
Abstract
Background
Sub-Saharan African populations undergo a nutrition transition towards diets associated with increased risk for metabolic and cardiovascular diseases. For targeted prevention, we aimed to characterize dietary patterns and determine their sociodemographic factors of adherence.
Methods
We recruited 1,018 adults aged > = 25 years from two formal and three informal settlements within the Health and Demographic Surveillance System, Ouagadougou, Burkina Faso, between February and April 2021. In a cross-sectional sample, a culture-specific food-propensity questionnaire with 134 food items and a sociodemographic questionnaire were used to collect the data. Exploratory dietary patterns were derived using principal component analysis, and sociodemographic factors of adherence were calculated using multivariable linear regression models.
Results
In this study population (median age: 42 years, interquartile range 21 years; male: 35.7%), the diet relied on starchy foods and other plant-based staples with rare consumption of animal-based products. We identified three dietary patterns, explaining 10.2%, 9.8%, and 8.9% of variation in food intake, respectively: a meat and egg-based pattern associated with younger age, male sex, better education, and economic situation; a fish-based pattern prevailed among women, higher educational levels, and better economic situation; and a starchy food-based was associated with younger age and sharing a home with other adults.
Conclusions
This study population is at an early stage of the nutrition transition and shows low intakes of health-beneficial food groups. Yet, progress along the nutrition transition varies according to age, educational attainment, and economic status. Particularly, younger and well-off people seem to adhere more strongly to diets high in animal-based products. These findings can inform strategies in public health nutrition for sub-Saharan African populations.
Similar content being viewed by others

Background
Unhealthy diets constitute an important risk factor for morbidity and mortality worldwide. The Global Burden of Disease Study estimates that in 2019, 7.94 million deaths globally were attributable to poor diet, defined as too much intake of unhealthy foods (e.g., salt, red meat, sugar-sweetened beverages) or too little intake of healthy foods (e.g., fruits, vegetables, whole grain products). The majority of these deaths were of cardiovascular nature, such as ischaemic heart disease or stroke. [1]
This risk factor has become more pertinent for sub-Saharan African (SSA) countries in recent decades, as this region is undergoing major shifts in dietary behaviour and faces subsequent health risks. It is widely accepted that many countries in sub-Saharan Africa experience a so-called nutrition transition, characterized by a “modernization” of the diet (e.g. higher intake of refined carbohydrates, processed foods, red meat), while traditional diets (e.g. high intake of grains, vegetables) are less commonly consumed [2]. This change in dietary behaviour leads to an increased risk of obesity and noncommunicable diseases, while the burden of infectious diseases only declines slowly, resulting in a “double burden of disease” [3, 4]. Urbanization forms a major driver of rapid changes in lifestyle, including dietary habits [5]. A commonly used framework to describe stages of the nutrition transition for population groups and corresponding demographic, economic, and health characteristics has been proposed by Popkin [2]. According to this framework, low- and middle-income countries are positioned at various stages of the change from diets of low variety with a high consumption of fibre, starchy foods, but a low consumption of fat and meat (stage 3) towards a diet high in fat, sugar, and processed foods (stage 4), before moving towards a more health-conscious pattern of reduced fat and sugar, but more fruits and vegetables (stage 5). [2]
In sub-Saharan Africa, inhabitants of urban areas are particularly exposed to drastic changes in lifestyle and diet, resulting from rapid economic growth and rural-to-urban migration [6]. This is particularly true for inhabitants of informal settlements. The United Nations Human Settlement Programme estimates that in 2018, at least 238 million people in sub-Saharan Africa lived in informal settlements [7]. Generally speaking, inhabitants of informal settlements face a multitude of health risks, one of which is poor nutrition and less diverse diets [8]. Ouagadougou has been experiencing a massive increase in population size over the last decades, mainly in the form of unplanned growth in the outskirts of the city [9].
While the concept of changes in nutrition in accordance with economic development is widely accepted, data from low-income countries remain scarce in scientific literature, hence little is known about the current state of this transition, for instance in Burkina Faso [4]. Furthermore, existing studies on dietary habits are limited in sample size [10, 11] or focus on specific population groups, such as mothers and children [12, 13], and thus lack representativeness for other contexts.
Traditionally, epidemiological studies examining the relationship between diet and health outcomes or diet and sociodemographic indicators have focused on individual foods or nutrients. However, this does not reflect the complexity and variability of human nutrition. As a result, dietary pattern analysis has emerged as a tool to capture diet more holistically [14]. Principal component analysis (PCA) is one of the most popular techniques to construct dietary patterns empirically and purely data-driven [15, 16]. This exploratory approach is especially useful to characterize population-specific dietary practices in diverse sociocultural contexts. Additionally, characterizing dietary patterns can inform the design of nutrition interventions, and public health messages about dietary patterns might be easier to comprehend than recommendations about single food items or nutrients.
A considerable volume of literature suggests a causal relationship between higher socioeconomic status and a healthier diet (here defined as a diverse diet high in intake of foods such as whole grains, lean meat, fruits, and vegetables, but low in energy-dense and nutrient-poor foods) [17,18,19]. However, the majority of these studies have been conducted in populations from the global north, not appreciating different social compositions and dietary habits in other contexts. In contrast to high-income countries, in low- and middle-income countries, the opposite effect might be observed, when higher socioeconomic status increases access to, e.g., highly processed, store-bought foods high in saturated fats and sugar, while this access might be limited for people with less resources [20]. Focusing on the link between sociodemographic characteristics and dietary patterns is the basis for informing stakeholders in policy-making and designing target-group specific interventions. Conducting this study in the only urban health and demographic surveillance system in Western Africa ensures representativeness and makes sure that informal settlement dwellers are included.
In summary, there is a lack of representative studies which assess the state of nutrition transition and its links to socioeconomic factors in low-income countries, particularly in SSA. Our study aimed to fill this gap by i) characterizing prevailing dietary patterns and ii) defining the relationships between sociodemographic factors and adherence to different dietary patterns in a representative sample of adults from Ouagadougou, Burkina Faso.
