
Abstract
Background
The relationship between the lateral deviation of chin and the upper and middle facial third asymmetry is still controversial. The purpose of this study is to evaluate the correlation of upper and middle facial third asymmetry with lateral deviation of chin using 3-dimensional computed tomography. The study was conducted on patients who underwent orthognathic surgery from January 2016 to August 2017. A total of 40 patients were included in this retrospective study. A spiral scanner was used to obtain the 3-dimensional computed tomography scans. The landmarks were assigned on the reconstructed 3-dimensional images, and their locations were verified on the axial, midsagittal, and coronal slices. The Pearson correlation analysis was performed to evaluate the correlation between chin deviation and difference between the measurements of distances in paired craniofacial structures. Statistical analysis was performed at a significance level of 5%.
Results
In mandible, the degree of chin deviation was correlated with the mandibular length and mandibular body length. Mandibular length and mandibular body length are shorter on the deviated-chin side compared to that on the non-deviated side (mandibular length, r = −0.897, p value < 0.001; mandibular body length, r = −0.318, p value = 0.045). In the upper and middle facial thirds, the degree of chin deviation was correlated with the vertical asymmetry of the glenoid fossa and zygonion. Glenoid fossa and zygonion are superior on the deviated-chin side than on the non-deviated side (glenoid fossa, r = 0.317, p value = 0.046; zygonion, r = 0.357, p value = 0.024).
Conclusion
Lateral deviation of chin is correlated with upper and middle facial third asymmetry as well as lower facial third asymmetry. As a result, treatment planning in patients with chin deviation should involve a careful evaluation of the asymmetry of the upper and middle facial thirds to ensure complete patient satisfaction.
Similar content being viewed by others

Background
Facial asymmetry is a relatively common feature with a prevalence rate of 21–85%. In majority of cases, facial asymmetry is mild and hardly recognizable, and hence, surgical intervention is not usually necessary [1,2,3,4]. However, patients with apparent facial asymmetry may not be satisfied with their appearance; such patients are more likely to opt for surgical intervention for esthetic and occlusal improvement [3].
The most common type of facial asymmetry is observed in the lower third of face with lateral deviation of the chin (75%) [3]. The most common cause is unilateral mandibular hyperplasia, i.e., enlargement of the mandible [5]. Functional disharmony of the masticatory muscles may be associated with lower facial third asymmetry with lateral deviation of chin [6].
Facial asymmetry often involves varying degrees of upper (5%) and middle (36%) facial third asymmetries [3]. In a previous study, asymmetry of the glenoid cavity, a type of upper and middle facial third asymmetry, was reported [7]. Asymmetry of the glenoid cavity is caused by defects in generation, proliferation, migration, and differentiation of cranial neural crest cells [8] or craniofacial structure modeling from the cerebrum [9,10,11]. As a result, asymmetry of the glenoid cavity causes lateral deviation of the chin [7].
The relationship between the lateral deviation of chin and the upper and middle facial third asymmetry is still controversial. López Buitrago et al. reported lateral deviation of chin is associated with upper and middle facial third asymmetry, while Kwon et al. reported lateral deviation of chin is not closely related with upper and middle facial third asymmetry [7, 12].The purpose of this study was to evaluate the correlation of upper and middle facial third asymmetry with lateral deviation of chin using 3-dimensional computed tomography (3-D CT).
