
Abstract
Introduction
The rupture of the anterior cruciate ligament (ACL) is one of the most common injuries of the knee. Women have a higher injury rate for ACL ruptures than men. Various indicators for this sex-specific difference are controversially discussed.
Aim
A systematic review of the literature that compares surface electromyography (EMG) values of adult female and male subjects to find out if there is a difference in neuromuscular activation of the knee stabilizing muscles.
Methods
This systematic review has been guided and informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Studies which examined sex-specific differences with surface EMG measurements (integral, root mean squares, mean values, analysis of time and amplitude) of the knee stabilizing muscles were retrieved via searches from the databases PubMed, CINAHL, Embase, CENTRAL and SPORTDiscus. The risk of bias of included studies was assessed with the National Heart, Lung and Blood Institute (NHLBI) study quality assessment tool. A synthesis of results was performed for relevant outcomes.
Results
Fifteen studies with 462 healthy participants, 233 women (mean age 21.9 (± 2.29) years) and 299 men (mean age 22.6 (± 2.43) years), were included in the systematic review. The methodological quality of the studies was mostly rated “fair” (40%). A significantly higher activity of the muscles vastus lateralis and vastus medialis was found in females, in three studies. Two studies found significantly lower neuromuscular activity in the muscles biceps femoris and semitendinosus in females. All other included studies found no significant differences or reported even contradicting results.
Conclusion
The controversial findings do not allow for a concluding answer to the question of a sex-specific neuromuscular activation. Further research with higher statistical power and a more homogeneous methodical procedure (tasks and data normalisation) of the included studies may provide insight into possibly existing sex-specific differences in neuromuscular activation. This systematic review could help to improve the methodical design of future studies to get a more valid conclusion of the issue.
Trial registration
CRD42020189504.
Similar content being viewed by others


Introduction
The rupture of the anterior cruciate ligament (ACL) is one of the most common injuries of the knee [1, 2]. Consequences can be severe, such as pain, reduced range of motion, reduced physical activity and long-term joint degeneration [3, 4]. Furthermore, the return to sport rate differs depending on the level of competition: i.e. 81% returned to any sport, 65% returned to the preinjury level of activity and only 55% returned to competition level after surgery [5]. However, after one year only a minority of athletes have returned to their preinjury level [6] and the rate of sustaining a second ACL injury exceeds 20% [7, 8].
Women have a higher injury rate for ACL ruptures than men [9, 10]. This applies in particular for non-contact injuries where women have a three and a half times higher risk to rupture the ACL [11,12,13]. Another study stated that women playing sports such as soccer or basketball even have a two to eight times higher risk of an ACL rupture [14].
To summarize the points mentioned above, it is important to find out why there is such a large sex difference in non-contact ACL injuries. Various indicators for this increased risk of injury in women, such as biomechanical, hormonal and neuromuscular aspects, are controversially discussed. These contributing factors can be classified into intrinsic (not controllable), extrinsic (controllable), or both (partially controllable) [15]. One study considered the neuromuscular factors as the most likely ones for the increased risk of injury in women [16]. Therefore, the focus of this systematic review will be on neuromuscular factors assessed by EMG, and the comparison of neuromuscular activation between women and men. A narrative review of various cross-sectional studies assumes that the sex difference in injury rates is due to sex-specific neuromuscular adaptation and biomechanical landing techniques [17]. Other studies describe a difference between women and men in activation timing or force intensity of the knee stabilizing muscles [18,19,20,21,22,23]. Furthermore, a dominance of the quadriceps muscle over the hamstring muscles in women is described. This larger quadriceps to hamstrings ratio could be a risk factor for ACL injuries, as it could promote anterior tibial translation [21, 22, 24, 25]. The quadriceps dominance in women was found in various activities. For example, during jumps, cutting and swerving manoeuvres [26,27,28]. However, these statements are contradicted by a systematic review which summarizes the sex differences in landing and cutting manoeuvres [29]. A total of seven studies, all cross-sectionally designed, were included in the analysis. The authors summarize that the biomechanical sex differences are based on questionable clinical relevance and that they did not find any quadriceps dominance for the activities described [29]. Furthermore, other authors could not find any sex-specific differences in the explosive quadriceps-hamstrings ratio [30]. In addition, a recent study paired women and men in terms of strength and concluded that strength-paired women and men showed no significant differences in neuromuscular activity [31]. Regarding the controversy of sex-specific differences in neuromuscular activation, it is of general interest to compile data to better understand whether there are sex-specific differences in neuromuscular activation present or not.
