
Abstract
Background
We tested the hypothesis that the C-MAC® video laryngoscope (C-MAC) with an external display is more useful than the disposable i-view™ video laryngoscope (i-view) with an integrated display or a Macintosh direct laryngoscope (Macintosh) for tracheal intubation with an aerosol box.
Methods
In this randomized, crossover manikin study, we recruited 37 medical personnel with > 2 years of dedicated anesthesia experience from five hospitals. After the three successful intubations within 60 s using each laryngoscope without a box, the participants performed tracheal intubation thrice with each laryngoscope with at least 2-h intervals in a determined order. The primary outcome was the intubation time. The secondary outcomes were success rate, Cormack-Lehane grade, and subjective difficulty scale score.
Results
Thirty-seven personnel (11 women and 26 men) with 12 [5–19] (median [interquartile range]) years of anesthesia and intensive care experience were enrolled. There was no significant difference in the intubation time: 30 [26–32] s for Macintosh, 29 [26–32] s for i-view, and 29 [25–31] s for C-MAC (P = 0.247). The success rate was 95–100%, without a significant difference (P = 0.135). The i-view and C-MAC exhibited superior Cormack-Lehane grades and lower subjective difficulty scale scores than the Macintosh; however, there were no differences between the i-view and C-MAC.
Conclusions
Rapid and highly successful tracheal intubation was possible with both Macintosh, i-view, and C-MAC on a normal airway manikin in an aerosol box. Improved Cormack-Lehane grade and the ease of performing the procedure may support the use of video laryngoscopes.
Trial registration
UMIN Clinical Trials Registry, UMIN000040269. Registered 30 April 2020.
Similar content being viewed by others


Background
The outbreak of coronavirus disease 2019 (COVID-19) is an important concern for healthcare providers because the causative agent, respiratory syndrome-corona virus-2 (SARS-CoV-2), is highly contagious, primarily via direct contact or droplet transmission. Tracheal intubation is considered one of the highest-risk procedures because of possible aerosol generation and the need to be in close physical proximity with the patient [1,2,3,4,5,6,7,8,9].
The “aerosol box” was first conceived by a Taiwanese doctor and was reported effective in preventing widespread dispersion of cough droplets during tracheal intubation [10,11,12]. This box was also expected to be useful in situations where higher-level personal protective equipment (PPE), such as the medical protective head hood and powered air-purifying respirator, is unavailable [13, 14]. However, some previous reports suggested that tracheal intubation in the box can be challenging because it restricts hand movements [11, 14,15,16].
Video laryngoscopes are recommended for tracheal intubation in patients with COVID-19 to keep distance from patient’s airway [1,2,3,4,5,6,7]. Currently, several types of video laryngoscopes are commercially available; some have an integrated display on the body, while others have an external display. There are some recommendations for the use of video laryngoscopes with an external display for patients with COVID-19 because it allows the healthcare practitioner to maintain a reasonable distance from the patient’s airway [3,4,5]. On the other hand, disposable video laryngoscopes such as i-view™ (i-view; Intersurgical, Wokingham, UK) may be beneficial for considering the risk of virus contamination. Furthermore, given the short supply of disposables for video laryngoscopes and the possible reduced risk of infection, a Macintosh direct laryngoscope (Macintosh) might be considered for use with an aerosol box [5, 6]. Many patients with COVID-19 who are undergoing tracheal intubation are hypoxemic and require rapid, highly successful procedures; therefore, it is essential to identify the optimal device to use with the box [2, 7].
When using an aerosol box, the box’s seam and barriers (eye-protective PPE and box wall) between the operator’s eyes and the patient’s glottis or integrated monitor of the video laryngoscope may impair the operator’s visibility. Thus, a video laryngoscope with an external display may be more useful than other types of laryngoscopes during tracheal intubation with an aerosol box. We, therefore, designed this study to test the hypothesis that the C-MAC® video laryngoscope (C-MAC; KARL STORZ, Tuttlingen, Germany) with an external display is more useful than the i-view with an integrated display when used with an aerosol box.
