
Abstract
Background
Although chlorhexidine allergy has been shown to be mediated by immunoglobulin (Ig) E, few reports investigated the mechanism of chlorhexidine-induced anaphylaxis using basophil activation tests (BATs).
Case presentation
A 79-year-old man underwent cholecystectomy under general anesthesia. Anaphylaxis was diagnosed based on the clinical symptoms and high serum tryptase and histamine levels. Skin tests showed positive results only for chlorhexidine. Subsequently, BATs demonstrated that the causative agent was likely chlorhexidine. The inhibitory effect of wortmannin, an inhibitor of phosphoinositide 3-kinase, on basophil activation suggested an IgE-dependent mechanism underlying chlorhexidine-induced anaphylaxis.
An 89-year-old man underwent inguinal hernioplasty under general anesthesia. Anaphylaxis was diagnosed based on the clinical symptoms and high serum tryptase and histamine levels. Skin tests and BATs with wortmannin were performed, showing similar results to case 1.
Conclusions
BATs suggested an IgE-dependent mechanism for chlorhexidine-induced anaphylaxis and might be useful for investigating the mechanisms underlying drug-induced anaphylaxis.
Similar content being viewed by others


Background
Chlorhexidine is an antiseptic with a broad spectrum of activity and persistent effects on the skin. Since the widespread use of chlorhexidine, many cases of anaphylaxis have been reported [1]. The risk of chlorhexidine allergy has increasingly been recognized in recent years [2]. Chlorhexidine was the third-most common cause of perioperative anaphylaxis after antibiotics and neuromuscular blocking agents [3]. The mechanisms underlying anaphylactic reactions to chlorhexidine have been investigated, and chlorhexidine allergy has been shown to be mediated by immunoglobulin (Ig) E [4]. To the best of our knowledge, this is the first report suggesting an IgE-dependent mechanism, as indicated by basophil activation tests (BATs).
Case presentation
Case 1
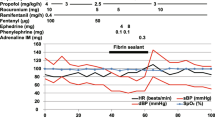
A 79-year-old man (weight, 73 kg; height, 161 cm) underwent cholecystectomy under general anesthesia. Anesthesia was induced with propofol, rocuronium, fentanyl, and inhalation of sevoflurane. Anesthesia was maintained with sevoflurane and remifentanil. He was given sulbactam and cefoperazone, and his skin was previously disinfected with chlorhexidine 1% (Hexak®; Yoshida Pharmaceutical Company, Tokyo, Japan). During surgery, frequent administrations of ephedrine and phenylephrine were required intraoperatively. Postoperatively, cutaneous wheals were observed, mainly over the abdomen. On suspicion of anaphylaxis, we administered 100 mg of hydrocortisone intravenously and 0.7 mg of adrenaline intramuscularly, stabilizing his general condition. He was transferred to the intensive care unit without extubation, and his trachea was extubated the next day. Serum tryptase levels measured at 30 min, 2 h, and 24 h after the reaction was identified were 9.6 μg/L, 10.0 μg/L, and 3.1 μg/L, respectively. Serum histamine levels measured at the same time points were 3.93 ng/L, 1.07 ng/L, and 1.27 ng/L, respectively. We diagnosed anaphylaxis based on the clinical symptoms and high serum tryptase and histamine levels.
Eighty-three days later, skin tests were performed with all suspected agents, showing positive results only for chlorhexidine (Hexak®) (Table 1). BATs with CD203c and CD63 (Beckman Coulter, Brea, USA) were subsequently performed using serial dilutions of chlorhexidine (Hexak® and Stericlon®; KENEI Pharmaceutical Company, Osaka, Japan). Hexak® contains alcohol, but Stericlon® does not. The methods of the BATs are detailed elsewhere [5]. Briefly, the basophils were incubated at 37 °C for 15 min with antibodies and drugs. Anti-IgE antibody (Beckman Coulter) and formyl-methionine-leucyl-phenylamine (fMLP; Sigma-Aldrich, St. Louis, USA) were used as positive controls. The isotype of the anti-IgE antibody is IgG1, and the host species is a mouse. Unlike anti-IgE, fMLP activates basophils through an IgE-independent pathway [5, 6]. Wortmannin (Abcam, Cambridge, UK), an inhibitor of phosphoinositide 3-kinase (PI3-K), was used to investigate whether anaphylaxis was caused by an IgE-dependent or -independent mechanism [7]. We added one μM wortmannin at the same time as other drugs. Compared to CD203c + basophils from a healthy control, those in the patient were significantly elevated after adding Hexak® and Stericlon® (Fig. 1). Similar results were obtained for CD63 + basophils. These results showed that the causative agent was likely chlorhexidine. The rates of CD203c + basophils that responded to negative control, anti-IgE at 10 μg/mL, and fMLP at 1.3 μg/mL stimulation were 5.0%, 22.9%, and 17.3%, and those with pretreatment wortmannin were 3.2%, 2.5%, and 7.7%, respectively. Pretreatment with wortmannin inhibited basophil activation induced by anti-IgE and chlorhexidine. However, only a relatively small change was observed when fMLP was used as a basophil stimulator. The inhibitory effect of wortmannin on basophil activation suggested an IgE-dependent mechanism underlying chlorhexidine-induced anaphylaxis (Fig. 1). In addition, the level of specific IgE to chlorhexidine was measured at 6.63 UA/mL.