The purpose of this systematic review is to find out if there is a difference in neuromuscular activity in adult women and men assessed with electromyography. Results could help as a guideline to the omnipresent question in clinical studies regarding the need to differentiate between women and men in the evaluation of data on neuromuscular activation. Moreover, results could have an impact on the rehabilitation process as the results could focus on a new aspect to consider when defining the rehabilitation strategy for women and men. Consequently, these objectives result in the following research question: Are there sex-specific differences in neuromuscular activation of the knee stabilizing muscles in adults with or without an ACL injury?
Methods
Protocol and registration
This systematic review has been guided and informed by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines [32, 33]. The protocol has been registered a priori on the International Prospective Register of Systematic Reviews Database – PROSPERO (CRD42020189504).
Eligibility criteria
To define relevant keywords for the systematic literature search, the Population-Exposure-Comparator-Outcome framework (PECO) was used [34] (Table 1). In addition, the following inclusion criteria were defined: Study participants had to be healthy or suffer from an ACL injury (either treated conservatively or surgically with an ACL reconstruction), comparisons of neuromuscular control between females and males had to be provided, and the EMG-related outcomes had to be reported as mean, root mean squares (RMS), integral, in the domains of amplitude or time etc. Moreover, included studies had to be original articles with any experimental study design (e.g. cross-sectional study, randomized-controlled trial etc.) published in peer-reviewed, scientific journals, and available as full text. No language restrictions were defined. Exclusion criteria were children and adolescents as participants, other injuries of the lower extremity than ACL injuries, neurological diseases, chronic pain or inflammatory processes, data from interventions with a fatigue protocol, and publications such as editorials, book chapters and reviews.
Information sources and search strategy
The search was conducted between August and September 2020 using five electronic databases: PubMed, CINAHL, Embase, Cochrane Central Register of Controlled Trials (CENTRAL) and SPORTDiscus. The search strategy was based on the predetermined research question and the PECO method. The following search string was used: “(EMG OR electromyography) AND (lower extremity OR knee OR anterior cruciate ligament OR ACL) AND (neuromuscular activation OR neuromuscular control OR neuromuscular activity) AND (gender bias OR sex differences OR sex factors OR female OR females OR woman OR women OR male OR males OR man OR men)”. The adaption of the search string for each database was conducted with the help of the “Ref-Hunter Manual” for literature research [35]. The database search was completed by checking the reference lists of included studies to identify additional and potentially eligible studies. There was no search for grey literature.
Study selection
The acquired data was extracted and organized with the Endnote software (EndNote X9.2 (Bld 13,018), Clarivate Analytics, Philadelphia, USA). After exclusion of all duplicates, two reviewers (MS and AB) independently assessed titles and abstracts of the retrieved, eligible literature based on the defined criteria in Table 1. Clearly ineligible studies were excluded. The assessment of the references was coordinated with the Rayyan QCRI software [36]. Disagreements were discussed and resolved by consensus, where necessary, with a third reviewer (HB). Afterwards, a second screening procedure followed. Therefore, all eligible articles were retrieved in full text and reviewed independently for inclusion by the same two reviewers (MS and AB).
Assessment of risk of bias
The quality of each study included was evaluated using the “Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies” (QAT) from the NHLBI [37]. This assessment tool is widely used and recommended. It includes fourteen questions for evaluating potential bias in studies such as patient selection, study power, confounding and the strength of causality in the association between interventions and outcomes. As a reviewer you can select “yes”, “no” or “cannot determine / not applicable / not reported”. There is no quantitative rating of the level of evidence. After a calibration regarding the assessment tool, both reviewers (MS and AB) assessed the quality of the included studies independently. Disagreements were discussed and solved by consensus. All studies remained included regardless the outcome of the quality assessment.
