
Abstract
Background
The persistent quality gap in maternal health services in Nepal has resulted in poor maternal health outcomes. Accordingly, the Government of Nepal (GoN) has placed emphasis on responsive and accountable maternal health services and initiated social accountability interventions as a strategical approach simultaneously. This review critically explores the social accountability interventions in maternal health services in Nepal and its outcomes by analyzing existing evidence to contribute to the informed policy formulation process.
Methods
A literature review and desk study undertaken between December 2018 and May 2019. An adapted framework of social accountability by Lodenstein et al. was used for critical analysis of the existing literature between January 2000 and May 2019 from Nepal and other low-and-middle-income countries (LMICs) that have similar operational context to Nepal. The literature was searched and extracted from database such as PubMed and ScienceDirect, and web search engines such as Google Scholar using defined keywords.
Results
The study found various social accountability interventions that have been initiated by GoN and external development partners in maternal health services in Nepal. Evidence from Nepal and other LMICs showed that the social accountability interventions improved the quality of maternal health services by improving health system responsiveness, enhancing community ownership, addressing inequalities and enabling the community to influence the policy decision-making process. Strong gender norms, caste-hierarchy system, socio-political and economic context and weak enforceability mechanism in the health system are found to be the major contextual factors influencing community engagement in social accountability interventions in Nepal.
Conclusions
Social accountability interventions have potential to improve the quality of maternal health services in Nepal. The critical factor for successful outcomes in maternal health services is quality implementation of interventions. Similarly, continuous effort is needed from policymakers to strengthen monitoring and regulatory mechanism of the health system and decentralization process, to improve access to the information and to establish proper complaints and feedback system from the community to ensure the effectiveness and sustainability of the interventions. Furthermore, more study needs to be conducted to evaluate the impact of the existing social accountability interventions in improving maternal health services in Nepal.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
The Government of Nepal (GoN) launched the Safe Motherhood Programme in 1997 to improve maternal and neonatal outcomes [1]. The programme particularly placed emphasis on addressing financial barriers to access maternal and newborn health services, institutional delivery and skilled birth attendant (SBA) at each birth [2, 3]. As a result, institutional delivery is widely promoted which led to nationwide expansion of birthing centres. Since then, there has been a considerable increment in the coverage of institutional delivery, from 8% in 1996 to 57% in 2016. However, expansion of birthing centres has not ensured the quality of care (QoC) at service delivery point as envisioned by the programme [4]. Despite the intense effort of the programme, Nepal is still facing challenges to reduce maternal mortality rate (MMR) as per the national and global target; the statistics is 239 per 100,000 live births [5]. Two major causes—persistent equity and quality gap—are observed as underlying causes for the slow and steady progress in maternal health outcomes in Nepal [2, 6]. The access and utilization of maternal health services are still primarily low among less educated women, women of the lowest wealth quintile and hard-to-reach (Table 1) [5].
A national survey of birthing centres reported only 5% of birthing centres satisfy the requirements of the Safe Motherhood Programme. Only half of the nursing staff of birthing centres are certified SBA. The infection prevention practices are considerably low among the staffs [4]. The health system-related factors such as cleanliness, hygiene, poor counselling, audio-visual privacy, lack of essential drugs and supplies, staff absenteeism and their attitude are major reasons behind dissatisfaction to maternal health services among the maternity clients [7]. Similarly, the lack of confidence in services being provided is a reason for underutilization of primary level of care which has resulted into overcrowding at the maternity unit in referral hospitals [8]. Available evidences, particularly from the developing contexts, suggest that it is essential not only to go beyond maximizing essential interventions to accelerate the progress in maternal health outcomes but also to invest for the quality maternal health services through accountable health system [9, 10].
Social accountability refers to an approach that enables the citizens to make service providers and policymakers responsible and answerable for their acts [11]. It has been considered an effective strategy to aggregate the voice of disadvantaged and marginalized people, enhance citizen-service provider relationships and improve state/service provider responsiveness towards effective and quality service delivery contributing to better maternal health outcomes in developing context [11,12,13,14].
The GoN with its commitment to inclusive and quality health care services has explicitly emphasized accountability and governance in its health strategy as a core principle to attain sustainable development goals (SDGs) in relation to maternal and newborn health [2, 15]. Major focus has been on universal health coverage (UHC) and its progressive expansion with continuous improvement in the quality of care being delivered, making service more affordable and covering wider population in need, especially the poor and vulnerable through social accountability interventions [2, 6].
Social accountability interventions aimed to improve maternal health are reported in many developing countries, but such reports in Nepal are very limited. Through the review of available literature, this paper intends to address the knowledge gap. The finding of the study is expected to provide comprehensive information about social accountability initiatives and right-based approaches to policymakers and health service providers engaged in health system, strengthening social accountability initiatives and right-based approaches to improve quality of maternal health services in Nepal.
Methods
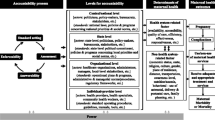
In-depth review of literature from different LMICs including Nepal was conducted to explore the social accountability interventions and their outcome in maternal health services. The review was done in December 2018 to May 2019. The adapted framework (Fig. 1) of Lodenstein et al. was used to critically analyse and synthesize existing literature. The framework was chosen over the World Bank accountability framework as the World Bank’s model specifically focuses on the citizen-policymaker relationship and does not discuss the importance of the contextual factors [16].

Conceptual framework of social accountability adapted from Lodenstein et al. [17]
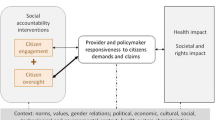
Originally, Lodenstein et al. conceptualized the social accountability interventions as a citizen-driven mechanism, where citizens voice their concern on the quality of services or/and service providers’ and policymakers’ performance. In return, the service providers and policymakers are asked to respond to those concerns [17]. Equally, citizen oversight the service providers’ and policymakers’ actions and decisions using accountability mechanism which result in improved responsiveness of service providers and policymakers. Improved responsiveness ultimately creates health and rights impact. The interventions, outcome and impact are, however, influenced by different contextual factors [17].
