
Abstract
Background
Using the technique of co-production to develop research is considered good practice. Co-production involves the public, practitioners and academics working together as equals throughout a research project. Co-production may help develop alternative ways of delivering care for older adults that are acceptable to those who live and work in care homes. However, guidance about applying co-production approaches in this context is lacking. This scoping review aims to map co-production approaches used in care homes for older adults in previous research to support the inclusion of residents and care staff as equal collaborators in future studies.
Methods
A scoping review was conducted using the Joanna Briggs Institute scoping review methodology. Seven electronic databases were searched for peer-reviewed primary studies using co-production approaches in care home settings for older adults. Studies were independently screened against eligibility criteria by two reviewers. Citation searching was completed. Data relating to study characteristics, co-production approaches used, including any barriers and facilitators, was charted by one reviewer and checked by another. Data was summarised using tables and diagrams with an accompanying narrative description. A collaborator group of care home and health service representatives were involved in the interpretation of the findings from their perspectives.
Results
19 studies were selected for inclusion. A diverse range of approaches to co-production and engaging key stakeholders in care home settings were identified. 11 studies reported barriers and 13 reported facilitators affecting the co-production process. Barriers and facilitators to building relationships and achieving inclusive, equitable and reciprocal co-production were identified in alignment with the five NIHR principles. Practical considerations were also identified as potential barriers and facilitators.
Conclusion
The components of co-production approaches, barriers and facilitators identified should inform the design of future research using co-production approaches in care homes. Future studies should be explicit in reporting what is meant by co-production, the methods used to support co-production, and steps taken to enact the principles of co-production. Sharing of key learning is required to support this field to develop. Evaluation of co-production approaches, including participants’ experiences of taking part in co-production processes, are areas for future research in care home settings.
Plain English Summary
Co-production involves people from different backgrounds working together as equals throughout a research project. Co-production may be a useful approach to help ensure that research in care homes focuses on approaches that are important and agreeable to older people and staff. A wide range of research and guidance about co-production has been published but there is limited guidance about how to do co-production in care homes. We carried out a review that involved pulling together previous research that used co-production in care homes for older adults. We looked at published research studies to learn about:
-
Key components of the strategies used to achieve co-production,
-
How care home residents and care home staff were involved,
-
What helped or made co-production difficult to achieve.
A collaborator group including representatives from care homes and healthcare services were involved in this research. They helped decide what was most important about the results.
We found 19 published research articles that used co-production in care homes. The strategies used in the articles differed. There were also differences in how care home residents and staff were involved in co-production. Factors that helped people involved to work together in an inclusive and equal way were identified. At the same time, there were also many challenges.
These results should be used to design future research using co-production in care homes. Future studies should clearly report what is meant by co-production, the strategies used and key learning points. Evaluation of co-production and the experiences of people involved is needed.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Many definitions of co-production exist and how the term is used often depends on a combination of factors, including the field in which it is applied, what is being produced, and the individuals and organisations involved [1, 2]. In this review, we consider co-production in health and social care research to be the involvement of service users, professionals and academics working together in equal partnership and sharing responsibility for generating knowledge and solutions to problems [3, 4]. Overarching guiding principles of co-production, such as power sharing, inclusivity, equality and reciprocity, have been developed; however, limited guidance based on empirical evidence is available regarding the practicalities of using co-production approaches in social care settings [3, 5, 6].
There is overlap between co-production and other terms, such as co-creation and co-design. These terms have originated from different fields and there are various lines of thought about whether they mean the same thing, or reflect different levels or types of involvement; however, it is generally accepted that all three terms involve the collaborative participation of multiple stakeholders in any or all stages of research [2, 7, 8]. Recent reviews have found co-methodologies have become increasingly popular over the last decade but there is variation in how such approaches are described and operationalised in health research [5, 9, 10]. Very few of the studies included in these reviews were conducted in social care settings such as care homes.
In the United Kingdom (UK), approximately 410,000 people live in care homes, many of whom are older adults with multiple health conditions and complex care needs, and demand is expected to increase due to the ageing population [11, 12]. Care homes also differ organisationally for many reasons, such as their ownership and commissioning arrangements, size, specialisms and culture [13]. Consequently, delivery of care in each unique care home setting requires a broad range of expertise and collaboration between stakeholders across numerous sectors in order to meet the individual needs and preferences of older care home residents [12].
By attending to these unique contextual factors, and harnessing the collective expertise and experiences of all stakeholders in care home settings, co-production research approaches may be more likely to be implemented and incorporated into routine practices in care homes [14]. However, achieving authentic co-production in alignment with its principles may be challenging and is likely to be influenced by many factors such as power relationships, social and cultural norms, and conflicting expectations and priorities. For instance, previous research has identified that patients accessing health services, the public and NHS staff perceived old age and poor health, both common characteristics of care home residents, as potential barriers to co-production [15]. This study did not appear to include care home staff or residents as participants. Barriers and facilitators to involving care home residents as Patient and Public Involvement (PPI) members in research have been identified, including social factors, organisational factors, skills and resources [16]. However, it is unclear whether the same factors would apply to co-production of research and whether there would be different factors to consider for involving other stakeholders, such as care home staff.
While co-production has been used in care homes in primary studies [17, 18], no reviews to date have focussed specifically on mapping the use of co-production in care home settings (to our knowledge). The aim of this scoping review is to map co-production approaches used in care homes for older adults to inform the design of future co-production research. The review sought to address the following questions:
-
What co-production approaches have been used in care home settings for older adults?
-
What are the key components of co-production approaches used in this context?
-
What approaches were used to engage older residents and care home staff in the process?