Results of basophil activation tests with CD203c. A Chlorhexidine (Hexak®) induced CD203c upregulation in case 1 (filled circles), but not in a volunteer (filled triangles). Wortmannin significantly suppressed chlorhexidine-induced CD203c upregulation (filled rectangles). B Chlorhexidine (Stericlon®)-induced CD203c upregulation in the patient (open circles), but not in a volunteer (open triangles). C Basophil activation tests in case 2 show similar results to A. D Basophil activation tests in case 2 show similar results to B
Case 2
An 89-year-old man (weight, 47 kg; height, 160 cm) underwent inguinal hernioplasty under general anesthesia. Anesthesia was induced with propofol, rocuronium, fentanyl, and inhalation of desflurane. Anesthesia was maintained with desflurane and remifentanil. He was given sulbactam and ampicillin, and his skin had been previously disinfected with chlorhexidine 0.5% (Hexak®). Blood pressure fell to approximately 50 mmHg in the middle of the operation. Suspecting anaphylaxis, a total of 0.6 mg of adrenaline, chlorpheniramine 5 mg, and famotidine 20 mg were administered, resulting in stabilization of his general condition. Generalized erythema was observed when the surgery was concluded. Since he did not show any respiratory symptoms at the end of anesthesia, he was transferred to the high care unit after extubation. Serum tryptase levels measured at 30 min, 2 h, and 24 h after the reaction were 11.0 μg/L, 18.9 μg/L, and 4.9 μg/L, respectively. Serum histamine levels measured at the same time points were 67.1 ng/L, 2.94 ng/L, and 0.81 ng/L, respectively. Anaphylaxis was diagnosed based on the clinical symptoms and high serum tryptase and histamine levels.
Thirty-four days later, skin tests and BATs with wortmannin were performed, showing similar results to case 1 (Table 1, Fig. 1). Rates of CD203c + basophils that responded to negative control, anti-IgE 10 μg/mL, and fMLP 1.3 μg/mL stimulation were 5.0%, 68.9%, and 59.1%, and those with wortmannin were 3.6%, 3.8%, and 58.6%, respectively. In addition, the level of specific IgE to chlorhexidine was 1.45 UA/mL.
Discussion
We report two cases of chlorhexidine-induced anaphylaxis diagnosed by skin tests, BATs, and specific IgE quantification. BATs suggested an IgE-dependent mechanism for chlorhexidine-induced anaphylaxis.
Correct diagnosis is crucial in perioperative anaphylaxis, and skin tests remain the gold standard for detecting culprit drugs. However, skin tests carry a risk of inducing a recurrence of anaphylaxis, and the positive predictive value of skin tests is not 100%. Hence, there seems to be room for other in vitro tests to diagnose anaphylaxis [9]. The following in vitro tests are available to assess the diagnosis of chlorhexidine allergy: detection of specific IgE, histamine release test, and BATs. Although many patients have undergone quantification of specific IgE, few patients with chlorhexidine-induced anaphylaxis have undergone BATs [1]. We performed BATs in addition to specific IgE in our cases, with positive results in both. The positive reaction on BATs by chlorhexidine preparations with or without alcohol suggested that chlorhexidine itself is an allergen.
In recent years, BATs with wortmannin have become available to investigate the involvement of IgE. As PI3-K is an essential enzyme in the IgE-mediated pathway of basophil activation, suppression of basophil activation by wortmannin suggests IgE involvement [7, 10]. In the current cases, wortmannin almost completely suppressed basophil activation by chlorhexidine, suggesting an IgE-dependent mechanism of chlorhexidine-induced basophil activation.