Methods
Patients
The study was conducted on patients who underwent orthognathic surgery at the Department of Oral and Maxillofacial surgery, Gangnam Severance Hospital, Seoul, Korea, between January 2016 and August 2017. Patients with (1) history of trauma to the jaw and (2) congenital deformities, such as cleft lip and/or palate, were excluded from this study. Finally, 40 patients (18 males and 22 females; mean age, 25.50 years [range, 19 to 42]) were included this retrospective study. This study was approved by Gangnam Severance Hospital Institutional Review Board (Approval No. 3-2019-0119)
Image acquisition and analysis
A spiral scanner was used for 3-D CT scans advised before orthognathic surgery for pre-surgical evaluation. (SOMATOM sensation 64; Siemens, Erlangen, Germany). During the process of CT scan, the patient’s teeth were maintained in centric occlusion, and the scan was obtained with following settings: gantry angle of 0°, 1024 × 1024 matrix, 120 kV, 90 mA, 1.0 mm slice thickness, and 0.5 sec gantry rotation time. The CT analysis software was used to reconstruct the digital imaging and communication in medicine (DICOM) images into 3-D images (Mimics version 23.0; Materalise Dental, Leuven, Belgium).
3-dimensional reference plane and craniofacial landmarks
Landmarks were assigned on the reconstructed 3-D image, and their locations were verified on the axial, midsagittal, and coronal slices. The landmarks and measurements of the craniofacial structures to be performed were selected with reference to previous studies [12, 13]. The various landmarks studies are summarized in Figs. 1, 2 and Table 1.

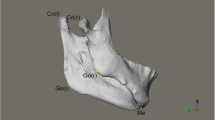
Three-dimensional reference planes and craniofacial landmarks. Cr, crista galli; Cl, clinoid process; Op, opisthion; Po, porion; Me, menton; Go, gonion; Gf, glenoid fossa; Or, orbitale; Zy, zygonion

Computed tomography (CT) scans of craniofacial landmarks. Cr, crista galli; Cl, clinoid process; Op, opisthion; MSP, midsagittal plane; CoP, coronal plane
To determine the standard orientation, 3-D reference planes were initially located. The axial plane (AxP) was defined as a plane including the porion (Po) on both sides and the left orbitale (OrL). The midsagittal plane (MSP) was defined as a plane perpendicular to the AxP, including the crista galli (Cr) and the midpoint of the anterior clinoid process (Cl). The coronal plane (CoP) was defined as a plane perpendicular to the AxP and the MSP passing through opisthion (Op).
Craniofacial measurements
The craniofacial measurements performed in the study are summarized in Table 2. Distance between the menton (Me) and MSP was defined as dMe, for convenience of comparison; (+) indicated right side deviation of menton. In the mandible, distance from the condylar superius (Con) to Me, distance from gonion (Go) to Me, and the distance from Con to Go were defined as mandibular length (dML), mandibular body length (dMBL), and ramal height (dRH), respectively. Distance from glenoid fossa (Gf) to MSP, CoP and AxP was defined as dGfx, dGfy, and dGfz, respectively. Distance from orbitale (Or) and zygonion (Zy) to each plane was defined as the same way.
Differences between the measurements of distances in the paired craniofacial structures are given in Table 3. (R-L) was the mean difference between the measurements of distances in the paired craniofacial structures. (R-L) from MSP, CoP, and AxP was defined as x(R-L), y(R-L), and z(R-L). A positive value of x(R-L) indicates that the right craniofacial structure is more lateral than the left craniofacial structure from MSP, positive value of y(R-L) indicates that the right craniofacial structure is more anterior than the left craniofacial structure from CoP, and positive value of z(R-L) indicates that the right craniofacial structure is more superior than the left craniofacial structure from AxP. The relationship between the measurements of distances in the paired craniofacial structures and chin deviation was studied.
Statistical analysis
To avoid inter-observer errors in measurements, all the measurements were performed by a single observer. The Pearson’s correlation analysis was performed to evaluate the correlation between chin deviation and difference between the measurements of distances in paired craniofacial structures. Statistical analysis was performed at a significance level of 5% with SPSS version 25.0 (IBM Corp, Armonk, NY, USA).
The intraclass correlation coefficient was used to evaluate intra-observer error by the same observer 1 week apart. In this study, the second set of measurements was used.