-
What barriers and facilitators to achieving co-production were reported?
Methods
The review was undertaken following the Joanna Briggs Institute (JBI) scoping review methodology [19]. Protocol development and reporting was guided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist (Additional file 1) [20]. The protocol is published on the Open Science Framework [21].
Search strategy
Eligibility criteria were developed using the Population, Concept, Context (PCC) framework and are outlined in Table 1 [19]. In this review, co-production was viewed as an umbrella term for describing stakeholders working together in equal partnership. We therefore included studies using co-production, co-creation or co-design as these terms are often used indiscriminately [7, 10].
A comprehensive three-stage search strategy was conducted. Initial searches of MEDLINE and EMBASE were completed with advice from an information specialist at the University of Nottingham. Titles, abstracts and key terms from relevant texts identified through initial searching were analysed and used to create a tailored strategy for each information source based on variations of the following key concepts: older adults, co-production and care homes. An example search strategy is included in Additional file 2. A second search was completed in the following health and social care research databases on the 20th December 2021: AMED, ASSIA, CINAHL, EMBASE, MEDLINE, PsychInfo, Social Care Online. Thirdly, forwards and backwards citation searching of studies meeting the eligibility criteria was completed using Web of Science. Retrieved studies were imported into an EndNote X9 library.
Study selection
Duplicates were removed using EndNote. Titles and abstracts were independently screened against the eligibility criteria by two reviewers (FHB, KR) using Rayyan [22]. Studies which used participatory research methods but did not explicitly state using co-production, co-creation or co-design in the abstract were included at this stage, as were studies which included terms with similar connotations to co-production (for instance, civil engagement, altruistic action) to minimise the risk of excluding relevant studies. Full texts were then screened independently by both reviewers and only included if use of co-production, co-creation or co-design was explicitly reported. Differences were resolved through discussion between the reviewers. Reasons for exclusion were recorded.
Data charting
Data relating to co-production approaches used, involvement of key stakeholders, barriers and facilitators to achieving co-production reported in results or discussion sections, and key study characteristics were extracted from included studies. A data charting table (Additional file 3) was developed from a co-creation reporting checklist [26]. The checklist was used based on reviewers’ experiences of piloting the draft data charting table on five studies. Piloting was completed by two reviewers who found it difficult to systematically extract relevant data due to the heterogeneity of the approaches used across the studies. The co-creation checklist therefore helped to refine the structure and support a standardised approach to data charting [23]. For all included studies, one reviewer charted relevant data (FHB) and another checked the charted data for accuracy (KR). Discrepancies were resolved through discussion between the reviewers.
Summarising and presenting findings
A PRISMA flow diagram was used to record the study selection process (Fig. 1) [24]. A narrative summary with accompanying tables and diagrams was developed to describe study characteristics, the co-production approaches used, their key components, and how care home staff and residents were involved. Reported barriers and facilitators to co-production were mapped against the NIHR principles of co-production [3] using a deductive, thematic analysis approach. The principles were originally developed by NIHR INVOLVE which is now part of the NIHR Centre for Engagement and Dissemination. Using an iterative approach, one reviewer (FHB) grouped barriers and facilitators from the included studies into themes based on similarity in meaning under the co-production principles. An “other” category was used for any factors that fell outside this framework. The themes and their placement under the co-production principles were then reviewed and revised by the second reviewer (KR), and finalised through discussion with the wider research team (PL, ST).

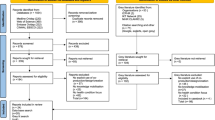
PRISMA flow diagram of the search strategy [24].
In keeping with the JBI scoping review methodology, studies were not critically appraised as the review was not intended to guide the selection of interventions for use in clinical practice [19, 25]. A collaborator group including care home, patient and public, and health care representatives were involved in decision-making about presentation of findings and their implications for future research. The group’s contribution to the review is reported using the GRIPP2 Short Form [26] in Additional file 4.
Results
Study selection
The process for identifying eligible studies is outlined in Fig. 1. Database searching yielded 983 records. After removal of 124 duplicates, titles and abstracts of 859 records were reviewed against the eligibility criteria. Of these, 85 were eligible for full text screening. Of the 83 that could be accessed, 19 were included in the review. Reasons for exclusion at the full text screening stage are provided in Fig. 1. No further studies were identified from forward and backwards citation searching.
Characteristics of included studies
Table 2 summarises the key characteristics of studies included in the review. The included studies were published between 2013 and 2021, with 68% (n = 13) published from 2018 onwards (Fig. 2). All studies were completed in high income countries and the lead author of most studies (n = 12) were based in the UK. 12 studies used qualitative research methods [17, 18, 27,28,29,30,31,32,33,34,35,36], six used mixed methods [37,38,39,40,41,42] and one was a descriptive piece about a collaborative partnership approach [43]. 15 studies reported using participatory research methodologies, with nine using participatory action research approaches [17, 18, 28, 29, 31, 35, 37, 38, 41] and four using appreciative inquiry [27, 30, 33, 39]. Collaborative enquiry [36], experienced-based co-design [42] and nominal group methods [42] were used once respectively.