Data items, collection process and synthesis methods
Concerning the data items and collection, a spreadsheet was developed a priori to the data extraction. The data extraction was conducted by the first author (MS) followed by an accuracy examination of the last author as second reviewer (AB) to assure quality control. The following variables regarding study characteristics were extracted: first author, publication year, country where study had been conducted, study design, number of participants measured, mean age of participants, intervention/task, outcomes, main results, and conclusion. Quantities of surface electromyography (EMG) measurements such as root mean squares (RMS), integrals, mean values, and analysis in time and amplitude domain were extracted as outcomes.
The weighted overall effect size of the standardized mean difference and the 95% confidence interval (95%-CI) were calculated for each included study. The Hedges’g within a random-effect model was used as a standardization. The software RevMan 5.3 (Review Manager, Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) was used. Due to heterogeneity between the studies (e.g. various tasks, different measurement units, different ways to normalize EMG data, various levels of sport of the participants) it was not appropriate to pool the data for the purpose of a meta-analysis. For this reason, a systematic review with a synthesis according to PRISMA [33, 34] was carried out (Additional file 1).
Results
Study selection
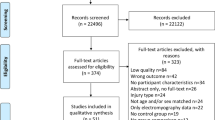
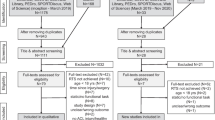
Figure 1 presents all the screened and included studies in this review. Fifteen studies [20, 22, 24, 27, 28, 38,39,40,41,42,43,44,45,46,47] of a total of 2′607 papers retrieved from the database search, met the inclusion criteria.

Flow chart of the search strategy, adapted from PRISMA [33]. Abbreviation: f/m = female/male
Quality assessment
The methodological quality of the 15 included studies was rated according to the NHLBI assessment tool [37] (see Table 2). All studies were cross-sectionally designed. Six studies were rated to have a fair quality (40%), four showed a good quality (27%) and five had a poor quality (33%). The total agreement (good/fair/poor) between the two reviewers amounted to 73% (11/15 studies) and the inter-rater reliability, measured using the Cohen’s Kappa, was good (K = 0.6) [48]. The main limitations were (i) no mention of a sample size justification as 11 of 15 studies reported no power description [20, 22, 24, 27, 28, 39,40,41, 44,45,46] and (ii) the lack of consideration of confounders as six out of 15 studies had a more heterogeneous subject group without any statistical adjustment [27, 39, 42, 43, 46, 47]. In addition, none of the studies reported blinding of the assessors. Common strengths were the clearly stated objectives and accurate description of the independent and dependent variables, respectively.
Study participants
In total, 462 healthy participants, 233 women and 229 men, were tested. The mean age was 21.9 (± 2.29) years for women and 22.6 (± 2.43) years for men. Excluded from this calculation are 20 participants from the study of Wu et al. (2016) [47]. In this study an older group with a mean age of 66.8 ± 3.4 years for men and 66.1 ± 4.4 years for women had been measured (see Table 3).
Synthesis of study results
Three studies found a significantly higher activity in the muscles VL and VM in females, compared to males during a vertical jump, two side-step cutting manoeuvres and two-legged hopping at two different rates [22, 24, 28]. Two studies reported significantly lower neuromuscular activity in the BF and ST in females compared to males during a vertical jump and a side-cutting manoeuvres [22, 38]. No significant differences of neuromuscular activation between females and males, or even contradicting results [39, 47] were found in all other included studies (see Table 4). The effect size of six studies [20, 38, 40, 44, 46, 47] favour female sex, and nine [22, 24, 27, 28, 39, 41,42,43, 45] favour male sex for higher neuromuscular activation. The effect sizes presented showed a small to medium effect [49]. Only two studies reported a large effect: Deschenes et al. (2009) [40] reported an effect size of -1.71 (95%-CI: -2.77; -0.65), and Wu et al. (2016) [47] an effect size of -0.74 (95%-CI: -1.18; -0.31). Moreover, the calculated effect size of nine studies indicates a p-value higher than 0.5 as the 95%-CI includes the null hypothesis and thus does not favour either sex [22, 27, 38, 39, 41, 42, 44,45,46].
One study had a fatigue-protocol which was applied after the baseline measurement to examine the effect of fatigue [46]. Another study performed an unloading-protocol by walking on crutches and with a fixed knee brace for one week after baseline measurement [40]. From these two studies, only baseline measurements were included in the results as the aspect of fatigue was part of the exclusion criteria. A follow-up study had to be excluded, because the same data as in the first study was used as baseline data (see Fig. 1).
