
Abstract
Background
Housing is a social determinant of health. Extensive research has highlighted its adverse effects on health. However, less is known about the effects of cohousing typology on health, which has the potential to create lively social networks and healthy communities and environments. We report the findings of a scoping study designed to gather and synthesise all known evidence on the relationship between cohousing and wellbeing and health.
Method
Using the scoping review method, we conducted a literature review in PubMed, ProQuest, Scopus, Web of Science, Science Direct and JSTOR in May 2019 and selected articles published from 1960 onwards, with no geographical limit and no design restrictions. Retrieved articles underwent three sequential screening phases. The results were described through a narrative synthesis of the evidence.
Results
Of the 2560 articles identified, we selected 25 full-text articles analysing 77 experiences. All of them were conducted in high-income countries. Ten studies analysed the impact of cohousing on physical and mental health or quality of life and wellbeing. Eight of the 10 studies found a positive association. In addition, 22 studies analysed one or more psychosocial determinants of health (such as social support, sense of community and physical, emotional and economic security) and most found a positive association. Through these determinants, quality of life, wellbeing and health could be improved. However, the quality of the evidence was low.
Discussion
The cohousing model could enhance health and wellbeing mediated by psychosocial determinants of health. However, extreme caution should be exercised in drawing any conclusions due to the dearth of data identified and the designs used in the included studies, with most being cross-sectional or qualitative studies, which precluded causal-based interpretations. Because housing is a major social determinant of health, more evidence is needed on the impact of this model on health through both psychosocial and material pathways.
Similar content being viewed by others


Background
Housing is widely recognised as a social determinant of health [1, 2]. Health outcomes are affected by housing affordability, stability, quality and the emotional link to housing, along with the physical and social characteristics of neighbourhoods [3, 4]. While the evidence for the adverse effects of housing on physical and mental health has been reviewed [2, 3, 5, 6], there has been little assessment of the beneficial health effects of housing arrangements where people intentionally live together in a community. Evidence suggests that communal living arrangements reduce feelings of loneliness and increase perceived wellbeing among the senior population compared with residents living in single arrangements [7, 8].
Among communal living arrangements, here we review the cohousing model. The existing literature on cohousing is characterised by a certain degree of ambiguity and overlap between different terms and experiences. However, there is consensus among different authors in defining cohousing as a form of community living that contains a mix of private and communal spaces with substantial self-managed common facilities and activities aimed at everyday living [9,10,11].
To date, the evidence suggests that cohousing decreases isolation in seniors, positively impacts inhabitants’ quality of life and benefits physical and mental health [12, 13]. Among intergenerational housing residents, cohousing also increased mutual support and created a sense of community among residents [14,15,16]. These feelings could be extended to the neighbourhood by increasing the sense of community beyond the boundaries of cohousing, resulting in improved wellbeing among residents [17]. However, there are fewer studies on the physical and mental health effects in intergenerational populations, and the results appear unclear.
The cohousing model was created in Denmark in the early 1970s as an innovative form of collective housing and later spread to other northern European countries, the USA [18] and other latitudes such as Uruguay [19]. In recent years, cohousing has re-emerged in the USA, Europe, Australia, New Zealand and Japan [16, 20, 21]. This re-emergence has been associated with a growing desire for a sense of belonging, to experience more connection with the community and an increasing rejection of dominant consumption patterns [22]. In addition, it has been boosted by the lack of affordable housing and poor rental conditions and has been presented as a potential alternative to conventional tenure arrangements [16, 18, 23]. Research on the cohousing model has so far covered different topics. For example, the architectural features and physical layout of buildings [15, 24, 25], the environmental sustainability practices in communities [26,27,28,29] and self-management and decision processes [30]. Few studies, however, have explored the different tenure modalities [23, 31], their ability to promote social capital [16] and whether social housing could be an opportunity for municipalities to promote socially inclusive urban development [32].
The cohousing model has also attracted the attention of public health [33]. The driving motivation is to provide evidence of the increased quality of life among people living in cohousing, which is often an objective of cohousing projects but is rarely assessed, to facilitate evidence-based decision-making. From the point of view of health promotion, the expansion of this model is related to the need to respond to the phenomenon of social isolation through community-based housing models that promote healthy built environments and foster people’s social cohesion [33]. Furthermore, the cohousing model is credited with the ability to improve the affordability of housing [18], which is known to be beneficial to the wellbeing of the population.