Methods
This prospective, randomized, crossover manikin study was conducted at the Nagoya City University Hospital and the Nagoya City East Medical Center from April 30, 2020, to May 11, 2020. The study protocol was reviewed and approved by the Nagoya City University Graduate School of Medical Sciences and Nagoya City University Hospital Institutional Review Board. This study was registered with the UMIN Clinical Trials Registry (identifier UMIN000040269). After verbally explaining the study flow to the participants and showing the video made for instruction, we obtained written consent for study participation. The patients were not involved in the study. All the methods were performed in accordance with the CONSORT 2010 statement: extension to randomized crossover trials.
We recruited medical personnel who were working in the fields of anesthesia and intensive care without previous experience with aerosol boxes from five hospitals (Nagoya City University Hospital, Nagoya City East Medical Center, Kainan Hospital, Kariya Toyota General Hospital, and Aichi Children’s Health and Medical Center) in Japan. According to the standard recommendations, only experienced physicians should perform tracheal intubation for patients with COVID-19; therefore, our study only included personnel with > 2 years of dedicated anesthesia experience after completion of residency training [1,2,3,4,5,6,7,8]. All participants were familiar with Macintosh and other types of video laryngoscopes such as the McGRATH MAC video laryngoscope (Medtronic, Minneapolis, MN, USA) or Airway Scope (Nihon Kohden, Tokyo, Japan) but had little experience with i-view and C-MAC.
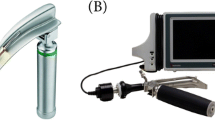
In this study, we compared the following three types of laryngoscopes: Macintosh, i-view, and C-MAC. The C-MAC is a video laryngoscope with an external display, while the i-view is a display-integrated, one-size-fits-all (equivalent to a Macintosh size 4), single-use video laryngoscope (Fig. 1). A reused size-3 blade was used for Macintosh, and a single-use size-3 Macintosh type blade was used for C-MAC. The AirSim Combo Bronchi X (TruCorp, Lurgan, Ireland) manikin designed for normal airway training was used for all the procedures. A 7.0-mm tracheal tube with a stylet, angled by each participant, was used. Although some arrangements have been reported [16, 17], we created and used an acrylic box based on the original version of the report [10].

Macintosh, i-view, and C-MAC laryngoscope and visual images of tracheal intubation with an aerosol box. A Macintosh direct laryngoscope. B i-view video laryngoscope. C C-MAC video laryngoscope. D–F Laryngoscopic view of the glottis in each laryngoscope. G–I Lateral image during the tracheal intubation in each laryngoscope. The white arrows show the operator’s lines of sight
Before the main measurement using the box, the participants were trained to familiarize themselves with the three laryngoscopes and the manikin used in the study. The training was conducted in the same manner as the main study, except in the following order (Macintosh, i-view, and C-MAC) without the box until three successful procedures within 60 s with each laryngoscope. All the training and main studies were conducted in an operating room at the two hospitals (Nagoya City University Hospital and Nagoya City East Medical Center). The manikin was placed on the operating table in the supine position under the box. Both the manikin and box were fixed with tape on the table so that the top of the manikin’s head was 10 cm away from the box. During training and the main test, the participating physician wore a long-sleeved gown, double gloves, a surgical mask, face shield or goggles, and a surgical cap. The N95 mask was not used because they are in short supply and have limited influence on intubation procedures. Neither a covering hood nor a powered air-purifying respirator was used. The height of the operating table was adjusted for each participant. In the box, a laryngoscope was placed on the left side of the manikin, and a tray was placed on the right side, where a tracheal tube and a cuff syringe with 8 ml of air were prepared. Six l/min of oxygen was administered to the manikin with a facemask. The participants removed the mask, opened the manikin’s mouth and picked up the laryngoscope. Then the participants picked up a tracheal tube, performed tracheal intubation, and removed the stylet and inflated air into the cuff of the tube by themselves, considering the minimal number of personnel in the operating room. Direct laryngoscopy was used with Macintosh, whereas an indirect (monitor) view was used with i-view and C-MAC for tracheal intubation (Fig. 1). The participants removed the outer glove on their right hand and grasped the reservoir bag for ventilation. The investigators (TN and YS) stood on the right side of the manikin, recording the intubation time with a stopwatch, and helped connect the anesthesia circuit to the tracheal tube. The intubation time was defined as the time between holding the laryngoscope and confirming the first expansion in both lungs. An intubation time > 60 s, esophageal intubation, or single-lung intubation were considered to indicate failure. After each procedure, the participant assessed the Cormack-Lehane grade and the subjective difficulty scale score of tracheal intubation (numeric rating scale 0–10, 0: no difficulty, 10: highest difficulty).
