.07.002.
Emina JB, Kandala N, Inungu J, Ye Y. Maternal education and child nutritional status in the democratic republic of Congo. J Public Health Epidemiol. 2011;3(12):576–92.
Seboka BT, Hailegebreal S, Mamo TT, Yehualashet DE, Gilano G, Kabthymer RH, et al. Spatial trends and projections of chronic malnutrition among children under 5 years of age in Ethiopia from 2011 to 2019: a geographically weighted regression analysis. J Heal Popul Nutr. 2022;41(1):1–17. https://doi.org/10.1186/s41043-022-00309-7.
Adeyemi RA, Zewotir T, Ramroop S. Joint spatial mapping of childhood anemia and malnutrition in sub-Saharan Africa: a cross-sectional study of small-scale geographical disparities. African Health Sci. 2019;19(3):2692–712.
Kazembe LN. Mapping socio-economic inequalities in health status among Malawian children: a mixed model approach. In: Manda SOM, Kandala N-B, Ghilagaber G, editors. Advanced techniques for modelling maternal and child health in Africa. 2014. https://doi.org/10.1007/978-94-007-6778-2_5
Habyarimana F, Zewotir T, Ramroop S, Ayele DG. Spatial distribution of determinants of malnutrition of children under five years in Rwanda: simultaneous measurement of three anthropometric indices. J Hum Ecol. 2016;54(3):138–49.
Musheiguza E, Mahande MJ, Malamala E, Msuya SE, Charles F, Philemon R, et al. Inequalities in stunting among under-five children in Tanzania: decomposing the concentration indexes using demographic health surveys from 2004/5 to 2015/6. Int J Equity Health. 2021;20(1):1–10.
Mgongo M, Chotta NAS, Hashim TH, Uriyo JG, Damian DJ, Stray-pedersen B, et al. Underweight , Stunting and Wasting among Children in Kilimanjaro Region, Tanzania ; a population-based cross-sectional study. 2017;1–12.
Mohammed S, Asfaw ZG. Bayesian Gaussian regression analysis of malnutrition for children under five years of age in Ethiopia, EMDHS 2014. Arch Public Heal. 2018;76(1):1–11.
Takele K, Zewotir T, Ndanguza D. Spatial joint modelling of children under-five malnutrition in Ethiopia. J Hum Ecol. 2020;70(1–3):132–42.
Lindtjørn B. Spatial variation of child stunting and maternal malnutrition after controlling for known risk factors in a drought-prone rural community in. Glob Heal. 2021;87(1):1–14.
Jahanpour OF, Okango EL, Todd J, Mwambi H, Mahande MJ. Role of clusters in exclusive breastfeeding practices in Tanzania: a secondary analysis study using demographic and health survey data (2015/2016). Front Pediatr. 2022. https://doi.org/10.3389/fped.2022.939706/full.
Sunguya BF, Zhu S, Mpembeni R, Huang J. Trends in prevalence and determinants of stunting in Tanzania: an analysis of Tanzania demographic health surveys (1991–2016). Nutr J. 2019;18(1):1–13.
Novignon J, Nonvignon J. Socioeconomic status and the prevalence of fever in children under age five: Evidence from four sub-Saharan African countries. BMC Res Notes. 2012;5.
Moshi CC, Sebastian PJ, Mushumbusi DG, Azizi KA, Meghji WP, Kitunda ME, et al. Determinants of underweight among children aged 0–23 months in Tanzania. Food Sci Nutr. 2022;10(4):1167–74.
Chirande L, Charwe D, Mbwana H, Victor R, Kimboka S, Issaka AI, et al. Determinants of stunting and severe stunting among under-fives in Tanzania: evidence from the 2010 cross-sectional household survey. BMC Pediatr. 2015;15(1):1–13. https://doi.org/10.1186/s12887-015-0482-9.
Modern G, Sauli E, Mpolya E. Correlates of diarrhea and stunting among under-five children in Ruvuma, Tanzania; a hospital-based cross-sectional study. Sci African. 2020;8:e00430. https://doi.org/10.1016/j.sciaf.2020.e00430.
Nattey C, Masanja H, Klipstein-Grobusch K. Relationship between household socio-economic status and under-five mortality in Rufiji DSS. Tanzania Glob Health Action. 2017;2013(6):19278.
Khamis AG, Mwanri AW, Ntwenya JE, Kreppel K. The influence of dietary diversity on the nutritional status of children between 6 and 23 months of age in Tanzania. BMC Pediatr. 2019;19(1):1–9.