Although there is only a modest number of studies on cohousing and health, wellbeing, or quality of life, research in this field is slowly increasing. The present review aims to gather and synthesise all the known evidence on the relationship between cohousing and health and wellbeing.
Methods
We conducted a literature review using the scoping review method. This method has an exploratory character and is indicated to synthesise the scientific knowledge and identify the key concepts and research gaps in areas of study with little available scientific evidence [34]. The literature search was performed in May 2019, and we consulted databases in social sciences, architecture and health: PubMed, ProQuest, Scopus, Web of Science, Science Direct and JSTOR. Full details of the search strings used for the various databases are shown in Supplementary 1. Note that to capture articles related to cohousing and health, the search syntax was adapted to each database.
The inclusion criteria were peer-reviewed documents: (1) studies of cohousing living arrangements where communal spaces and/or common facilities or services are available and self-managed; (2) documents published after 1960, as the cohousing model started in Denmark in the 1960s; (3) documents that analysed at least one health outcome such as physical or mental health, self-perceived health, or wellbeing, or assessed psychosocial determinants of health, such as social support, social isolation, life satisfaction, happiness, or sense of community; and (4) documents written in English, Spanish, French, German or Italian. We excluded books and conference communications and studies without an available summary.
We applied three sequential phases of document screening to the list of documents retrieved by the searches. In phases 1 and 2, we screened the documents by title/abstract and full text, respectively. In phase 3, we manually retrieved additional documents that also met the inclusion criteria from the reference lists of the documents selected, as well as the literature identified after expert consultation and repeated the same screening procedure. Details of the experts contacted are shown in Supplementary 2. To ensure internal validity, we triangulated the results as follows: phases 1 and 2 were carried out separately by three independent pairs of researchers, who discussed the inclusion/exclusion of the documents that generated doubts. A third researcher was included if there were still doubts. For the articles retrieved in phase 3, we replicated the same selection and triangulation process, but only one pair of researchers participated.
For each selected document, we extracted the following information: (a) characteristics of the studies, (b) characteristics of cohousing projects studied and (c) health-related outcomes. The included characteristics of the studies were year of publication, type of methods and number of projects studied. The characteristics of cohousing projects were year of cohousing project creation, country of cohousing project, age target and co-ownership tenure. The health-related outcomes analysed were grouped in (i) self-perceived physical and mental health, (ii) quality of life and wellbeing and (iii) psychosocial determinants of health, which include social support, social isolation, sense of community and sense of security and safety.
Finally, we provide an in-depth description of the main health-related findings of cohousing projects studied.
Results
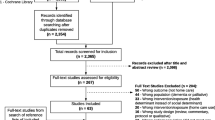
The search and selection process and the documents included are summarised in Fig. 1. The search resulted in a total of 2983 documents: 516 in PubMed, 31 in ProQuest, 913 in Scopus, 922 in the Web of Science, 93 in Science Direct and 508 in JSTOR. Of these, 269 were duplicates. In all, 2291 documents were excluded after reviewing the title and abstract. After reading the full text of the remaining 137 documents, 24 were included. We reviewed the references from these documents, and we contacted experts by e-mail. Eight experts offered information or referred us to other experts or specialised organisations. As a result, 41 new documents were retrieved, and 1 was selected for the review. A total of 25 documents were finally included in the scoping review.

Flowchart of the search and selection procedure of documents
Table 1 shows the main characteristics of the documents selected. The publication rate tended to increase over time, with 24% of the documents published between 2001 and 2010, and 64% of documents published after 2010. Regarding the study designs, 20% were quantitative studies, all were cross-sectional and two of them had a comparison group. A total of 40% were qualitative studies, and the most commonly used techniques were in-depth interviews (n = 6) and semi-structured interviews (n = 4), while four studies applied more than one technique. Mixed methods were employed by 40% of the studies. Three of them used longitudinal designs. Two studies used a comparison group in the quantitative approach, while in-depth interview was the most commonly applied technique in the qualitative approach.