At least 2 h after the training, the participants began the main part of the study using an aerosol box. To compare the three laryngoscopes, we used a randomized crossover design by dividing the participants into six groups and testing them in the determined order (Fig. 2). An investigator (TN) who did not participate in the study performed the computer-generated randomization and allocated the participants to the six groups. The participant was blinded to the allocation until immediately before preparing the determined laryngoscope. The participants performed tracheal intubation on the manikin with the box three times by using each assigned laryngoscope. A washout period of at least 2 h was required before the next laryngoscope was used. The primary outcome was the intubation time. The secondary outcome included the success rate, Cormack-Lehane grade, and subjective difficulty scale score.

CONSORT diagram of the study participants
Statistical analysis
On the basis of the preliminary analysis performed by investigators who did not participate in the study, we estimated an intubation time of 25 s for C-MAC and 35 s for i-view. With an α error of 1.67% (adjusted for Bonferroni method), power of 90%, SD of 7, and correlation coefficient of 0.5 for 2-tailed statistical analysis, we arrived at a minimum sample size of 10 participants. However, we recruited as many eligible physicians as possible in the study because it also aimed to provide simulation training and increase the secondary endpoint estimate accuracy (success rate).
To compare the intubation time, Cormack-Lehane grade, and subjective difficulty scale score of the three laryngoscopes, we used the median values of the three measurements, considering the learning effect. The intubation time of i-view showed a non-normal distribution (Shapiro-Wilk test P < 0.05); the intubation times of the three laryngoscopes are presented as the median [interquartile range (IQR)] values. The Cormack-Lehane grade and subjective difficulty scale score are also presented as median [IQR] values. We used the Friedman test to compare the three devices’ performances. If a significant difference was found, the Wilcoxon signed-rank test with Bonferroni adjustment was used for pairwise comparisons. We compared the proportion of participants who successfully performed all three procedures between the three different laryngoscopes by using the Cochran Q test. All the statistical analyses were performed using the R software (version 3.6.3, R Foundation for Statistical Computing, Vienna, Austria). A P value of <0.05 was considered statistically significant.
Results
We enrolled 37 personnel (11 women and 26 men) with 12 [5–19] years of anesthesia and intensive care experience; all their records were incorporated into the final analysis (Fig. 2).
A summary of the results obtained with the box is shown in Table 1. The intubation time was 30 [26–32] s for Macintosh, 29 [26–32] s for i-view, and 29 [25–31] s for C-MAC, showing no significant difference (P = 0.247). The success rate was 95–100% without a significant difference, with two failed attempts with the i-view (one took 66 s, and the other was stopped after 60 s). The Cormack-Lehane grade was lower in i-view and C-MAC than in Macintosh. The subjective difficulty scale score was higher with Macintosh than with i-view or C-MAC. However, there were no differences in the Cormack-Lehane grade and the subjective difficulty scale score between i-view and C-MAC.
Detailed results obtained with and without the aerosol box are shown in Supplementary Tables 1 and 2, respectively. In training without the box, the intubation time was 29 [25–33] s for Macintosh, 29 [24–32] s for i-view, and 26 [24–30] s for C-MAC.
Discussion
In this simulation study that compared the performances of three types of laryngoscopes, namely, Macintosh, i-view, and C-MAC, for tracheal intubation in a manikin with an aerosol box, we found no significant differences in intubation time among the three types of laryngoscopes. All three laryngoscopes facilitated quick tracheal intubation with a 95–100% success rate; however, Macintosh had a higher subjective difficulty scale score and worse Cormack-Lehane grade than i-view and C-MAC.