Methods
Study design and setting
Between February and April 2021, we conducted this cross-sectional study in Ouagadougou, the capital of Burkina Faso, which has approximately 2.7 million inhabitants. The city is host to the Ouagadougou Health and Demographic Surveillance System (HDSS), covering a contiguous population of about 82,000 people in official neighbourhoods of the city (‘formal’ settlements), as well as unregulated parts in the periphery (‘informal’ settlements). HDSS participants are visited regularly (on average every 10 months) by fieldworkers in their homes to monitor vital events (such as births or death), as well as in- and out-migration. [21]
This manuscript follows the STROBE-nut guideline to provide more transparent reporting (see Additional file 1 for the corresponding checklist) [22].
Sampling and recruitment
Adults aged ≥ 25 years were eligible for this study. Fieldwork was conducted in accordance with national anti-COVID-19 measures, and personal protective equipment was made available to the fieldworkers.
We based our sample size calculation on the previously observed distribution of energy intake in urban Ghana, measured by the same food-frequency questionnaire [23]. In this previous study, mean energy intake was 2313 kcal/d, and the standard deviation was 668 kcal/d. At 95% confidence interval and an acceptable error of 45 kcal/d, the estimated population size for the present study was 852. Allowing for potential non-participation, we aimed at recruiting 1000 study participants.
To account for unavailable would-be participants and those unwilling to participate, a total of 1945 households with at least one adult aged > = 25 years were drawn from the HDSS population with equal distribution between formal and informal settlements. Of those households, one adult was randomly selected for the interview. Trained field workers visited the homes and enrolled eligible household members. Upon visiting these households, we met 1,087 eligible subjects (formal settlements: 545, informal: 542). Of these, 93.6% were successfully interviewed (formal settlements: 92.8%, informal: 94.5), for a grand total of 1,018 participants (formal settlements: 506, informal: 512).
Figure 1 shows the locations where the participants were recruited within the Ouagadougou HDSS.

Recruitment sites in Ouagadougou and number of participants. Numbers next to each neighbourhood represent the mean IWI score, also reflected in the colour hue.
Dietary assessment
Questionnaires were administered by trained fieldworkers in face-to-face interviews at the homes of the participants. We used tablets and the Survey CTO software (Dobility, Inc., Cambridge, Massachusetts, USA) for data collection and management. Dietary assessments were conducted using the African Food Propensity Questionnaire (AFPQ), a semi-quantitative food-frequency questionnaire that has been adapted from the Ghana-Food Propensity Questionnaire [24]. The AFPQ queries for the intake frequencies of 134 food items in pre-defined portion sizes over the last 12 months. To ensure a common understanding of portion sizes among participants, we showed standardized portion sizes using pictures of common household measures, such as table spoons or cups.
We used the West African Food Composition Database [25] and the German Nutrient Database (BLS 3.01) (2010) to calculate the intakes of energy (kcal per day), as well as macronutrients (energy%) and micronutrients (grams per day).
The original AFPQ and sociodemographic questionnaire were in English. Translation into French was done by a bilingual researcher at the institute, and back-translation was performed to ensure accuracy of the translation.
Assessment of demographic and socioeconomic factors
During the face-to-face interviews, field workers collected demographic and socioeconomic data. Demographic data comprised age (years), sex (male, female), and self-reported ethnic group (10 categories). Socioeconomic data included educational level (none, primary, junior secondary, senior secondary, vocational training, tertiary), employment status (employed, retired, unemployed, unable to work, on social benefits, full-time homemaker, student), occupation (subsistence farmer, commercial farmer, casual worker, merchant/vendor, craftsperson, civil servant, other), marital status (married, cohabitating, single, divorced/separated, widowed), number of people living in the household, and information, whether the respondents were living together with their partner/toddler/child/parents/in-laws/other adults, or if they were living in a retirement home. Please note that we use the term “homemaker” as an answer option in the employment variable for lack of a better term, although the true workload though additional activities outside the home might not be reflected by it.
Further data for the individual households were available from previous HDSS surveys (2019–2020). Those included information on the source of energy available (gas, firewood, coal), access to electricity/water, floor quality, the type of toiled used, and availability of household items (phone, bicycle, car, television, refrigerator).
Missing data handling
In total, 1018 questionnaires were completed successfully. After the initial data quality checks, 5% of the participants with the most extreme values (2.5% with the lowest and 2.5% with the highest values) for energy intake (kcal per day) were revisited to confirm the accuracy of their answers. Of those 50 study subjects, 39 were met at home and had their interviews retaken in the same manner as in the first round. Because food intake data reported during the second visit were much more plausible, these data were used in the present analysis.
In this nutrition survey, we did not perform anthropometric assessments. To approximate energy expenditure, we used literature-based, fixed energy intake cut-offs for men and women as a criterion for data plausibility [26]. For men, we applied plausible ranges of energy intake between 800 kcal and 4,000 kcal; for women, this range was 500 kcal and 3,500 kcal. Figure 2 shows the exclusion of participants based on implausible or missing data. Of the recruited 1018 participants, 5 men and 13 women had implausible values for energy intake. Thus, 1,000 participants were included in principal component analysis and descriptive statistics. Also, there were 27 men and 38 women who had missing data on demographic or socioeconomic variables. Hence, the final analytical sample size was 935 participants, used in the calculation of the International Wealth Index and in the regression models.

Flowchart of participants included in the analysis and reasons for exclusion. PCA = principal component analysis, SES = socioeconomic status.
Data analysis
For the characteristics of the study population and the distribution of food intake, we calculated proportions (%) for categorical data, medians and interquartile ranges for non-normally distributed data, and means and standard deviations (SD) for normally distributed data. As a summary variable for measuring the economic status of the households, we used the International Wealth Index (IWI) according to [27], ranging from 0–100 points. Higher score points reflect better access to infrastructure and possessing more household assets. Base variables for the calculation of the score were: household possession (yes/no) of phone/bicycle/car/television/fridge, and whether the household had access to electricity. Floor quality, water quality, and type of toilet were also considered. To test significance of differences in IWI scores between settlement types, we used an unpaired t test with a significance level of 0.05.