The proportion of articles examining between two and five cohousing living arrangements projects per document was high (44%). The 25 studies examined a total of 77 projects. A quarter (25%) of the cohousing projects studied were created before 1990, 22% between 1990 and 2000, 39% between 2001 and 2010 and only 5% after 2010. Most projects (53%) were conducted in European countries, with the vast majority being conducted in northern countries, followed by the USA (23%) and Canada (23%). Cohousing projects target predominantly the intergenerational population (62%), and tenure was co-ownership (35%).
Regarding health outcomes, four studies analysed physical and mental health through self-perceived assessment, and one of them measured healthcare requirements. Six studies analysed quality of life and wellbeing. Twenty-two selected studies included the psychosocial determinants of health. Finally, beneficial effects of cohousing on health outcomes were reported in three studies analysing physical and mental health, in five analysing quality of life and wellbeing and in twenty assessing psychosocial determinants of health.
Cohousing-related health effects
Table 2 describes the health outcomes and the psychosocial determinants of health of the cohousing projects studied, and Table 3 summarises their observed effects.
Self-perceived physical and mental health
Four studies aimed to assess the impact of cohousing on self-perceived physical and mental health. Two of them used mixed methods [35, 36], one used quantitative method [37] and the other applied a qualitative design [38]. The former did not provide the guide used in the interviews. The three studies employing survey-based quantitative approaches used a validated question—self-perceived health—and no other scales. Mental health was assessed one-dimensionally, with no scales measuring more than one mental health domain.
Self-perceived physical and mental health in two senior projects increased in the follow-up [35, 36], while in the intergenerational projects the effect on health was less clear. No significant differences were observed in self-perceived physical health in the single article that used a comparison group, although cohousing residents reported less need for health and social care services [37]. In contrast, a project for low-income middle-aged women found that residents reported a deterioration in their physical and mental health after they moved to the cohousing cooperative [38].
Quality of life and wellbeing
All but one study assessing quality of life and wellbeing reported positive benefits for cohousing residents, two using qualitative methods [39,40,41], one mixed method [42] and another one quantitative method [43]. The single study that did not report significant benefits used a quantitative method with a comparison group [44]. The latter compared cohousing residents who were owners with residents in congregated apartments who were tenants. Only one study using a qualitative approach provided information on the interview guide used [39]. Two of the studies employing quantitative approaches provided information on the questions used to assess quality of life [43, 44]; none of the studies used the same scale.
The studies that found improvements in quality of life and wellbeing explained these gains by increased autonomy, increased opportunities to participate in the community and greater solidarity among cohousing residents, in both senior [39,40,41] and intergenerational [42, 43] projects. One of these intergenerational projects was based on Canadian non-profit cohousing cooperatives for people with functional diversity [42]. In this case, improvements in the quality of life of the residents were more related to the ability to decide how to live individually and socially than to the ability to control the physical environment.
Psychosocial determinants of health
Social support
Social support was assessed through seven studies using a mixed methods design [12, 35, 45,46,47,48,49], including two with a comparison group [14, 50], nine qualitative methods [15, 16, 38,39,40,41, 51,52,53] and four quantitative methods [13, 37, 43, 54]. Two studies with a comparison group [14, 37] and three studies that compared the actual situation with previous situation [43, 46, 48] reported that social support was more evident in the cohousing model. In addition, the residents’ social networks were strengthened after they moved into cohousing [45].
Most studies reported that the cohousing model had beneficial effects on the residents’ social support. This effect could be found both in senior [12, 13, 35, 39, 41, 45, 47,48,49,50, 52, 54] and intergenerational projects [14,15,16, 37, 40, 43, 46, 53, 54]. One study found beneficial effects of social support among same-generation residents while intergenerational social support was less evident [51].
Three studies indicated less obvious effects. One studied a project targeting low-income women in which social support was not an immediate effect due to the diversity of the residents, although over time it seemed to be able to increase [38]. Other found no significant differences in the increase in social support comparing the perception of cohousing residents with the perception of residents in rental apartments with social activities. However, socialisation patterns were more open and autonomous among cohousing residents [52]. The third states that intergenerational solidarity was not evident [51].
Among studies reporting a beneficial effect on social support, three types of social support can be described: (a) instrumental (or functional) social support involving activities such as borrowing, housework, meal preparation, care during illness or childcare [12,13,14, 45, 47, 53]; (b) emotional support such as having close friendships, listening or providing support when someone had a personal problem [13, 35, 47]; and (c) recreational support, provided through different social activities organised by residents themselves [15, 50, 54].