World Health Organization (WHO) has recognized community engagement interventions as a cornerstone to improve the quality of maternal and newborn care. Accordingly, Nepal has adopted a community participation approach in its health system and has incorporated community engagement and community oversight as central elements of the social accountability interventions [2, 18]. In this review, the term community engagement refers to the community voice or expression of concerns for the quality maternal health services without formal enforcement and community oversight which includes joint monitoring and evaluation of the maternal health services and health system. The interventions are anticipated to improve health service providers’ and policymakers’ responsiveness toward delivering quality maternal health services. Improved responsiveness ultimately creates health and rights impact by reducing maternal mortality and promoting equity and good governance.
The main keywords related to conceptual framework, that is, ‘social accountability interventions,’ ‘maternal health services,’ ‘community participation,’ ‘outcomes’ and ‘Nepal’ were combined using Boolean operators ‘OR’ and ‘AND’ to narrow down the search and produce conclusive evidence on the interventions. Literature was searched and extracted via search engines such as Google and PubMed database (search strategy presented in Appendix 1). For the national reports and data, authentic websites of GoN, different development agencies and organizations websites which include Ministry of Health and Population (MoHP) Nepal, Department of Health Services (DoHS) Nepal, Ministry of Federal Affairs and Local Development (MoFALD), WHO, World Bank and CARE Nepal were visited. Additionally, a snowball approach was used to access references mentioned in key review papers. While limited evidence related to outcomes of social accountability interventions in Nepal were found, evidences from other LMICs having similar maternal health and socio-economic context were included.
Aligning with the Local Self-Governance Act 1999, the MoHP implemented decentralization in the health sector in 2000, the same year was set as the lower limit for literature search. All published as well as unpublished (grey) and open-access literature between January 2000 and May 2019 were included in this review. Some relevant policy documents that were originally published in the Nepali language and later translated into English are also included in the review. Studies focussing on other approaches and interventions to improve maternal health services were excluded. For the national data, researchers NDHS 2016 and Annual report of the DoHS were used as a reference. Altogether, 451 free full-text articles from January 2000 to May 2019 were identified from the PubMed. Additional 63 articles were identified from Google Scholar, ScienceDirect and reference section of selected articles. Among the total 514 articles, 405 were removed from the review list as they did not match the title of study, place of the study and study population. From the remaining 109 articles, 48 duplicate articles were excluded. Similarly, 35 articles were removed as they did not contain relevant information, and 26 articles alongside national reports and documents were finally reviewed. The article selection process is presented in Fig. 2. The details of the articles included in the review with their key characteristics are presented in Table 2 (see Appendix 2 for the details of all literature included).

Article selection process
This review has summarized the findings according to the main elements of the conceptual framework linking it to QoC. The framework is based on theoretical perspectives that include social accountability, social accountability interventions, health system responsiveness and QoC, as defined in Table 3.
Results
Social accountability interventions and their outcome in maternal health services in Nepal
In Nepal, different social accountability tools have been used and tested by GoN and development partners to ensure community engagement in social accountability interventions in maternal health services. Similarly, there are established structures in the health system which facilitate community oversight to ensure the governance for improved quality maternal health services and promote social accountability. The major social accountability interventions and contextual factors affecting the interventions are listed in Table 4.
The key findings related to the social accountability interventions, process of the interventions and outcomes are presented in Table 5.
Community engagement
Social audit
Social audit is one of the major social accountability interventions which is initiated to improve the transparency of Safe Motherhood Programme and promote equity in the health system. Till fiscal year 2016/17, the programme was scaled up to 70 districts out of 77. The government has a plan to scale up the programme into all 77 districts by 2020 [6, 22].
Given that no scientific research examining the outcomes of social audit in Nepal or any other LMIC was found, the findings from the evaluation and review study of social audit in Nepal has been presented as evidence (Table 5). An evaluation study [23] undertaken in health facilities of Nepal reported overall improvement in the responsiveness of maternal health services. However, the study reported a different level of impact in each study district [22]. It was more effective in Palpa and Rupandehi where the social audit was conducted on regular basis with the technical support of donor agencies compared to Jhapa and Ilam where it was solely implemented by the government without any support from development partners [22]. This result suggests that regular practice of social audit improve maternal health outcomes.
Maternal Perinatal Death Surveillance and Response (MPDSR)
WHO has recognized the Maternal Death Review (MDR) as a relevant accountability tool for improved quality of the maternal and neonatal health (MNH) services which are based on the concept of the monitor-review-act cycle [23, 25, 43]. The GoN has merged the MDR program with ‘Maternal Perinatal Death Review (MPDR)’ programme and developed a comprehensive surveillance system named ‘MPDSR’. There are two types of MPDSR: facility-based and community-based in Nepal (see Appendix 3) [23].
The MoHP has established a web-based system to capture maternal deaths in Nepal. With the available data, MoHP has been able to identify the causes of death, and the MPDSR committee has developed action plans for different levels of care; yet, the implementation of those action plans has remained a challenge [2]. Nigeria encountered a similar problem in death reporting and implementation of developed action plans in the initial days. However, they incorporated the scorecard to monitor whether the action plans are being developed and if recommendations were being acted upon accordingly [25]. Based on experiences from Nigeria, this example can possibly be applied in Nepal to overcome the challenges and improve the outcomes of the MDR/MPDSR intervention.
Community Score Card/Community Health Score Board (CSC/CHSB)
Both community scorecard (CSC) and community health scoreboard (CHSB) were introduced at the same time in Nepal to promote health sector accountability. The CSC was piloted in 16 health posts by GoN with the support of World Bank in 2011 [26, 27]. CSC was found to contribute to actionable information regarding facility performance; however, due to high implementation cost and lack of competent human resources for the facilitation of the process, the government could not scale it up further in Nepal [21].
Based on the successful experience of CSC in Malawi, CARE-International introduced community health scoreboard (CHSB) in Nepal to improve the maternal health outcomes [28, 30]. Given the contextual similarities between Nepal and Malawi, Nepal is believed to expect similar outcomes of the CSC and/or CHSB in maternal health services. However, the sustainability of the intervention in Nepal is a major challenge, as its execution is being carried out by the donor with minimal involvement of government [21, 44].
Citizen Charter
Citizen charter is a tool to ensure the constitutional right of the Nepali citizen to access the information and the commitment of government for providing quality services in a transparent and accountable way [27]. The tool has been used mandatorily in the health sector to ensure transparency, improve service providers’ accountability, make the service users informed about the services and address the concern/grievances of citizen about the services. However, many oversights have been identified while posting information about the availability of essential drugs and services in the health facilities [45]. No evidence is found on the contribution/effectiveness of charter in the maternal health services in Nepal as well as in the other LMICs.