To characterize dietary intake, we grouped 134 food items into 30 food categories based on their nutrient profiles and culinary use (Table 1). Using common household measures and portion sizes, we calculated the intake in grams per day for each food group, using the West African Food Composition Table [25]. We present measures of central tendency (median) and dispersion (interquartile range) in the form of bar charts.
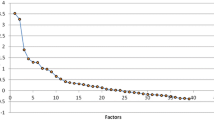
To find combinations of food categories that were often eaten together, we applied principal component analysis (PCA) using the PROC FACTOR procedure in SAS/STAT® 9.4 (SAS Institute Inc., Cary, NC, USA). We retained factors based on the Eigenvalue criterion > 1, the scree plot, and the interpretability of the pattern scores. We applied the varimax rotation to ensure that the extracted factors remain uncorrelated. Factors were labelled and interpreted as dietary patterns based on the food groups with the highest factor loadings (|correlation coefficient|> 0.4). Participants were allocated a score for each factor based on their individual intake and respective factor loading of the food groups. Factor scores were standardized to have a mean of 0 and an SD of 1.
The robustness of factors was tested by applying PCA to random-split samples, and comparing the resulting pattern scores and their factor loadings with each other. We also ran PCA separately for formal and informal settlements to test the stability of pattern scores.
For the description of factors of adherence, we constructed quintiles of the identified pattern scores and calculated the distribution of demographic and socioeconomic variables across these quintiles. We calculated p-values for trend using the Jonckheere–Terpstra test (non-normally distributed continuous variables), linear regression (normally distributed variables), the Cochran–Armitage trend test (binary variables), and the Cochran–Mantel–Haenszel test for categorical variables. Variables that seemed to have a linear trend across the quintiles of the pattern scores were subjected to correlation analysis to identify intercorrelation. For the following regression models, we have removed variables that showed a moderate to strong correlation with other similar variables (Cramér’s V > 0.3) [28], such as occupation and employment, in order to make the regression models more parsimonious and improve interpretability.
For the associations of demographic and socioeconomic factors with the identified dietary pattern scores, we calculated beta coefficients per one-unit increase, their 95% confidence intervals (CIs), p-values, and the explained variance in the outcome variable (R2). We constructed multivariate linear regression models for each dietary pattern with the following set of independent variables: age, sex, education level, employment status, occupation, International Wealth Index, marital status, and living together with a toddler/in-laws/other adults.
Results
Characteristics of the study population
Figure 1 provides an overview of the study area with the number of participants from each neighbourhood. The demographic and socioeconomic characteristics of the total study population and by settlement type are shown in Table 2.
Most of the respondents were female (64.3%). The median age in the sample was 42 (IQR: 21) years; this number was 47 years (IQR: 25 years) in the formal settlements and 39 years (IQR: 15 years) in the informal settlements. The majority of participants identified as Mossi, the biggest ethnic group in Burkina Faso. Most people had not completed any formal education (51% to 64%). Also, the majority of participants were not in a stable employment situation, either being unemployed (29.0%) or being a full-time homemaker (34.3%, formal: 28.1%, informal: 40.5%). The median number of household members was 6 (IQR: 4).
The mean IWI score was 56.9 ± 16.5, being 65.5 ± 14.9 in the formal settlement and 47.5 ± 12.5 in the informal settlements. This indicates a significant difference in IWI scores between the settlement types (p < 0.0001). The mean IWI scores for each neighbourhood are shown in Fig. 1 (colour shading).
Food groups and nutrient intakes
Figures 3 and 4 show the median consumption of 30 food categories in g/d for the total study population and by settlement type. The highest intake was seen for coffee and tea; rice, pasta and corn; maize-based foods; vegetables; and white bread and cereals (Fig. 3). In contrast, alcoholic beverages, margarine, cooking fats, olive oil, processed meat, and sweet spreads were rarely consumed. In general, animal-based products (e.g., egg, poultry, dairy products, red meat, and fish) were rarely consumed. Table 3 shows the energy intake and nutrient consumption for the total study population, by settlement type and by sex. The median energy intake in the whole sample was 1834 kcal/d (IQR: 908), amounting to 1958 kcal/d (IQR: 875) in formal settlements, and to 1731 kcal/d (IQR: 884) in informal settlements. Carbohydrates, total fats, and protein accounted for 62%, 24%, and 13% of energy intake, respectively. Mean fibre intake was 25 ± 17 g/d, and the ratio of saturated versus unsaturated fats was 0.81 ± 0.27.

Median daily consumption of food groups (> 15 g/d) among 1000 adults in Ouagadougou

Median daily consumption of food groups (≤ 15 g/d) among 1000 adults in Ouagadougou
Dietary patterns and their factors of adherence
We retained three dietary pattern scores from PCA that explained 29% of the total variation in food group intake. Table 4 shows the dietary patterns and their rotated factor loadings for 30 food groups.
The first dietary pattern explained 10.2% of the variation in food group intake and was characterized by high intakes of poultry (0.62), meaty mixed dishes (0.61), red meat (0.54), eggs (0.54), potatoes (0.45), and processed meat (0.42). Therefore, we labelled it as “meat and egg-based dietary pattern”.
The second dietary pattern explained 9.8% of the total variation in food group intake and was characterized by frequent consumption of fish (0.71), palm oil (0.70), condiments (0.63), red meat (0.55), meaty mixed dishes (0.50), vegetables (0.47), and nuts and seeds (0.44). Accordingly, we named this the “fish-based dietary pattern”.
Finally, the third dietary pattern explained 8.9% of the total variation in food group intake and had positive correlations with rice, pasta, and corn (0.61), roots and tubers (0.48), maize-based foods (0.47), condiments (0.46), vegetables (0.46), nuts and seeds (0.44), cakes and sweets (0.44), legumes (0.43), fruits (0.43), and potatoes (0.42). It was labelled “starchy food-based dietary pattern”.