Results
Study subjects
The characteristics of patients included in the study are summarized in Table 4. A total of 40 patients (18 males and 22 females; mean age, 25.50 years [range, 19 to 42]) were included in this study. In our study, 18 patients (45%) showed chin deviation to the right side, and 22 patients (55%) showed chin deviation to the left side (mean, −1.82 mm [range, −16.44 mm to 8.44 mm]), and (+) indicates right side deviation of menton. Of the 40 patients, skeletal class III, class II, and class I malocclusions were evident in 33, 3, and 4 patients, as determined by lateral cephalograms.
The intraclass correlation coefficients of craniofacial distance measurements are shown in Table 5. The intraclass correlation coefficient ranged from 0.91 to 0.99, which showed that data from one observer were very reliable.
The correlation between chin deviation and difference between the measurements of distances in paired lower facial third structures
The correlation between chin deviation and difference between the measurements of distances in paired lower facial third structures is shown in Table 6. In the lower facial thirds, the degree of chin deviation was related to mandibular length and mandibular body length. Mandibular length and mandibular body length are shorter on the deviated-chin side compared to that on the non-deviated side (mandibular length, r = − 0.897, value < 0.001; mandibular body length, r = − 0.318, p value = 0.045). However, no significant relation was observed between the degree of chin deviation and ramal height.
The correlation between chin deviation and difference between the measurements of distances in paired upper and middle facial third structures
The correlation between chin deviation and difference between the measurements of distances in paired upper and middle facial third structures is shown in Table 7. In the upper and middle facial thirds, the degree of chin deviation was correlated with the vertical asymmetry of glenoid fossa and zygonion. Glenoid fossa and zygonion were superior on the deviated-chin side compared to that on the non-deviated side (glenoid fossa, r = 0.317, p value = 0.046; zygonion, r = 0.357, p value = 0.024). However, no significant relation was observed between the degree of chin deviation and position of orbitale.
Discussion
The purpose of this study was to evaluate the correlation between upper and middle facial third asymmetry and lateral deviation of chin using 3-D CT.
Traditionally, posteroanterior cephalograms, submentovertex view radiographs, or frontal facial photos have been used for diagnosing facial asymmetry. Certainly, these diagnostic modalities have proven their worth over the years. However, they have limited diagnostic abilities due to problems related to magnification, distortion, and superimposition of craniofacial structures [14,15,16,17]. However, 3-D CT reduces errors due to magnification and distortion and allows the quantitative measurements of craniofacial structures [18,19,20].
Currently, the external auditory meatus is regarded as a reliable reference for the analysis of craniofacial characteristics because of its stable shape [21]. Previous 3-D studies use the Frankfort’s horizontal plane as the reference axial plane [22,23,24]. For these reasons, in this study, the Frankfort’s horizontal plane passing through bilateral porion and left orbitale was used as the axial plane. Then, a plane perpendicular to the axial plane passing through the crita galli (Cr) and the midpoint between the anterior clinoid processes (Cl) was defined as midsagittal plane [12]. A plane perpendicular to axial and midsagittal plane with passing through opisthion (Op) was defined as a coronal plane based on the study of Kwon et al .[12].
The glenoid fossa is a depression in the temporal bone that articulates with the mandible to form the temporomandibular joint [25]. Positional changes in the glenoid fossa during growth can lead to facial asymmetry and malocclusion [7]. The location of the orbit and zygomatic bone plays an important role in facial symmetry and esthetics [26, 27]. For these reasons, the glenoid fossa, orbitale, and zygomatic arch were analyzed in this study. Mandibular length, mandibular body length, and ramal height were also analyzed to evaluate lower facial third asymmetry.