Discussion
The aim of this systematic review was to determine whether there are sex differences in neuromuscular activation of knee stabilizing muscles. Only seven studies reported EMG activity as %MVC, with the main findings of a significantly higher activation in VL/VM [22, 24, 28] and significantly lower activation in the hamstrings [22, 38] in females. But one study [39] found significantly higher activation in the hamstrings in females and two studies [42, 44] found no significant sex-difference. However, these studies differed in terms of the task performed during the measurement. Furthermore, the eight studies which had another normalisation of their EMG activity also showed opposing results [20, 27, 40, 41, 43, 45,46,47].
There are some differences between the registered protocol in PROSPERO and the review: Post-hoc changes to eligibility criteria had to be made and pre-specified inclusion criteria had to be adapted due to insufficient data [50]. Moreover, the risk of bias assessment was evaluated using the QAT from the NHLBI [37] instead of the Downs and Black Quality Index [51]. The QAT is better suited for the quality assessment of cross-sectional studies.
There are many different quality assessment tools for cross-sectional studies, but no gold standard exists [52]. The NHLBI assessment tool QAT [37] was used to reason why some questions were not applicable for cross-sectional studies addressing different tasks with EMG measurements. For instance, assessor blinding was not mentioned in the studies. However, it can be assumed that blinding was given by detection of objective EMG data with the computer. Moreover, the computer analysis could be carried out by a second researcher who had not been involved in the recruitment and measurement process. To overcome this problem, future studies should report the exact data collection procedure. The QAT [37] is widely used and recommended by Ma et al. (2020) [53] and Carbia et al. (2018) [54] for the quality assessment of observational cohort and cross-sectional studies [53, 54]. The evaluation of the overall quality rating remains subjective to a certain extent as no scores are awarded. This subjectivity is somewhat reduced by the QAT guidelines [37]. The guidelines force the researcher to look at the overall picture of the individual studies including their methodological differences as well as how the various aspects of the QAT [37] have to be weighted in reference to the research questions. In addition, the total agreement between the researchers and the inter-rater reliability was calculated which can objectify the results of the quality assessment.
The results from the five studies with poor quality showed contradictory results. A significant higher activation or time to peak in women was found in three studies, but in different muscles [42, 46, 29]. One study found a lower activation in the VL in women [50], and one found no significant difference [49]. The seven studies which had a data normalisation with %MVC still differed in the task carried out during the measurement [23, 25, 29, 41, 42, 45, 47]. The same problem concerned all the studies which were rated having good quality [21, 41, 44, 48]. Even though three studies found sex-specific differences in neuromuscular activation, they all used a different data normalisation method [21, 41, 48]. Therefore, subgroup analyses were also not possible. The methodological limitations in the selected studies, which made the quantitative summarization by a meta-analysis impossible, was also found in previous systematic reviews [55, 56]. According to Martin-Fuentes et al. (2020) [56], the methodological issue is the main concern for the interpretation of EMG data and involves a potential risk of bias. Therefore, it is suggested that future studies should account for these issues.
Several differences in the study characteristics of the included studies were found but this was not the case for the study design as they were all cross-sectional studies. Even though most of the participants were within the same age range between 20 to 30 years and healthy, the results cannot be generalized for this population only due to the uncertainty of the results. The fact that only studies with adult participants were included lead to a small number of eligible hits from the databases. Many studies had to be excluded which had examined the neuromuscular control in adolescents. However, this decision can be justified by the fact that adolescence is a time of physical change and hormonal adaption which could have an influence on sex-specific neuromuscular activation [57].
Five studies also assessed activation of further muscles (gluteus medius and maximus, soleus and tibialis anterior) which are not directly related to knee stability [24, 28, 39, 41, 44]. Therefore, these muscles were not included in this systematic review. Also, all other outcomes in the included studies such as kinematics and joint laxity were not considered in this systematic review.