A report about social accountability in the health sector [21] stated that 29% of health facilities do not have citizen charter at their premises and even in places where there are charters, it is not being updated and maintained on a timely basis [21]. This is mainly because of weak enforceability mechanism in the health sector [21, 45].
Grievance/complaint handling tool
GoN enforced establishment of a grievance/complain handling mechanism in every public sector including health under the good governance (management and operation) act 2008 [27]. In the health facility, suggestion or complaint boxes are mandatory for handling the grievances and complaints [21]. The box is placed in the premises of health facilities to receive the complaints and/or grievances from the service users, communities as well as other stakeholders about the health services they receive [21].
“… not only at the health facility level but even at the district level, the situation is that suggestion boxes are filled up with ‘spider webs.’ As far as I know the suggestion box is not in use. No one puts their complaints or suggestions [into the suggestion box] by writing onto a piece of paper. Many do not know about its existence. So, I do not see any importance of it”—PHC clinic manager [46].
Moreover, MoHP Nepal has established a digital system to receive complaints via email and Twitter [47]. The district hospitals and district public/health offices are instructed to have their websites which must include information regarding organization, programme and activities including budget and also run a Facebook and Twitter account to foster accountability and transparency and improve service users’ access to the information [21]. Apart from that, MOH has initiated a digital monitoring campaign called ‘Smart Health Nepal’ through its website: https://www.mohp.gov.np [48]. Although the complaint/grievance box contributes to enhancing accountability and transparency, their uses are limited in practice and the required attention is given to systematically place it as a part of a broader accountability system; thus, it fails to serve its purpose [21, 32, 46]. The statement from a study in Nepal as shared in [46] also highlights the attitude of the health workers on the usefulness of complaint box [46].
Community oversight
Health Facility Operation Management Committee (HFOMC)
In line with the objective of Local Self-Governance Act 1999, MoHP devolved its power and responsibilities to HFOMC at the local level for the overall management of their respective health facilities [44, 49]. Furthermore, the local government operation act 2017, has given necessary responsibility to the HFOMC for planning, implementation, and monitoring of the health services [34, 50]. The committee plays an influential role in raising resources for maternal health services in the community. They serve as a strong and inclusive voice mechanism of the community in social accountability interventions [29, 34, 51].
According to the HFOMC guideline, the committee is required to meet once a month to discuss the health facility issues and operational challenges, develop plan of action for effective management of the health facility and review previous action plans, but this is limited in practice [21, 34].
Female Community Health Volunteers (FCHVs)
The FCHV programme was initiated in 1988 in Nepal. Initially, the volunteers were assigned to promote Family Planning (FP) services in the community. With improved performance of the programme, their role and responsibilities were gradually expanded to the continuum of care [36]. The FCHVs are known for their remarkable contribution to the reduction of maternal and child morbidity and mortality in Nepal [2, 37].
The FCHVs liaison the mothers’ group and HFOMC at the community level [38]. Moreover, they play an important role in the initial reporting system in community-based MPDSR and voice mechanism of the marginalized and disadvantaged women in the social accountability interventions [2, 21]. Being an important stakeholder of the community, they also monitor and evaluate the performance and quality of health services [36]. Various development partners and government line agencies have mobilized them in health system strengthening programmes recognizing their proximity with the community people and their contribution in MCH sector [21, 39].
Mothers’ group for health
The mothers’ group have been recognized as an innovative strategy for ensuring women’s participation to improve the MCH outcomes in Nepal. They are formed at the community level under the initiation of the local health facility [36]. The group is a voice mechanism to raise maternal health concerns in social accountability interventions [21]. This accountability intervention has been considered a cost-effective strategy to save women’s life as per as WHO standard [41]. A study in Nepal concluded that mothers’ group are trusted representatives of women and intermediaries in the social accountability interventions. However, a clear mandate from the policy level is required and their capabilities need to be improved for their active role in social accountability process [29].
Civil Society Organization (CSO)
CSOs have been identified as a strong community engagement and oversight mechanism in the accountability and governance process in the health sector [21, 42]. In regards to maternal health, they have played a vital role in advocacy for addressing maternal health problems and promoting accountability from community to central level [39]. In Nepal, local NGOs are mostly involved in implementing social accountability interventions initiated either by the government or development agencies [21]. Some of the NGOs also provide preventive and promotive maternal health services and maternal care too in some cases [2, 21]. Meanwhile, the INGOs provide technical and financial support to the government for the policy and guideline development and for the implementation of social accountability interventions and strategies in the health system [2, 21, 22, 52].
Contextual factors influencing social accountability interventions in Nepal
Social-cultural context
Gender Norms
Nepalese society is a patriarchal society where strong gender norms exist. Traditionally, men are privileged with power and position; consequently, women’s participation in the governance system is considerably low [53]. Therefore, to address the issue and empower women for their meaningful participation in each sector of development, GoN has made a reservation for women [42, 54]. Women’s participation has also been ensured in the HFOMC with the mandatory provision of having at least three women out of seven committee members [34].
While government has emphasized women and marginalized groups’ participation in each level of governance to enhance gender equality and social inclusion, they tend to show less interest in accountability interventions due to unequal power relationship, low education, and overload with household chores as well as productive and reproductive works [21, 53, 55]. In most cases, women’s presence in the meetings are not meaningful as they speak only if explicitly requested [53]. Hence women’s roles are confined only up to their physical presence at the programmes while men are the ultimate decision-makers [53]. However, evidence has shown that the increased women’s involvement in participatory decision-making process results in a notable improvement in maternal health services which ultimately reduces maternal mortality and morbidity [40, 41, 56].
Social structure
The country has a complex caste system with diverse ethnic groups where the Brahman/Chhetri refers to the so-called upper caste and are most privileged group while the Dalit as disadvantaged caste and Janjati—indigenous group—are underprivileged [57]. This caste-based social structure in Nepal has hindered effective participation of the marginalized groups in the social accountability interventions [53]. Earlier, there was a mandatory reservation for a marginalized and disadvantaged group in the HFOMC; in 2019, the provision was abolished from the system. Now, they (one member from Dalit, disable and adolescent) are invitee member of the committee, and they do not have an influencing role as a core member in the decision-making process [34].
