
Abstract
Background
We measured catecholamine levels during periodic blood pressure fluctuations in patients with pheochromocytoma.
Case presentation
A 43-year-old man presented with periodic blood pressure fluctuations during surgery for a renal pelvic tumor. His blood levels of catecholamines (ng/mL) changed dramatically over a short time during blood pressure fluctuations: adrenaline 0.36 to 3.22, noradrenaline 0.47 to 1.98, and dopamine 0.02. After the diagnosis of pheochromocytoma, oral treatment with doxazosin 2 mg/day was administered, and left adrenalectomy was performed 4 months after the initial surgery. Periodic circulation fluctuations occurred after tracheal intubation at the time of anesthesia induction, but the degree of fluctuation was smaller than that of the first surgery.
Conclusions
The data suggest that the periodic blood pressure fluctuations in pheochromocytoma patients are caused by changes in blood catecholamine levels. Our data suggests that alpha blockers may also be effective against the cyclic fluctuations that occur in patients with pheochromocytoma.
Similar content being viewed by others

Introduction
Pheochromocytoma is a disease that exhibits various symptoms, such as hypertension, hypermetabolism, and hyperglycemia, due to abnormal catecholamine production by the tumor. It is well known that pheochromocytoma causes transient abnormal hypertension due to physical pressure on the tumor; however, there are few reports to date of periodic blood pressure fluctuations [1]. The cause of these fluctuations remains unknown [2, 3]. Some reports have speculated that periodic changes in blood pressure occur either in the case of sympathetic reflex or central nervous system ischemic reflex. They have also shown that stabilizing circulating blood volume may be the solution to this anomaly that interrupts the circulating cycle [2]. It is still unclear whether the pathophysiology of periodic blood pressure fluctuations in patients with pheochromocytoma is associated with this sympathetic and parasympathetic reflex cycle or the central nervous system ischemic reflex [4, 5].
We report a case of pheochromocytoma with periodic abnormal circulatory fluctuations during two surgeries. We found that blood catecholamine levels fluctuated during the periodic blood pressure fluctuations. Written and informed consent has been obtained from the patient for the publication of this case report.
Case description
Our patient was a 43-year-old man with a weight of 93 kg and height of 174 cm. He had been undergoing hemodialysis for 20 years because of chronic renal failure. He had been taking cinacalcet, calcium carbonate, montelukast, loratadine, and nalfurafine before the surgery. There were no preoperative symptoms of suspected pheochromocytoma and no history of hypertension. His blood pressure was 140/82 mmHg, heart rate 76 beats/min, body temperature 36.2 °C, and normal respiratory rhythm with an O2 saturation of 96% on room air. Blood tests demonstrated BUN of 60.2 mg/dL and creatinine of 13.3 mg/dL, but coagulability, liver function, and electrolytes were normal.
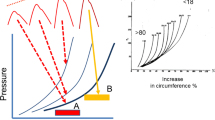
A close examination of hematuria revealed a tumor in the right renal pelvis, and retroperitoneal total right nephroureterectomy was scheduled. The tumor in the right adrenal gland was followed up because there was no clear malignant finding on CT. On the day before surgery, 5100 mL of body fluid was removed by hemodialysis. Propofol and remifentanil were used for the induction and maintenance of anesthesia. After tracheal intubation, periodic systolic blood pressure fluctuations within the range of 70–260 mmHg, diastolic blood pressure fluctuations within the range of 40–90 mmHg, and heart rate of 80–110 beats/min were observed at intervals of approximately 8 min (Fig. 1A). Intermittent and continuous administration of nicardipine was not effective for suppressing the fluctuation, which lasted for approximately 3 h and disappeared spontaneously after completion of laparoscopic surgery. Intermittent and continuous administration of nicardipine was performed because of this circulatory fluctuation; however, it could not be suppressed. Periodic blood pressure fluctuations disappeared spontaneously at the end of laparoscopic surgery. Blood samples were collected during the cycle of circulatory fluctuations. The catecholamine levels of the blood samples were as follows: [1] first blood pressure fluctuation: adrenaline 3.22 ng/mL, noradrenaline 1.98 ng/mL, and dopamine 0.02 ng/mL; [2] second blood pressure fluctuation: adrenaline 6.32 ng/mL, noradrenaline 3.12 ng/mL, and dopamine 0.02 ng/mL; and [3] at the end of blood pressure fluctuation: adrenaline 0.36 ng/mL, noradrenaline 0.47 ng/mL, and dopamine 0.02 ng/mL. A postoperative examination revealed that the highest blood catecholamine levels were adrenaline, with 0.03 ng/mL (normal value: 0–0.10 ng/mL); noradrenaline, with 0.52 ng/mL (normal value: 0.10–0.50 ng/mL); and dopamine, with 0.03 ng/mL (normal value: 0–0.03 ng/ml). In addition, scintigraphy identified an increased uptake of 131iodine-metaiodobenzylguanidine corresponding to the left adrenal gland, suggesting pheochromocytoma (Fig. 2). After the diagnosis of pheochromocytoma, oral treatment with doxazosin 2 mg/day was administered, and left adrenalectomy was performed 4 months after the initial surgery.