The last four rows of Table 5 show total energy (kcal) and macronutrient (% energy) intake across different quintiles of dietary pattern scores, thus showing the trend of these intakes for increasing adherence to the respective dietary pattern. The meat and egg-based dietary pattern showed decreasing carbohydrate intake (quintile 1: 66%, quintile 5: 57%), and increasing protein intake (quintile 1: 12%, quintile 5: 14%) with increasing adherence to the pattern. The fish-based dietary pattern, in contrast, exhibited decreasing carbohydrate intake (quintile 1: 71%, quintile 5: 46%), increasing fat intake (quintile 1: 17%, quintile 5: 37%), and increasing protein intake (quintile 1: 11%, quintile 5: 16%). The starchy food-based pattern showed increasing total energy intake (quintile 1: 1321 kcal, quintile 5: 2544 kcal) with increasing adherence to the pattern.
To determine the variables to be included in the multivariate linear regression models, we assessed the association between factor score quintiles and sociodemographic variables (Table 5). We found no linear association for ethnic group, main source of energy used for cooking, number of refrigerators, number of housemates, living with child, and living in retirement home. The variables ‘living with partner’ and ‘living with parents’ were eliminated because they showed an association with marital status of Cramér’s V > 0.3. The remaining sociodemographic characteristics were included as independent variables in the models: age, sex, education level, employment status, occupation, International Wealth Index, marital status, and living together with a toddler/in-laws/other adults.
Table 6 shows the multivariate associations of demographic and socioeconomic variables with the dietary patterns. For the meat and egg-based dietary pattern, the explained variance was 29%. Positive associations with this dietary pattern were seen for a lower age, being male, having a higher education (reference: no formal education), being a full-time homemaker, a paid employee or being unable to work (reference: being unemployed); having a higher IWI score. Casual workers (reference: merchant); cohabitating people (reference: married); and people living with other adults were less likely to have a high score for this pattern.
For the fish-based dietary pattern, positive associations were discernible with female sex, higher education (reference: no education); not being unemployed (reference: being unemployed); a higher IWI score; cohabitating, being single or widowed (reference: married). Negative associations with this dietary pattern score comprised being a civil servant or a craftsperson (reference: merchant) or living with other adults. These factors explained 40% in the variance of the fish-based dietary pattern score.
Lastly, for the starchy food-based dietary pattern, we observed an explained variance of 15%, and positive associations with younger age, having obtained advanced secondary schooling (reference: no formal education), or living with other adults. Being widowed (reference: married) was negatively associated with this dietary pattern score.
Sensitivity analysis
To test the robustness of the extracted dietary pattern scores, we performed a split-half analysis. The results are shown in Table 7. In both randomly selected halves, we observed the same three patterns with similar correlation coefficients between factors and food groups.
In order to examine the robustness of the derived dietary patterns, we conducted a sensitivity analysis, performing PCA separately by settlement type. The resulting factors with associated food groups are shown in Table 8. The pattern scores in the formal settlements corresponded well to the three patterns from the total sample, also representing a meat- and egg-based pattern, a fish-based pattern, and a pattern with high loadings of starchy foods. In the informal settlements, we also found patterns with similar interpretation: a fish- and meat-based pattern, a pattern with high loadings for starchy staples and other plant-based foods, and a pattern with a combination of animal-based foods. Owing to the similarities of dietary pattern scores between settlement types, it was reasonable to use the PCA results of the total sample for the subsequent association analyses.
Discussion
Key findings
The purpose of this study was to identify common dietary patterns and to describe their sociodemographic factors of adherence in a representative sample from urban sub-Saharan Africa. The most frequently consumed food groups included plant-based staples (rice, pasta, and corn; maize-based foods; vegetables; white bread and cereals); animal-based products (egg, poultry, dairy products, red meat, fish) were rarely consumed. We found three distinct dietary patterns: a meat and egg-based pattern that was strongly correlated with poultry, meaty dishes, red meat, and eggs; a fish-based pattern characterized by fish, palm oil, condiments, and red meat; and a starchy food-based pattern that correlated with rice, pasta, and corn, roots and tubers, maize-based foods, and condiments. Adherence to the meat and egg-based pattern was associated with younger age, male sex, higher education, and an advanced economic situation; the fish-based pattern was associated with female sex, a higher education, and a higher economic status; whereas the starchy food-based pattern was related with younger age, and sharing a house with other adults.
Study population
A noteworthy finding pertaining to the study population is the overrepresentation of women of 64.3% compared to a balanced men to women ratio of 100.6:100 in the total HDSS population [21]. This is a common phenomenon in surveys conducted in the homes of participants. One sensible explanation is that, on average, women might spend more time at home than men [29]. However, the sex ratio in the present study was very similar between the different settlement types, suggesting that this effect had a similar influence, regardless of the neighbourhood.
Dietary habits and the nutrition transition
According to Popkin’s framework of the nutrition transition, shifts in dietary behaviour are associated with economic development, demographic changes and changes in the prevalence of certain diseases or risk factors. In the following section, the results of this study are put into context of the stages in this model, ranging from stage 3 (high consumption of fibre, starchy foods, low consumption of fat and meat) through stage 4 (high in fat, sugar, and processed foods) and up to stage 5 (more health-conscious, consisting of reduced intake of fat and sugar in favour of more fruits and vegetables). [2]
In this study population, absolute intakes of all macronutrients and energy seemed to be much lower in informal settlements as compared to formal settlements. This relative difference between settlement types suggests that the population in informal settlements consumes less food overall. The intake of macronutrients relative to energy intake was similar for the different groups analysed. In the total study population, the median carbohydrate intake of 62 energy% slightly exceed the reference intakes suggested by the European Food Safety Authority of 45–60 energy% [30]. Conversely, total fat intake and protein intake were lower in the present study group than the recommended intakes [30]. In summary, the low intake of protein and fat with high intake of carbohydrates suggests that this population is at an early stage of the nutrition transition (stage 3), holding true not only for the general study population but also for the different settlement types analysed [2].