Line diagram of publications per year
Approaches to co-production and their components
Descriptions of approaches
A mixture of co-production, co-creation and co-design approaches were used. Table 3 outlines how these terms were defined across the included studies. All studies (n = 4) using co-production approaches provided a definition [17, 18, 38, 41], as did most of the studies (n = 6) using co-creation [28, 29, 31, 36, 37, 43]. However, only two out of eight studies using co-design approaches included a definition [29, 42] and three studies used the term co-design interchangeably with co-production [32, 33, 42]. Co-design was described as an approach centred on valuing lived experiences at any or all stages of research in order to understand needs and develop a useful product. Co-creation was defined as a collaborative approach involving stakeholders or end-users in the shared creation of outputs that were mutually valuable. In comparison to co-design, co-creation was used to develop a wider range of outputs, ranging from knowledge to outcomes. While definitions of co-production also emphasised collaborative working between stakeholders, these definitions incorporated the concept of equality. Equality was considered in relation to partnership working, respecting knowledge and disrupting power asymmetries.
Focus and topics
Co-production approaches were used to explore a diverse range of problems or topics across multiple fields such as the arts, design, technology and health. The focus of the co-production approaches broadly aligned into three categories (Table 4). Four studies used co-production or co-design to increase understanding or explore a given topic area [17, 18, 32, 33]. Nine studies used co-creation or co-design to develop new ways to deliver care [27,28,29, 31, 34, 37, 39, 40, 43]. These studies specifically focused on dementia care, implementing digital technology, art-based approaches, and individualised approaches. Six studies used co-production, co-creation or co-design to support care home workforce development [30, 35, 36, 38, 41, 42], with five co-producing outputs aimed at developing capabilities and one addressing motivation at work.
Stakeholder involvement
Stakeholder involvement in the co-production process varied across the studies (Fig. 3). Care home staff and academic institute staff were most often involved (n = 18), followed by residents (n = 11), family and relatives (n = 11) and health and social care professionals or teams (n = 10) respectively. Some studies (n = 7) included proxy representatives for care home residents, such as older people. Other stakeholder groups were linked to the problem or topic area to be addressed, such as design and technology staff.

Bar chart of stakeholder group involvement
Stages and levels of stakeholder participation
Stakeholders participated in co-production at various stages as represented by the image below of two carousels connected by a path (Fig. 4). The carousels depict how stakeholders participated in the cyclical process of co-producing the research project, or of co-producing the intended output, or in elements of both processes. Outputs of co-production in the included studies ranged from conceptual knowledge or models to tangible products.

Carousels of co-production
There was variation in the points at which stakeholders became involved or ceased involvement in each co-production cycle, shown by the stakeholders on the diagram getting on and off the co-production carousals at different points. An illustrative example is provided in Fig. 5

Illustrative example of stakeholder participation in co-production processes
For the research process, stakeholders were most often reported to participate in conducting the research (n = 10) [17, 18, 28, 30, 32, 35, 37,38,39, 43] and less commonly reported to be involved exclusively in the design (n = 3) [17, 39, 41] or evaluation (n = 5) [18, 29, 35, 37, 39] stages of the co-production research process. Stakeholders were commonly involved in the co-production of the output, mostly in the development stage (n = 15) [17, 18, 27,28,29,30,31, 33, 34, 36,37,38, 40,41,42]. Stakeholders tested early iterations or prototypes in some studies (n = 8) [30,31,32, 34, 35, 40,41,42].
Involvement of stakeholders across the studies differed. There was no pattern in the stages that stakeholders were involved in based on the use of the terms co-production, co-creation or co-design. Sometimes reporting of involvement seemed to be linked to the article’s aim and the context and timelines of research programmes. For instance, Manthorpe at el [39]. aimed to reflect on the completion of a large five year research programme and report involvement in all stages of the co-production research process. Other studies [27, 36], appeared to be smaller projects with an aim to develop a specific output and reported involvement of stakeholders exclusively in co-production of the output through participation in interviews and workshops. Stages of involvement in the included studies were sometimes difficult to decipher based on the information reported in the original studies. For instance, Fowler-Davis et al. [32] reported a co-produced evaluation of an approach to support care homes during the Covid-19 pandemic. NHS and care home staff were then involved in sharing their experiences of the approach. While the authors state the approach itself was collaborative, it is unclear whether it was also co-produced. Thus, some of the variation seen may be due to differences in reporting.
The level of active stakeholder participation in the studies, on a sliding scale of high to low, is depicted by the horses moving up and down on the carousels. The degree to which stakeholders were supported to participate as equal partners in alignment with key principles of co-production was rarely reported. Where information was provided, the level of participation appeared to vary. For example, in some studies stakeholders attended co-creation workshops to contribute their ideas or perspectives but the topics and format of the discussion were set by the research team [29, 34]. In other studies, stakeholders were actively involved in deciding the focus of discussions, as well as contributing their ideas and perspectives, suggesting a higher degree of stakeholder involvement [18, 28].
Approaches to engaging care home staff and residents
Co-production of the research
Care home staff in various roles, residents and groups representing residents were involved in the co-production of the research using numerous approaches. Residents, older people and care home staff were part of research advisory groups involved in designing research projects or programmes [17, 28]. Most commonly (n = 9), staff and groups who represented residents were involved in conducting the research as a member of a core research group [18, 28, 30, 32, 35], as a co-researcher [17, 36, 39, 43], or through an established academic-care collaboration [38, 43]. Five studies involved residents, groups who represent residents and staff in evaluating the co-production process. This was done by conducting semi-structured interviews about their experiences of the process [18, 29, 35], incorporating stakeholder reflections into the evaluation [17, 39], or through involvement in data analysis [37, 39].
Co-production of the output
Care home staff, residents, and representatives of residents were more often involved in the process of co-producing the output in comparison to co-producing the research. A wide variety of methods were used across 16 studies to engage staff and residents in developing the output [17, 18, 27,28,29,30,31, 33,34,35,36,37,38, 40,41,42]. The most common approach was to hold a series of workshops or meetings [18, 27, 29, 33, 34, 37]. Similarly, there was heterogeneity in approaches to engage staff in testing the output across seven studies [30,31,32, 35, 40,41,42], with the most common approach being one-to-one interviews. In contrast, only two studies involved residents, and specifically residents with cognitive impairments, in testing the outputs and both used user-testing methods [34, 40].