In the lower facial thirds, chin deviation is correlated with mandibular length and mandibular body length asymmetry, coincident with the findings of previous studies [12, 21, 28]. Moreover, in our study, chin deviation was also correlated with the upper and middle facial third asymmetry, especially vertical asymmetry of the glenoid fossa and zygomatic arch, coincident with the findings of another stud y[7]. In a previous study, asymmetry of the glenoid cavity, a type of upper and middle facial third asymmetry, was reported [7]. The asymmetry of glenoid cavity is often caused by the defects in generation, proliferation, migration, and differentiation of cranial neural crest cells [8] or craniofacial structure modeling from the cerebrum [9,10,11]. As a result, the glenoid cavity is located superiorly where developmental defects occurred (affected side) [7]. Similarly, supraorbital arch, zygomatic bone, and external auditory meatus are also located superiorly on affected side (orbiculo-zygomatic-meatal and articular asymmetry) [7]. Finally, the asymmetry of glenoid cavity functionally affects condylar position, causing lateral deviation of chin to the affected side [7].
This study showed that lateral deviation of chin is correlated with upper and middle facial third asymmetry as well as lower facial third asymmetry, especially vertical asymmetry of the glenoid fossa and zygomatic arch. Correction of chin deviation by mandibular surgery alone will not correct the asymmetry of the upper and middle facial thirds.
A limitation of this study is that a small number of craniofacial landmarks were analyzed for the correlation with the lateral deviation of chin, and further studies incorporating more number of craniofacial landmarks should be conducted for a deeper understanding of the correlation between the lateral deviation of chin and craniofacial landmarks.
To be best of our knowledge, this is the first study to evaluate craniofacial characteristics associated with the lateral deviation of chin using 3-dimensional imaging modalities. Considering the high prevalence and the impact of facial asymmetry on patient’s treatment outcome, this study is very relevant in the present scenario. Knowledge about the fact that facial symmetry is influenced by the upper and middle thirds of face will help clinicians around the world in proper treatment planning and hence, in providing better treatment to such patients.
Conclusions
Lateral deviation of chin is correlated with upper and middle facial third asymmetry as well as lower facial third asymmetry. Correction of chin deviation by mandibular surgery alone will not correct the asymmetry of the upper and middle facial thirds. As a result, treatment planning in patients with chin deviation should involve a careful evaluation of the asymmetry of the upper and middle facial thirds to ensure complete patient satisfaction.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- (R-L):
-
Difference between the measurements of distances in paired craniofacial structures (right–left)
- 3-D CT:
-
3-dimensional computed tomography
- AxP:
-
Axial plane
- Cl:
-
Clinoid process
- Con:
-
Condylar superius
- ConL:
-
Left condylar superius
- ConR:
-
Right condylar superius
- CoP:
-
Coronal plane
- Cr:
-
Crista galli
- dGfx:
-
Distance from Gf to midsagittal plane