This interpretation is further corroborated by the predominating foods in our survey. These were starchy staples based on maize and other cereals, and vegetables. At the same time, the consumption of meat, processed meat, added fats, and sweet spreads was rather low.
Finally, the combination of foods consumed, as identified by PCA, and the associated sociodemographic factors of adherence underpin the notion that enhanced economic status leads to modernized dietary practices (referring to higher intake of refined carbohydrates, processed foods, red meat). Certain groups are more inclined to eat a diet richer in animal-based products (the meat- and egg-based dietary pattern) than others. Here, younger people, men, better educated subjects, and those with in a better economic situation have a higher probability of adhering to this diet. Similarly, Table 3 shows that people from formal settlements have higher scores for this dietary pattern. This might suggest that men, better educated people and those in a better economic situation might be the groups that are already on their way to the next stage of the nutrition transition (stage 4 according to Popkin).
Factors of adherence to dietary patterns in sub-Saharan Africa
Compared to other studies from urban sub-Saharan Africa, we found an unusually homogenous meat and egg-based pattern. Nkondjock et al. [31] found a similar pattern made up mostly of bush meat, poultry and red meat in 541 Cameroonian adults. Other studies, however, found meat-heavy dietary patterns that also showed strong association with fish and wheat-based foods [24] or with nuts and legumes [32]. Nkondjock et al.’s meat-based pattern was associated with older age, higher energy intake and BMI, as well as low educational level. This contradicts our finding that the meat- and egg-based pattern was associated with younger age and a high educational level. One reason for this might be that the population studied by Nkondjock et al. (members of the Cameroonian military) overall had a higher socioeconomic status than the population we studied. Whereas in our study population, animal-based products might be hard to access for a large part of the group for economic reasons, this might not have been a limiting factor in Nkondjock et al.’s study. The dietary pattern that included meat and fish in the study by Galbete et al.[24] was associated with living in urban Ghana, as opposed to residing in Europe or rural Ghana, with a higher educational level, male sex, younger age; and more physical activity. This corresponds well to the association we found regarding male sex and younger age being associated with stronger adherence to the meat- and egg-based pattern. Obasohan et al. [32] sought to determine the association of dietary patterns with high blood pressure in Nigerian civil servants but did not identify the meat, nuts, and legume pattern as a significant risk factor.
Mank et al. [33] also found a fish-based dietary pattern in 514 children from rural Burkina Faso. In contrast to the pattern we found, however, it was also strongly associated with maize-based foods, whereas our fish-based pattern had a negative association with maize-based foods.
The starchy food-based pattern in this study corresponds best to the “traditional” patterns found in many studies, most frequently consisting of cereals, grains, roots and tubers, corn, nuts and legumes, fermented foods, and staples, such as tô (the national dish of Burkina Faso consisting of corn, millet or sorghum flour) [10, 13, 24, 34]. One study conducted in 2010 in 330 households in Ouagadougou found one “traditional” dietary pattern through cluster analysis, which was characterized by high intakes of leafy vegetables and local cereals and comprised 71% of the population as opposed to 29% classified in an “urban” dietary pattern (higher intake of fat and sugar). Similar to our findings, the traditional dietary pattern had positive associations with the female sex, lower income, and lower education. [10] Similarly, two studies from Ghana also found associations between “traditional” dietary patterns, lower education, lower income, and rural populations [24, 34]. Comparable combinations of foods to the “traditional” dietary patterns are sometimes also summarized as “health conscious” (in this study characterized by high intakes of foods such as vegetables, fruits, roots and tubers, while being low in snacks and sweetened foods) [35]. Classifying such patterns as health conscious, however, is difficult using this methodology, as important factors to the healthfulness of a diet (e.g., dietary variety) are not considered. This is one of the reasons why we opted to name the dietary patterns we found in a more descriptive manner, mentioning the most highly loading food groups.
Unlike previous literature, we did not identify a “sweets” or “snacking” pattern, characterized by high intakes of sweetened snacks, soft drinks, and similar foods [12, 13, 35, 37]. One reason for this might be the fact that many of the studies identifying this pattern were conducted in children or adolescents and the pattern seems to correlate with younger age [37], whereas our study included only adults starting from the age of 25. In addition, the lack of a snacking pattern in our study supports the conclusion that our study population is still at an early stage of the nutrition transition.
Strengths and limitations of this study
This study stands out through its large sample size of 1,000 participants, drawn from a representative sample within the only urban HDSS in Western Africa, including formal and informal settlements. Using PCA to derive dietary patterns, we did not have to rely on “a-priori” reference values. Furthermore, through this method we were able to take into account the whole diet, not just single nutrients. In contrast to cluster analysis (CA), PCA yields continuous variables as results, suitable for subsequent regression analyses. Unlike CA, PCA does not rely on a reference group, thus not limiting statistical power [38]. Moreover, PCA assigns a score to each participant for every dietary pattern unlike CA which yields uneven, mutually exclusive groups, which might limit interpretability [39]. The detailed, region-specific food-frequency questionnaire allowed to cover a wide range of foods and dishes common in the target population.
Food-frequency questionnaires tend to underestimate energy intake due to the closed list of food items. Therefore, the derivation of absolute nutrient intakes may not be accurate. However, on a population basis and for between-group comparisons, FFQ data can be useful to rank participants according to their nutrient intakes. Energy intake, for example, might be underreported by as much as 20% [40]. Furthermore, the AFPQ has not been validated in a Burkinabe population yet. For this reason, we focused on relative intergroup differences, rather than using absolute intake values. Additionally, food-frequency questionnaires do not take into account the mode of preparation of the foods which might impact nutrient uptake. Further limitations of our study include the subjective decisions involved in principle component analysis, such as deciding the number of components to retain, the rotation method, and setting cut-off values for factor loading scores. This might limit comparability with other studies. While the sample was designed to be representative and sample size was comparatively large, the validity of our results might be impacted by response bias due to some sociodemographic groups being more willing to participate, as demonstrated by the disbalanced sex distribution of the respondents. Also, in retrospective dietary assessment, recall bias can distort the findings, when some groups respond systematically differently than others.