Barriers and facilitators to achieving co-production
Barriers to in 11 studies [17, 18, 29,30,31, 33, 34, 37, 39, 41, 42] and facilitators of co-production were reported in 13 studies [17, 18, 29,30,31, 34, 35, 37,38,39,40, 42, 43]. As few studies formally evaluated the co-production process, these were mostly reported in the discussion sections of included studies.
Barriers and facilitators to achieving each NIHR co-production principle [3] are provided in Table 5 with specific examples explained below. Barriers and facilitators are presented according to the principle that the research team felt they most strongly resonated with; however, it should be noted that they often related to more than one principle as the principles are interconnected. Barriers and facilitators are presented in the same manner as they were portrayed in the original articles.
Some barriers and facilitators are closely related. For instance, balancing different forms of knowledge was a reported barrier, whereas recognising and utilising different forms of knowledge was a facilitator.
Sharing power
Sharing power relates to shared ownership of research [3].
Four barriers to achieving this principle were identified from four studies: the burden of supporting resident involvement on care staff [39, 41], gatekeeping [39, 42], ethical procedures [17], delineating roles in the research process [17, 39]. For example, one study [17] discussed how ethical procedures, such as formal signed consent, may have reinforced power imbalances by categorising older people as vulnerable or dependent, and restrictions on how residents could participate deterred some from taking part.
However, two facilitators of power sharing were reported in three studies: creating opportunities to challenge dominant views [17, 18, 39], reflexivity of project leads and researchers [18]. For instance, expert roles helped to challenge dominant views by elevating the social status of residents, enabling authority and opportunities to be involved in discussions [17]. Provision of opportunities for critical reflection and discussion was reported as beneficial in a study exploring LGBT inclusion [18].
Including all perspectives and skills
This principle relates to ensuring that research teams involve diverse experiences, expertise and skills [3].
Five barriers relating to inclusivity were noted across eight studies: not enough involvement of key stakeholders [18, 31, 41, 42], pressures on care home and healthcare professionals [18, 37,38,39], care home resident characteristics [37, 39], limited depth of discussion [31, 37], difficulties with stretching perspectives [18, 34]. Focusing on characteristics of residents as an example, recruitment of people with dementia was described as challenging due to reduced cognition and stigma associated with this condition [37, 39]. Fatigue and low concentration levels led to less time to cover planned topic areas in workshops [37].
In contrast, three facilitators to inclusive co-production were identified from five studies: stimulating experiences [29, 40], care home staff’s willingness to participate [18, 38], flexible approaches [18, 34, 40]. Stimulating experience was specific to studies that involved stakeholders from the fields of arts and design. For instance, Treadaway et al. [40] held an event in an art studio with multiple stakeholders, including older people, family members, carers, health professionals, and designers, and provided sensory stimulation through handling materials. This was reported to facilitate creativity and fun by attendees.
Respecting and valuing knowledge
This principle involves viewing and appreciating all types of knowledge as equal [3].
Two challenges to this principle were reported across five studies: lack of self-confidence [18, 30, 37], balancing different forms of knowledge [28, 37]. Lack of self-confidence affected a range of stakeholders. One study described residents’ “feelings of being useless” (p.11) [37]. Similarly, advisors in another study described feeling “out of their depth” (p.6) [18]. Care home staff lacked confidence in their influencing skills [30].
Involvement across design stages [42] and recognizing and utilising different forms of knowledge were facilitators to respecting knowledge across six studies [17, 18, 31, 39, 40, 42]. The latter involved valuing the experiential, subject-specific, organisational and political knowledge held by different stakeholders as assets.
Reciprocity
Reciprocity refers to benefitting from participation in co-production [3].
Potential harms of participation were noted in studies exploring difficult experiences and discrimination. For example, advisors who identified as LGBT in Willis et al.’s [18]. study described re-living painful experiences and feeling anxious when challenging beliefs of other participants. Older adults were worried there may be negative consequences to sharing their experiences regarding mistreatment of residents [17].
However, two facilitators to reciprocity were noted in five studies: providing support [18], providing learning opportunities [18, 29, 35, 40], clarifying expectations [38]. Using Willis et al. [18] as an example, advocates were provided emotional and practical support through regular contact with the project leader and received peer support through working in pairs to mitigate against potential harms. Learning opportunities were provided through structured training to provide background to the project and build connection between advisors.
Building and maintaining relationships
Relational working is a core component of co-production [3].
Four barriers to this concept were noted in six studies and related to: relationships with management [18, 31, 41], optimising links with stakeholders [37, 39], differences between stakeholders [18, 31, 35, 37, 39], practical challenges [18, 31, 39]. Differences between stakeholders was most often mentioned. Several studies mentioned a lack of understanding between stakeholders due to differences in language, theories, moral beliefs, and professional and organisational cultures [18, 31, 35, 39].
More often, six facilitators regarding relationships were noted across nine studies: building and utilising existing partnerships [38, 39], regular meetings and dialogue [18, 31, 39], establishing ways of working [31, 39, 40], project leadership [31, 35, 37, 39], connection through creative approaches [29, 30], sustaining relationships through participatory approaches [39]. To support relational working between different stakeholders, approaches such as developing common language [31], processes and outcomes [39] were used. However, in Treadaway et al.’s [40] project, establishing ways of working involved recognising that one stakeholder group (technologists) preferred a different way of working to other stakeholders.