The present results did not support our hypothesis that the use of C-MAC, which has an external display, is more useful than i-view for tracheal intubation with an aerosol box. This result suggests that skilled personnel may be able to overcome our concerns about visual problems such as the box’s seam and barriers between the eyes and the glottis or monitor (Fig. 1). Recently, Madabhushi et al. enrolled 78 patients with normal airways who had no COVID-19 and found that by using Glidescope (Verathon, Bothell, WA, USA) with an external display, the tracheal intubation time with the aerosol box was non-inferior to that without the box [18]. Furthermore, Puthenveettil et al. reported that C-MAC was easier to use than Macintosh for tracheal intubation with an aerosol box in 60 patients with normal airways without COVID-19 [19]. These results may suggest the potential benefit of an external display when performing tracheal intubation with an aerosol box in real patients [18, 19]. Although an external display might be useful in clinical settings where visual conditions are more unfavorable, such as cloudy or well-worn eye-protective PPE or aerosol boxes, we could not confirm the advantage in this simulation study using a transparent acrylic box.
The subjective difficulty scale score for tracheal intubation was higher for Macintosh than for i-view and C-MAC. In situations where both a Macintosh laryngoscope and a video laryngoscope can be used, our results support using a video laryngoscope because it would facilitate tracheal intubation with the aerosol box. However, video laryngoscopes may not be available because of an insufficient supply of disposable healthcare products [8, 9]. The Macintosh facilitated quick tracheal intubation with a high success rate that was unexpectedly comparable with that of video laryngoscopes, despite the greater difficulty and worse Cormack-Lehane grade. Our study is similar to that of Wakabayashi et al. who found that experienced anesthesiologists did not have clinically prolonged intubation times despite the poorer glottic view when using Macintosh with an aerosol box than without the box [20]. For medical personnel skilled in using Macintosh laryngoscopes, the combined use of a Macintosh laryngoscope and an aerosol box might be an option if a difficult airway is not anticipated and the availability of video laryngoscopes is limited.
Tracheal intubations in the aerosol box were performed with a highly successful rate (95–100%) and median intubation time of 29–30 s, which was not clinically different from the median intubation time of 26–29 s without the box. A recently published meta-analysis revealed that intubation time with an aerosol box increased by 4 s (95% confidence interval 2.4–5.6 s) as compared with that without a box, but this may not be clinically relevant [21]. This meta-analysis also revealed no significant prolongation of intubation time of 1.9 s when the video laryngoscope was used by a consultant. The shorter intubation time in our study may be due to experiences of the participants and their familiarity with the device and manikin through training. The high success rate and short intubation time observed in our study suggest that an aerosol box can be used safely after sufficient training by experienced personnel.
Our study has several strengths. First, we enrolled a moderate number of physicians who had > 2 years of dedicated anesthesia experience and were engaged in airway management at multiple centers. Moreover, the participants in our study wore PPE and underwent tracheal intubation with minimal assistance, referring to recommendations for airway management in patients with COVID-19. Second, we measured the outcomes three times for each laryngoscope and used the median values for the comparisons. In unfamiliarity, one-time measurements may result in long intubation times, which is not clinically meaningful.
Certain limitations of the present study need to be noted. First, this simulation study was performed using a manikin. It is necessary to examine the safety and efficacy of aerosol boxes in clinical practice. Evidence for the use of aerosol boxes in real patients is lacking and must be studied in the near future [21, 22]. Second, differences in the participants’ familiarity with the three laryngoscopes might have affected the results. However, we believe that these effects were minimized because we provided training to the participants before initiating the main study. Third, we did not evaluate physician safety in this study in terms of droplet splash, aerosol spread, and PPE breakage, although no breakage of long-sleeved gowns occurred in our study. Fourth, we used the box with the original design; however, various modifications to the box, with regard to shape and draping, have been reported [10, 16, 17]. These might make it difficult to generalize our study results. Finally, we did not simulate a difficult airway setting in the present study. Furthermore, the participants in our study placed airway management equipment in their optimal position. Our results are not applicable to situations such as difficult airways and emergency airway settings. In such situations, the box should be removed and the airway secured in the best possible manner [11, 12, 17].