This caste hierarchy often produces an unequal power relation between the service providers and service users. The marginalized community have less power to negotiate for change in the health service providers attitude and behaviour [31, 59, 60]. In a qualitative study by Gurung et al., a Dalit member expressed how caste hierarchy system has suppressed their voice and participation in the accountability process [58].
“In the committee, most of the members are from higher castes. When we have meetings of the committee or any other programme, and when there is time for taking snacks, the other committee members sit a short distance away from me. There is thus still discrimination in our society. It [untouchability issue] is not in all places, but still exists with some people in some places. Due to this, it causes me stress inside. Then, how can I speak in the meeting or any events without hesitation?” [58].
Any form of discrimination is prohibited by law in Nepal; yet, the issue of caste-based discrimination is still deeply rooted in the community [54, 58, 61]. Hence, the existing informal power relationship and the dynamics of social structures need to be taken into consideration to ensure the effectiveness of the social accountability process.
Awareness, value, beliefs and practices
The effectiveness of social accountability interventions is often influenced by the level of people’s awareness about their rights and entitlements, the existing governance mechanism to protect it and their role in it [12]. In Nepal, majority of the people are unaware of the concept of accountability and governance that makes it difficult to hold service providers accountable for their actions [21, 31]. Although access to the information is a constitutional right of every Nepali citizen, women, the poor and disadvantaged groups are less likely to be aware of their rights to get quality health services [54]. Meanwhile, literacy level, perception and cultural beliefs are hindering factors for it [31, 62].
In Nepal, health belief and practices also influence the level of community participation in social accountability interventions [63]. Similarly, engaging youth and marginalized people in the social accountability interventions are difficult, as youth often hesitate to share their opinion in front of elders and mass, respectively, while marginalized people think their issues are irrelevant to be addressed [63, 64]. Despite having grievances regarding health services and providers’ performance, in most cases, the community tend to stay silent and thus are generally vulnerable and marginalized [46]. Similarly, in Nepalese society, the culture of raising questions and providing feedback to the power holders and prompt respond toward feedback is not properly established which also affect the community engagement in the social accountability interventions [46].
Political and economic context
Nepal has gone through various political and structural transitions in the last two decades which has resulted in the unstable political situation and huge governance challenges [31, 44]. Similarly, the issue of political interference in the health sector has been well reported. Often, politics acts as a driving force in the formation and functioning of the HFOMC [58] that interfere with the social accountability process [22, 44]. The decisions are often made on the political ground by the leaders often undermining the community’s concerns. The bureaucracy of health facility, kinship and health worker’s power tends to determine the level of community engagement in the accountability interventions [44, 58, 65].
An evaluation of social audit reported the issue of political pressure in the selection and retention of competent NGO to facilitate the social audit process in the health facilities [22]. Sometimes, intense pressure from government officials and local leaders result in the replacement of experienced NGO with the favoured one which directly affects the quality implementation of social accountability interventions [22]. This kind of political influences tends to increase conflict of interest in social accountability interventions, process and outcomes.
In Nepal, most of the health workers are associated with trade union and sister organization of political parties. The health workers often use this nexus for their deployment and retention at well-facilitated places; it has resulted in a persistent vacant post of regular and skilled staffs in the remote health facilities [44, 65, 66].
Health system context
Client-provider relationship
Health workers are recognized as an intellectual and respected personality in the community, and their profession is perceived as a highly prestigious profession in Nepal. Hence, the community hardly thinks that health workers commit any mistakes while providing and managing services. This perception often imbalances the power-relation between service users and providers, and often impacts the dialogue and negotiation in the social accountability interventions [46]. In fact, in remote areas where there are no choices for health services, the community often hesitate to complain or to provide feedback to avoid unnecessary conflict and/or the fear of getting poor quality of services in the next visit. A quote from the interview with a NGO staff in a rural health facility reflects the perception of the community toward accountability interventions [46].
“How can Dalit, women, and the marginalized speak their minds with service providers? They think what the government does is all right. Health is the matter related to life and death. If you or your family member becomes ill, you have to go to the same place. Then, how could you take issue with the service providers? In villages, there is no option”— (Qualitative interview, staff, NGO) [46].
Sometimes, health workers and HFOMC members also tend to skip the interface with the community due to the fear of being criticized in the accountability interventions like social audit, CHSB etc. [44, 67].
Resource availability
Persistent resource deficiency in the health sector limits the health workers’ and policymakers’ responsiveness towards the community [22, 67]. The health facility management has been handed over to the local authority; however, human resource and logistics management are still being performed centrally which has made demand-supply procedure complex [21, 44]. This has resulted in the frequent stock-outs of essential drugs and supplies and scarcity of human resources. Moreover, in the federal government system, the line of accountability between MoHP, provincial and the local government has not been explicitly defined which has further created responsibility dilemma among local authorities to manage health facilities under their responsibilities [21, 44, 61].
The budget provided to local government is insufficient to fulfil the community health priorities identified during the social accountability interventions—a major chunk of it needs to be spent in the staffs’ salary and operation costs [21]. Additionally, due to the human resources gap at community level health facility, FCHVs are overwhelmed with community-based health interventions like Safe Motherhood Programme, FP, immunization, nutrition, MPDSR and mothers’ group meetings, among others. They are also being used by other several sectors such as education, forest groups and micro-credit finance groups for their accountability purpose in the community [37]. Ultimately, they are volunteers and only get an event-based incentive; therefore, increased responsibilities with minimal incentive decrease their motivation to work [36, 37]. This might impact the quality service delivery and their responsiveness toward the community concerns.
Monitoring and evaluation
The different levels of GoN monitor social audit process, budget versus expenditure, use of citizen charter, use of grievance handling mechanism, the regularity of HFOMC meeting and regulatory of mother groups meetings. Besides, local councils also monitor programs/activities of the CSOs regularly [44, 50]. However, low responsiveness of the health system has interlinkages with the absence of proper monitoring and evaluation mechanism [6, 49]. Understandably, very few facilities and those located only at feasible geographic locations are frequently monitored and receive regular supervision from the higher authorities [21, 65]. District supervisors are often busy in conducting training and workshops which leave them with less time for supervision and monitoring at community-level health facilities [65]. This has weakened the effectiveness of established social accountability interventions. The regular follow-up and analysis of social audit action plans from the district and/or central level are almost non-existent in the health system [21, 22, 44].