Other practical considerations
Practical considerations that did not fit within the principles of co-production were captured by some studies. Patel et al. [41] highlighted that feasibility of co-production on a wider scale may be challenging and reflected on concerns regarding the practicalities of involving a larger number of care homes in the co-production process and providing their co-produced training on a larger scale. In contrast, four studies identified logistical arrangements that may facilitate co-production. Access to time and resources was most commonly mentioned; this related to optimising the success of workshops [31], opportunities for reflexivity [18] and expanding research programmes [43].
Discussion
This scoping review identified that research using co-production approaches in care homes is limited. Most studies employed qualitative methods and participatory methodologies. Research was conducted across a variety of fields, involved multiple stakeholders, and addressed a wide range of topics of relevance to care home residents and staff. A range of approaches, such as workshops, interviews and focus groups, were used to engage care home residents and staff in co-production; however, the co-production process or the co-produced output was rarely evaluated. The review has identified setting-specific insights into using co-production in care homes, such as identification of key stakeholders, approaches for involving them in research, and identification of potential barriers and facilitators when applying principles of co-production in this context. These findings could be used to inform the design of future studies and to actively involve residents and care home staff in this process.
Wider context
In line with other reviews exploring co-production in health and social care research [5, 53], we identified growth in publications using co-production in care home settings over the last decade. Whereas co-production research conducted in the health field began to appear as early as the 1990s, [5] the earliest study identified in this review was published in 2013. This suggests that there is a lag in the use of co-production approaches between health and care home settings therefore continual investigation of co-production in care home contexts is required. The 2021 UK Government social care policy white paper ‘People at the Heart of Care’ [54] directly references co-production on multiple occasions therefore it is likely that the co-production research in care home settings will continue to accelerate in the UK in the coming years.
Heterogeneity in reporting of definitions and the underpinning co-production principles was also a common feature of the studies included in the review. This concurs with a scoping review of definitions of co-production and co-design in health and social care research which found a third of included articles provided no definition or explanation [53]. This review also identified an increase in the number of new definitions and an increase in the number of publications using the terms co‐production or co‐design while not involving patients or the public over the last decade [53]. There is much debate about the need for standardised definitions. Concerns have been raised regarding broad definitions which may have the potential to be misappropriated [55]. On the other hand, it has been suggested that a looser definition of co-production allows more flexibility to adapt approaches depending on the context, and holding research against rigid principles may be more harmful by inadvertently discouraging participation through setting unattainable standards [3, 9, 56]. Based on our experiences of completing this review, and in alignment with the conclusions of reviews in other settings [9, 10, 53], we suggest clearer reporting about how authors define and operationalise co-production in care home settings would be a pragmatic compromise which allows for flexibility while also aiding the reader’s assessment of authenticity. Reporting frameworks such as the one that guided the data extraction process in this review may be helpful [23]; however, based on our experiences of using the framework to support data charting, further refinement may be needed if the framework is to encapsulate all approaches that fall under the co-production umbrella. Some aspects of the framework could be streamlined to avoid repetition while others require further explanation. Reporting of co-production research is therefore an area for further development.
Evaluation of the co-production process, how well stakeholders were engaged in the process, and the output of co-production was lacking in the included studies. This is similar to findings of other reviews and ethnographic research which focussed on co-production in health settings rather than social care settings [9, 10, 57, 58]. Further exploration of how to evaluate co-production approaches and outputs of co-production is required. Reporting and reflection on the process of co-production may support others to learn from past research. The collaborator group involved in this review were also surprised at the lack of reporting about the emotional component of co-production and how it feels to be a co-researcher or stakeholder working in the space of co-production. Exploration of experiences’ of PPI in research and clinical commissioning group (CCG) activities identified mixed feelings among PPI representatives regarding the extent to which they felt valued, respected and confident in their PPI role [59, 60]. Feelings of frustration and apprehension have been reported as barriers to resident involvement in PPI research activities, whereas feeling valued and trusting relationships were identified as facilitators [16]. While these findings may be relevant, it is unclear whether the same factors would apply to co-production activities, which seek to address power imbalances, and to the multiple stakeholder groups in care home settings. This is another area for future research.
Barriers and facilitators to co-production in care home research were identified. These may be helpful for planning future co-production approaches in this context. Our review adds to the existing literature by identifying barriers and facilitators that are specific to co-production in care home settings, such as consideration of care home resident characteristics and the potential burden on care home staff. Flexibility and early engagement of care home residents and staff will be needed to plan co-production activities in a way that is inclusive of their needs. Some of the factors identified align with key considerations identified from co-production research in wider health settings, including the importance of support from management and frontline staff, researchers’ skill sets (building relationships, managing expectations, negotiation, flexibility), and the impact of traditional academic practice and logistical arrangements on facilitating authentic co-production [9]. This suggests that greater investment in training and programme funding, and reviewing academic structures, such as governance processes and resource allocation, may be required if authentic co-production is the intended aim.
Strengths and limitations
There is increasing interest in the use of co-production in social care settings and the review is timely to support researchers in undertaking co-production activities in care home contexts. A collaborator group of care home and health care representatives were involved in decision-making regarding the presentation and implications of findings from their perspectives. The review was completed in line with the JBI scoping review methodology [19] and PRISMA-ScR reporting guidelines [20] to aid transparency and rigour. No data restrictions were applied which allowed us to capture the breadth of available published literature. All studies were independently screened by two reviewers, and data charting and synthesis involved multiple reviewers to enhance replicability.