Public health implications
Interventions with the goal of promoting a more healthful diet that can profit from the insights gained in this study range from the individual level to interventions that target the general food environment.
On the individual level, nutrition education interventions have been used successfully to improve nutrition knowledge and physical activity level [41, 42]. Our study suggests that educational interventions in Ouagadougou should focus on promoting moderate intakes of starchy foods, while increasing the intake of protein sources. However, interventions should also highlight the risks associated with high intakes of red meat and promote adoption of alternative protein sources (poultry, pulses and other plant-based protein sources). As the nutrition transition progresses, the population should be encouraged to maintain the current habits of low snacking, and avoiding sweets, alcohol, and red meat. Special attention should be paid to the role of men, younger and more affluent population groups, as those appear to have a stronger inclination for meat- and egg-based dietary patterns. Those groups could be the first to move away from traditional diets and thus, becoming at risk of adopting unhealthy diets.
Interventions that work on the food environment level could improve the availability and desirability of certain foods, developing value chains, accompanied by community work [43]. Alternative sources of protein (other than red meat) should be made available and promoted through marketing campaigns. On the policy level, governments can influence the risk of nutrition-related noncommunicable diseases through interventions such as restricting marketing for unhealthful foods (e.g., sweets and snacks) to prevent those from gaining more popularity in this population), funding research on specific risk factors, and improving monitoring and evaluation of adverse consequences [44]. Taxing highly processed foods can be a means of influencing both obesity, as well as undernutrition [45].
Research Implications
With the aim of understanding determinants of a healthy diet, it is necessary to conduct further research into the interpersonal, environmental and policy levels of influence, as those upstream factors of individual decision making are still poorly understood [46]. With the knowledge of how people eat, the question opens up why they choose to do so and what might be barriers on the interpersonal, environmental, and policy levels that prevent individuals from choosing a more healthful diet. Future research should be dedicated to understanding the health consequences of different dietary patterns. It will be important to understand the relationship between meat-based dietary patterns and cardiovascular diseases or type 2 diabetes. Another important factor that might be target of future research in similar contexts is the role of food processing. Using food processing classification systems, such as the NOVA [47] system to classify the food items present in the dietary patterns found could be helpful in understanding the progress of the nutrition transition.
Our study provides a valid starting point to generate in-depth understanding about the nature of the nutrition transition in Ouagadougou and other urban areas in sub-Saharan Africa. In the future, repeated measurements are desirable to evaluate the changes in dietary behaviour over time [48]. This might allow for new insights into the dynamics of diet and for predictions regarding future trends. Health and demographic surveillance systems, such as the one in Ouagadougou, would be ideal for such studies, offering the infrastructure and representative samples of urban populations.
Conclusions
We conclude that in this population from urban Burkina Faso, distinct dietary patterns are discernible that vary according to economic status, age, and educational attainment. A dietary pattern high in animal-based products is prevalent among young, affluent and well-educated individuals. This contrasts with a diet high in starchy foods and associated with bigger households and lower educational attainment. Interestingly, the differences between sociodemographic groups seem to be minor, with an overall low intake of processed foods or meat, and high intakes of starchy foods. In general, this study population seems to be at an early stage of the nutrition transition (stage 3) and health consequences need to be investigated.
These findings imply that a general reduction of starchy roots and tubers with increased intake of plant-based protein sources should be encouraged. At the same time, important nuances in dietary practices that stem from differences in socioeconomic characteristics highlight the need for target-group-specific interventions in this area.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AFPQ:
-
African Food Propensity Questionnaire
- CA:
-
Cluster Analysis
- CI:
-
Confidence Interval
- HDSS:
-
Health and Demographic Surveillance System
- IWI:
-
International Wealth Index
- PCA:
-
Principal Component Analysis
- SD:
-
Standard Deviation
- SSA:
-
Sub-Saharan Africa
References
Murray CJL, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396:1223–49. https://doi.org/10.1016/S0140-6736(20)30752-2.
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70:3–21. https://doi.org/10.1111/j.1753-4887.2011.00456.x.
Bygbjerg IC. Double burden of noncommunicable and infectious diseases in developing countries. Science. 2012;337:1499–501. https://doi.org/10.1126/science.1223466.
Dalal S, Beunza JJ, Volmink J, Adebamowo C, Bajunirwe F, Njelekela M, et al. Non-communicable diseases in sub-Saharan Africa: what we know now. Int J Epidemiol. 2011;40:885–901. https://doi.org/10.1093/ije/dyr050.
Popkin BM. Urbanization, lifestyle changes and the nutrition transition. World Dev. 1999;27:1905–16. https://doi.org/10.1016/S0305-750X(99)00094-7.
Tsolekile L. (2007) Urbanization and lifestyle changes related to non-communicable diseases: An exploration of experiences of urban residents who have relocated from the rural areas to Khayelitsha, an urban township in Cape Town.
UN-Habitat. (2020) The value of sustainable urbanization. Nairobi, Kenya: UN-Habitat
Zerbo A, Delgado RC, González PA. Vulnerability and everyday health risks of urban informal settlements in Sub-Saharan Africa. Global Health J. 2020;4:46–50. https://doi.org/10.1016/j.glohj.2020.04.003.
Schug F, Okujeni A, Hauer J, Hostert P, Nielsen JØ, van der Linden S. Mapping patterns of urban development in Ouagadougou, Burkina Faso, using machine learning regression modeling with bi-seasonal Landsat time series. Remote Sens Environ. 2018;210:217–28. https://doi.org/10.1016/j.rse.2018.03.022.