Conclusions
BATs suggested an IgE-dependent mechanism for chlorhexidine-induced anaphylaxis. BATs might be useful for investigating the mechanisms underlying drug-induced anaphylaxis.
Availability of data and materials
Data relevant to this case report are not available for public access because of patient privacy concerns, but are available from the corresponding author on reasonable request.
Abbreviations
- BATs:
-
Basophil activation tests
- IgE:
-
Immunoglobulin-E
- PI3-K:
-
Phosphoinositide 3-kinase
- fMLP:
-
Formyl-methionine-leucyl-phenylamine
References
Fernandes M, Lourenco T, Lopes A, Spinola Santos A, Pereira Santos MC, Pereira BM. Chlorhexidine: a hidden life-threatening allergen. Asia Pac Allergy. 2019;9(4):e29.
Garvey LH, Hunter JM. Changing culprits in perioperative anaphylaxis. Br J Anaesth. 2018;121(1):114–7.
Harper NJN, Cook TM, Garcez T, Farmer L, Floss K, Marinho S, et al. Anaesthesia, surgery, and life-threatening allergic reactions: epidemiology and clinical features of perioperative anaphylaxis in the 6th National Audit Project (NAP6). Br J Anaesth. 2018;121(1):159–71.
Garvey LH, Kroigaard M, Poulsen LK, Skov PS, Mosbech H, Venemalm L, et al. IgE-mediated allergy to chlorhexidine. J Allergy Clin Immunol. 2007;120(2):409–15.
Horiuchi T, Yokohama A, Orihara M, Tomita Y, Tomioka A, Yoshida N, et al. Usefulness of basophil activation tests for diagnosis of sugammadex-induced anaphylaxis. Anesth Analg. 2018;126(5):1509–16.
Miura K, Lavens-Phillips S, MacGlashan DW Jr. Localizing a control region in the pathway to leukotriene C(4) secretion following stimulation of human basophils with anti-IgE antibody. J Immunol. 2001;167(12):7027–37.
Horiuchi T, Takazawa T, Sakamoto S, Orihara M, Yokohama A, Uchiyama M, et al. Possible immunoglobulin-E-dependent sugammadex-induced anaphylaxis caused by an epitope other than γ-cyclodextrin: a case report. Journal of Medical Case Reports. 2021;15(1):1–4.
Mertes PM, Malinovsky JM, Jouffroy L. Working Group of the S, Sfa, Aberer W, et al. Reducing the risk of anaphylaxis during anesthesia: 2011 updated guidelines for clinical practice. J Investig Allergol Clin Immunol. 2011;21(6):442–53.
Takazawa T, Sabato V, Ebo DG. In vitro diagnostic tests for perioperative hypersensitivity, a narrative review: potential, limitations, and perspectives. Br J Anaesth. 2019;123(1):e117–25.
Aranda A, Mayorga C, Ariza A, Dona I, Rosado A, Blanca-Lopez N, et al. In vitro evaluation of IgE-mediated hypersensitivity reactions to quinolones. Allergy. 2011;66(2):247–54.
Acknowledgements
Not applicable.
Funding
The preparation of this manuscript was supported by the JSPS KAKENHI Grant Numbers 19K18286 and 18K08809.
Author information
Authors and Affiliations
Contributions
MO and TT wrote the manuscript. TH, KN, NM, AT, and SS revised and edited the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
We obtained the basophil activation test data in healthy volunteers according to a study protocol approved by the Ethics Committee of Gunma University Hospital (identification [ID]: 1259). The study protocol was registered with the University Hospital Medical Information Network Clinical Trials Registry (ID: UMIN000016761). Written informed consent for participation was obtained from the healthy volunteers.
Consent for publication
Written informed consent for publication was obtained from the patient using a form approved by the ethics committee of Takasaki General Medical Center and JCHO Gunma Chuo Hospital.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Orihara, M., Takazawa, T., Horiuchi, T. et al. Intraoperative chlorhexidine-induced anaphylaxis suggesting an immunoglobulin-E-dependent mechanism indicated by basophil activation tests: two case reports. JA Clin Rep 8, 91 (2022). https://doi.org/10.1186/s40981-022-00581-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40981-022-00581-w