Evidence shows that the demand-side social accountability interventions involve dialogue process which usually puts soft pressure to the health workers to be accountable for their action and responsibility. It is argued that, in the long run, without the threat of penalty from the state or enforcing legal mechanism, the social accountability interventions are likely to address only surface level service delivery issues and thereby affect the sustainability of the interventions [13, 29]. Thus, the health system needs to strengthen the monitoring and supervision mechanism and enforce legal mandate for effective and sustained outcomes of social accountability interventions.
Discussion
The study found that GoN is committed to improving the responsiveness of maternal health services; hence, various social accountability interventions have been implemented by government/state (supply-side) and development partners (demand-side). Social audit, MPDSR, citizen charter and complaint/grievances handling interventions have been identified as supply-side community engagement interventions, whereas the CSC and CHSB are demand-side interventions. The HFOMC, FCHVs, and mothers’ group for health are a formal structure in the health system to ensure community engagement and oversight in the social accountability interventions. They are considered to bridge the gap between community and health system. Further, they serve as mediators to voice community concerns especially for the women, disadvantaged and marginalized groups in the decision-making process. Meanwhile, CSOs are non-state structures and found to have an advocacy role for the interventions.
This study identified a gap in meaningful community engagement in the accountability process. Mostly, the involvement of women, Dalit and adolescents in the HFOMC meetings and the decision-making process is often done as a formal procedure. Similarly, their level and depth of participation have not been utilized properly [21, 46, 53, 58]. In brief, strong gender norms, caste discrimination, political and economic influences, resource deficiencies and weak enforceability mechanism are found as the most influencing factors for social accountability interventions in Nepal which need to be considered while designing and implementing the interventions.
Social audit and MPDSR are widely promoted supply-side interventions in maternal health services by GoN. This review showed that the government has contributed to improving the responsiveness of Nepal’s health system and the delivery of quality maternal health services. However, further scientific studies are needed to generate a strong argument for that. Despite its effectiveness, there is a gap in the quality implementation of the social audit which consequently affects its outcomes. This is due to the contextual factors such as weak monitoring and regulatory mechanism, political interference, resource constraints in the health system and power limitation at the local level. The social audit has been practised as an event to expenses budget rather than a process; thus, interventions are not producing expected outcomes. There is a lack of reflection on the processes and built action plans from related higher authorities. Additionally, a gap identified in the integration of developed action plans during social audit into the policy level decision-making aggravates the problem further [21, 22, 44].
Concerning MPDSR, further research is recommended to generate strong evidence. MPDSR could be effective to improve the quality of maternal health services and avoid ‘delays’ in receiving the services if the developed action plans are implemented [10, 24, 25, 43]. However, as the tool specifically focusses on individual mistakes, it might promote fear among health care workers around the management of obstetric emergency care. Therefore, it is imperative to consider constructive environment focuses on systematic weakness with an opportunity to improve [25].
Considering the difficulties of illiterate people who cannot read the information written in citizen charter, it is necessary to prepare alternatives to inform people about the availability of services. Disseminating the information from television, radio and mobile phone can be alternative means for these groups. The fact that almost every household in Nepal has at least one mobile phone [5] shows the opportunity of information dissemination via short message or voice message. Though the short message may not work for illiterate people, voice message or toll-free call services can be considered more effective message dissemination tool for such communities.
A report by Commissions for the Investigation of Abuse of Authority (CIAA) showed the health sector in Nepal in 5th place amongst the 9 sectors for the highest number of complaint about power abuse which indicated potential corruption vulnerabilities in the health system [68]. To address such serious issue, CSOs and local government need to collaborate with the local councils for enforcement of regulations for the internal control systems of the local governance ordinance [21].
Mafuta, in his research [12], highlighted that social accountability interventions work effectively in maternal health services if women are allowed to express their concerns and have access to channels to provide feedback, and health service providers are positive toward user feedback and willing for behavioural changes [12]. This is relevant to Nepal as well as past researches which have shown a positive correlation between women participation in social accountability intervention and its impact on maternal health outcomes [40, 41].
Poor information dissemination might result in information asymmetry between providers and users, ultimately affecting the quality of the service delivery. Without awareness, the community may not be able to evaluate the components of QoC in maternal health services and to claim their rights entitlements; this ultimately leads to superficial community participation and produce suboptimal outcomes [69]. The study also identified a gap in the complaint capturing and handling mechanism in the health system. Community people often prefer informal channels to express their complaint/grievances or provide feedback in Nepal. The initiatives of MoHP through a web-based complaint handling mechanism [48], however, may not be feasible for the local population who are not internet users and technology-friendly. According to the International Telecommunication Union (ITU), only 34% of the Nepalese population has access to the internet [70]. Therefore, an effort is needed to establish other informal channels such as mobilization of committee members, mothers’ group and anonymous complaint registry through call, among others, to acquire the relevant feedback.
Political instability and bureaucratic influences have resulted in low trust among the community over the state, and thus, the government needs to put an effort in improving trust between citizen and state [13, 44, 65]. This will help to improve the client-provider relationships and effectiveness of social accountability interventions. To do so, it is very necessary to improve access to information for the community and increase their awareness of the right entitlements and legal enforcement.
Without sufficient resources and power at the local level, social accountability cannot produce optimal outcomes. Studies have shown that fulfilment of the permanent post, construction of major infrastructures, purchase of drugs and commodities and improving monitoring and a supervisory visit to health facilities, etc are not under the control of health management committee and community people [21, 22, 30, 44, 58]. Therefore, there is a need for proper devolution of power at a local level and strengthening of their political capabilities. This would be a critical step to avoid political and economic interference and power symmetry as well as contribute to managing resource constraints at the local level.
For the evidences to drive into action in maternal health services, they need to be designed and communicated in a way that triggers the policymakers’ will to address persistent resource scarcity [71]. Local NGOs and INGOs can play a crucial role to enforce policy into action as they are mostly engaged in an advocacy role and policy support at multiple levels.
Regarding demand-side interventions, the study found that they have proven to improve the quality of maternal health services in different LMICs including Nepal. Nevertheless, despite their effectiveness of improving health system responsiveness, some limitations have been observed. For example, CHSB is focused on specific groups and is project-oriented where sustainability largely depends on the donors funding. Similarly, MOHP is not able to scale-up CSC due to resource constraint and lack of technical competencies. The study found that donor-initiated interventions have been implemented without a clear vision of their sustainability [21, 44]. The CSC, CHSB and social audit have many similarities; thus, implementation of fragmented interventions may lead to duplication of efforts and wastage of resources. Therefore, specific and collaborative effort is required from both government and development partners for the integration of those interventions and institutionalization of those interventions to improve efficiency and to ensure the sustainability which will ultimately improve maternal health services in Nepal.