Anesthesia record of the first (A) and the second surgery (B). A Periodic blood pressure fluctuations occurred after tracheal intubation, lasted approximately for 150 min, and subsided at the end of laparoscopic surgery. Levels of adrenaline, noradrenaline, and dopamine were 3.22, 1.98, and 0.02 ng/ml at the point of [1], 6.32, 3.12, and 0.02 ng/ml [2] and 0.36, 0.47, and 0.02 ng/ml [3], respectively. B Periodic blood pressure fluctuations occurred after anesthesia induction, lasted approximately for 200 min, and disappeared after pheochromocytoma resection. The fluctuations were approximately 10 min apart, and the degree was smaller than that of the first surgery

Abdominal computed tomography (A) and 131I-metaiodobenzylguanidine scintigraphy images (B). A Computed tomography showed multiple renal cysts in both kidneys, left kidney atrophy, and right renal pelvis tumor (64 × 55 mm). B Scintigraphy identified an increased uptake of 131I-metaiodobenzylguanidine corresponding to the adrenal tumor
Before surgery, his blood pressure was 170/92 mmHg, heart rate 80 beats/min, body temperature 36.5 °C, and normal respiratory rhythm with an O2 saturation of 96% on room air. Blood tests demonstrated Hb of 10.4 g/dL, BUN of 46.9 mg/dL, and creatinine of 11.6 mg/dL, but coagulability, liver function, and electrolytes were normal. Echocardiography showed left ventricular hypertrophy and mild left ventricular wall hypokinesis. On the day before surgery, 4300 mL of body fluid was removed by hemodialysis. Pheochromocytoma resection was performed under general anesthesia with propofol and remifentanil. As with the initial surgery, periodic circulation fluctuations occurred after tracheal intubation at the time of anesthesia induction, but the fluctuations were approximately 10 min apart, and the degree of fluctuation was smaller than that of the first surgery. Intermittent and continuous administration of nicardipine and landiolol was performed for circulatory fluctuation; however, once again, the fluctuations could not be suppressed. Dopamine was administered to maintain circulation after tumor removal. The periodic fluctuations disappeared after the ligation of the left adrenal artery and did not occur thereafter. The intraoperative course of the second surgery is shown in Fig. 1 (Fig. 1B).
Discussion
Pheochromocytoma is a catecholamine-producing tumor, and abnormal hypertension, one of its symptoms, is generally divided into paroxysmal, persistent, and mixed types [6, 7]. There are few reports of cyclical fluctuations of blood pressure in patients with pheochromocytoma during awake condition [8] and under anesthesia [9], but no reports describe such fluctuations recurred during repeated surgeries as observed in our case. The pathophysiology of this blood pressure cyclical fluctuation is unknown; however, baroreceptors respond to a rapid rise in blood pressure during an acute attack, activating a negative feedback loop through both the sympathetic and parasympathetic nervous systems [8, 9]. A presumed result is a sharp rise and fall in blood pressure. We found that blood catecholamine levels fluctuated significantly according to blood pressure fluctuation, and it decreased when the blood fluctuation disappeared. Furthermore, the blood pressure fluctuation disappeared after removal of the tumor, suggesting that circulation fluctuation was caused by catecholamine released by the pheochromocytoma.
Wave-like patterns of blood pressure changes can be produced in laboratory animals under certain conditions and are called Mayer waves. This is likely due to reflex mechanisms involving either chemoreceptors or baroreceptors [4]. These physiological reflexes may be accentuated in pheochromocytoma. It is not known whether periodic abnormal blood pressure fluctuations which occur in patients with pheochromocytoma are caused by enhancement of physiological reflexes by tumor-released catecholamines or by cycles of tumor-released catecholamines themselves. However, the fact that periodic blood pressure fluctuations disappeared after tumor resection in our patient suggests that catecholamines were periodically released from the tumor.
The trigger for the periodic cyclic fluctuations was unknown. In general, the causes of catecholamine release associated with pheochromocytoma include tumor blood flow, physical compression, tumor tissue collapse, and drugs such as nicotine and dopamine antagonists. In our case, since periodic circulatory fluctuations started after tracheal intubation, it is possible that the blood flow of the tumor changed due to changes in hemodynamics caused by the anesthesia-inducing drugs and stimulation of the tracheal intubation [10]. On the other hand, stabilizing circulating blood volume has been reported as a possible solution to interrupt the hypertensive cycle [2]. A decrease in intravascular volume due to preoperative hemodialysis and induction of anesthesia may have triggered periodic abnormal hypertension.