Conclusions
In summary, tracheal intubation in an aerosol box can be performed using any of the following three types of laryngoscopes, namely, Macintosh, i-view, and C-MAC, with an intubation time of 29–30 s and a success rate of 95–100%. Improved Cormack-Lehane grade and ease of procedure may support using a video laryngoscope when using the aerosol box.
Availability of data and materials
Data are available from the corresponding author on reasonable request.
Abbreviations
- COVID-19:
-
Coronavirus disease 2019
- IQR:
-
Interquartile range
- PPE:
-
Personal protective equipment
References
Zuo MZ, Huang YG, Ma WH, Xue ZG, Zhang JQ, Gong YH, et al. Expert recommendations for tracheal intubation in critically ill patients with novel coronavirus disease 2019. Chin Med Sci J. 2020;35:105–9.
Meng L, Qiu H, Wan L, Ai Y, Xue Z, Guo Q, et al. Intubation and ventilation amid the COVID-19 outbreak: Wuhan’s experience. Anesthesiology. 2020;132(6):1317–32. https://doi.org/10.1097/ALN.0000000000003296.
Wax RS, Christian MD. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anaesth. 2020;67(5):568–76. https://doi.org/10.1007/s12630-020-01591-x.
Sorbello M, El-Boghdadly K, Di Giacinto I, Cataldo R, Esposito C, Falcetta S, et al. The Italian coronavirus disease 2019 outbreak: recommendations from clinical practice. Anaesthesia. 2020;75(6):724–32. https://doi.org/10.1111/anae.15049.
Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 2020;75(6):785–99. https://doi.org/10.1111/anae.15054.
Brewster DJ, Chrimes N, Do TB, Fraser K, Groombridge CJ, Higgs A, et al. Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group. Med J Aust. 2020;212(10):472–81. https://doi.org/10.5694/mja2.50598.
Yao W, Wang T, Jiang B, Gao F, Wang L, Zheng H, et al. Emergency tracheal intubation in 202 patients with COVID-19 in Wuhan, China: lessons learnt and international expert recommendations. Br J Anaesth. 2020;125(1):e28–37. https://doi.org/10.1016/j.bja.2020.03.026.
Chen X, Liu Y, Gong Y, Guo X, Zuo M, Li J, et al. Perioperative management of patients infected with the novel coronavirus: recommendation from the Joint Task Force of the Chinese Society of Anesthesiology and the Chinese Association of Anesthesiologists. Anesthesiology. 2020;132(6):1307–16. https://doi.org/10.1097/ALN.0000000000003301.
Cook TM. Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic - a narrative review. Anaesthesia. 2020;75(7):920–7. https://doi.org/10.1111/anae.15071.
Everington K. Taiwanese doctor invents device to protect US doctors against coronavirus: Taiwan news. https://www.taiwannews.com.tw/en/news/3902435. Accessed 18 May 2020
Canelli R, Connor CW, Gonzalez M, Nozari A, Ortega R. Barrier enclosure during endotracheal intubation. N Engl J Med. 2020;382(20):1957–8. https://doi.org/10.1056/NEJMc2007589.
Yang SS, Zhang M, Chong JJR. Comparison of three tracheal intubation methods for reducing droplet spread for use in COVID-19 patients. Br J Anaesth. 2020;125(1):e190–1. https://doi.org/10.1016/j.bja.2020.04.083.
Tsai PB. Barrier shields: not just for intubations in today’s COVID-19 world? Anesth Analg. 2020;131(1):e44–5. https://doi.org/10.1213/ANE.0000000000004902.
Leyva Moraga FA, Leyva Moraga E, Leyva Moraga F, Juanz González A, Ibarra Celaya JM, Ocejo Gallegos JA, et al. Aerosol box, an operating room security measure in COVID-19 pandemic. World J Surg. 2020;44(7):2049–50. https://doi.org/10.1007/s00268-020-05542-x.
Gould CL, Alexander PDG, Allen CN, McGrath BA, Shelton CL. Protecting staff and patients during airway management in the COVID-19 pandemic: are intubation boxes safe? Br J Anaesth. 2020;125(3):e292–3. https://doi.org/10.1016/j.bja.2020.05.001.