Limitations
The findings of this study ground on literature review and desk study of the available scholarly literature and study reports. Among them, very limited researches provided a comprehensive information on the outcomes of social accountability interventions in the maternal health services in Nepal. This might be due to the lack of required emphasis on the focused studies. Given this condition, the studies from LMICs having similar maternal health and socio-economic context are presented to give an overview of how social accountability improves maternal health services in the contexts like Nepal.
Furthermore, the analysis of the study focused on quality issues in public health facilities. Understandably, private health institutions providing maternal health services also have cases of poor QoC, but they have not been explored in this review [6, 8]. Conclusions, therefore, should be comprehended and interpreted considering this limitation as well. None of these limitations, however, should be understood as a compromise to the quality issues; they have been ensured by reviewing all peer-reviewed articles, national-level survey reports and evaluation studies, and evidences published in official governmental and organizational websites.
Conclusions
Various social accountability interventions, both at supply-side and demand-side, have been implemented to improve the responsiveness of maternal health services in Nepal. Despite the effective outcomes of the supply-side interventions, quality implementation is a key issue. Insufficient monitoring and evaluation, resource constraints, weak response system and political influences are identified as major responsible factors. Demand-side interventions are also found to have positive influences on the health system responsiveness. However, the interventions are project-oriented and donor-dependent. Therefore, clear policy guidance is needed for standardization and sustainability of the donor-initiated social accountability interventions. Similarly, contextual factors, such as socio-cultural factors (gender norms, social structure, value beliefs), health system factors (client-provider relationship, resource availability, monitoring and evaluation), and political-economic factors are found to operate as determining factors for effectiveness and sustainability of the social accountability interventions. Eventually, the evidence that directly links social accountability to improved maternal health services is not strong. Therefore, there is a strong need for investment in research in social accountability interventions and its impact on maternal health services in Nepal to enhance evidence-based practices and approaches.
Availability of data and materials
Not applicable
Abbreviations
- ANC:
-
Antenatal care
- CARE:
-
Cooperative for Assistance and Relief Everywhere
- CHSB:
-
Community Health Score Board
- CSC:
-
Community Score Card
- CSOs:
-
Civil Society Organizations
- DFID:
-
Department for International Development
- DHO/DPHO:
-
District Health Office/District Public Health Office
- DoHS:
-
Department of Health Services
- FCHVs:
-
Female Community Health Volunteers
- HFOMC:
-
Health Facility Operation and Management Committee
- INGOs:
-
International Non-Governmental Organizations
- LMICs:
-
Low and middle-income countries
- MCH:
-
Maternal and child health
- MDR:
-
Maternal death review
- MMR:
-
Maternal mortality ratio
- MNH:
-
Maternal and neonatal health
- MoFALD:
-
Ministry of Federal Affairs and Local Development
- MoH:
-
Ministry of Health
- MoHP:
-
Ministry of Health and Population
- MPDR:
-
Maternal Perinatal Death Review
- MPDSR:
-
Maternal Perinatal Death Surveillance and Response
- NHRC:
-
Nepal Health Research Council
- NHSS:
-
Nepal Health Sector Strategy
- PHC:
-
Primary health care
- QoC:
-
Quality of care
- RCT:
-
Randomized controlled trial
- SDGs:
-
Sustainable development goals
- SBA:
-
Skilled birth attendant
- UHC:
-
Universal Health Coverage
- WHO:
-
World Health Organization
References
Ministry of Health and Population. Second Long Term Health Plan 1997-2017: Perspective Plan for Health Sector Development. Kathmandu: Health Sector Reform Unit; 2007.
Ministry of Health and Population. Annual Report 2073/74 (2016/17). Kathmandu: Department of Health Services; 2018.
Ministry of Health and Population. National Policy on Skilled Birth Attendants: Supplementary to Safe Motherhood Policy 1998. Kathmandu: Family Health Division; 2006.
Ministry of Health and Population. Results from assessing birthing centers in Nepal. Kathmandu: Family Health Division; 2014.
Ministry of Health Nepal, New ERA and, ICF. Nepal Demographic and Health Survey 2016. Kathmadu; 2017.
Government of Nepal. Nepal Health Sector Strategy 2015-2020. Kathmadu: Ministry of Health and Population; 2015.
Ministry of Health and Population (MOHP) [Nepal], Social Development Forum and, Nepal Health Sector Support Program (NHSSP). Service Tracking Survey 2013. Kathmandu; 2014.
Ministry of Health. Nepal’s Every Newborn Action Plan. Kathmandu: Department of Health Services; 2016.
Tunçalp Ӧ, Were W, MacLennan C, Oladapo O, Gülmezoglu A, Bahl R, et al. Quality of care for pregnant women and newborns—the WHO vision. BJOG An Int J Obstet Gynaecol. 2015;122:1045–9. https://doi.org/10.1111/1471-0528.13451.
Hulton L, Matthews Z, Bandali S, Izge A, Daroda R, Stones W. Accountability for quality of care: monitoring all aspects of quality across a framework adapted for action. Int J Gynecol Obstet. 2016;132:110–6. https://doi.org/10.1016/j.ijgo.2015.11.005.
Malena C, Forster R, Singh J. Social accountability: an introduction to the concept and emerging practice. Washington DC: World Bank Social Development Papers: Participation and Civic Engagement; 2004.
Mafuta EM. Improving performance and responsiveness of maternal health services through social accountability mechanisms in the Democratic Republic of the Congo: Strengthening the interface role in community participation: Vrije Universiteit; 2017.
Lodenstein E, Dieleman M, Gerretsen B, Broerse JE. Health provider responsiveness to social accountability initiatives in low- and middle-income countries: a realist review. Health Policy Plan. 2017;32:125–40. https://doi.org/10.1093/heapol/czw089.
Mafuta EM, Dieleman MA, Hogema LM, Khomba PN, Zioko FM, Kayembe PK, et al. Social accountability for maternal health services in Muanda and Bolenge Health Zones, Democratic Republic of Congo: a situation analysis. BMC Health Serv Res. 2015;15:514. https://doi.org/10.1186/s12913-015-1176-6.