- dGfx(R-L):
-
dGfxR–dGfxL
- dGfxL:
-
Left dGfx
- dGfxR:
-
Right dGfx
- dGfy:
-
Distance from Gf to coronal plane
- dGfy(R-L):
-
dGfyR–dGfyL
- dGfyL:
-
Left dGfy
- dGfyR:
-
Right dGfy
- dGfz:
-
Distance from Gf to axial plane
- dGfz(R-L):
-
dGfzR–dGfzL
- dGfzL:
-
Left dGfz
- dGfzR:
-
Right dGfz
- DICOM:
-
Digital imaging and communication in medicine
- dMBL:
-
Mandibular body length, distance from Go to Me
- dMBL(R-L):
-
dMBLR–dMBLL
- dMe:
-
Distance from Me to midsagittal plane
- dML:
-
Mandibular length, distance from Con to Me
- dML(R-L):
-
dMLR–dMLL
- dOrx:
-
Distance from Or to midsagittal plane
- dOrx(R-L):
-
dOrxR–dOrxL
- dOrxL:
-
Left dOrx
- dOrxR:
-
Right dOrx
- dOry:
-
Distance from Or to coronal plane
- dOry(R-L):
-
dOryR–dOryL
- dOryL:
-
Left dOry
- dOryR:
-
Right dOry
- dOrz:
-
Distance from Or to axial plane
- dOrz(R-L):
-
dOrzR–dOrzL
- dOrzL:
-
Left dOrz
- dOrzR:
-
Right dOrz
- dRH:
-
Ramal height, distance from Con to Go
- dRH(R-L):
-
dRHR–dRHL
- dZyx:
-
Distance from Zy to midsagittal plane
- dZyx(R-L):
-
dZyxR–dZyxL
- dZyxL:
-
Left dZyx
- dZyxR:
-
Right dZyx
- dZyy:
-
Distance from Zy to coronal plane
- dZyy(R-L):
-
dZyyR–dZyyL
- dZyyL:
-
Left dZyy
- dZyyR:
-
Right dZyy
- dZyz(R-L):
-
dZyzR–dZyzL
- dZyz:
-
Distance from Zy to axial plane
- dZyzL:
-
Left dZyz
- dZyzR:
-
Right dZyz
- Gf:
-
Glenoid fossa
- GfL:
-
Left glenoid fossa
- GfR:
-
Right glenoid fossa
- Go:
-
Gonion
- GoL:
-
Left gonion
- GoR:
-
Right gonion
- Me:
-
Renton
- MSP:
-
Midsagittal plane
- Op:
-
Opithion
- Or:
-
Orbitale
- OrL:
-
Left orbitale
- OrR:
-
Right orbitale
- Po:
-
Porion
- PoL:
-
Left porion
- PoR:
-
Right porion
- x(R-L):
-
Difference between the measurements of distances in paired craniofacial structures from MSP
- y(R-L):
-
Difference between the measurements of distances in paired craniofacial structures from CoP
- z(R-L):
-
Difference between the measurements of distances in paired craniofacial structures from AxP
- Zy:
-
Zygonion
- ZyL:
-
Left zygonion
- ZyR:
-
Right zygonion
References
Haraguchi S, Takada K, Yasuda Y (2002) Facial asymmetry in subjects with skeletal class III deformity. Angle Orthod 72:28–35
Samman N, Tong AC, Cheung DL, Tideman H (1992) Analysis of 300 dentofacial deformities in Hong Kong. Int J Adult Orthodon Orthognath Surg 7:181–185
Severt TR, Proffit WR (1997) The prevalence of facial asymmetry in the dentofacial deformities population at the University of North Carolina. Int J Adult Orthodon Orthognath Surg 12:171–176
Burstone CJ (1998) Diagnosis and treatment planning of patients with asymmetries. Semin Orthod 4:153–164
Obwegeser HL, Makek MS (1986) Hemimandibular hyperplasia--hemimandibular elongation. J Maxillofac Surg 14:183–208
Poikela A, Kantomaa T, Pirttiniemi P (1997) Craniofacial growth after a period of unilateral masticatory function in young rabbits. Eur J Oral Sci 105:331–337
López Buitrago DF, Ruiz Botero J (2017) Asymmetry of glenoid fossa as differential diagnosis for hemimandibular elongation. Revista Mexicana de Ortodoncia 5:e217–ee26
Minoux M, Rijli FM (2010) Molecular mechanisms of cranial neural crest cell migration and patterning in craniofacial development. Development 137:2605–2621
de Cráneo AdlB, el Crecimiento D (2011) Asymmetry of human skull base during growth. Int J Morphol 29:1028-1032.