The level or type of sport varied between the studies and this could have distorted the results as the activity level could have an influence on the sex-specific neuromuscular activation [58]. The performance of the different tasks in the studies depended on the sport level and whether the participants were familiar with the tasks. For example, jogging, jumping one- and two-legged, or side-cutting and -stepping manoeuvres were used to assess neuromuscular activation of participants. In order not to narrow the search too much, the task was not specified in advance. The question arises whether it is appropriate to compare neuromuscular activity between different tasks to evaluate sex-specific neuromuscular activation and not a particular task. The systematic review of Benjaminse et al. (2011) [29] laid their focus on the plant and cut manoeuvres and thereby only had two references which examined the sex-specific neuromuscular activation with surface EMG. Another systematic review limited the tasks to dynamic activities and searched for neuromuscular control in ACL patients but did not compare between sexes [59].
The selection of included EMG data was restricted a priori to variables in the domains of amplitude (mean, RMS, integral) and time (onset, offset, time to peak). Frequency analysis of EMG data was not appropriate for the research question related to dynamic movement situations. Therefore, studies which assessed sex-specific differences under the aspect of fatigue were excluded. In addition, data normalisation varied between the included studies, which did not allow to pool data adequately. This problem had also been observed in previous reviews [55, 56]. EMG data normalization for lower extremity could be done by taking neuromuscular activation during treadmill walking as 100% [60, 61].
The sample size had a large effect on the significance of the results leading to lower power [29]. This fact could be one reason for the heterogenous results. Only four studies provided a sample size justification. Moreover, the sample size was small with a mean of fifteen subjects included in each intervention or control group [38, 42, 43, 47]. The question remains whether a conclusive result can be drawn from a cross-sectional study design with small sample sizes. For a better understanding, cohort studies or randomised controlled trials could show clearer results.
As the results showed different and contradictory findings, the question arises whether it is purposeful to examine isolated neuromuscular activation. Factors such as anatomy, biomechanics and hormones could influence the measurements [62]. Significant differences in foot and hip positions during a single-legged squat in women and men were associated with a decreased ability for women to maintain a varus knee position [63]. Benjaminse et al. (2011) [29] questioned whether the ACL injuries during plant and cutting manoeuvres were sex-related and stated that “the biomechanical and neuromuscular contributions to injury risk should not be isolated and should extend beyond an isolated gender focus”. Furthermore, participants with different body fat levels should be analysed since this variable could influence the EMG activity recorded [64].
Another interesting aspect could be the influence of unloading which could explain the sex difference in increased risk of injury. One of the included studies found out that after one week of unloading men had a significantly higher activity and the decline in EMG activity from pre- to post-unloading was significant in women [40]. The conclusion was “that women suffer a greater degree of neuromuscular disturbance than men as a result of short-term muscle unloading” [40]. These results suggested that women might be more sensitive to a lack of neuromuscular stimulus. One could conclude that this could have a large influence on the rehabilitation after injury and that preventive muscle training could be more important for women than for men. Therefore, future studies assessing patients with an ACL rupture are needed to further understand how the injury itself, treatment modalities, or sex influences neuromuscular activation.
Conclusion
This systematic review provides an objective overview of the current research available about sex-specific differences in neuromuscular activation of the lower extremity in healthy adults. The controversial findings do not allow for a concluding answer to the question of sex-specific neuromuscular activation of the lower extremity. In addition, the study quality of the included studies was mainly fair, which suggest the need of more high-quality research to draw a solid conclusion and reduce the risk of bias. Specifically, further research with higher statistical power and a more homogeneous methodical procedure (tasks and data normalisation) of the included studies may help to evaluate whether a sex-specific difference in neuromuscular activation exists. Beside from that, conducting studies with ACL-injured subjects and healthy controls would be important to find out how neuromuscular activation may change in women and men after an ACL injury.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- EMG:
-
Electromyography
- ACL:
-
Anterior cruciate ligament
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analysis
- PROSPERO:
-
Prospective Register of Systematic Reviews Database
- PECO:
-
Population/Exposure/Comparator/Outcome
- QAT:
-
Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies
- NHLBI:
-
National Heart, Lung and Blood Institute
- MVC:
-
Maximum voluntary contraction
- RMS:
-
Root mean square
- RF:
-
Rectus femoris muscle
- VL:
-
Vastus lateralis muscle
- VM:
-
Vastus medialis muscle
- ST:
-
Semitendinosus muscle
- BF:
-
Biceps femoris muscle
- MG:
-
Medial gastrocnemius muscle
- LG:
-
Lateral gastrocnemius muscle
- CENTRAL:
-
Cochrane Central Register of Controlled Trials
- SM:
-
Semimembranosus muscle
References
Eggli S. Patienteninformation Dynamische Intraligamentäre Stabilisierung (DIS); Orthopädie Sonnenhof; retrieved on 01.03.2020 from https://docplayer.org/24634868-Patienteninformation-dynamische-intraligamentaere-stabilisierung-dis.html. 2020.
Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42(2):311–9.
Busch A, Blasimann A, Henle P, Baur H. Neuromuscular activity during stair descent in ACL reconstructed patients: a pilot study. Knee. 2019;26(2):310–6.
Lohmander LS, Ostenberg A, Englund M, Roos H. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 2004;50(10):3145–52.
Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-five per cent return to competitive sport following anterior cruciate ligament reconstruction surgery: an updated systematic review and meta-analysis including aspects of physical functioning and contextual factors. Br J Sports Med. 2014;48(21):1543–52.
Ardern CL, Webster KE, Taylor NF, Feller JA. Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: two-thirds of patients have not returned by 12 months after surgery. Am J Sports Med. 2011;39(3):538–43.
Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2016;44(7):1861–76.
Thomas AC, Villwock M, Wojtys EM, Palmieri-Smith RM. Lower extremity muscle strength after anterior cruciate ligament injury and reconstruction. J Athl Train. 2013;48(5):610–20.
Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: Part 1, mechanisms and risk factors. Am J Sports Med. 2006;34(2):299–311.
Kobayashi H, Kanamura T, Koshida S, Miyashita K, Okado T, Shimizu T, et al. Mechanisms of the anterior cruciate ligament injury in sports activities: a twenty-year clinical research of 1,700 athletes. J Sports Sci Med. 2010;9(4):669–75.
Ireland ML. The female ACL: why is it more prone to injury? Orthop Clin North Am. 2002;33(4):637–51.
Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St Pierre P, Taylor DC. Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 West Point cadets. Am J Sports Med. 2003;31(6):831–42.
Prodromos CC, Han Y, Rogowski J, Joyce B, Shi K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury-reduction regimen. Arthroscopy. 2007;23(12):1320-5 e6.
Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995;23(6):694–701.
Ireland ML. Anterior cruciate ligament injury in female athletes: epidemiology. J Athl Train. 1999;34(2):150–4.
Wojtys EM, Wylie BB, Huston LJ. The effects of muscle fatigue on neuromuscular function and anterior tibial translation in healthy knees. Am J Sports Med. 1996;24(5):615–21.
Voskanian N. ACL Injury prevention in female athletes: review of the literature and practical considerations in implementing an ACL prevention program. Curr Rev Musculoskelet Med. 2013;6(2):158–63.
Del Bel MJ, Flaxman TE, Smale KB, Alkjaer T, Simonsen EB, Krogsgaard MR, et al. A hierarchy in functional muscle roles at the knee is influenced by sex and anterior cruciate ligament deficiency. Clin Biomech. 2018;57:129–36.
Huston LJ, Wojtys EM. Neuromuscular performance characteristics in elite female athletes. Am J Sports Med. 1996;24(4):427–36.
Shultz SJ, Perrin DH, Adams MJ, Arnold BL, Gansneder BM, Granata KP. Neuromuscular response characteristics in men and women after knee perturbation in a single-leg. Weight-Bearing Stance J Athl Train. 2001;36(1):37–43.
Sigward SM, Powers CM. The influence of gender on knee kinematics, kinetics and muscle activation patterns during side-step cutting. Clin Biomech (Bristol, Avon). 2006;21(1):41–8.
Urabe Y, Kobayashi R, Sumida S, Tanaka K, Yoshida N, Nishiwaki GA, et al. Electromyographic analysis of the knee during jump landing in male and female athletes. Knee. 2005;12(2):129–34.
White KK, Lee SS, Cutuk A, Hargens AR, Pedowitz RA. EMG power spectra of intercollegiate athletes and anterior cruciate ligament injury risk in females. Med Sci Sports Exerc. 2003;35(3):371–6.