Altare C, Delbiso TD, Mutwiri GM, Kopplow R, Guha-sapir D. Factors associated with stunting among pre-school children in southern highlands of Tanzania. 2016; 390–408.
Khamis AG, Mwanri AW, Kreppel K, Kwesigabo G. The burden and correlates of childhood undernutrition in Tanzania according to composite index of anthropometric failure. BMC Nutr. 2020;6(39):1–13.
Makori N, Kassim N, Kinabo J, Matemu A. Factors associated with stunting in Dodoma Region, Tanzania. African J Food Agric Nutr Dev. 2018;18(3):13842–61.
Chirande L, Charwe D, Mbwana H, Victor R, Kimboka S, Issaka AI, et al. Determinants of stunting and severe stunting among under-fives in Tanzania: evidence from the 2010 cross-sectional household survey. BMC Pediatr. 2015;15(1):1–13. https://doi.org/10.1186/s12887-015-0482-9.
Vittinghoff E, Shiboski SC, McCulloch CE, Glidden DV. Regression methods in biostatistics: linear, logistics, survival, and reapeated measures models. Second Edi. Gail M, Krickeberg K, Samet JM, Tsiatis A, Wong W, editors. vol. 23, Int J Neural Syst. 2013.
Austin PC, Merlo J. Intermediate and advanced topics in multilevel logistic regression analysis. Stat Med. 2017;36(20):3257–77.
Zitzmann S, Lüdtke O, Robitzsch A, Hecht M. On the performance of bayesian approaches in small samples: a comment on Smid, McNeish, Miocevic, van de Schoot (2020). Struct Equ Model A Multidiscip J. 2021;28(1):40–50. https://doi.org/10.1080/10705511.2020.1752216.
Baldwin SA, Fellingham GW. Bayesian methods for the analysis of small sample multilevel data with a complex variance structure. Psychol Methods. 2013;18(2):151–64.
Maas CJM, Hox JJ. Sufficient sample sizes for multilevel modeling. Methodology. 2005;1(3):86–92.
Rutstein SO, Rojas G. Guide to DHS statistics [Internet]. Calverton, MD: ORC Macro. 2006. Available from: http://www.measuredhs.com/pubs/pdf/DHSG1/Guide_to_DHS_Statistics_29Oct2012_DHSG1.pdf%5Cn, http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.431.8235&rep=rep1&type=pdf
MoHCDGEC. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016 [Internet]. Government Statistician ICF. 2016. Available from: https://dhsprogram.com/pubs/pdf/FR321/FR321.pdf.
Onis M De, Onyango A, M DO. WHO child growth standards. Paediatr Croat Suppl. 2008;52(SUPP.1):13–7. Available from: http://hpps.kbsplit.hr/hpps-2008/pdf/dok03.pdf%5Cn, http://cdrwww.who.int/entity/childgrowth/publications/ca_symposium_comparison/en/.
Asmare AA, Agmas YA. Determinants of coexistence of stunting, wasting, and underweight among children under five years in the Gambia; evidence from 2019/20 Gambian demographic health survey: application of multivariate binary logistic regression model. BMC Public Health. 2022;22(1):1–13. https://doi.org/10.1186/s12889-022-14000-3.
Haile D, Azage M, Mola T, Rainey R. Exploring spatial variations and factors associated with childhood stunting in Ethiopia: spatial and multilevel analysis. BMC Pediatr. 2016;16(1):1–14. https://doi.org/10.1186/s12887-016-0587-9.
Taleke BA, Gezle LD, Alamneh TS. Pooled prevalence of stunting and associated factors among children aged 6–59 months in Sub-Saharan Africa countries: a Bayesian multilevel approach. PLoS One. 2022;17(10):1–19. https://doi.org/10.1371/journal.pone.0275889.
Sarma H, Khan JR, Asaduzzaman M, Uddin F, Tarannum S, Hasan MM, et al. Factors influencing the prevalence of stunting among children aged below five years in Bangladesh. Food Nutr Bull. 2017;38(3):291–301.
UNESCO. International standard classification of education (ISCED) 2011. Vol. 5, Prospects. Succursale Centre-Ville, Canada: UNESCO; 1975.
ILO. International Standard Classification of Occupations: ISCO-08 [Internet]. Vol. I, Department of Statistics International Labour Office. Geneva; 2008. http://www.ilo.org/public/english/bureau/stat/isco/index.htm.