Social isolation
The five studies assessing social isolation reported less loneliness among cohousing inhabitants using quantitative [13], mixed [48, 50] and qualitative methods [38, 52]. None incorporated a comparison group in the analysis. The four studies targeting the senior population reported that an active lifestyle in settings prevented social isolation and loneliness, which is a general problem among senior residents. Social interaction was enhanced by the architectural design of both indoor and outdoor common spaces, which was also described as an effective way to reduce social isolation [38, 48], in particular among elderly residents who were sick and frail [50]. However, it was not always experienced beneficially since privacy was valued as something that mattered [52].
Sense of community
Evidence was obtained through one study with quantitative methods [13], 6 using mixed methods [12, 14, 35, 47, 50, 55], including only one with a comparison group [14], and four qualitative designs [16, 38, 52, 53].
Several studies showed a beneficial influence of the cohousing model on the residents’ sense of community, both in senior [12, 13, 35, 47, 50, 52] and intergenerational projects [16, 53]. In contrast, one study about a project for low-income women showed detrimental effects on residents’ perception of sense of community. Moreover, another study reported contradictory effects. Living in cohousing increased the sense of community but could also be a source of struggle and fatigue to maintain it [14].
The studies reporting beneficial effects uncovered some sense of community-building pathways. For example, two studies reported that individuals intentionally chose the cohousing model in search of a sense of community [35, 50, 53]. In addition, they outlined the relevance of the residents’ engagement pathway throughout all stages of the cohousing development process as a critical source of community building, such as participation in the start-up stages in co-ownership projects [12, 16], self-management of common spaces and facilities [16] and the day-to-day community and mutual support [12, 47, 50, 55].
Sense of security
Nine studies examined the impact of cohousing on the sense of security [13, 16, 38, 45,46,47,48,49, 53]. All of them reported a positive association. The evidence was obtained from five studies using mixed methods [45,46,47,48,49], 3 qualitative studies [16, 38, 53] and one study using quantitative methods [13].
The sense of security gained was found among both senior [13, 45, 47, 48] and intergenerational projects [16, 38, 40, 46, 53]. The studies found that cohousing increased residents’ sense of security through both the physical and the social environment. In addition, it reduced residents’ sense of economic insecurity [38]. The physical aspects emphasised were open and well-lit spaces [16], safe children’s play areas [53] and a neighbourhood with a rich and pleasant atmosphere [38]. The social features that led to feelings of security were social relationships and trust [47], community coping [48] and social support among neighbours [13, 47, 48]. An economic sense of security among low-income women residents reduced stress, helplessness and frustration [38].
Discussion
Main findings
The purpose of this study was to examine all the known evidence on the relationship between communal living arrangements characterised as cohousing and health and wellbeing. Our review indicates that the cohousing model can be positively associated with health outcomes through psychosocial determinants of health, such as increased social support, sense of community and physical, emotional and economic security, as well as reduced social isolation. This association was more evident in cohousing models targeting the older population. Likewise, we found a limited number of studies assessing the direct health effects of the cohousing model. Some studies suggest that cohousing is positively associated with self-perceived physical and mental health outcomes and quality of life and wellbeing. However, extreme caution should be exercised in drawing any conclusions due to the dearth of data identified and the study designs used—mostly cross-sectional, with small samples or no comparison group—that precluded causal-based interpretations.
What health outcomes have been studied in relation to cohousing?
With respect to the effect of cohousing on health outcomes, only 10 studies analysed the effect of cohousing on self-perceived health [35,36,37,38, 49] and quality of life and wellbeing [39,40,41,42,43,44].
The studies evaluating both health and quality of life showed relatively limited reproducibility and comparability. No other subjective health measures are available such as joy, happiness, sense of self-worth and value to others, or other measures related to stress and mental health. There is also a lack of evidence on other objective health measures such as the ability to perform physical, mental and social tasks or healthy behaviours. Other health measures that could be important to assess are health-related quality of life indices. For example, the EuroQoL-5 index is one of the most widely used instruments underpinning economic evaluations, which would allow quantification of quality of life and analysis of health effects in terms of the associated costs of this model compared with conventional housing arrangements.
How could cohousing affect health, quality of life and wellbeing?