There are several limitations to the review. The search strategy may not have identified all studies due to the exclusion of non-English studies and grey literature. Our decision to include only papers that explicitly stated they had used co-production, co-creation or co-design may have excluded relevant studies using wider terminology. These terms were not used in social care research papers published before 2013 therefore the review may have missed earlier studies that used approaches in keeping with the principles of co-production. However, as these terms are already unclear concepts, we were mindful of not adding to this confusion and muddying the implications of the review’s findings. Although data charted was checked by a second reviewer, modification of the data charting table using a reporting checklist that was developed from a small number of co-creation case studies may have led us to overlook important components of co-production approaches that were not included in this. Our focus on published research may mean that the findings from the included studies are written from researchers’ perspectives for an academic audience therefore the review findings may not be representative of the views of the diverse stakeholders involved in co-production approaches in care homes. Another limitation is that the study collaborator group involved in this review does not include representation of current care home residents therefore the interpretation of the review findings may not be reflective of residents’ perspectives. Please see Additional file 4 for further information about our attempts to involve residents in this project and our reflections on this experience.
Conclusions
This review has identified studies which used co-production approaches in a care home setting. A diverse range of approaches to co-production were used and a wide range of stakeholders participated at various stages and levels, including staff and residents. Barriers and facilitators to achieving authentic co-production in care home settings were also identified. The components, barriers and facilitators identified should be used to inform future co-production research. Future studies should be explicit in reporting what is meant by co-production, the methods used to support co-production and the extent to which co-production was achieved. Sharing of key learning is required to support this field to develop. Evaluation of co-production processes from diverse perspectives, including stakeholders’ experiences of co-production, are areas for future research in care home settings.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CCG:
-
Clinical Commissioning Group
- JBI:
-
Joanna Briggs Institute
- PCC:
-
Population, concept, context
- PPI:
-
Patient and Public Involvement
- PRISMA-ScR:
-
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews
References
Filipe A, Renedo A, Marston C. The co-production of what? Knowledge, values, and social relations in health care. PLoS Biol. 2017;15(5): e2001403. https://doi.org/10.1371/journal.pbio.2001403.
Verschuere B, Brandsen T, Pestoff V. Co-production: The state of the art in research and the future agenda. VOLUNTAS Int J Volunt Nonprofit Organ. 2012;23(4):1083–101. https://doi.org/10.1007/s11266-012-9307-8.
National Institute for Health Research. Guidance on co-producing a research project. https://www.learningforinvolvement.org.uk/?opportunity=nihr-guidance-on-co-producing-a-research-project. Accessed 30 Sep 2022.
Social Care Institute for Excellence. Co-production in social care: what it is and how to do it—at a glance. https://www.scie.org.uk/publications/guides/guide51/at-a-glance/. Accessed 30 Sep 2022.
Fusco F, Marsilio M, Guglielmetti C. Co-production in health policy and management: a comprehensive bibliometric review. BMC Health Serv Res. 2020;20(1):504.
New Economics Foundation. Co-production: a manifesto for growing the core economy. https://neweconomics.org/uploads/files/5abec531b2a775dc8d_qjm6bqzpt.pdf. Accessed 30 Sep 2022.
Brandsen T, Steen T, Verschuere B. Co-production and co-creation: engaging citizens in public services. New York: Routledge; 2018.
Vargas C, Whelan J, Brimblecombe J, Allender S. Co-creation, co-design, co-production for public health—a perspective on definitions and distinctions. Public Health Res Pract. 2022;32(2): e3222211. https://doi.org/10.17061/phrp3222211.
Smith H, Budworth L, Grindey C, Hague I, Hamer N, Kislov R, et al. Co-production practice and future research priorities in United Kingdom-funded applied health research: a scoping review. Health Res Policy Syst. 2022;20(1):36. https://doi.org/10.1186/s12961-022-00838-x.
Slattery P, Saeri AK, Bragge P. Research co-design in health: a rapid overview of reviews. Health Res Policy Syst. 2020;18(1):17. https://doi.org/10.1186/s12961-020-0528-9.
Competitions and Markets Authority. Care homes market study: summary of final report. https://www.gov.uk/government/publications/care-homes-market-study-summary-of-final-report/care-homes-market-study-summary-of-final-report. Accessed 30 Sep 2022.
Gordon AL, Franklin M, Bradshaw L, Logan P, Elliott R, Gladman JRF. Health status of UK care home residents: a cohort study. Age Ageing. 2013;43(1):97–103. https://doi.org/10.1093/ageing/aft077.
Baylis A, Perks-Baker S. Enhanced health in care homes: learning from experiences so far. London: The King’s Fund; 2017.
Peryer G, Kelly S, Blake J, Burton JK, Irvine L, Cowan A, et al. Contextual factors influencing complex intervention research processes in care homes: a systematic review and framework synthesis. Age Ageing. 2022;51(3):afac014. https://doi.org/10.1093/ageing/afac014.
Holland-Hart DM, Addis SM, Edwards A, Kenkre JE, Wood F. Coproduction and health: public and clinicians’ perceptions of the barriers and facilitators. Health Expect. 2019;22(1):93–101. https://doi.org/10.1111/hex.12834.
Backhouse T, Kenkmann A, Lane K, Penhale B, Poland F, Killett A. Older care-home residents as collaborators or advisors in research: a systematic review. Age Ageing. 2016;45(3):337–45. https://doi.org/10.1093/ageing/afv201.
Burns D, Hyde P, Killett A, Poland F, Gray R. Participatory organizational research: examining voice in the co-production of knowledge. Br J Manag. 2014;25(1):133–44. https://doi.org/10.1111/j.1467-8551.2012.00841.x.