Glenn J, Laput J, Go2 GL. Disentangling the Effects of Maternal Employment on Child Stunting in the Philippines1 Disentangling the Effects of Maternal Employment on Child Stunting in the Philippines. Philipp J Dev. 2022;46(1).
Montgomery MR, Gragnolati M, Burke KA, Paredes E. Measuring living standards with proxy variables. Demography. 2000;37(2):155–74.
WHO/UNICEF. Progress on Sanitation and DrWorld Health Organization Unicef Joint Monitoring Programme for Water Supply and Sanitationinking Water: Update 2010. WHO Library. Geneva; 2010.
WHO\UNICEF. Progress on household drinking water, sanitation and hygiene 2000–2020: five years into the SDGs. Joint Water Supply, & Sanitation Monitoring Programme. Geneva; 2021. Available from: http://apps.who.int/bookorders.
Vyas S, Kumaranayake L. Constructing socio-economic status indices: How to use principal components analysis. Health Policy Plan. 2006;21(6):459–68.
Filmer D, Pritchett LH. Estimating wealth effects without expenditure data-or tears: an application to educational enrollments in states of India. Demography. 2001;38(1):115–32.
Krefis AC, Schwarz NG, Nkrumah B, Acquah S, Loag W, Sarpong N, et al. Principal component analysis of socioeconomic factors and their association with malaria in children from the Ashanti region. Ghana Malar J. 2010;9(1):1–7.
Wolfinger R, O’Connell M. Generalized linear mixed models: a pseudo-likelihood approach. J Stat Comput Simul. 1993;48(3–4):233–43.
Bolker BM, Brooks ME, Clark CJ, Geange SW, Poulsen JR, Stevens MHH, et al. Generalized linear mixed models: a practical guide for ecology and evolution. Trends Ecol Evol. 2009;24(3):127–35.
Myung IJ. Tutorial on maximum likelihood estimation. J Math Psychol. 2003;47(1):90–100.
Boedeker P. Hierarchical linear modeling with maximum likelihood, restricted maximum likelihood, and fully Bayesian estimation. Pract Assessment Res Eval. 2017;22(2):1–10.
Corbeil RR, Searle SR. Restricted maximum likelihood (REML) estimation of variance components in the mixed model. Taylor Fr. 2016;18(1):31–8.
Peugh JL. A practical guide to multilevel modeling. J Sch Psychol. 2010;48(1):85–112. https://doi.org/10.1016/j.jsp.2009.09.002.
Held L, Bové DS. Applied statistical inference: likelihood and bayes. Berlin Heidelberg: Springer-Verlag; 2014.
Berger JO. J.O. Berger-1985-Statistical Decision Theory and Bayesian.pdf. Second. New York: Springer-Verlag; 1985.
Box GEP, Tiao GC. Bayesian Inference in Statistical Analysis. Bayesian Inference in Statistical Analysis. 1992.
Zitzmann S, Helm C, Hecht M. Prior specification for more stable bayesian estimation of multilevel latent variable models in small samples: a comparative investigation of two different approaches. Front Psychol. 2021;11(January):1–11.
Holtmann J, Koch T, Lochner K, Eid M. A comparison of ML, WLSMV, and Bayesian methods for multilevel structural equation models in small samples: a simulation study. Multivariate Behav Res. 2016;51(5):661–80.
Zondervan-Zwijnenburg M, Peeters M, Depaoli S, Van de Schoot R. Where do priors come from? applying guidelines to construct informative priors in small sample research. Res Hum Dev. 2017;14(4):305–20. https://doi.org/10.1080/15427609.2017.1370966.
Zellner A, Siow A. Posterior odds ratios for selected regression hypotheses. Trab Estad Y Investig Oper. 1980;31(1):585–603.
Hicks T, Rodríguez-Campos L, Choi JH. Bayesian posterior odds ratios: statistical tools for collaborative evaluations. Am J Eval. 2018;39(2):278–89.
Gelman A. Struggles with survey weighting and regression modeling. Stat Sci. 2007;22(2):153–64.
Gelman A, Carlin JB, Stern HS, Rubin DB. Bayesian data analysis: texts in statistical science. Second. Evolution. CRC Press; 1998. p 346.
Akombi BJ. Stunting, wasting and underweight in Sub-Saharan Africa: a systematic review. Int J Environ Res. 2017;14(8):1–18.
Demilew YM. Factors associated with mothers’ knowledge on infant and young child feeding recommendation in slum areas of Bahir Dar City, Ethiopia: cross sectional study. BMC Res Notes. 2017;10(1):1–7.