The cohousing model may be positively associated with health status through psychosocial pathways underlying health and illness. These mechanisms would be coherent with the evidence found in measures such as social support [12,13,14,15,16, 35, 37, 38, 40, 41, 43, 45, 47,48,49,50,51,52,53,54], sense of community [12, 16, 35, 38, 46, 47] and sense of security [13, 16, 38, 47, 48, 53]. This finding is consistent with other studies reporting the relationship between social support and health and wellbeing. For example, lack of a social network and support, social isolation and loneliness are linked to poor cardiovascular and mental health outcomes [56]. In contrast, living in a community characterised by higher levels of communication and mobilisation is positively associated with residents’ self-rated health status [57], especially in elderly persons. In addition, it has been shown that high social support and participation in social networks alleviates stress in older people, preventing them from developing functional decline [58] and mental health problems [59]. A sense of community has also been positively related to a range of health outcomes and indicators of wellbeing, including life satisfaction and loneliness [60], happiness [61], and quality of life [62].
There is a lack of studies aiming to identify the differential health and wellbeing effects resulting from cohousing models based on co-ownership. We found only one study that comparatively assessed the effect of tenure on quality of life [44]. That study observed no additional benefits among residents living in a model based on co-ownership tenure. We found some evidence to suggest that the co-ownership regime helped to increase autonomy and a sense of control among residents, which could enhance quality of life [42]. Further research is required on the potential health and quality of life gains among the different tenure arrangements in the cohousing model.
Issues arising from the review
Over the last few years, cohousing has reappeared in various high-income countries. This has not gone unnoticed by several social sectors such as urbanists, politicians, social movements and non-profit organisations, with all of them showing a willingness to promote it. However, we cannot dismiss the possibility that the promotion of this model may increase social and health inequalities. Several studies discussed here [16, 52] have observed unequal access to cohousing projects. Populations from disadvantaged social classes would appear to have fewer opportunities to access them and thus less chance to benefit from the potential positive social and health effects. Therefore, we should not rule out the so-called paradox of promotion in public health, in which health promotion can have undesirable effects and increase health inequalities. This effect has been previously documented in a review of unintended harm in public health interventions [63]. Therefore, the unintended effects of cohousing on social and health inequalities should be considered by entities interested in promoting this model and in future research.
In this review, we found no evidence linking housing affordability and health among the cohousing experiences studied. However, there is some evidence that cohousing provides residential security as residents value living in a home at an affordable price for a long period of time [16, 38, 52]. Housing affordability is recognised as a material pathway to health, and there is substantial evidence linking housing affordability problems with a range of adverse health effects [3, 4] and health inequalities [64]. Potentially, cohousing has been considered a housing model that could help to decrease the commoditisation of housing, since it conceives housing as a social good that prioritises its use value over its exchange value. It is known that commodification of other key areas of a person’s life, such as food [65], care [66] or the health care system [67], among others, can lead to worse health. In general, in an intentional housing community, housing construction costs are often less subject to the capital gains of promoters; there is greater long-term stability of housing prices and mutual economic support that results in stable economic and social security for residents, who are less exposed to the precarious conditions of the neo-liberal housing market [18]. In this regard, there is a literature gap in relationship between cohousing and its potential effect on health at the individual and community level through socioeconomic aspects. Therefore, further research is required on the potential health gains associated with the affordability, stability, or collectivisation of economic uncertainties of cohousing living arrangements.
Limitations and strengths
There is still no consensus on the definition of cohousing models. Some authors have attempted to define it and standardise its use for international communication avoiding the use of inconsistent and vague concepts [9]. This makes the search for evidence less complex and the comparative analysis more reliable. However, most of the studies selected were published before this effort at conceptualisation. Therefore, there may be a bias in the article selection due to divergence in search terms. However, the scoping review method used in this review is more flexible than a systemic review. This enabled us to have more flexible exclusion and inclusion protocols and to include articles that would have been ruled out using other review methods. Another limitation could be bias due to the use of language restrictions. Although the present review used the English, Spanish, French, German and Italian languages, cohousing has a long history in Denmark, and Danish was not a language covered in this review. However, to overcome this limitation, we contacted experts to find relevant references. The references gained did not allow us to identify new documents studying the relationship between cohousing and health, although additional information on the cohousing model was obtained that facilitated the discussion of the results obtained.