Basili C, Costa H, Sasaguri K, Akimoto S, Slavicek R, Sato S (2009) Comparison of the position of the mandibular fossa using 3D CBCT in different skeletal frames in human caucasic skulls. Int J Stomatol Occlusion Med 2:179–190
Slavicek R (2001) The dynamic functional anatomy of craniofacial complex and its relation to the articulation of the dentitions. Das Kauorgan Funktione und Dysfunktionen:482–514
Kwon TG, Park HS, Ryoo HM, Lee SH (2006) A comparison of craniofacial morphology in patients with and without facial asymmetry-a three-dimensional analysis with computed tomography. Int J Oral Maxillofac Surg 35:43–48
You KH, Lee KJ, Lee SH, Baik HS (2010) Three-dimensional computed tomography analysis of mandibular morphology in patients with facial asymmetry and mandibular prognathism. Am J Orthod Dentofacial Orthop 138:540.e1–540.e8 discussion -1
Ahlqvist J, Eliasson S, Welander U (1983) The cephalometric projection. part II. principles of image distortion in cephalography. Dentomaxillofac Radiol 12:101–108
Bergersen EO (1980) Enlargement and distortion in cephalometric radiography: compensation tables for linear measurements. Angle Orthod 50:230–244
Gravely JF, Benzies PM (1974) The clinical significance of tracing error in cephalometry. Br J Orthod 1:95–101
Savara BS, Tracy WE, Miller PA (1966) Analysis of errors in cephalometric measurements of three-dimensional distances on the mandible. Arch Oral Biol 11:209–217
Fuhrmann RA, Schnappauf A, Diedrich PR (1995) Three-dimensional imaging of craniomaxillofacial structures with a standard personal computer. Dentomaxillofac Radiol 24:260–263
Katsumata A, Fujishita M, Maeda M, Ariji Y, Ariji E, Langlais RP (2005) 3D-CT evaluation of facial asymmetry. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 99:212–220
Xia J, Ip HH, Samman N, Wang D, Kot CS, Yeung RW et al (2000) Computer-assisted three-dimensional surgical planning and simulation: 3D virtual osteotomy. Int J Oral Maxillofac Surg 29:11–17
Kim YH, Sato K, Mitani H, Shimizu Y, Kikuchi M (2003) Asymmetry of the sphenoid bone and its suitability as a reference for analyzing craniofacial asymmetry. Am J Orthod Dentofacial Orthop 124:656–662
Captier G, Leboucq N, Bigorre M, Canovas F, Bonnel F, Bonnafe A et al (2003) Plagiocephaly: morphometry of skull base asymmetry. Surg Radiol Anat 25:226–233
Lo LJ, Marsh JL, Pilgram TK, Vannier MW (1996) Plagiocephaly: differential diagnosis based on endocranial morphology. Plast Reconstr Surg 97:282–291
Yu CC, Wong FH, Lo LJ, Chen YR (2004) Craniofacial deformity in patients with uncorrected congenital muscular torticollis: an assessment from three-dimensional computed tomography imaging. Plast Reconstr Surg 113:24–33
Sato S, Takamoto K, Fushima K, Akimoto S, Suzuki Y (1989) A new orthodontic approach to mandibular lateral displacement malocclusion-importance of occlusal plane reconstruction. Dent Jpn 26:81–85
Springer IN, Wannicke B, Warnke PH, Zernial O, Wiltfang J, Russo PA et al (2007) Facial attractiveness: visual impact of symmetry increases significantly towards the midline. Ann Plast Surg 59:156–162
Khaqani MS, Tavosi F, Gholami M, Eftekharian HR, Khojastepour L (2018) Analysis of facial symmetry after zygomatic bone fracture management. J Oral Maxillofac Surg 76:595–604
Baek C, Paeng JY, Lee JS, Hong J (2012) Morphologic evaluation and classification of facial asymmetry using 3-dimensional computed tomography. J Oral Maxillofac Surg 70:1161–1169
Acknowledgements
We would like to thank Editage (www.editage.co.kr) for English language editing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for profit sectors.
Author information
Authors and Affiliations
Contributions
HWC and BK were responsible for collecting and analyzing the data. JYK was responsible for statistical analysis and translation of the data. KHP and JKH contributed to the direction and design of the research and contributed to the review of the paper. All the authors have read the final version of the paper and have agreed to its publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by Gangnam Severance Hospital Institutional Review Board (Approval No. 3-2019-0119).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
CHOI, HW., KIM, B., KIM, JY. et al. Three-dimensional computed tomography evaluation of craniofacial characteristics according to lateral deviation of chin. Maxillofac Plast Reconstr Surg 41, 57 (2019). https://doi.org/10.1186/s40902-019-0241-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40902-019-0241-1