In our patient, nicardipine and landiolol were administered for blood pressure fluctuations; however, the response was poor. Hemodynamic control was considered impossible due to the release of very strong catecholamines during the periodic fluctuations. Alpha blockers have been reported to stabilize hypertension due to pheochromocytoma. Our patient developed hemodynamic fluctuations after two inductions of anesthesia, but the degree of fluctuation was smaller during the second surgery than during the first. It is possible that the degree of periodic fluctuation was reduced via the oral administration of doxazosin after the first surgery. In general, administration of an alpha blocker for 1–2 weeks is recommended before pheochromocytoma resection for intraoperative hemodynamic stabilization. In this case, the alpha blocker was also effective against periodic fluctuations.
In conclusion, periodic abnormal circulatory fluctuations were observed during anesthesia due to periodic catecholamine release from the pheochromocytoma. The cause of rare periodic blood pressure fluctuations in patients with pheochromocytoma is thought to be related not only to the cycle of sympathetic and parasympathetic reflexes but also to the periodic secretion of catecholamines.
Availability of data and materials
The data used in this case report are available from the corresponding author upon reasonable request.
Abbreviations
- HR:
-
Heart rate
- SBP:
-
Systolic blood pressure
- DAP:
-
Diastolic blood pressure
- NIBP:
-
Noninvasive blood pressure
- Hb:
-
Hemoglobin
- BUN:
-
Blood urea nitrogen
- Cre:
-
Creatinine
References
Manger WM, Gifford RW. Pheochromocytoma. J Clin Hypertens (Greenwich). 2002;4:62–72. https://doi.org/10.1111/j.1524-6175.2002.01452.x.
Ganguly A, Grim CE, Weinberger MH, et al. Rapid cyclic fluctuations of blood pressure associated with an adrenal pheochromocytoma. Hypertension. 1984;6:281–4. https://doi.org/10.1161/01.HYP.6.2.281.
Matsuguchi H, Tsuneyoshi M, Takeshita A, et al. Noradrenaline-secreting glomus jugulare tumor with cyclic change of blood pressure. Arch Intern Med. 1975;135:1110–3. https://doi.org/10.1001/archinte.1975.00330080112018.
Ferretti R, Cherniack NS, Longobardo G, et al. Systemic and pulmonary vasomotor waves. Am J Physiol. 1965;209:37–50. https://doi.org/10.1152/ajplegacy.1965.209.1.37.
Guyton AC, Statterfield JH. Vasomotor waves possibly resulting from CNS ischemic reflex oscillation. Am J Physiol. 1952;170:601–5. https://doi.org/10.1152/ajplegacy.1952.170.3.601.
Calhoun DA, Jones D, Textor S, et al. Resistant hypertension: diagnosis, evaluation, and treatment. A scientific statement from the American Heart Association Professional Education Committee of the Council for high blood pressure research. Hypertension. 2008;51:1403–19. https://doi.org/10.1161/HYPERTENSIONAHA.108.189141.
Guérin M, Guillemot J, Thouënnon E, et al. Granins and their derived peptides in normal and tumoral chromaffin tissue: implications for the diagnosis and prognosis of pheochromocytoma. Regul Pept. 2010;165:21–9 https://www.sciencedirect.com/science/article/abs/pii/S016701151000128X.
Kobal SL, Paran E, Jamali A, Mizrahi S, Siegel RJ, Leor J. Pheochromocytoma: cyclic attacks of hypertension alternating with hypotension. Nat Clin Pract Cardiovasc Med. 2008;5:53–7. https://doi.org/10.1038/ncpcardio1054.
Ionescu CN, Sakharova OV, Harwood MD, et al. Cyclic rapid fluctuation of hypertension and hypotension in pheochromocytoma. J Clin Hypertens (Greenwich). 2008;10:936–40. https://doi.org/10.1111/j.1751-7176.2008.00046.x.
Zuber SM, Kantorovich V, Pacak K. Hypertension in pheochromocytoma: characteristics and treatment. Endocrinol Metab Clin North Am. 2011;40:295–311. https://doi.org/10.1016/j.ecl.2011.02.002.
Acknowledgements
Not applicable
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
TW, this author helped with data collection and editing the manuscript. HM, this author helped conceive/design the case report, write the manuscript, and analyzing the data. RN, this author helped with data collection and editing the manuscript. SO, this author helped with the anesthesia procedure and helped with data collection and editing the manuscript. NS, this author helped with the anesthesia procedure and helped with data collection and editing the manuscript. YMT, this author helped conceive/design the case report and editing the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Watanabe, T., Miyoshi, H., Nakamura, R. et al. Rapid cyclic fluctuations in blood pressure during two surgeries associated with pheochromocytoma: a case report. JA Clin Rep 8, 80 (2022). https://doi.org/10.1186/s40981-022-00569-6
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40981-022-00569-6