Begley JL, Lavery KE, Nickson CP, Brewster DJ. The aerosol box for intubation in coronavirus disease 2019 patients: an in-situ simulation crossover study. Anaesthesia. 2020;75(8):1014–21. https://doi.org/10.1111/anae.15115.
Malik JS, Jenner C, Ward PA. Maximising application of the aerosol box in protecting healthcare workers during the COVID-19 pandemic. Anaesthesia. 2020;75(7):974–5. https://doi.org/10.1111/anae.15109.
Madabhushi P, Kinthala S, Ankam A, Chopra N, Porter BR. Time to adapt in the pandemic era: a prospective randomized non -inferiority study comparing time to intubate with and without the barrier box. BMC Anesthesiol. 2020;20(1):232. https://doi.org/10.1186/s12871-020-01149-w.
Puthenveettil N, Rahman S, Vijayaraghavan S, Suresh S, Kadapamannil D, Paul J. Comparison of aerosol box intubation with C-MAC video laryngoscope and direct laryngoscopy-a randomised controlled trial. Indian J Anaesth. 2021;65(2):133–8. https://doi.org/10.4103/ija.IJA_1218_20.
Wakabayashi R, Ishida T, Yamada T, Kawamata M. Effect of an aerosol box on tracheal intubation difficulty. J Anesth. 2020;34(5):790–3. https://doi.org/10.1007/s00540-020-02835-2.
Lim ZJ, Ponnapa Reddy M, Karalapillai D, Shekar K, Subramaniam A. Impact of an aerosol box on time to tracheal intubation: systematic review and meta-analysis. Br J Anaesth. 2021;126(3):e122–5. https://doi.org/10.1016/j.bja.2020.11.036.
Sorbello M, Rosenblatt W, Hofmeyr R, Greif R, Urdaneta F. Aerosol boxes and barrier enclosures for airway management in COVID-19 patients: a scoping review and narrative synthesis. Br J Anaesth. 2020;125(6):880–94. https://doi.org/10.1016/j.bja.2020.08.038.
Acknowledgements
The authors would like to thank Hiroya Hashimoto, Ph.D., Clinical Research Management Center, Nagoya City University Hospital (Nagoya, Japan), for the statistical advice; Aiji Sato, D.D.S., Ph.D., Department of Anesthesiology, Aichi Gakuin University School of Dentistry (Nagoya, Japan); and Tatsuya Tsuji, M.D., Department of Anesthesiology and Intensive Care Medicine, Nagoya City University Graduate School of Medical Sciences (Nagoya, Japan), for the advice on the manuscript, and all the participants for their cooperation in the study. The preprint of this manuscript was deposited in Research Square with DOI:10.21203/rs.3.rs-90522/v1. The authors would like to thank Enago (www.enago.jp) for the English language review.
Funding
None declared.
Author information
Authors and Affiliations
Contributions
TN designed and conducted the study, analyzed the data, and wrote the manuscript. YS helped design and conduct the study, and revise the manuscript. YK helped design and conduct the study, and revise the manuscript. KS helped design and conduct the study, and revise the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Nagoya City University Graduate School of Medical Sciences and Nagoya City University Hospital Institutional Review Board (reference number, 60-20-0032). After explaining the study flow to the participants by verbally and the video made for instruction, we obtained written informed consent for study participation from all the participants.
Consent for publication
We obtained written consent for publication. Patients were not involved in the study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Detailed results using the Macintosh, i-view, and C-MAC laryngoscopes for tracheal intubation in the aerosol box. Supplementary Table 2. Detailed training results using the Macintosh, i-view, and C-MAC laryngoscopes for tracheal intubation without the aerosol box.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nakanishi, T., Sento, Y., Kamimura, Y. et al. Macintosh laryngoscope and i-view™ and C-MAC® video laryngoscopes for tracheal intubation with an aerosol box: a randomized crossover manikin study. JA Clin Rep 7, 52 (2021). https://doi.org/10.1186/s40981-021-00455-7
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40981-021-00455-7