Despite these limitations, this review provides an important contribution to public health and social policies because, to the best of our knowledge, it is the first review to gather and systematise the scientific evidence related to this housing model, aiming to assess its health and welfare effects. The review also identifies knowledge gaps and could be used to inform future research. Likewise, gathering the present evidence will facilitate the design of evidence-based policies in the cohousing domain. In addition, a strong effort has been made to search for evidence by not limiting it to articles indexed in biomedical databases. The search was also performed in social science databases, enabling us to find articles that, although they were not focused on health effects, included them among their findings.
Conclusions
This study examined the available evidence on cohousing from a public health perspective. The rationale is that housing is an important determinant of health and health inequalities, and cohousing is a potentially health-enhancing form of community living that raises many expectations for creating vivid social networks, communities and healthy environments. Various studies have provided a relatively consistent picture of the increased psychosocial health benefits of the community dimension and the emotional and social bond of this model of housing. However, more research is needed to address the knowledge gaps identified in this review. Future studies should measure health with objective and/or subjective health outcomes because most studies conducted to date have been performed in relation to psychosocial determinants of health. Furthermore, there is a need for studies with methodological approaches that provide clearer evidence of the effects of cohousing on health. Housing is a collection of components that together affect individuals’ lives. In that sense, other cohousing dimensions related to economic aspects, such as cost and stability, or environmental sustainability, their interactions and their impact on health and wellbeing, need to be explored in the future.
Availability of data and materials
Not applicable.
References
Borrell C, Malmusi D, Artazcoz L, Diez E. Rodríguez-Sanz IP y. M, Campos P, et al. Propuesta de políticas e intervenciones para reducir las desigualdades sociales en salud en España. Gac Sanit. 2012;26:182–9.
Krieger J, Higgins DL. Housing and health: time again for public health action. Am. J. Public Health. American Public Health Association; 2002. p. 758–768.
Bonnefoy X. Inadequate housing and health: an overview. Int J Environ Pollut. 2007;30:411–29.
Novoa AM, Bosch J, Díaz F, Malmusi D, Darnell M, Trilla C. Impact of the crisis on the relationship between housing and health. Policies for good practice to reduce inequalities in health related to housing conditions. Gac Sanit. SESPAS; 2014;28:44–50.
Gibson M, Petticrew M, Bambra C, Sowden AJ, Wright KE, Whitehead M. Housing and health inequalities: a synthesis of systematic reviews of interventions aimed at different pathways linking housing and health. Health Place. Pergamon. 2011;17:175–84.
Ormandy D, Ezratty V. Health and thermal comfort: from WHO guidance to housing strategies. Energy Policy. Copenhagen. Denmark. 2012;49:116–21.
Cramm JM, Nieboer AP. Building social capital may protect against loss of well-being among older people. Soc Cap as a Heal Resour Later Life Relev Context. 2015. p. 145–54.
Norstrand JA, Glicksman A. Influence of living arrangements of community dwelling older adults on the association between social capital and health. Soc Cap as a Heal Resour Later Life Relev Context. 2015. p. 89–107.
Vestbro. Concepts and terminology. Living together – cohousing ideas and realities around the world. Stockholm; 2010.
Vestbro DU. From collective housing to cohousing - a summary of research; 2000.
Vestbro DU, Horelli L. Design for gender equality: the history of co-housing ideas and realities. Built Environ. 2012;38:315–35.
Glass AP. Lessons learned from a new elder cohousing community; 2013.
Glass AP. Resident-managed elder intentional neighborhoods: do they promote social resources for older adults? J Gerontol Soc Work; 2016.
Markle EA, Rodgers R, Sanchez W, Ballou M. Social support in the cohousing model of community: a mixed-methods analysis. Community Dev. 2015;46(5):616–31.
Williams J. Designing neighbourhoods for social interaction: The case of cohousing; 2005.
Ruiu ML. The effects of cohousing on the social housing system: the case of the Threshold Centre; 2015.
Sanguinetti A. Transformational practices in cohousing: enhancing residents’ connection to community and nature. J Environ Psychol. 2014;40:86–96.