Willis P, Almack K, Hafford-Letchfield T, Simpson P, Billings B, Mall N. Turning the co-production corner: methodological reflections from an action research project to promote lgbt inclusion in care homes for older people. Int J Environ Res Public Health. 2018;15(4):695. https://doi.org/10.3390/ijerph15040695.
Peters MDJGC, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: Scoping reviews (2020 version). In: Aromataris EMZ, editor. JBI manual for evidence synthesis. Adelaide: Joanna Briggs Institute; 2020.
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73. https://doi.org/10.7326/M18-0850.
Hallam F. Approaches to co-production in care homes: a scoping review. https://doi.org/10.17605/OSF.IO/TFPHC
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210.
Leask CF, Sandlund M, Skelton DA, Altenburg TM, Cardon G, Chinapaw MJM, et al. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res Involv Engagem. 2019;5(1):2. https://doi.org/10.1186/s40900-018-0136-9.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71. https://doi.org/10.1136/bmj.n71.
Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):143. https://doi.org/10.1186/s12874-018-0611-x.
Staniszewska S, Brett J, Simera I, Seers K, Mockford C, Goodlad S, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. Res Involv Engagem. 2017;3(1):13. https://doi.org/10.1186/s40900-017-0062-2.
Curtis K, Brooks S. Digital health technology: factors affecting implementation in nursing homes. Nurs Older People. 2020;32(2):14–21. https://doi.org/10.7748/nop.2020.e1236.
de Boer B, Bozdemir B, Jansen J, Hermans M, Hamers JPH, Verbeek H. The homestead: developing a conceptual framework through co-creation for innovating long-term dementia care environments. Int J Environ Res Public Health. 2020;18(1):23. https://doi.org/10.3390/ijerph18010057.
Demecs IP, Miller E. Participatory art in residential aged care: a visual and interpretative phenomenological analysis of older residents’ engagement with tapestry weaving. J Occup Sci. 2019;26(1):99–114. https://doi.org/10.1080/14427591.2018.1515649.
Dewar B, MacBride T. Developing caring conversations in care homes: an appreciative inquiry. Health Soc Care Community. 2017;25(4):1375–86. https://doi.org/10.1111/hsc.12436.
Dugstad J, Eide T, Nilsen ER, Eide H. Towards successful digital transformation through co-creation: a longitudinal study of a four-year implementation of digital monitoring technology in residential care for persons with dementia. BMC Health Serv Res. 2019;19(1):366. https://doi.org/10.1186/s12913-019-4191-1.
Fowler-Davis S, Cholerton R, Philbin M, Clark K, Hunt G. Impact of the enhanced universal support offer to care homes during COVID-19 in the UK: evaluation using appreciative inquiry. Health Soc Care Community. 2021;25:25. https://doi.org/10.1111/hsc.13612.
Hafford-Letchfield T, Gleeson H, Ryan P, Billings B, Teacher R, Quaife M, et al. “He just gave up”: an exploratory study into the perspectives of paid carers on supporting older people living in care homes with depression, self-harm, and suicide ideation and behaviours. Ageing Soc. 2020;40(5):984–1003. https://doi.org/10.1017/S0144686X18001447.
Jamin G, Luyten T, Delsing R, Braun S. The process of co-creating the interface for VENSTER, an interactive artwork for nursing home residents with dementia. Disabil Rehabil Assist Technol. 2018;13(8):809–18. https://doi.org/10.1080/17483107.2017.1385102.
Prentice J, Weatherall M, Grainger R, Levack W. “Tell someone who cares”: participation action research on workplace engagement of caregivers in aged residential care, NZ. Australas J Ageing. 2021;40(2):e109–15. https://doi.org/10.1111/ajag.12876.
Watson J, Horseman Z, Fawcett T, Hockley J, Rhynas S. Care home nursing: co-creating curricular content with student nurses. Nurse Educ Today. 2020;84: 104233. https://doi.org/10.1016/j.nedt.2019.104233.
Gine-Garriga M, Lund M, Dall PM, Chastin SFM, Perez S, Skelton DA. A novel approach to reduce sedentary behaviour in care home residents: The GET READY Study utilising service-learning and co-creation. Int J Environ Res Public Health. 2019;16(3):01. https://doi.org/10.3390/ijerph16030418.
Griffiths AW, Devi R, Cheetham B, Heaton L, Le A, Ellwood A, et al. Maintaining and improving mouth care for care home residents: A participatory research project. Int J Older People Nurs. 2021;16(5): e12394. https://doi.org/10.1111/opn.12394.
Manthorpe J, Iliffe S, Goodman C, Drennan V, Warner J. Working together in dementia research: reflections on the EVIDEM programme. Work Older People. 2013;17(4):138–45. https://doi.org/10.1108/WWOP-08-2013-0017.
Treadaway C, Kenning G. Sensor e-textiles: person centered co-design for people with late stage dementia. Work Older People. 2016;20(2):76–85. https://doi.org/10.1108/WWOP-09-2015-0022.
Patel R, Robertson C, Gallagher JE. Collaborating for oral health in support of vulnerable older people: co-production of oral health training in care homes. J Public Health. 2019;41(1):164–9. https://doi.org/10.1093/pubmed/fdx162.
Pownall S, Barnett E, Skilbeck J, Jimenez-Aranda A, Fowler-Davis S. The development of a digital dysphagia guide with care homes: co-production and evaluation of a nutrition support tool. Geriatrics. 2019;4(3):15. https://doi.org/10.3390/geriatrics4030048.