Zeba AN, Delisle HF, Renier G. Dietary patterns and physical inactivity, two contributing factors to the double burden of malnutrition among adults in Burkina Faso. West Africa J Nutr Sci. 2014;3: e50. https://doi.org/10.1017/jns.2014.11.
Sodjinou R, Agueh V, Fayomi B, Delisle H. Dietary patterns of urban adults in Benin: relationship with overall diet quality and socio-demographic characteristics. Eur J Clin Nutr. 2009;63:222–8. https://doi.org/10.1038/sj.ejcn.1602906.
Kumordzie SM, Okronipa H, Arimond M, Adu-Afarwuah S, Ocansey ME, Young RR, et al. Maternal and child factors associated with child body fatness in a Ghanaian cohort. Public Health Nutr. 2020;23:309–18. https://doi.org/10.1017/S1368980019001745.
Abizari A-R, Ali Z. Dietary patterns and associated factors of schooling Ghanaian adolescents. J Health Popul Nutr. 2019;38:5. https://doi.org/10.1186/s41043-019-0162-8.
Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol. 2002;13:3.
Newby PK, Tucker KL. Empirically derived eating patterns using factor or cluster analysis: a review. Nutr Rev. 2004;62:177–203. https://doi.org/10.1111/j.1753-4887.2004.tb00040.x.
Schulze MB, Hoffmann K. Methodological approaches to study dietary patterns in relation to risk of coronary heart disease and stroke. Br J Nutr. 2006;95:860–9. https://doi.org/10.1079/bjn20061731.
Darmon N, Drewnowski A. Does social class predict diet quality? Am J Clin Nutr. 2008;87:1107–17. https://doi.org/10.1093/ajcn/87.5.1107.
Mullie P, Clarys P, Hulens M, Vansant G. Dietary patterns and socioeconomic position. Eur J Clin Nutr. 2010;64:231–8. https://doi.org/10.1038/ejcn.2009.145.
Cutler GJ, Flood A, Hannan P, Neumark-Sztainer D. Multiple sociodemographic and socioenvironmental characteristics are correlated with major patterns of dietary intake in adolescents. J Am Diet Assoc. 2011;111:230–40. https://doi.org/10.1016/j.jada.2010.10.052.
Manyanga T, Tremblay MS, Chaput J-P, Katzmarzyk PT, Fogelholm M, Hu G, et al. Socioeconomic status and dietary patterns in children from around the world: different associations by levels of country human development? BMC Public Health. 2017;17:457. https://doi.org/10.1186/s12889-017-4383-8.
Rossier C, Soura A, Baya B, Compaoré G, Dabiré B, Dos Santos S, et al. Profile: the Ouagadougou Health and demographic surveillance system. Int J Epidemiol. 2012;41:658–66. https://doi.org/10.1093/ije/dys090.
Lachat C, Hawwash D, Ocké MC, Berg C, Forsum E, Hörnell A, et al. Strengthening the reporting of observational studies in epidemiology-nutritional epidemiology (STROBE-nut): an extension of the STROBE statement. PLoS Med. 2016;13: e1002036. https://doi.org/10.1371/journal.pmed.1002036.
Galbete C, Nicolaou M, Meeks K, Klipstein-Grobusch K, De-Graft Aikins A, Addo J, et al. Dietary patterns and type 2 diabetes among Ghanaian migrants in Europe and their compatriots in Ghana: the RODAM study. Nutr Diabetes. 2018;8:25. https://doi.org/10.1038/s41387-018-0029-x.
Galbete C, Nicolaou M, Meeks KA, De-Graft Aikins A, Addo J, Amoah SK, et al. Food consumption, nutrient intake, and dietary patterns in Ghanaian migrants in Europe and their compatriots in Ghana. Food Nutr Res. 2017;61:1341809. https://doi.org/10.1080/16546628.2017.1341809.
Barbara Stadlmayr, Ruth U Charrondière, Victor N Enujiugha, Romaric G Bayili, Barbara Burlingame. West African Food Composition Table/ Table De Composition Des Aliments D'afrique De L'ouest; 2012.
Willett W, editor. Nutritional epidemiology. 3rd ed. New York: Oxford University Press; 2013.
Smits J, Steendijk R. The international wealth index (IWI). Soc Indic Res. 2015;122:65–85. https://doi.org/10.1007/s11205-014-0683-x.
Crewson P. Applied statistics handbook: AcaStat Software; 2006.
Stoop IAL (2010) Improving survey response: Lessons learned from the European Social Survey / Ineke Stoop … [et al.]. Oxford: Wiley
Dietary Reference Values for nutrients Summary report. (2017) EFS3. 14:e15121E. doi:https://doi.org/10.2903/sp.efsa.2017.e15121.
Nkondjock A, Bizome E. Dietary patterns associated with hypertension prevalence in the Cameroon defence forces. Eur J Clin Nutr. 2010;64:1014–21. https://doi.org/10.1038/ejcn.2010.109.
Obasohan PE, Okorie JN, Sule AL, Ndako KJ. Impact of dietary patterns, individual and workplace characteristics on blood pressure status among civil servants in Bida and Wushishi communities of Niger State Nigeria. PLoS ONE. 2019;14:e0226231. https://doi.org/10.1371/journal.pone.0226231.
Mank I, Vandormael A, Traoré I, Ouédraogo WA, Sauerborn R, Danquah I. Dietary habits associated with growth development of children aged < 5 years in the Nouna Health and Demographic Surveillance System. Burkina Faso Nutr J. 2020;19:81. https://doi.org/10.1186/s12937-020-00591-3.
Frank LK, Kröger J, Schulze MB, Bedu-Addo G, Mockenhaupt FP, Danquah I. Dietary patterns in urban Ghana and risk of type 2 diabetes. Br J Nutr. 2014;112:89–98. https://doi.org/10.1017/S000711451400052X.
Abubakari A, Jahn A. Maternal dietary patterns and practices and birth weight in Northern Ghana. PLoS ONE. 2016;11:e0162285. https://doi.org/10.1371/journal.pone.0162285.