Hanson AM, Padua DA, Troy Blackburn J, Prentice WE, Hirth CJ. Muscle activation during side-step cutting maneuvers in male and female soccer athletes. J Athl Train. 2008;43(2):133–43.
Chappell JD, Creighton RA, Giuliani C, Yu B, Garrett WE. Kinematics and electromyography of landing preparation in vertical stop-jump: risks for noncontact anterior cruciate ligament injury. Am J Sports Med. 2007;35(2):235–41.
Malinzak RA, Colby SM, Kirkendall DT, Yu B, Garrett WE. A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clin Biomech. 2001;16(5):438–45.
Myer GD, Ford KR, Hewett TE. The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position. J Electromyogr Kinesiol. 2005;15(2):181–9.
Padua DA, Carcia CR, Arnold BL, Granata KP. Gender differences in leg stiffness and stiffness recruitment strategy during two-legged hopping. J Mot Behav. 2005;37(2):111–25.
Benjaminse A, Gokeler A, Fleisig GS, Sell TC, Otten B. What is the true evidence for gender-related differences during plant and cut maneuvers? a systematic review. Knee Surg Sports Traumatol Arthrosc. 2011;19(1):42–54.
Hannah R, Folland JP, Smith SL, Minshull C. Explosive hamstrings-to-quadriceps force ratio of males versus females. Eur J Appl Physiol. 2015;115(4):837–47.
Nimphius S, McBride JM, Rice PE, Goodman-Capps CL, Capps CR. Comparison of quadriceps and hamstring muscle activity during an isometric squat between strength-matched men and women. J Sports Sci Med. 2019;18(1):101–8.
Page M, McKenzie J, Bossuyt P, Boutron I, Hoffmann T, Mulrow C, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. 2009;62(10):e1-34.
Morgana R, Whaleyb P, Thayerc K, Schünemanna H. Identifying the PECO: a framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ Int. 2018;121(Pt 1):1027–31.
Nordhausen T, Hirt J. Manual zur Literaturrecherche in Fachdatenbanken, RefHunter, Version 4.0., retrieved on 31.01.2020 from https://refhunter.eu/. 2020.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
NHLBI. National Heart, Lung, and Blood Institute; National Institutes of Health; U.S. Department of Health and Human Services; retrieved on 11.02.2021 from https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. 2021.
Bencke J, Zebis MK. The influence of gender on neuromuscular pre-activity during side-cutting. J Electromyogr Kinesiol. 2011;21(2):371–5.
DeMont RG, Lephart SM. Effect of sex on preactivation of the gastrocnemius and hamstring muscles. Br J Sports Med. 2004;38(2):120–4.
Deschenes MR, McCoy RW, Holdren AN, Eason MK. Gender influences neuromuscular adaptations to muscle unloading. Eur J Appl Physiol. 2009;105(6):889–97.
Hart JM, Garrison JC, Kerrigan DC, Palmieri-Smith R, Ingersoll CD. Gender differences in gluteus medius muscle activity exist in soccer players performing a forward jump. Res Sports Med. 2007;15(2):147–55.
Kim AS, Needle AR, Thomas SJ, Higginson CI, Kaminski TW, Swanik CB. A sex comparison of reactive knee stiffness regulation strategies under cognitive loads. Clin Biomech (Bristol, Avon). 2016;35:86–92.
Lee SJ, Ren Y, Kang SH, Geiger F, Zhang LQ. Pivoting neuromuscular control and proprioception in females and males. Eur J Appl Physiol. 2015;115(4):775–84.
Palmieri-Smith RM, Wojtys EM, Ashton-Miller JA, Palmieri-Smith RM, Wojtys EM, Ashton-Miller JA. Association between preparatory muscle activation and peak valgus knee angle. J Electromyogr Kinesiol. 2007;18(6):973–9.
Rozzi SL, Lephart SM, Gear WS, Fu FH. Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med. 1999;27(3):312–9.
Smith MP, Sizer PS, James CR. Effects of fatigue on frontal plane knee motion, muscle activity, and ground reaction forces in men and women during landing. J Sports Sci Med. 2009;8(3):419–27.
Wu R, Delahunt E, Ditroilo M, Lowery M, De Vito G. Effects of age and sex on neuromuscular-mechanical determinants of muscle strength. Age (Dordr). 2016;38(3):57.