Joseph G, Haque SS, Moqueet N, Hoo YR. Children Need Clean Water to Grow: E. Coli Contamination of Drinking Water and Childhood Nutrition in Bangladesh. Children Need Clean Water to Grow: E. Coli Contamination of Drinking Water and Childhood Nutrition in Bangladesh. World Bank Group; 2019.
Ikeda N, Irie Y, Shibuya K. Determinants of reduced child stunting in Cambodia: analysis of pooled data from three demographic and health surveys. Bull World Health Organ. 2013;91(5):341–9.
Wamani H, Tylleskär T, Åstrøm AN, Tumwine JK, Peterson S. Mothers’ education but not fathers’ education, household assets or land ownership is the best predictor of child health inequalities in rural Uganda. Int J Equity Health. 2004;3(1):1–8.
Kavosi E, Rostami ZH, Kavosi Z, Nasihatkon A, Moghadami M, Heidari M. Prevalence and determinants of under-nutrition among children under six: a cross-sectional survey in Fars province. Iran Int J Heal Policy Manag. 2014;3(2):71–6.
Abeway S, Gebremichael B, Murugan R, Assefa M, Adinew YM. Stunting and its determinants among children aged 6—59 Months in Northern Ethiopia: a cross-sectional study. J Nutr Metab. 2018;2018.
Budhathoki SS, Bhandari A, Gurung R, Gurung A, Kc A. Stunting among under 5-year—olds in Nepal: trends and risk factors. Matern Child Health J. 2019. https://doi.org/10.1007/s10995-019-02817-1.
Mzumara B, Bwembya P, Halwiindi H, Mugode R, Banda J. Factors associated with stunting among children below five years of age in Zambia: evidence from the 2014 Zambia demographic and health survey. BMC Nutr. 2018;4(1):1–8.
Win H, Shafique S, Mizan S, Wallenborn J, Probst-Hensch N, Fink G. Association between mother’s work status and child stunting in urban slums: a cross-sectional assessment of 346 child-mother dyads in Dhaka, Bangladesh. Arch Public Heal. 2022;80(1):1–16. https://doi.org/10.1186/s13690-022-00948-6.
Amaha ND, Woldeamanuel BT. Maternal factors associated with moderate and severe stunting in Ethiopian children: analysis of some environmental factors based on 2016 demographic health survey. Nutr J. 2021;20(1):1–9.
Braveman PA, Cubbin C, Egerter S, Chideya S, Marchi KS, Metzler M, et al. Socioeconomic status in health research: one size does not fit all. JAMA. 2005;294(22):2879.
Krieger N, Williams DR, Moss NE. Measuring social class in us public health research: concepts, methodologies, and guidelines. Annu Rev Public Health. 1997;18(16):341–78.
Wang Y, Wang B. Multidimensional poverty measure and analysis: a case study from Hechi City, China. Springerplus. 2016;5(1).
Næss Ø, Claussen B, Thelle DS, Smith GD. Four indicators of socioeconomic position: relative ranking across causes of death. Scand J Public Health. 2005;33(3):215–21.
Martikainen P, Blomgren J, Valkonen T. Change in the total and independent effects of education and occupational social class on mortality: Analyses of all Finnish men and women in the period 1971–2000. J Epidemiol Commun Health. 2007;61(6):499–505.
Savitz DA, Wellenius GA. Can cross-sectional studies contribute to causal inference? It depends. Am J Epidemiol. 2022;00(00):1–3.
Rosenman R, Tennekoon V. Measuring bias in self-reported data. Int J Behav Healthc Res. 2011;2(4):320.
Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. J Multidiscip Healthc [Internet]. 2016 May;9:211. Available from: https://www.dovepress.com/information-bias-in-health-research-definition-pitfalls-and-adjustment-peer-reviewed-article-JMDH.
Acknowledgements
We acknowledge the DHS efforts for making sure that these larger datasets are freely available for researchers and academicians.
Funding
No funding.
Author information
Authors and Affiliations
Contributions
EM designed the study, downloaded the dataset from the DHS measure website, and hence conducted the statistical analysis as well as manuscript writing. TM and JM guided from the study design to analysis and manuscript write-up.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
The DHS requires whoever uses the dataset should publish. In this manner, the consent for publication was granted upon requesting the dataset from the website.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Musheiguza, E., Mbegalo, T. & Mbukwa, J.N. Bayesian multilevel modelling of the association between socio-economic status and stunting among under-five-year children in Tanzania. J Health Popul Nutr 42, 135 (2023). https://doi.org/10.1186/s41043-023-00474-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-023-00474-3