Galbete C, Nicolaou M, Meeks KA, Aikins ADG, Addo J, Amoah SK, et al. Food consumption, nutrient intake, and dietary patterns in Ghanaian migrants in Europe and their compatriots in Ghana. Food Nutr Res. 2017. https://doi.org/10.1080/16546628.2017.1341809.
Becquey E, Savy M, Danel P, Dabiré HB, Tapsoba S, Martin-Prével Y. Dietary patterns of adults living in Ouagadougou and their association with overweight. Nutr J. 2010;9:13. https://doi.org/10.1186/1475-2891-9-13.
Wirfält E, Drake I, Wallström P. What do review papers conclude about food and dietary patterns? Food Nutr Res. 2013. https://doi.org/10.3402/fnr.v57i0.20523.
Thorpe MG, Milte CM, Crawford D, McNaughton SA. A comparison of the dietary patterns derived by principal component analysis and cluster analysis in older Australians. Int J Behav Nutr Phys Act. 2016;13:30. https://doi.org/10.1186/s12966-016-0353-2.
Horner NK, Patterson RE, Neuhouser ML, Lampe JW, Beresford SA, Prentice RL. Participant characteristics associated with errors in self-reported energy intake from the Women’s Health Initiative food-frequency questionnaire. Am J Clin Nutr. 2002;76:766–73. https://doi.org/10.1093/ajcn/76.4.766.
Antwi J, Ohemeng A, Boateng L, Quaidoo E, Bannerman B. Primary school-based nutrition education intervention on nutrition knowledge, attitude and practices among school-age children in Ghana. Glob Health Promot. 2020;27:114–22. https://doi.org/10.1177/1757975920945241.
Annan RA, Apprey C, Agyemang GO, Tuekpe DM, Asamoah-Boakye O, Okonogi S, et al. Nutrition education improves knowledge and BMI-for-age in Ghanaian school-aged children. Afr Health Sci. 2021;21:927–41. https://doi.org/10.4314/ahs.v21i2.55.
Gelli A, Becquey E, Ganaba R, Headey D, Hidrobo M, Huybregts L, et al. Improving diets and nutrition through an integrated poultry value chain and nutrition intervention (SELEVER) in Burkina Faso: study protocol for a randomized trial. Trials. 2017;18:412. https://doi.org/10.1186/s13063-017-2156-4.
Laar A, Barnes A, Aryeetey R, Tandoh A, Bash K, Mensah K, et al. Implementation of healthy food environment policies to prevent nutrition-related non-communicable diseases in Ghana: National experts’ assessment of government action. Food Policy. 2020;93:101907. https://doi.org/10.1016/j.foodpol.2020.101907.
Boysen O, Boysen-Urban K, Bradford H, Balié J. Taxing highly processed foods: What could be the impacts on obesity and underweight in sub-Saharan Africa? World Dev. 2019;119:55–67. https://doi.org/10.1016/j.worlddev.2019.03.006.
Symmank C, Mai R, Hoffmann S, Stok FM, Renner B, Lien N, Rohm H. Predictors of food decision making: a systematic interdisciplinary mapping (SIM) review. Appetite. 2017;110:25–35. https://doi.org/10.1016/j.appet.2016.11.023.
Monteiro CA, Cannon G, Levy RB, Moubarac J-C, Louzada ML, Rauber F, et al. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. 2019;22:936–41. https://doi.org/10.1017/S1368980018003762.
Pachucki MA. Food pattern analysis over time: unhealthful eating trajectories predict obesity. Int J Obes (Lond). 2012;36:686–94. https://doi.org/10.1038/ijo.2011.133.
Arsenault JE, Nikiema L, Allemand P, Ayassou KA, Lanou H, Moursi M, et al. Seasonal differences in food and nutrient intakes among young children and their mothers in rural Burkina Faso. J Nutr Sci. 2014;3: e55. https://doi.org/10.1017/jns.2014.53.
Becquey E, Delpeuch F, Konaté AM, Delsol H, Lange M, Zoungrana M, Martin-Prevel Y. Seasonality of the dietary dimension of household food security in urban Burkina Faso. Br J Nutr. 2012;107:1860–70. https://doi.org/10.1017/S0007114511005071.
Acknowledgements
We are grateful to the study team for supporting data collection and management, as well as to the participants for taking part in this study.
Funding
Open Access funding enabled and organized by Projekt DEAL. We acknowledge financial support for Konstantin Weil and Hannah Fuelbert by the Else Kröner-Fresenius-Stiftung within the Heidelberg Graduate School of Global Health. Else Kröner-Fresenius-Stiftung had no role in the design, analysis or writing of this article. The study and Ina Danquah were supported by the Robert Bosch Foundation within the framework of the Robert Bosch Junior Professorship 2019 (grant number 01000035–002). Robert Bosch Foundation had no role in the design, analysis or writing of this article. Alina Herrmann, Roch Modeste Millogo, Issa Coulibaly: None.
Author information
Authors and Affiliations
Contributions
KW contributed to data curation, formal analysis, investigation, methodology, software, validation, visualization, writing—original draft. IC contributed to data curation, investigation, validation, and writing–review and editing. HF performed project administration, investigation, and writing—review and editing. AH contributed to conceptualization, formal analysis, investigation, funding acquisition, methodology, project administration, and writing—review and editing. RMM contributed to conceptualization, data curation, investigation, methodology, project administration, supervision, and writing—review and editing. ID conceptualization, formal analysis, funding acquisition, investigation, methodology, project administration, software, supervision, and writing—review and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Ethics Committee for Medical Research, Health Ministry of Burkina Faso (2021–01-001, 13 January 2021). All participants gave written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: STROBE-nut checklist.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Weil, K., Coulibaly, I., Fuelbert, H. et al. Dietary patterns and their socioeconomic factors of adherence among adults in urban Burkina Faso: a cross-sectional study. J Health Popul Nutr 42, 107 (2023). https://doi.org/10.1186/s41043-023-00451-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-023-00451-w