Government of Nepal. Nepal’s Sustainable Development Goals Status and Roadmap: 2016-2030. Kathmandu; 2017.
The World Bank. World development report 2004: Making services work for poor people. Washington, D.C.: The World Bank and Oxford University Press; 2004.
Lodenstein E, Dieleman M, Gerretsen B, Broerse JE. A realist synthesis of the effect of social accountability interventions on health service providers’ and policymakers’ responsiveness. Syst Rev. 2013;2:98. https://doi.org/10.1186/2046-4053-2-98.
Standards for improving quality of maternal and newborn care in health facilities: WHO; World Health Organization, Geneva, 2016.
de Silva A. A framework for measuring responsiveness. In: GPE Discussion Paper Series: No. 32. Geneva: World Health Organization; 2000. p. 1–42.
Neupane BD. A review of social audit guidelines and practices in Nepal. Kathmandu: Nepal Health Sector Support Programme; 2011.
Jarman D, Ghimire K. Situation Analysis on Social Accountability in the Health Sector (SAHS). Kathmandu: DFID/Nepal Health Sector Programme III (NHSP3); 2017.
Human Resource Development Center. Social Audit Process Evaluation Report. Kathmandu: Ministry of Health and Nepal Health Sector Support Programme; 2015.
Ministry of Health and Population. Maternal and Perinatal Death Surveillance and Review (MPDSR) Guideline. Kathmandu: Department of Health Services. Family Health Division; 2015.
Biswas A, Rahman F, Halim A, Eriksson C, Dalal K. Maternal and neonatal death review (MNDR): a useful approach to identifying appropriate and effective maternal and neonatal health initiatives in Bangladesh. Health. 2014;06:1669–79. https://doi.org/10.4236/health.2014.614198.
Bandali S, Thomas C, Hukin E, Matthews Z, Mathai M, Ramachandran Dilip T, et al. Maternal Death Surveillance and Response Systems in driving accountability and influencing change. Int J Gynecol Obstet. 2016;135:365–71. https://doi.org/10.1016/j.ijgo.2016.10.002.
World Bank. Social Accountability In Action. Kathmandu: Program for Accountability in Nepal (PRAN); 2011.
Kedar K, Chiranjibi B. Sourcebook of 21 Social Accountability Tools. World Bank. Kathmandu: Program for Accountability in Nepal (PRAN); 2012.
CARE-Nepal. Community Health Score Board (CHSB); 2012. p. 1–8. http://www.carenepal.org/uploads/pdf/publication/_CHSB_final document.pdf. Accessed 2 May 2019.
Hamal M, Heiter K, Schoenmakers L, Smid M, de Cock BT, De Brouwere V, et al. Social accountability in maternal health services in the far-western development region in Nepal: an exploratory study. Int J Health Policy Manag. 2019;8:280–91. https://doi.org/10.15171/ijhpm.2019.05.
Gullo S, Galavotti C, Sebert Kuhlmann A, Msiska T, Hastings P, Marti CN. Effects of a social accountability approach, CARE’s Community Score Card, on reproductive health-related outcomes in Malawi: a cluster-randomized controlled evaluation. PLoS One. 2017;12:e0171316. https://doi.org/10.1371/journal.pone.0171316.
Tamang S, Malena C. The political economy of social accountability in Nepal. Kathmandu: Program for Accountability in Nepal (PRAN); 2011.
Gurung G, Gauld R, Hill PC, Derrett S. Citizen’s Charter in a primary health-care setting of Nepal: an accountability tool or a “mere wall poster”? Health Expect. 2018;21:149–58. https://doi.org/10.1111/hex.12596.
Atela M, Bakibinga P, Ettarh R, Kyobutungi C, Cohn S. Strengthening health system governance using health facility service charters: a mixed methods assessment of community experiences and perceptions in a district in Kenya. BMC Health Serv Res. 2015;15:539. https://doi.org/10.1186/s12913-015-1204-6.
Ministry of Health and Population. Health Facility Operation and Management Committee—a reference guideline for local level. Kathmandu: Department of Health Services. National Health Training Center; 2019.
Shakya HS, Adhikari S, Gurung G, Pant S, Aryal S, Singh AB, et al. Strengthening national health systems for improving efficiency of health service delivery in Nepal. J Nepal Health Res Counc. 2012;10:101–7 http://www.ncbi.nlm.nih.gov/pubmed/23034370.
Ministry of Health and Population. National Female Community Health Volunteer Program Strategy (Unofficial Translation). Kathmandu: Family Health Division; 2010.
Khatri RB, Mishra SR, Khanal V. Female community health volunteers in community-based health programs of Nepal: future perspective. Front Public Health. 2017;5:1–4. https://doi.org/10.3389/fpubh.2017.00181.
Hamal M, Dieleman M, De Brouwere V, de Cock Buning T. How do accountability problems lead to maternal health inequities? A review of qualitative literature from Indian public sector. Public Health Rev. 2018;39:9. https://doi.org/10.1186/s40985-018-0081-z.
Ministry of Health and Population. Success factors for women’s and children’s health: Nepal. Geneva: World Health Organization; 2014.
Manandhar D, Osrin D, Shrestha B, Mesko N, Morrison J, Tumabhangphe K, et al. Effect of a participatory intervention with women’s group on birth outcomes in Nepal: cluster randomized controlled trial. Lancet. 2004;364:970–9.
Prost A, Colbourn T, Seward N, Azad K, Coomarasamy A, Copas A, et al. Women’s groups practising participatory learning and action to improve maternal and newborn health in low-resource settings: a systematic review and meta-analysis. Lancet. 2013;381:1736–46. https://doi.org/10.1016/S0140-6736(13)60685-6.
Ministry of Federal Affairs and Local Development. Annual Progress Report- NFY 2073/74 (2016/2017). Kathmandu: Local Governance and Community Development Programme (LGCDP)-II; 2017.
van den Broek N, Graham W. Quality of care for maternal and newborn health: the neglected agenda. BJOG An Int J Obstet Gynaecol. 2009;116(Suppl. 1):18–21. https://doi.org/10.1111/j.1471-0528.2009.02333.x.
Pact. Social Accountability in the Health Sector Programme (SAHS): applied political economy analysis (baseline). Kathmandu: U.K. Agency for International Development; 2017.
Nepal RB. A study on the policies and practices of the Government of Nepal on the free distribution of medicine. Kathmandu: Transparency International Nepal; 2016.