Hagbert P, Larsen HG, Thörn H, Wasshede C, Larsen HG, Thörn H, et al. Contemporary co-housing in Europe. First. Hagbert P, Larsen HG, Thörn H, Wasshede C, editors. Contemp. Co-housing Eur. Milton Park, Abingdon, Oxon ; New York, NY : Routledge, 2020.: Routledge; 2019.
Bredenoord J. Self-managed cooperative housing by mutual-assistance as introduced in Central America between 2004 and 2016 the attractiveness of the ‘FUCVAM’ model of Uruguay. J Archit Eng Technol. 2017;06:1–9.
Lang R, Carriou C, Czischke D. Collaborative housing research (1990–2017): a systematic review and thematic analysis of the field; 2018.
Tummers L. Understanding co-housing from a planning perspective: why and how? Urban Res Pract. Routledge. 2015;8:64–78.
Jarvis H. Sharing, togetherness and intentional degrowth. Prog Hum Geogr. SAGE Publications Ltd. 2019;43:256–75.
Larsen HG. Three phases of Danish cohousing: tenure and the development of an alternative housing form; 2019.
Marcus CC. Site planning, building design and a sense of community: an analysis of six cohousing schemes in Denmark, Sweden, and the Netherlands. J Archit Plann Res. 2000;17:146–63.
Sanguinetti A. The design of intentional communities: a recycled perspective on sustainable neighborhoods. Behav Soc Issues. 2012;21:5–25.
Bamford G. Bringing us home: cohousing and the environmental possibilities of reuniting people with neighbourhoods. Situating Environ Univ Queensl Situating Environ. 2001;2001:36–43.
Brown JR. Comparative analysis of energy consumption trends in cohousing and alternate housing arrangements. Dep Civ Environ Eng. 2004.
Williams J. Predicting an American future for cohousing. Futures. 2008;40:268–86.
Chatterton P. Towards an agenda for post-carbon cities: lessons from lilac, the uk’s first ecological, affordable cohousing community. Int J Urban Reg Res. 2013;37:1654–74.
Renz MA. Paving consensus: enacting, challenging, and revising the consensus process in a cohousing community; 2006.
Jakobsen P, Larsen HG. An alternative for whom? The evolution and socio-economy of Danish cohousing. Urban Res Pract. Routledge. 2019;12:414–30.
Droste C. German co-housing: an opportunity for municipalities to foster socially inclusive urban development? Urban Res Pract. Routledge. 2015;8:79–92.
Lubik A, Kosatsky T. Public health should promote co-operative housing and cohousing. Can J Public Heal. Canadian Journal of Public Health. 2019;110:121–6.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract. 2005;8:19–32.
Glass AP. Aging in a community of mutual support: the emergence of an elder intentional cohousing community in the United States; 2009.
Glass AP. Elder co-housing in the United States: three case studies. Built Environ. 2012;38:345–63.
Kehl K, Then V. Community and civil society returns of multi-generation cohousing in Germany; 2013.
Wasylishyn C, Johnson JL. Living in a housing co-operative for low income women: Issues of identity, environment and control. Soc Sci Med. 1998;47:973–81.
Nusbaum LE. How the elder co-housing model of living affects residents’ experience of autonomy: a self -determination theory perspective. ProQuest Diss Theses. Ann Arbor: The Wright Institute; 2010;77.
Labit A. Self-managed co-housing in the context of an ageing population in Europe. Urban Res Pract. 2015;8:32–45.
Rodríguez-Alonso N. Argemir DC. La construcción social del cuidado comunitario en La Muralleta, una cooperativa autogestionada para gente mayor. 2017;22:183–98.
Cooper M, Rodman MC. Accessibility and quality of life in housing cooperatives. Environ Behav. 1994;26:49–70.
Choi JS, Paulsson JAN. Evaluation of common activity and life in Swedish cohousing units. Int J Hum Ecol. 2011;12:133–46.
Altus DE, Mathews RM. Comparing the satisfaction of rural seniors with housing co-ops and congregate apartments: Is home ownership important? 2002.
Pedersen M. Senior co-housing communities in Denmark; 2015.
Fromm D. American cohousing: the first five years. J Archit Plann Res. 2000;17:94–109.
Jolanki O, Vilkko A. The meaning of a “sense of community” in a Finnish senior co-housing community. J Hous Elderly. 2015;29:111–25.