Altman DG. Practical Statistics for Medical Research. London: Chapman & Hall; 1991.
Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, N.J: L. Erlbaum Associates. 1988.
Cumpston M LT, Chandler J, Page MJ. Chapter III: Reporting the review. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.3 (updated February 2022). 2022.
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84.
Jarde A, Losilla JM, Vives J. Methodological quality assessment tools of non-experimental studies: a systematic review. Aanales de Psicología. 2012;28:617–28.
Ma LL, Wang YY, Yang ZH, Huang D, Weng H, Zeng XT. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil Med Res. 2020;7(1):7.
Carbia C, López-Caneda E, Corral M, Cadaveira F. A systematic review of neuropsychological studies involving young binge drinkers. Neurosci Biobehav Rev. 2018;90:332–49.
Oliva-Lozano JM, Muyor JM. Core muscle activity during physical fitness exercises: a systematic review. Int J Environ Res Public Health. 2020;17(12):4306.
Martin-Fuentes I, Oliva-Lozano JM, Muyor JM. Electromyographic activity in deadlift exercise and its variants. a systematic review. PLoS One. 2020;15(2):e0229507.
Beunen G, Malina R. Growth and physical performance relative to the timing of the adolescent spurt. Exerc Sport Sci Rev. 1988;16:503–40.
Medina JM, Valovich McLeod TC, Howell SK, Kingma JJ. Timing of neuromuscular activation of the quadriceps and hamstrings prior to landing in high school male athletes, female athletes, and female non-athletes. J Electromyogr Kinesiol. 2008;18(4):591–7.
Blasimann A, Koenig I, Baert I, Baur H, Vissers D. Which assessments are used to analyze neuromuscular control by electromyography after an anterior cruciate ligament injury to determine readiness to return to sports? a systematic review. BMC Sports Sci Med Rehabil. 2021;13(1):142.
Baur H, Hirschmüller A, Cassel M, Müller S, Mayer F. Gender-specific neuromuscular activity of the M. peroneus longus in healthy runners - a descriptive laboratory study. Clin Biomech (Bristol, Avon). 2010;25(9):938–43.
Baur H, Müller S, Hirschmüller A, Cassel M, Weber J, Mayer F. Comparison in lower leg neuromuscular activity between runners with unilateral mid-portion Achilles tendinopathy and healthy individuals. J Electromyogr Kinesiol. 2011;21:499–505.
Alentorn-Geli E, Myer GD, Silvers HJ, Samitier G, Romero D, Lazaro-Haro C, et al. Prevention of non-contact anterior cruciate ligament injuries in soccer players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surg Sports Traumatol Arthrosc. 2009;17(7):705–29.
Zeller BL, McCrory JL, Kibler WB, Uhl TL. Differences in kinematics and electromyographic activity between men and women during the single-legged squat. Am J Sports Med. 2003;31(3):449–56.
Nordander C, Willner J, Hansson GA, Larsson B, Unge J, Granquist L, et al. Influence of the subcutaneous fat layer, as measured by ultrasound, skinfold calipers and BMI, on the EMG amplitude. Eur J Appl Physiol. 2003;89(6):514–9.
Acknowledgements
This systematic review was completed as a result of the invaluable support of the dedicated contributors. We thank the librarian of the Bern University of Applied Sciences for the support during the development of the search strategy. Further, we want to thank everyone who supported the finalisation by proofreading the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to all of the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted. MS acted as the first researcher and developed the search strategy, conducted the data search, analysed / interpreted the data, and wrote the manuscript. AB acted as the second researcher in the study selection step and collaborated on data interpretation. HB was consulted during the study selection process in case of ambiguities and collaborated on data interpretation. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The requirements for authorship have been met and there is no financial or other relationship that might lead to a conflict of interest. All authors – Martina Steiner (MS), Angela Blasimann (AB), Heiner Baur (HB) – declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Steiner, M., Baur, H. & Blasimann, A. Sex-specific differences in neuromuscular activation of the knee stabilizing muscles in adults - a systematic review. Arch Physiother 13, 4 (2023). https://doi.org/10.1186/s40945-022-00158-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40945-022-00158-x