Gurung G, Derrett S, Gauld R, Hill PC. Why service users do not complain or have ‘voice’: a mixed-methods study from Nepal’s rural primary health care system. BMC Health Serv Res. 2017;17:81. https://doi.org/10.1186/s12913-017-2034-5.
Ministry of Health and Population. Feedback. Right to Information Act 2007. http://www.mohp.gov.np/feedbacks. Accessed 18 Dec 2018.
Ministry of Health and Population. Smart Health Nepal: Right to Information Act 2007; 2017. http://www.mohp.gov.np/. Accessed 15 Feb 2019.
Ministry of Health, New ERA Nepal, Nepal Health Sector Support Program (NHSSP) and, ICF. Nepal Health Facility Survey 2015. Kathmandu: Ministry of Health, Nepal; 2017.
Government of Nepal. Local Government Operation Act, 2074. Kathmandu: Nepal: Ministry of Law, Justice and Parliamentary Affairs; 2017.
Oostdam S, Hamal M, Dieleman M, De Brouwere V, Bardají A, Tiwari DP, et al. Social accountability in maternal health services in Baglung district, Nepal: a qualitative study. J Glob Heal Reports. 2018. https://doi.org/10.29392/joghr.2.e2018041.
Government of Nepal. Nepal Health Sector Strategy—Implementation Plan 2016–2021. Ministry of Health. Kathmandu; 2017.
Cima O. Accountability at the local level in fragile contexts: Nepal case study: Working Paper.HELVETAS and Institute of Development; 2013.
Government of Nepal. Constitution of Nepal, 2072 (2015). Kathmandu: Ministry of Law, Justice and Parliamentary Affairs; 2015.
National Planning Commission Secretariat. Nepal in Figures 2015. Kathmandu: Central Bureau of Statistics; 2015.
Rifkin SB. Examining the links between community participation and health outcomes: a review of the literature. Health Policy Plan. 2014;29(suppl 2):ii98–106. https://doi.org/10.1093/heapol/czu076.
National Planning Commission Secretariat. National Population and Housing Census 2011 (National report). Kathmandu: Central Bureau of Statistics; 2012.
Gurung G, Derrett S, Hill PC, Gauld R. Nepal’s Health Facility Operation and Management Committees: exploring community participation and influence in the Dang district’s primary care clinics. Prim Health Care Res Dev. 2018;19:492–502. https://doi.org/10.1017/S1463423618000026.
Ministry of Health and Population. Human Resources for Health Nepal Country Profile. Kathmandu: Nepal Health Sector Support Programme; 2013.
Paudel NR. Inclusive governance: a case study of civil service in Nepal. J Gov Innov. 2016;II:19–40 http://osderpublications.com/uploads/1551844368.pdf.
Ghale S. The long, hard road to federalism: a new report reveals the challenges that local governments are facing across the country: The Kathmandu Post; 2018. http://kathmandupost.ekantipur.com/printedition/news/2018-07-11/the-long-hard-road-to-federalism.html. Accessed 12 Jan 2019.
Fehringer J, Bhandari P, Ghimire D, Lohani JR, Dawadi B, Acharya V, et al. Impact evaluation of approaches to strengthen health facility operation and management committees in Nepal, Summary of the baseline report. MEASURE Evaluation. North Carolina; 2015.
McCoy DC, Hall JA, Ridge M. A systematic review of the literature for evidence on health facility committees in low- and middle-income countries. Health Policy Plan. 2012;27:449–66. https://doi.org/10.1093/heapol/czr077.
Hoffmann KD. The role of social accountability in improving health outcomes : overview and analysis of selected international NGO experiences to advance the field. Washington, DC: CORE Group; 2014.
Gurung G, Derrett S, Hill PC, Gauld R. Governance challenges in the Nepalese primary health care system: time to focus on greater community engagement? Int J Health Plann Manag. 2016;31:167–74. https://doi.org/10.1002/hpm.2290.
Harris D, Wales J, Jones H, Rana T, Chitrakar LR. Human resources for health in Nepal. In: The politics of access in remote areas. London: Overseas Development Institute; 2013.
Federal Ministry for Economic Cooperation and Development. Making local health services accountable: social auditing in Nepal’s health sector. Germany: GIZ (Deutsche Gesellschaft für Internationale Zusammenarbeit); 2015.
Commission for the Investigation of Abuse of Authority. 28th CIAA Annual Report. Kathmandu: CIAA; 2018.
Mafuta EM, De Cock BT, Lolobi DL, Mayala PM, Mambu TNM, Kayembe PK, et al. Factors influencing the capacity of women to voice their concerns about maternal health services in the Muanda and Bolenge Health Zones, Democratic Republic of the Congo: a multi-method study. BMC Health Serv Res. 2018;18:37. https://doi.org/10.1186/s12913-018-2842-2.
International Telecommunications Union (ITU). Percentage of individuals using the internet: Country ICT Data; 2018. https://www.itu.int/en/ITU-D/Statistics/Pages/stat/default.aspx. Accessed 16 Feb 2019.
Hulton L, Matthews Z, Martin-Hilber A, Adanu R, Ferla C, Getachew A, et al. Using evidence to drive action: A “revolution in accountability” to implement quality care for better maternal and newborn health in Africa. Int J Gynecol Obstet. 2014;127:96–101. https://doi.org/10.1016/j.ijgo.2014.07.002.
Acknowledgments
We acknowledge the guidance and supervision of Anke van der Kwaak.
Funding
No fund was available for this review.
Author information
Authors and Affiliations
Contributions
AN, SKD and AvdK all contributed to the concept of the study. All the authors agreed for the study methodology, conceptual framework and search strategy. AN and SKD searched and collected the literature and relevant reports. AN and SKD critically analysed the findings and drafted the manuscript. Critical revision of the manuscript for intellectual content was done by AvdK and SKD. All the authors were equally involved in drafting, revising, and finalizing the manuscript. The authors read and agreed for the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Appendix 1.
Search strategy
Additional file 2: Appendix 2.
References details
Additional file 3: Appendix 3.
Flow diagram of MPDR and MPDSR [23]
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Nepal, A., Dangol, S.K. & van der Kwaak, A. Improving maternal health services through social accountability interventions in Nepal: an analytical review of existing literature. Public Health Rev 41, 31 (2020). https://doi.org/10.1186/s40985-020-00147-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40985-020-00147-0