Glass AP, Vander Plaats RS. A conceptual model for aging better together intentionally. J Aging Stud. 2013;27:428–42.
Bamford G. Living together on one’s own’: cohousing for older people, a new housing type in Denmark and The Netherlands. Australas J Ageing. 2005;24:44–6.
Tyvimaa T. Social and physical environments in senior communities: The Finnish experience; 2011.
Labit A, Dubost N. Housing and ageing in France and Germany: the intergenerational solution. Housing, Care Support. 2016;19:45–54.
Motevasel IN. Senior housing in Sweden - a question of class differences and collective aging: an interview study in rental apartments and housing cooperatives; 2006.
Tchoukaleyska R. Co-housing childhoods: parents’ mediation of urban risk through participation in intentional communities; 2011.
Philippsen C. Fazit. Soz Netzwerke gemeinschaftlichen Wohnprojekten. 1st ed. Verlag Barbara Budrich; 2014. p. 233–268.
Meltzer G. Cohousing: verifying the importance of community in the application of environmentalism. J Archit Plann Res. 2000;17:110–32.
Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. Elsevier B.V.; 2017;152:157–71.
Jung M, Viswanath K. Does community capacity influence self-rated health? Multilevel contextual effects in Seoul. Korea. Soc Sci Med. 2013;77:60–9.
Unger JB, Johnson CA, Marks G. Functional decline in the elderly: evidence for direct and stress- buffering protective effects of social interactions and physical activity. Ann Behav Med. Springer New York LLC. 1997;19:152–60.
Kawachi I. Social ties and mental health. J Urban Heal Bull New York Acad Med. Springer. 2001;78:458–67.
Prezza M, Amici M, Roberti T, Tedeschi G. Sense of community referred to the whole town: its relations with neighboring, loneliness, life satisfaction, and area of residence. J Community Psychol. John Wiley & Sons, Ltd; 2001;29:29–52.
Davidson WB, Cotter PR. The relationship between sense of community and subjective well-being: a first look. J Community Psychol. John Wiley & Sons. Ltd. 1991;19:246–53.
Young AF, Russell A, Powers JR. The sense of belonging to a neighbourhood: can it be measured and is it related to health and well being in older women? Soc Sci Med. Pergamon. 2004;59:2627–37.
Allen-Scott LK, Hatfield JM, McIntyre L. A scoping review of unintended harm associated with public health interventions: towards a typology and an understanding of underlying factors. Int. J. Public Health. Birkhauser Verlag AG; 2014. p. 3–14.
Marí-Dell’Olmo M, Novoa AM, Camprubí L, Peralta A, Vásquez-Vera H, Bosch J, et al. Housing policies and health inequalities. Int J Heal Serv. 2017;47:207–32.
O’Kane G. What is the real cost of our food? Implications for the environment, society and public health nutrition. Public Health Nutr. Cambridge University Press. 2012;15:268–76.
Lietaert M. Cohousing’s relevance to degrowth theories. J Clean Prod. 2010;18:576–80.
Churchill LR. The United States health care system under managed care: how the commodification of health care distorts ethics and threatens equity. Heal. Care Anal. Springer; 1999. p. 393–411.
Acknowledgements
Not applicable.
Funding
The study is part of the Project “Impacto en salud y bienestar de la vivienda cooperativa en cesión de uso”, which received a research grant from the Carlos III Institute of Health, Ministry of Economy and Competitiveness (Spain), awarded on the 2018 call under the Health Strategy Action 2013-2016, within the National Research Program oriented to Societal Challenges, within the Technical, Scientific and Innovation Research National Plan 2013-2016, with reference PI18/01761, co-funded with European Union ERDF funds (European Regional Development Fund)”
Author information
Authors and Affiliations
Contributions
Study conception, planning, analysis, interpretation, and writing: JC and AR. Study conception, insights for the analysis, and interpretation and writing: AR, LO, AF, AP, AN, KP and CB. All authors have read and approved the revised version of this paper. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1.
Supplementary 1: Subject headings, keywords and search syntaxes. Supplementary 2: List of experts and organizations contacted
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Carrere, J., Reyes, A., Oliveras, L. et al. The effects of cohousing model on people’s health and wellbeing: a scoping review. Public Health Rev 41, 22 (2020). https://doi.org/10.1186/s40985-020-00138-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40985-020-00138-1