Luijkx K, van Boekel L, Janssen M, Verbiest M, Stoop A. The Academic collaborative center older adults: a description of co-creation between science, care practice and education with the aim to contribute to person-centered care for older adults. Int J Environ Res Public Health. 2020;17(23):1–14. https://doi.org/10.3390/ijerph17239014.
Stavros JM, Godwin LN, Cooperrider DL. Appreciative inquiry: organization development and the strengths revolution. In: Rothwell WJ, Stavros JM, Sullivan RL, editors. Practicing organization development: leading transformation and change. 4th ed. Hoboken: Wiley; 2015.
Bergdahl E, Ternestedt B-M, Berterö C, Andershed B. The theory of a co-creative process in advanced palliative home care nursing encounters: a qualitative deductive approach over time. Nurs Open. 2019;6(1):175–88. https://doi.org/10.1002/nop2.203.
Voorberg WH, Bekkers VJJM, Tummers LG. A systematic review of co-creation and co-production: embarking on the social innovation journey. Public Manag Rev. 2015;17(9):1333–57. https://doi.org/10.1080/14719037.2014.930505.
Dewar B. Caring about caring: an appreciative inquiry about compassionate relationship centred care. (Thesis). Edinburgh Napier University. http://researchrepository.napier.ac.uk/id/eprint/4845. Accessed 28 Nov 2022.
Ludema JD, Fry RE. The practice of appreciative inquiry. In: Reason P, Bradbury HB, editors. The SAGE handbook of action research. 2nd ed. London: SAGE; 2012. p. 2012.
Lewin K. Action research and minority problems. J Soc Issues. 1946;2:34–46. https://doi.org/10.1111/j.1540-4560.1946.tb02295.x.
Bovill C. An investigation of co-created curricula within higher education in the UK, Ireland and the USA. Innov Educ Teach Int. 2014;51(1):15–25. https://doi.org/10.1080/14703297.2013.770264.
Social Care Institute for Excellence. Improving oral health for adults in care homes: a quick guide for care home managers. https://www.scie.org.uk/publications/ataglance/improving-oral-health-for-adults-in-care-homes.asp. Accessed 28 Nov 2022.
Facer K, Enright B. Creating living knowledge: the connected communities programme, community-university partnerships and the participatory turn in the production of knowledge. https://research-information.bris.ac.uk/ws/portalfiles/portal/75082783/FINAL_FINAL_CC_Creating_Living_Knowledge_Report.pdf. Accessed 28 Nov 2022.
Masterson D, Areskoug Josefsson K, Robert G, Nylander E, Kjellström S. Mapping definitions of co-production and co-design in health and social care: a systematic scoping review providing lessons for the future. Health Expect. 2022;25(3):902–13. https://doi.org/10.1111/hex.13470.
UK Government Department of Health and Social Care. People at the Heart of Care: adult social care reform white paper. https://www.gov.uk/government/publications/people-at-the-heart-of-care-adult-social-care-reform-white-paper. Accessed 29 Sep 2022.
Williams O, Sarre S, Papoulias SC, Knowles S, Robert G, Beresford P, et al. Lost in the shadows: reflections on the dark side of co-production. Health Res Policy Syst. 2020;18(1):43. https://doi.org/10.1186/s12961-020-00558-0.
Oliver K, Kothari A, Mays N. The dark side of coproduction: do the costs outweigh the benefits for health research? Health Res Policy Syst. 2019;17(1):33. https://doi.org/10.1186/s12961-019-0432-3.
Cowdell F, Dyson J, Sykes M, Dam R, Pendleton R. How and how well have older people been engaged in healthcare intervention design, development or delivery using co-methodologies: a scoping review with narrative summary. Health Soc Care Community. 2020;30(2):776–98. https://doi.org/10.1111/hsc.13199.
Clarke J, Waring J, Timmons S. The challenge of inclusive coproduction: The importance of situated rituals and emotional inclusivity in the coproduction of health research projects. Soc Policy Adm. 2019;53(2):233–48. https://doi.org/10.1111/spol.12459.
Madison S, Colon-Moya AD, Morales-Cosme W, Lorenzi M, Diaz A, Hickson B, et al. Evolution of a research team: the patient partner perspective. Res Involv Engagem. 2022;8(1):42. https://doi.org/10.1186/s40900-022-00377-3.
O’Shea A, Boaz AL, Chambers M. A hierarchy of power: the place of patient and public involvement in healthcare service development. Front Sociol. 2019;4:38. https://doi.org/10.3389/fsoc.2019.00038.
Acknowledgements
We would like to thank all members of the NIHR Advanced Fellowship collaborator group for their input and unique insights into this work.
Funding
This report is independent research supported by the National Institute for Health Research NIHR Advanced Fellowship, Dr Katharine Robinson, NIHR300115. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.
Author information
Authors and Affiliations
Contributions
FHB contributed to the conceptualisation and the design of the review, collected and analysed data as the first reviewer, and wrote the first version of the manuscript; PL and ST contributed to the conceptualisation and design of the review, provided feedback on data analysis, and contributed to the writing of the manuscript; KR contributed to the conceptualisation and design of the review, collected and analysed data as the second reviewer, and contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA-ScR checklist
Additional file 2.
Example search strategy for MEDLINE
Additional file 3.
Data charting table
Additional file 4.
GRIPP2 reporting form
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Hallam-Bowles, F.V., Logan, P.A., Timmons, S. et al. Approaches to co-production of research in care homes: a scoping review. Res Involv Engagem 8, 74 (2022). https://doi.org/10.1186/s40900-022-00408-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40900-022-00408-z